
Abstract

Keywords
Three of the seven leading causes of disability globally are musculoskeletal in origin, with two involving the spine. 1,2 Disease burden diminishes the quality of our ever-increasing life spans as each year is accompanied by additional debilitating musculoskeletal conditions. Commensurate with its leading role in disability, low back pain is one of the costliest conditions treated annually with indirect and direct costs over $100 billion USD in the United States alone. 3 Current guidelines on the treatment and management of spine disorders are regionally heterogeneous and incomprehensive. Furthermore, a universally accepted and robust model of patient care does not yet exist anywhere in the world.
Technological advancement in recent years has brought intelligent computing to nearly every industry. Although its integration into the current healthcare landscape is notoriously slow, advancements in healthcare technologies are being made at blistering speed. This is especially true in spine care, and in orthopedic and neurological surgery as a whole. The purpose of this editorial is to describe several current healthcare models applied to spine care and their shortcomings. Specific focus will be placed on how artificial intelligence (AI) and other promising cutting-edge technologies will collectively pave the way for a revolutionary personalized-based model designed with the intent to provide precision care, known as—
Current Models in Spine Care
Three popular approaches to healthcare that are relevant to the treatment of spine pathology are the evidence, outcome, and values-based models. The
In practice, these models are not applied to patient care in exclusion, and they have inherent limitations, particularly in their ability to have more personalized or bespoke treatments. Providing care based on previous experiences or outcomes may fail to incorporate unique characteristics inherent to each patient and their condition. The problem may not be the paucity of data, but rather the “lack” of specific techniques applied to achieve the data’s optimal application.
Artificial Intelligence—Why Should We Use It?
One challenge in optimizing the treatment approach of spine disorders is interpreting the many data points that influence individual patient outcomes. For example, two patients may have identical imaging studies but vastly different symptoms and functional capacities, making the information available to physicians difficult for interpretation and interventional planning. For instance, in a review of 33 studies that included over 3,000 individuals, an extremely high prevalence of spine degeneration was found on imaging among asymptomatic individuals despite that radiographic evidence of degeneration is associated with low back pain. 9 Traditional approaches struggle to meaningfully apply the wealth of collected patient data to patient care. How can the spine community leverage this data to create a more precise spine care model that can better personalize treatment? With the power of AI, we can begin to understand the spine through multiple facets as they interact with one another instead of as independent occurrences, unlike how traditional statistics currently addresses the situation. Much confusion regarding the essence and definition of AI looms within the spine community. Often, the term AI in our colloquia is used interchangeably with machine learning (ML) or deep learning (DL). Since AI is an all-encompassing umbrella, which contains a vast array of subjects, most notably, natural language processing (NLP), ML, and DL, it has become important to explicitly delineate these terms as their respective technologies become more integrated into spine care.
Artificial Intelligence—How Is It Defined?
Various definitions of AI have included the evaluation of artificial thought processes, reasoning, and behaviors with respect to human or idealistic performance. 10 According to Arthur Samuel, 11 a pioneer in the field of AI, ML is a branch of AI which is defined as “the field of study that gives computers the ability to learn without being explicitly programmed.” As a subset of AI, the term ML might be intimidating or evoke imagery of various sci-fi movies, but many ML techniques are simple, and used frequently under more familiar names. For instance, linear regression falls under the title of both ML and AI. More broadly, ML consists of various predictive methods, such as regression, classification, and anomaly detection. One step further is DL, a subset of ML, concerned with collections of algorithms that function in a manner that approximate how networks of biological neural cells interlink. Machine learning algorithms are capable of making sense of seemingly stochastic datasets that are challenging for human observers to interpret and so may serve as the perfect tool set to tackle our data challenges.
Applications of Machine Learning
Regression techniques within ML may involve popular predictive algorithms, such as the LASSO or Ridge regression models, which entail an internal penalization to identify the most important independent variables required to predict the dependent outcome. In classification techniques there may be a solution to outcomes wherein the outcome predicted is classified into groups. Additionally, anomaly detection may present unique advantages in datasets for which the result may have a scarce minority class, such as in the case of postoperative complications. To date, the most impactful use of ML in the field of spine research has been the application of artificial neural networks. 12 With origins dating back as early as the 1940s, these artificial structures have now exceeded human performance in many tasks such as image processing and object classification, which employ convolutional neural networks and are the foundation of DL.
As early as 1988, a perceptron, a simple shallow artificial neural network, demonstrated the ability to diagnose low back pain into four categories with higher accuracy than physicians by using the inputs of symptoms and medical history. 13 In 2010, a support vector machine showed proficiency in classifying scoliotic curves based on radiographs. 14 Several studies have sought to leverage ML models to predict perioperative complications such as cardiac decompensation, need for blood transfusion, and wound infection with mixed results. 12 Others have focused on outcomes of spine surgery. For example, McGirt et al 15 performed linear regression with Bayesian model averaging to predict the Oswestry Disability Index at one year with score accuracies that varied from 72% to 84%. Belykh et al 16 predicted the likelihood of reherniation following a microdiscectomy at a single institute with relative success. Another application of ML modeling is to develop novel scoring methods that assess the risk of having a particular pathology. Goldschmidt et al 17 used 2 regression models, one with cervical and one with lumbar radiographic data, to develop scoring scales that assess risk of sagittal imbalance with strong results.
Existing ML-based decision support tools (DSTs) have been implemented in dermatology and radiology to enhance clinical decision-making by leveraging the predictive power of ML models to personalize care. Neural networks have been used in the development of computer-aided detection systems for analysis of radiographic data to assess spine disorders, such as pathological curvatures, vertebral fractures and intervertebral disc degeneration. 12 Current developments in DSTs are focused on surgical treatment, conservative care and prediction of intervention for low back pain. 12 Given the wide impact that ML has generated across many fields, it is evident that spine specialists are awaiting ML to intelligently personalize their clinical practices.
Applications of Deep Learning
Artificial intelligence techniques are increasingly used in several fields, such as object detection in images and videos, speech recognition, autonomous driving, and natural language processing. In particular, DL, which is typically based on artificial neural networks with multiple layers of processing units, is emerging as the most promising branch of AI for complex tasks such as medical image processing. 18 Its main advantage with respect to other ML techniques is the capability of learning independent variable importance solely from data, without the need for manual engineering and selection of independent variables. 19 Some years ago, scientists proved that DL can achieve superhuman performance in object recognition and image classification. 20 Current technologies widely exceed human results in several applications, 21 and the future promises an even brighter outlook.
Although the actual impact of DL on spine imaging is still rather low, some scientific studies are available in the literature. Scientists from the University of Oxford have reported on the automated extraction and classification of degenerative features in lumbar magnetic resonance imaging (MRI) scans, such as disc degeneration grading, disc narrowing, 22,23 endplate alteration, 24 localization of the so-called “evidence hotspots” which justify the model predictions, as well as automated localization and segmentation of intervertebral discs in 3-dimensional datasets. 25 Others have described ML methods for the evaluation of the severity of scoliosis on multi-planar x-ray projections 26,27 and to classify the pattern of curvature of adolescent scoliotic patients. 28
Companies providing imaging services, mostly consisting of supporting the imaging tasks in clinical trials, showed a limited interest in the use of DL methods in Neuroradiology so far. Well-known companies active in the spine field such as Medical Metrics, Inc. (Houston, TX, USA) and Raylytic GmbH (Leipzig, Germany) mostly focus on the quantification of motion and use non-AI methods. Mirada Medical Ltd. (Oxford, UK) is involved in the research carried out at the University of Oxford, but does not yet offer any commercial service that concerns the spine. A number of companies propose, among others, a few DL algorithms addressing specific clinical questions related to the spine. For example, Aidoc (Tel Aviv-Yafo, Israel) developed a DL-based product which includes the detection of bone hypodense findings in the cervical spine. Zebra Medical (Shefayim, Israel) offers a product which predicts the risk of osteoporotic fracture from existing spine CT datasets. Optasia Medical (Cheadle, UK) offers a commercial service for the analysis of osteoporotic vertebral collapse in sagittal x-rays and dual-energy X-ray absorptiometry (DXA) lateral scans.
Regarding medical image analysis, DL is increasingly used for a number of tasks, including detection of anatomical and pathological structures, image segmentation and computer-aided diagnosis. 19 Specific current clinical applications of DL include detecting mitosis 29 and cells 30 in breast cancer histological images, segmenting infant brain MRI scans to diagnose developmental anomalies, 31,32 classifying pulmonary nodules 33,34 and supporting the diagnosis of Alzheimer disease. 35 With respect to other research fields, medical imaging studies are typically characterized by a lower availability of data, in the range of hundreds or few thousands instead of millions of images, which poses technical challenges currently subject to intense research.
For the past 20 years, the spine field has seen a surge in studies addressing human genetics and the ability to identify millions of individual single nucleotide polymorphisms in relation to various imaging and/or clinical phenotypes. 36 -49 In fact, we have been witnesses to the rise of transcriptomics, proteomics, microbiome, metabolomics and a plethora of other big data “omics” platforms along with their applications toward spine disease. Even the phenotyping of disc cells and other spinal structures, the exponential rise of molecular and biomarker epidemiology, and motion kinematic and analyses further lend to multidimensional big data considerations and integration between different disciplines. 50 -54 Oftentimes the challenge is to find meaningful results that can be replicated in other cohorts and ethnic populations. How such data is interlinked, interacts with each other and is further related to imaging and other clinical parameters goes beyond a basic statistical undertaking and beckons much more complex analytical processing.
Natural Language Processing
Natural language processing (NLP), also known as neuro-linguistic programming, is a computational technique at the intersection of AI, theoretical computer science, and human language, involved in translating unstructured data into a structured format (i.e. human communication and language into numbers for computation). This is a method by which textual information may be chiseled into meaningful data. Broadly, NLP has been used to produce automated chat bots, speech recognition software, machine translation of human languages for communication, and much more. Examples of such algorithms include Amazon’s Alexa, Grammarly spell checking, or targeted advertisements based on one’s search history. More specifically, numerous applications of such techniques have been observed in orthopedic and neurological spine surgery research. Ehresman et al 55 employed NLP algorithms to extract patient data information to identify incidental durotomies through the review of free-text operative notes. Karhade et al 56 proved that NLP may offer entities such as national spine registries and hospital quality and safety departments automated tracking of such incidental durotomies with extreme accuracy.
The applications of NLP go beyond identification of durotomies in operative notes. Natural language processing has been used to identify clinical notes involving wound infection that required reoperation after lumbar discectomy, allowing for the accurate automation of such reporting. 57 These studies offer a glimpse into the possible applications. Such techniques may improve the efficacy of data collection and reporting considering the use of a single algorithm in lieu of manual extraction by multiple individuals for which variability may result.
Augmented, Mixed and Virtual Reality
Advancement in computing power and miniaturizing of key hardware components has led to significant advancement of virtual reality (VR), augmented reality (AR) and mixed reality (MR) systems. Virtual reality is a computer generated environment where the user is fully immersed into an artificial world. This is accomplished by having the user wear a head mounted display along with haptic feedback devices that allow the user to interact in the artificial environment. Augmented reality is different from VR in that it does not create a new artificial environment. It is an additional layer of computer generated imagery or information onto a real world environment. This additional layer supplements or augments the user’s real world environment. Mixed reality is an interplay of both virtual and real world environment, and allows the user to interact and manipulate components within the virtual and real world simultaneously. In spine surgery, VR has been employed in the education and guidance of trainees for pedicle screw fixation, showing increased accuracy in comparison to traditional teaching methods. 58,59 Further, AR has been used in spine surgery for surgical navigation, most commonly when performing pedicle screw placement. Studies have shown that AR was helpful in surgical navigation with high accuracy of pedicle screw placement. 60 The first AR surgical navigation system has received FDA clearance for spine surgery and has been used recently in posterior lumbar decompression and fixation surgery.
In terms of patient care, VR has been used as a distraction to attenuate pain, known as “VR Analgesia.” Patients have reported decreased subjective pain scores using VR. These findings were corroborated by functional MRI studies showing decreased brain activity in areas activated during thermal pain stimulation. 61 The concept of VR analgesia has been applied in different ways including attenuating procedural pain in children 62 and increasing range of motion and decreasing pain scores during physical therapy in adults. 63,64
Technological enhancements have led to wider access and adoption of VR and AR in general society. These systems have been used in medical training as well as in patient care. While promising, the technology is nascent, and studies are limited. Further robust studies will be needed for wider adoption of these modalities.
3D Image-Based Phenotyping, Segmentation and Printing
A natural extension to planar imaging is the development of 3D visualization modalities, including the ones described in the previous paragraph (see section
For the longest time, ironically, the most important limiting factor for adopting 3D clinical diagnostics has been the widely available planar radiograph. In historical terms, it can be said that the radiograph provided the earliest version of an image-based phenotype. Spinal features like the Cobb angle, disc height, disc grade classification (MRI-based) or spinal rotation in scoliosis cases (CT-based) are image-based phenotypes that provide clinicians and researchers with important information for basing treatment and advancing the field. 50,65,66 In fact, 3D classification-based systems for spine pathologies are starting to gain traction and may be more commonplace 67,68 as the technology becomes available and the understanding of their clinical relevance is robustly substantiated and superior to the traditional 2D. Since in the past the 2D perspective has yielded speculation as to its clinical relevance and actual utility, the 3D perspective can perhaps shed more robust understanding as to any association, prognostic, or targeted diagnostic assessment of structural spinal phenotypes in relation to the pain/function/disability profile. 69,70
While commonplace and low-cost, the x-ray does not serve the purpose of describing the 3D geometries of the spine and its components (or any other musculoskeletal structure, for that matter). By describing 3D data in 3D, more accurate research and clinical results are possible. The field is advancing in this direction with visualization techniques that, besides being immersive, are disruptive because they provide a tangible object for the clinician.
71
Instead of relying on planar images on a screen, these subject-specific models can be used for additive manufacturing (also known as 3D printing) of surgical guides, anatomical models or serial-replication of research-oriented models (i.e. printing rare cases or conditions for teaching, patient education, or laboratory research),
72
as well as computational analyses such as finite element analysis (FEA; see section
Besides a well-regulated practice of additive manufacturing, be it at the point-of-care or outsourced to a printing-service bureau, the issue of cost is always what drives the introduction and adoption of any new product to market. This is being addressed by other medical AM entities like the Radiological Society of North America (RSNA) and the American Medical Association (AMA). In fact, on July 1, 2019, the RSNA and AMA entered into an agreement to implement temporary current procedural terminology (CPT) codes 76 that enable reimbursement of 3D printed and segmented products. In a further boost to usage implementation, the American College of Radiology (ACR) and the RSNA have developed a registry to capture 3D printed and segmented product usage with the impetus of keeping the momentum toward full reimbursement. This impulse is shared by the U.S. Centers for Medicare and Medicaid Services (CMS), where plans to reimburse two of these codes motivate its use in a wider population.
The fact is that segmentation has opened new ways to analyze, diagnose and study subject-specific data and has contributed vastly to the improvement of diagnostics by creating new avenues to look at the spine. A vast majority of these new metrics need to be validated and used clinically to prove their utility as 3D image-based phenotyping. With the advent of additive manufacturing in medicine, new regulations and standards are needed to ensure the safety of 3D-printed implants, especially with respect to the implant alloy’s microstructure, residual impurities, and micro-porosities. There are on-going efforts by the Food and Drug Administration 77,78 and the ASTM/ISO in developing standards 79 for additive manufacturing worldwide. 80
Robotics and Surgical Planning
Technical advancements have led to the growth and adoption of surgical robotics and robotic-assisted spine surgery. In its current state, surgical robotics are highly reliant on perioperative surgical planning, radiographic imaging and stereotactic instrumentation with the goal of optimizing accuracy and efficiency. 81 Additional potential advantages include the inherent indefatigability associated with robotic systems and limiting radiation exposure associated with commonly performed spinal procedures. Clinically, these technologies may assist in producing consistent, reproducible outcomes that eliminate human error, though, comparison with manual techniques has revealed mixed results. 82,83
Integration of AI and ML to surgical robotics may be the next major development in this field. Artificial intelligence is already being harnessed for surgical planning and image processing, both of which are critical to robotic surgery. 84 At its core, robotic systems consist of three major components: sensors, end effectors, and a control matrix that synthesizes applied data into action. 85 Machine learning has the potential to augment the interaction between the robot, its environment, and the surgeon, whereby the ML augmentation is used to continuously analyze the data generated by the environment so that the robotic system learns from its own experience. This reinforcement learning would allow the system to potentiate good outcomes while avoiding negative outcomes through its feedback system. 86
Currently, robotic technology has been limited to robotic-assisted surgery using a human-controlled model rather than completely autonomous robotic surgery. The primary use of robotic-assisted spine surgery has been pedicle screw instrumentation, though its application for pelvic fixation and spine tumor surgery has also been described. 87 The indications for robotic-assisted spine surgery will likely continue to grow with advancements in imaging and navigation technology allowing for its application in surgical decompression and more complex procedures. With the incorporation of AI and ML platforms, this technology will also improve preoperative planning based on data analytics and image processing. Furthermore, the complex processing capabilities provided by AI could provide immediate feedback that not only allows for real time analysis, but anticipates dynamic changes intraoperatively. 88 While the transition to completely autonomous robotic spine surgery is unlikely in the near future, AI and ML can be used to negotiate continuous feedback between the human operator and machine with the goal of improved performance and clinical outcomes.
Sensors, Wearables and Remote Patient Monitoring
Remote patient monitoring (RPM) technology allows patients and physicians access to real-time data collected from wearable or implantable devices. 89 While physicians traditionally could only monitor and treat patients who were physically situated in healthcare facilities, RPM technologies have shifted this paradigm to allow for real-time data collection and feedback between patients and physicians regardless of patient location. Patient-generated data can now be uploaded to secure online platforms to be accessed in user-friendly formats by patients and their medical teams, allowing feedback systems to alert patients in real time about critical results. These platforms are transforming the care of medical conditions, such as diabetes and congestive heart failure, and more recently have found their way into orthopedic and spine care settings as well.
Smart implants have been designed for use and implantation in the spine. Rods connected to strain gauges have been used for decades to determine the amount of force across spine fixation constructs. 90 Sensor technology can now provide intraoperative data regarding rod strain during reconstructive spinal procedures, and technology currently being developed could build off this and potentially be implanted to provide this data post-operatively as well. Smart implants have also been designed to monitor load across segments. 91 Further iterations of these technologies may help determine if and when fusion occurs at operated levels, or better understand the load and wear dynamics of disc arthroplasties.
Cameras and gait analysis platforms have described patterns of gait dysfunction caused by conditions such as myelopathy. 92 Smart fabrics and shoes as well as other wearable devices using a variety of sensors such as accelerometers, gyroscopes, strain gauges and electrogoniometers, can further be used to collect real-time data to help monitor and manage patients remotely. Studies have used such technologies to track patients after spine surgery or after spinal cord injury to monitor rehabilitation progress. 93 Other devices have been developed to monitor posture and provide feedback when poor posture is encountered in hopes of decreasing injuries and promoting improved overall spine health, although these remote monitoring technologies have shown inconclusive results thus far. 94 Sensors have also been incorporated into braces used to treat children with scoliosis. 95,96 These allow remote monitoring of brace wear which, combined with physician feedback to patients about these results, can lead to improved compliance with bracing, which in turn can decrease curve progression in children with scoliosis.
In recent years, consumer wearables and sensors (i.e. smart phones and watches) have been highly promoted as a means to improve health and modulate physical activity. Data collected from wearables is not entirely reliable, accuracy varies between manufacturers, 97 and the devices themselves have not demonstrated a meaningful impact on health care outcomes. 98 This is not to say consumer wearables are without the potential for clinical utility, as the Apple Watch has been shown to accurately detect paroxysmal atrial fibrillation. 99 Wearable devices can also accurately assess sleep. 100 As there is a link between quality of sleep and pain, 101 including low back pain, if these devices positively influence sleep patterns, they may be useful in the management of such pain. The use of wearables by patients as a means of improving wellness has been advocated by healthcare entities. 102 Apple recently announced a healthcare initiative in partnership with the government of Singapore called LumiHealth that is designed to leverage the Apple Watch platform to encourage Singaporeans to adopt healthy habits. Efforts are being made to integrate consumable wearable technology meaningfully into healthcare infrastructure, and it may only be a matter of time before their effects are felt in upon the musculoskeletal community.
Computational Modeling
“Toward patient-specific modeling” is a frequent phrase found in the titles of scientific literature. In the past, limitations of computer power, time-intensive manual modeling procedures for patient-specific anatomy, limited resolution of clinical images, and the need for detailed characterization of material properties have limited the full application of patient-specific computational models. Today, advances in computational power and techniques are beginning to provide personalized predictions of patient reaction to implants, surgical procedures, and nonsurgical interventions, albeit only for a few patients to date. Computational modeling techniques, such as FEA have advanced to the point where we are close to the ability to virtually simulate interventions and predict the effect of surgery or non-surgical treatment on joint mechanics and biological behavior for large numbers of patients—all in an automated matter.
Much of the spine literature on patient-specific computational models for clinical decision making involve scoliosis treatment. Almost two decades ago, Gréalou et al 103 generated patient specific FEA models of the spine and rib cage to understand how costoplasty could help correct spinal scoliotic deformities. 103 More recently, patient specific FEA has been used to determine the best point of force application for brace design to correct scoliotic deformity. 104 Another tool was developed to monitor and plan treatments for adolescent idiopathic scoliosis on a web-based platform to facilitate collaborative clinical decision-making. 105 The intent was to provide a web-based approach to monitoring curvature change while minimizing the number of radiographs required and exposure to ionizing radiation. Computational models could also be used to monitor and guide future surgeries, as investigated by Jayaswal et al 106 for juvenile scoliosis patients. Partial curve correction surgery is performed with growing rods, followed by a series of lengthening surgeries to correct spinal curvature while allowing longitudinal growth of the spine. 107 -111 A patient-specific model of the juvenile scoliotic spine for the thoracic region was used to provide personalized distraction intervals that would avoid fracture of growth rods.
One barrier to using sophisticated FEA models as pre-clinical planning tools is the need for automatic mesh generation in highly complex structures, such as the spine. Researchers have developed sophisticated tools to ease the development of high quality hexahedral meshes. 112 Extensions of this work include virtual surgeries and treatment planning. Zhang et al 113 are developing an integrated computer aided design-FEA workflow for designing patient-specific spinal cages. The intent is that patient specific FEA can help determine the design of spinal cages that provide the most ideal mechanical environment to the system. The method of combining computer aided design and FEA decreases the amount of time it takes to create and evaluate a model and run multiple design iterations.
Finally, the newest techniques combine traditional FEA with mechanobiology to predict mechanical and biological outcomes. Van Rijsbergen et al 114 developed a model to predict if patients will have adjacent segment disc degeneration and bone remodeling after spinal fusion. In this case, patient-specific computational models require not only detailed patient geometry, but predictive rules for bone remodeling and biochemical disc responses. This moves toward predicting which patients are good candidates for spinal fusion versus those at high risk for adjacent segment degeneration. As techniques for automating model generation continue to improve, and theoretical models governing bone adaptation and biochemical responses become more sophisticated, patient-specific computational modeling will be one more tool that the clinician has in his/her arsenal to help with decision making.
Intelligence-Based Spine Care Model
Coupled with the expanded understanding of imaging and clinical phenotypes toward a more precision-based approach for managing spine patients, the multidimensionality of data-driven results and analytics become exponentially more complex. However, with the use of AI, ML, and DL platforms and the innate capacity of bioinformatics, the onus for quick, reliable diagnostics, clinical decision-making, risk profiling, patient stratification and predictive modeling in more unbiased dimensions seems to have ushered in the era of an
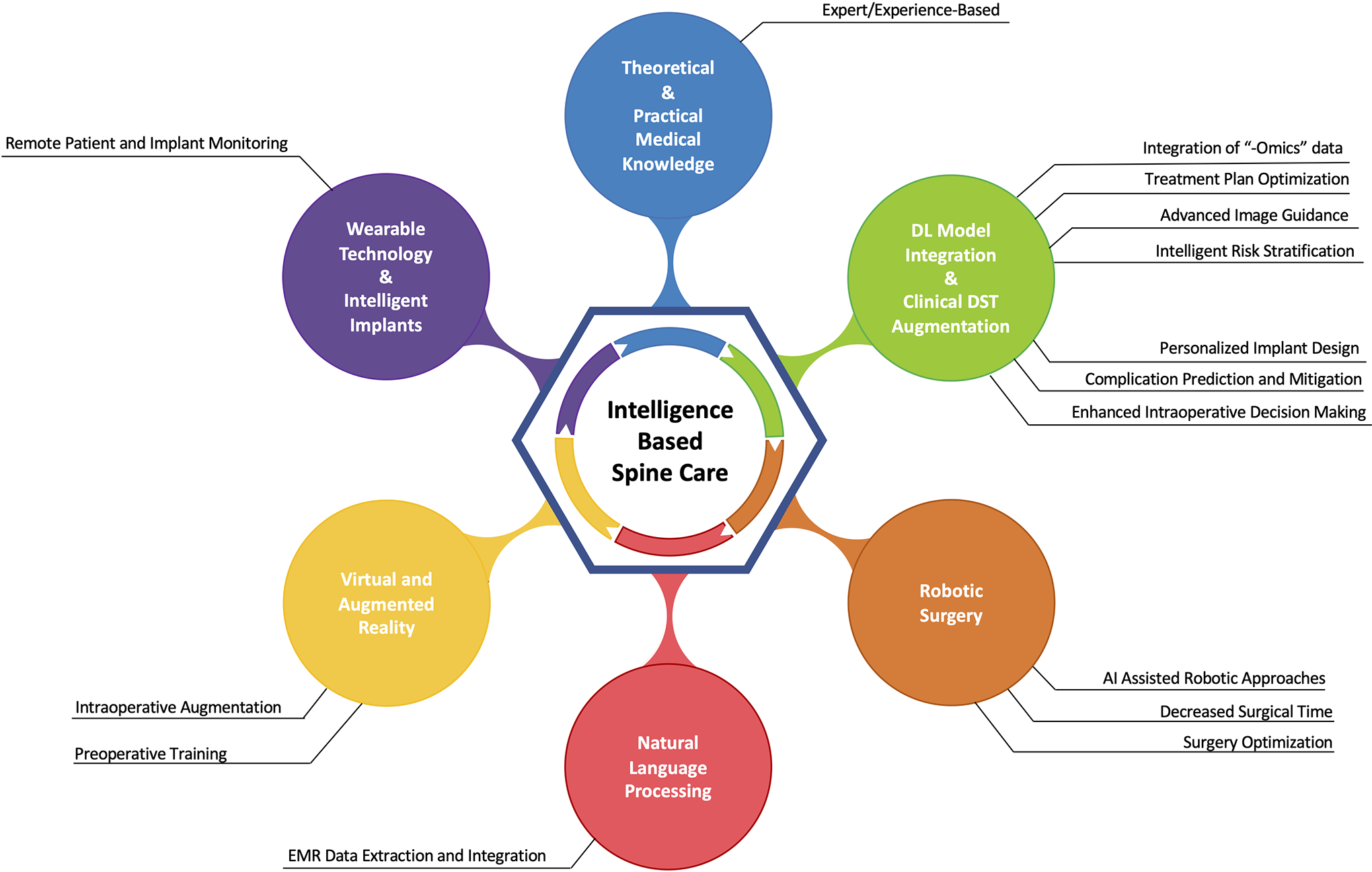
The intelligence-based spine care model. DL: deep learning; DST: decision support tools; EMR: electronic medical record.
Although IBSC appears attractive, additional studies are needed to assess the true efficacy of this model as well as the short and long-term costs of integrating advanced technologies into spine care. The infrastructure to support large-scale data-generating, merging, and sharing initiatives in the spine community is needed for various pathologies. Multidisciplinary collaborations are essential to provide training sets that may validate and refine various analytical models. Global initiatives are needed to assess ethnic variations and similarities that will further inform modeling. That said, spine clinicians need to become more familiar with such modeling techniques to make an informed decision for patient care in the emerging era of artificial intelligence.
In the near future, IBSC may use data from a patient’s smart apparel, intelligent implants, and electronic medical records to build a unique data profile, or fingerprint, that’s immediately actionable in the clinic. All known data about the patient, from the number of steps they take each day to the trends of their annual blood work are factored in. Intelligence-based spine care surgeries may be augmented by real-time DSTs that leverage a patient’s data fingerprint to more robustly consult patients, address expectations, and enhance perioperative decision-making, while also warning physicians of what to expect in the way of postoperative complications. The algorithms of IBSC may generate optimal tailor-made implants, and surgeons may be able to train preoperatively on VR and AR assisted robotic systems before installation. As patients progress through treatment, their IBSC management plan continuously adapts to new data to fit their specific needs to consequently maximize outcomes and reduce costs at every step of the way.
Conclusions
The building blocks of the IBSC model are currently being developed and perfected, and several have already brought technological innovation to other specialties. It’s not a question of “if,” but “when” AI will meaningfully connect these platforms to form a coherent IBSC that will, with the utmost precision, guide the treatment of various spine pathologies. However, before a recognizable IBSC model can take shape, research needs to be directed at integrating the various components of the IBSC model, and ML and DL models need to be validated across global regions to ensure efficacy across ethnically diverse populations. Moreover, data sharing and access to large datasets that promote collaboration and consortia need to be established. Additionally, a framework for maintaining and retraining models needs to be instituted to avoid model drift, or the degradation of prediction accuracy over time, as the mapping of historical observations to future outcomes is not static. As these challenges are surmounted and each platform interlinked, the IBSC model is sure to one day be highly impactful in the world of spine care, possibly even reducing years spent living with debilitating spine disorders and minimizing the financial burden that such conditions have on our healthcare systems.