
Abstract
Study Design
Prospective disease-oriented study.
Objective
To describe the MRI findings in patients with failed conservative treatment for degenerative lumbar diseases and to identify predictors of back pain intensity in these patients.
Methods
We analyzed demographic (sex, age) and clinical scale data as well as the lumbar MRI findings (Pfirrmann disc degeneration, Modic types, endplate defects, disc height and osteophytes) in RuDDS patients. We examined the prevalence of degenerative changes in different age groups and searched for predictors of back pain intensity after the procedure in patients with specific leading syndromes.
Results
Patients with failed conservative treatment demonstrate more severe degeneration of the discs and endplates, more Modic changes, and higher Jarosz scores than reported in population-based studies. Individuals with degenerative stenosis have the most severe lumbar spine degeneration compared to patients with other leading syndromes (facet joint pain, lumbar disc herniation, degenerative deformity) (P < 0.004). Lumbar MRI findings had a weak (β < 0.1) though statistically significant effect on back pain intensity before the procedure and clinically significant back pain attenuation after it. Smoking had a greater impact on back pain and its attenuation after the procedure, especially in patients with degenerative stenosis (β = 0.307 and OR = 2.03, respectively).
Conclusion
This is the first characterization of MRI findings in patients with failed conservative treatment. Smokers show more prominent back pain attenuation after the procedure than non-smokers; however it is not clear whether this treatment effect is sufficient.
The trial registry number is NCT04600544 on clinicaltrials.gov.
Introduction
Low back pain (LBP) sooner or later affects everyone.1,2 Being one of the major causes of LBP, degenerative diseases of the lumbar spine (DDLS) require more attention and effort in conservative treatment.3,4 DDLS therapy is a great challenge, especially when conservative treatment fails, 5 and minimally invasive procedures (such as radiofrequency ablation) and surgical options come into the forefront.
Every DDLS patient undergoing long-term conservative treatment or planning surgery undergoes lumbar spine MRI. Degenerative findings on MRI reflect DDLS and include intervertebral discs degradation, vertebral endplates defects, and osteophytes. There is information about lumbar MRI findings on a population scale,6-8 including their associations with ethnicity, 9 sagittal balance, 10 and bone mineral density. 11 However, there are no data on the most common group seen by spinal surgeons – those with failed conservative treatment. It remains unclear whether their MRI findings differ from those in the general population. Moreover, no such studies have been conducted in Russia. To date, there are only limited surveys of lumbar MRI in a small sample of footballers (soccer players in North American usage) from the Russian Premier League. 12
Regardless of the type of DDLS, whether surgical or minimally invasive procedures, both the doctor and patient expect an attenuation of back/leg pain and a decrease in functional disability.5,13 LBP intensity and its attenuation are extremely important after invasive procedures, which is why it is relevant to seek potential predictors, primarily among MRI findings. These associations are controversial: some studies indicate the absence of any association between MRI findings and LBP,6,7,14 while others suggest the opposite.15-17 Putative predictors of pain attenuation after surgery include the ODI value before the procedure,18,19 smoking,20,21 sex,21,22 etc. However, the information on them is heterogeneous, which makes it difficult to apply in practice.
The aim of our study was to describe MRI findings in patients with failed conservative treatment and to identify predictors of back pain intensity in these patients.
Materials and Methods
The Russian disc degeneration study (RuDDS) is a disease-oriented study conducted in two centers in Russia in 2021-2024 to examine lumbar disc degeneration. This is a prospective study (NCT04600544), whose design has been described previously in a protocol. 23 The study involved symptomatic patients with failed conservative treatment for degenerative lumbar diseases that had been conducted for ≥3 months and discontinued at the initiation point of the study. Conservative treatment included drug therapy, physiotherapy, rehabilitation, etc., unless there was evidence of progression of neurological deficit. According to the study protocol, the sample should have also included outpatients, patients with conservative treatment for symptomatic lumbar disc degeneration disease, and other patients with MRI scans of the lumbar spine; however, due to technical issues, it consisted of only inpatients with planned lumbar spine interventions (radiofrequency denervation and surgical procedures). From every patient, we collected socio-demographic data, lumbar spine MRI, and clinical questionnaires. Asymptomatic patients undergoing MRI as outpatients were not willing to participate in the study, fill out questionnaires, or give blood samples. By contrast, the inpatients were happy to participate in a study that could potentially help find the cause of their spinal pathology.
Using 1.5 Tesla scanners, we obtained anonymized lumbar spine MRI scans in DICOM format. We classified disc degeneration according to Pfirrmann grades
24
and assessed Modic changes (MC)
25
for each endplate of the lumbar vertebrae. We evaluated vertebral endplate defects using the Rajasekaran classification
26
and computed the total endplate score (TEP score) as the sum of the endplate defect scores of both upper and lower endplates at every level of the lumbar spine. We also applied the Jarosz classification
27
to estimate the disc height and osteophyte severity (Figure 1). Lumbar MRI image of a 51-year-old patient, Rajasekaran and Jarosz grading scales. -Endplate defect grades by Rajasekaran: L1-L2 – grade 3 and grade 2 (uppermost and lowermost), L2-L3 – grade 2 and grade 3 (uppermost and lowermost), L3-L4 – grade 4 and grade 5 (uppermost and lowermost), L4-L5 – grade 5 and grade 5 (uppermost and lowermost), L5-S1 – grade 5 and grade 5 (uppermost and lowermost). -Jarosz score = 14 (Jarosz disc height: L1-L2 – grade 0, L2-L3 – grade 0, L3-L4 – grade 1, L4-L5 – grade 2, L5-S1 – grade 3; Jarosz osteophytes: L1-L2 – grade 2, L2-L3 – grade 1, L3-L4 – grade 1, L4-L5 – grade 2, L5-S1 – grade 2). 164x223mm (96 x 96 DPI)
The Oswestry Disability Index (ODI) and Douleur Neuropathique 4 Questionnaire (DN4) (a score ≥4 corresponds to neuropathy), as well as Numeric Pain Rating Scales (NPRS) for back and leg pain intensity (ranging from 0 to 10, where 10 corresponds to the highest pain intensity) were completed before and after the procedure. The minimum clinically important difference (MCID) for back NPRS was defined as a ≥1.2 difference between the back NPRS scores before and after the procedure. 28
Based on the leading syndrome, the total sample was split into four groups of patients with (1) facet joint pain, (2) lumbar disc herniation, (3) degenerative stenosis, and (4) degenerative deformity, including spondylolisthesis and sagittal imbalance.
Statistical Analysis
We described the total sample and four groups of patients with different leading syndromes by 16 variables. In addition, we stratified the total sample into eight age groups (from 10 to 90 years with a 10-year gap) and assessed the prevalence of Pfirrmann grade ≥4, MC of any type, and TEP score ≥6 in each of them. We conducted ANOVA for variables transformed to normality with equal variance in four patient groups according to Levene’s test. The remaining quantitative and binary variables were analyzed using the Kruskal-Wallis test. We set a common threshold for statistical significance at P < 0.003. For post-hoc analyses, we used the pairwise t-test in ANOVA, Dunn’s test for quantitative, and Fisher’s exact/Chi-squared test for binary variables in the Kruskal-Wallis test. The significance threshold for post-hoc analyses was P < 0.005. We focused on two clinical outcomes: back NPRS before the procedure and MCID achievement. We utilized Lasso regression to identify predictors among preoperative parameters in the total sample and four patient groups with specific leading syndromes. All computations were performed in R (version 4.3.3).
Results
A total of 912 patients with lumbar spine MRI met the inclusion criteria (Supplemental Figure 1), 56.8% (518/912) of them had completed questionnaires before the intervention. The most common diagnosis among the patients was lumbar disc herniation, 41.11% (375/912); degenerative stenosis was observed in 27.96% (255/912); facet joint pain was diagnosed in 23.13% (211/912); and degenerative deformity was the least prevalent, 7.78% (71/912).
General Characteristics of and MRI Findings in RuDDS Sample With Patient Groups’ Comparison
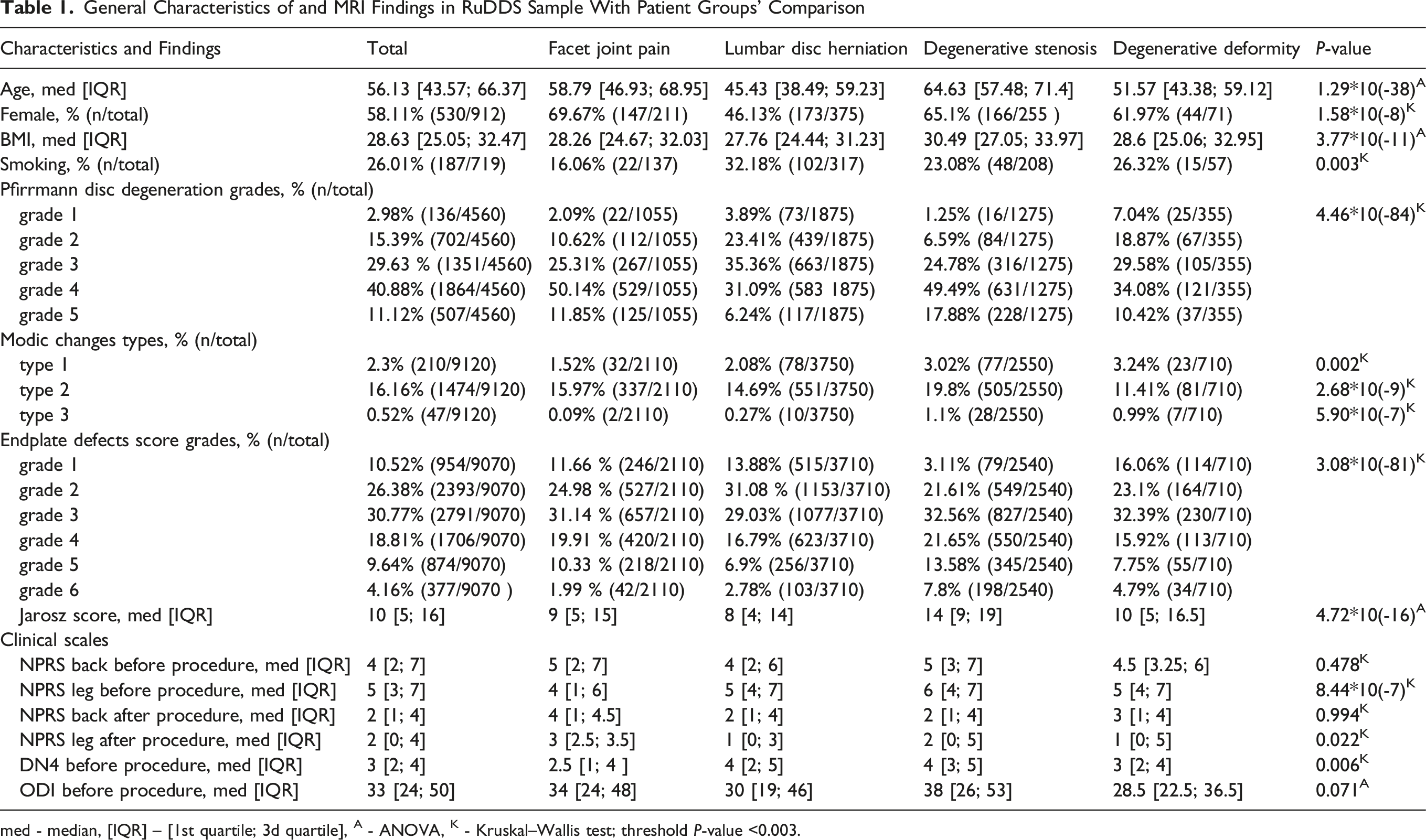
med - median, [IQR] – [1st quartile; 3d quartile], A - ANOVA, K - Kruskal–Wallis test; threshold P-value <0.003.
MRI Findings Across Age Groups
The distribution of pronounced degenerative changes in the lumbar spine (degenerated discs, MC and severe endplate defects) across the age groups is presented in Figure 2. Up to and including the age of 20, we observed only sporadic prominent degenerative changes in the lumbar spine. After the age of 20, at each spine level, at least two (and after 30, all three) types of degenerative changes were detected, with their prevalence being higher at lower levels. The prevalence of degenerative changes at all levels also tended to increase with age, although showing some age-specific patterns. Prevalence of degenerated discs (Pfirrmann grade ≥4), MC of any type and severe endplate defects (TEP score ≥6) across age decades in the total sample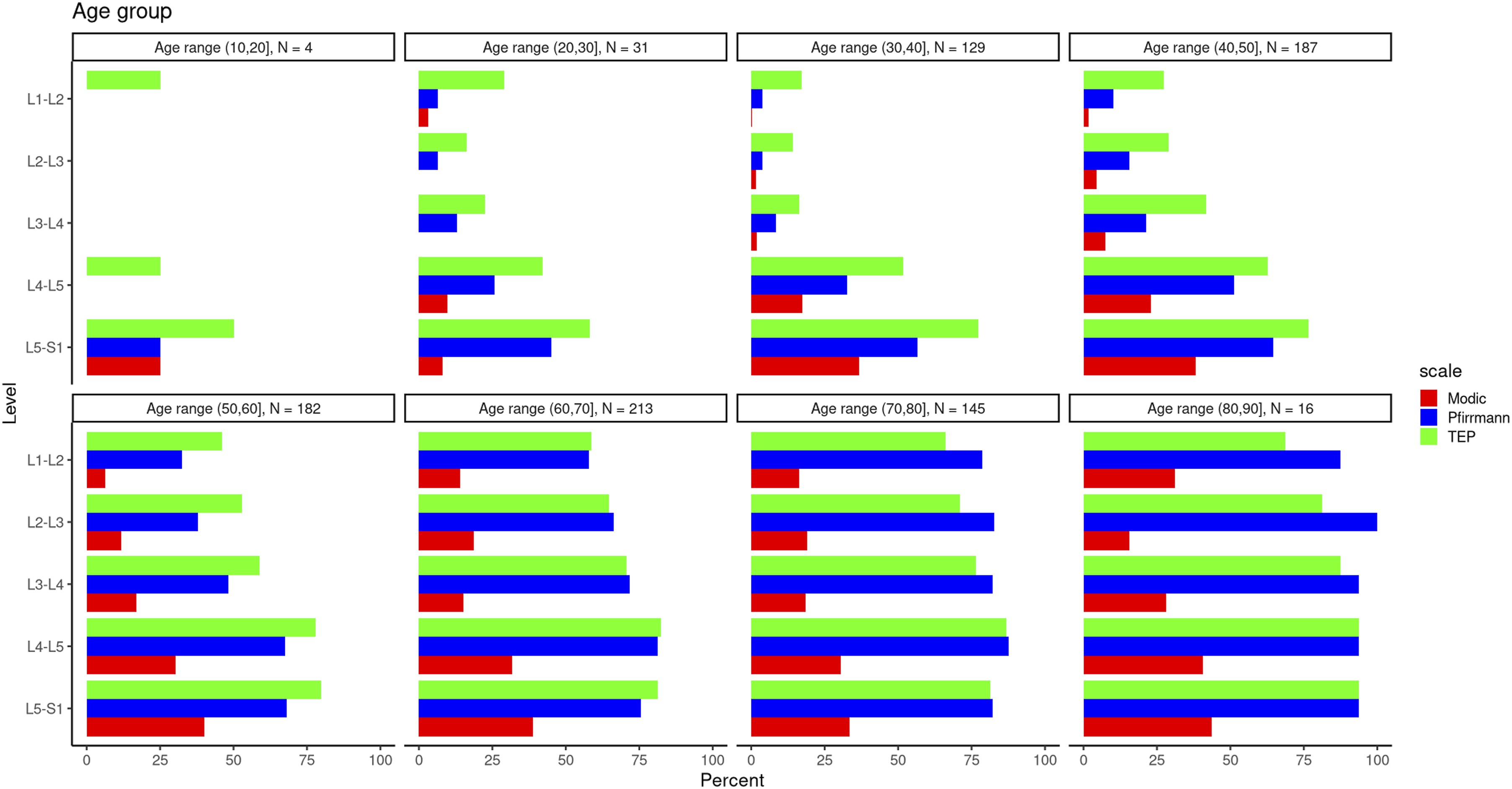
Up to and including the age of 20, severely degenerated discs with Pfirrmann grade ≥4 were observed only at L5-S1 (25%). For each spinal level, the prevalence of severely degenerated discs exceeded 25% after the age of 50 (with a minimum of 32.4% at L1-L2), exceeded 50% after 60 (with a minimum of 57.7% at L1-L2), and exceeded 75% after 70 (with the minimum prevalence being 78.6% at L1-L2).
Modic changes (MC) of any type in patients aged 20 or younger were identified only at L5-S1 (25%), while in the patients aged 20 to 30 years, the prevalence of MC was 3.2%, 9.7% and 8.1% at L1-L2, L4-L5 and L5-S1 levels, respectively. At ages 60-70, the prevalence of MC exceeded 10% for every level (with a minimum of 14.1% at L1-L2). In each age group, the highest prevalence of MC was observed at L5-S1, with a maximum of 43.8% in patients over 80 years old.
For individuals aged 20 years and younger, severe endplate defects (TEP score ≥6) were present at L4-L5 and L5-S1 levels, with a prevalence of 25% and 50%, respectively. They were also found at L1-L2 in 25% of cases as Schmorl’s hernias. We observed severe endplate defects at each spinal level for every age group over 20. At all spine levels, the prevalence of severe endplate defects exceeded 10% (with a minimum of 14.1% at L2-L3) in patients over 30, 25% in patients over 40 (with a minimum of 27.3% at L1-L2), and 50% in patients over 60 (with a minimum of 58.8% at L1-L2). In patients over 70, the highest prevalence of severe endplate defects was 93.8% at L4-L5.
Comparison of Patient Groups with Different Leading Syndromes
Results of the comparison of the four patient groups with different leading syndromes using ANOVA and Kruskal-Wallis tests are provided in Table 1. During the post-hoc analyses, we performed pairwise comparisons of baseline characteristics, including MRI findings, between these groups and found that patients with degenerative stenosis were older than the others, had a greater BMI, more severe disc degeneration according to the Pfirrmann scale, more MC, more prominent endplate defects, and higher Jarosz scores (Supplemental Table 1).
Predictors of Successful Treatment
Regression Coefficients a of Baseline Parameters Including MRI Findings on Back Pain Severity Assessed Based on NPRS and MCID
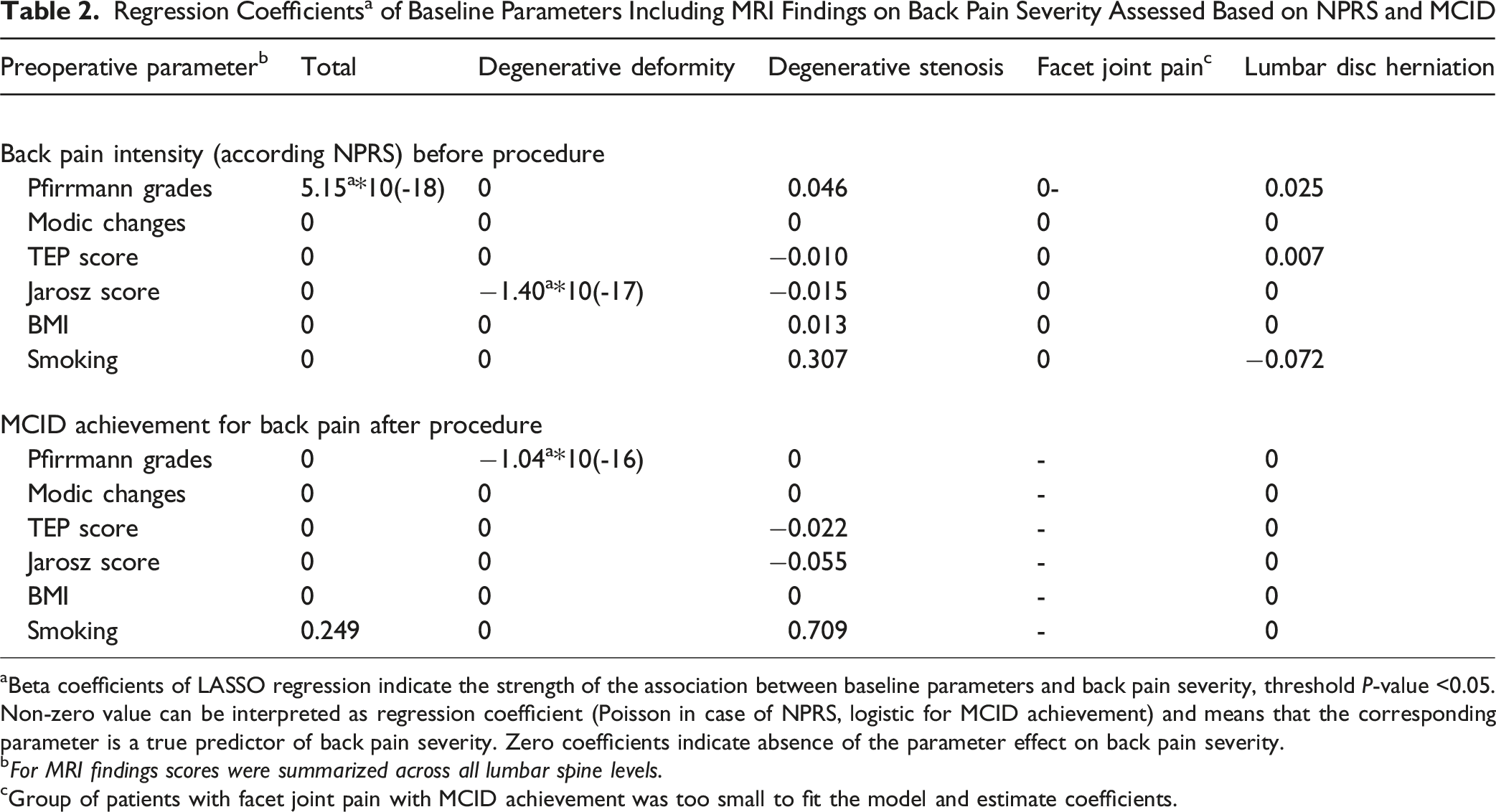
aBeta coefficients of LASSO regression indicate the strength of the association between baseline parameters and back pain severity, threshold P-value <0.05. Non-zero value can be interpreted as regression coefficient (Poisson in case of NPRS, logistic for MCID achievement) and means that the corresponding parameter is a true predictor of back pain severity. Zero coefficients indicate absence of the parameter effect on back pain severity.
bFor MRI findings scores were summarized across all lumbar spine levels.
cGroup of patients with facet joint pain with MCID achievement was too small to fit the model and estimate coefficients.
For MCID achievement, all effects of MRI findings were also modest (β < 0.1). However, smoking appeared to be a meaningful predictor: β = 0.249, OR = 1.28, and P < 0.05 in the total sample, and 0.709, OR = 2.03, P < 0.05 in patients with degenerative stenosis.
Discussion
The novelty of our study is in its focus on a group of patients with failed conservative treatment for degenerative lumbar diseases. These patients are more challenging to treat than their symptomatic peers: their symptoms are persistent, more severe, and may lead to disability, sometimes profound. Individuals considered for invasive procedures typically have persistent pain, with or without neurologic deficit.
Our finding demonstrate that patients with failed conservative treatment exhibit more severe degenerative changes on lumbar spine MRI compared to the general population. In our sample, the prevalence of severely degenerated discs (Pfirrmann grade ≥4) was 56.6% at L5-S1 in patients aged 30-40, increasing with age at all lumbar levels to reach a maximum of 100% at L2-L3 in patients over 80. According to one of the largest studies on MRI findings, 8 the prevalence of discs with severe degeneration was lower in symptomatic patients – 40% at the lower lumbar levels in 30-year-olds, rising to 80% by the age of 70. This suggests that patients with failed conservative treatment in our sample developed more degenerated discs earlier in life and experienced faster progression of degeneration compared to the symptomatic cohort.
In our sample, only 29% of endplates had MC; however, they were present at all lumbar levels in patients over 30. In individuals under 20, MC were observed in 25% of endplates at L5-S1. Previous studies reported MC in 38.9% of endplates in symptomatic patients, 8 representing a 1.3 times higher prevalence than in our study. We assume that MC may contribute to LBP, but they do not represent an indication for invasive procedures.
Data from the TwinsUK study reported a median Jarosz score of 3.46 (SD = 1.14) points. 29 By comparison, our patients demonstrated a median Jarosz score of 10 [5; 16] points, indicating approximately 3-fold more severe degenerative changes in the lumbar spine, and patients with degenerative stenosis showed the most advanced degeneration, with a median Jarosz score of 14 [9; 19] points.
Patients with degenerative stenosis comprised almost one-third of the sample (27.9%). These patients differed most markedly from the other study groups: they were older, had higher BMI values, showed the most advanced lumbar spine degeneration according to the Jarosz scale, exhibited the most degenerated discs according to the Pfirrmann classification, demonstrated more MC, and had more severe endplate defects.
There are several explanations for this. First, patients with degenerative stenosis were significantly older than their peers in the other groups, which is consistent with more severe degenerative changes in the lumbar spine, as demonstrated above. Secondly, spinal stenosis develops as part of global segmental degeneration rather than in isolation. 30 Finally, factors contributing to degenerative lumbar stenosis,31,32 disc degeneration, 33 and MC in the lumbar spine 34 are being widely discussed. Some studies provide evidence for common genetic factors of spinal degeneration. 35 This genetic overlap may explain the observed co-existence of these factors.
We showed that MRI findings (disc degeneration grades, endplate defects, and MC) did not have significant effects on LBP intensity or its attenuation after the procedure – all effects were weak. The studies examining the associations between degenerative findings on MRI and clinical symptoms are highly heterogeneous in terms of design. According to population-based cohort studies (n = 3369 6, n = 382 7), degenerative findings on MRI (disc degeneration, MC, etc.) show either small or no association with current or future LBP intensity. The second Wakayama Spine Study found an association between LBP, MC type 1 (n = 814) 15 and the combination of disc degeneration and endplate signal change (n = 975). 36 Disc degeneration showed the strongest correlation with LBP intensity in patients with non-specific LBP (n = 246); however, the association was weak (the maximum correlation coefficient of (0.22). 37 The NORDSTEN trial that included patients with spondylolisthesis and spinal stenosis (n = 437) reported no associations between preoperative MRI findings and LBP. 38
The above-mentioned studies examined population-based cohorts (symptomatic and asymptomatic) or patients with degenerative lumbar disorders after surgery. The majority of these studies indicate that the associations between degenerative findings on MRI and LBP intensity are weak or absent. We, too, state that the association between degenerative findings on MRI and back pain in our sample of patients with failed conservative treatment is questionable. A meta-analysis is required to systematize the results of existing homogeneous studies to obtain unambiguous conclusions.
Regarding smoking and surgical outcomes in DDLS, this association has been confirmed in many studies, including the NORDSTEN trial 38 and the SPORT study. 5 It has been shown that the treatment effect of surgery in smokers is almost 7 times lower than in non-smokers. 19
We showed that smoking in patients with degenerative stenosis was associated with LBP intensity before the procedure (β = 0.307) and with pain attenuation (MCID achievement) after the procedure in the total sample (OR = 1.28) and, particularly, in patients with degenerative stenosis (OR = 2.03). This effect contradicts the literature, 19 and is interesting by itself: smokers have higher pain intensity before and after the procedure, but show meaningful pain attenuation. The initially high pain intensity may limit the treatment effect – the pain may decrease after the procedure, but smokers might not achieve a patient-acceptable symptom state. Pain attenuation is clinically significant and meaningful (MCID achieved); however, whether this reduction is sufficient given the high pain intensity before the procedure and whether smoking patients are satisfied with the outcome, requires further investigation.
The strengths of this study are: (1) a large sample size; (2) focus on the spinal surgeons’ most common patients, who have not been characterized previously; (3) an optimal range of MRI findings and clinical scales. Further studies should include the following: (1) use of some other specific clinical methods (eg, X-ray) for diagnosis of spinal pathology; (2) assessment of MRI parameters and clinical results in a long term, as this knowledge is useful for understanding the patterns of DDLS progression; (3) contrasting MRI findings between smokers and non-smokers. In addition, we used only one MCID value for back NPRS (≥1.2 points) for all patients. The MCID value is highly dependent on the type of surgery, the follow-up time, and specific pathology. Nevertheless, we analyzed all RuDDS patients as a cohort with failed conservative treatment, aiming to identify a universal predictor. This approach may affect the results and limit predictor identification.
Conclusion
Patients with failed conservative treatment for degenerative lumbar disease tend to have more prominent degenerative changes of the lumbar spine, including disc and endplate degeneration, MC, and higher Jarosz scores. The most severe changes were observed in patients with degenerative stenosis, which might be due to their older age, degeneration covering all lumbar spine structures, and common genetic factors underlying different manifestations of the degenerative process. We found that lumbar MRI findings have only limited effect (β < 0.1) on back pain intensity before the intervention and its clinically significant attenuation (MCID achievement) after the procedure. The most pronounced effect on these parameters was associated with smoking, with the maximum magnitude observed in patients with degenerative stenosis (β = 0.307 for back pain intensity before the procedure and β = 0.709, OR = 2.03 for MCID achievement, P < 0.05).
Supplemental Material
Supplemental Material - Lumbar MRI and Back Pain After Failed Conservative Treatment: The RuDDS Study
Supplemental Material for Lumbar MRI and Back Pain After Failed Conservative Treatment: The RuDDS Study by Olga Leonova, Elizaveta Elgaeva, Anna Berdnikova, Yakov Tsepilov, Aleksandr Krutko in Global Spine Journal.
Footnotes
Acknowledgments
The authors thank Alexey Peleganchuk and Ilya Isakov for contributing to the setting of working with Novosibirsk Research Institute of Traumatology and Orthopaedics n.a. Ya.L. Tsivyan. The authors thank Vladimir Filonenko for his help with the translation and correction of this manuscript.
Ethical Approval
The study was performed according to the Helsinki Declaration; the study protocol was approved and supported by the Local Ethical Committee of the Novosibirsk Research Institute of Traumatology and Orthopedics (№034/20 dated 02 Oct 2020) and by the Local Ethical Committee of the Priorov National Medical Research Center of Traumatology and Orthopedics (№1/21 dated 25 Feb 2021).
Informed Consent
All participants provided written informed consent prior to enrolment in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Russian Science Foundation (grant #22-15-20037) and Government of the Novosibirsk region.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.