
Abstract
Study Design
Comparative Study.
Objectives
The purpose of this study is to utilize the 2021 Global Burden of Disease (GBD) database to analyze the epidemiology of Spinal Cord Injury (SCI) and assess its burden globally and in America, China, and India from 1990 to 2021.
Methods
Data on SCI incidence and Years Lived with Disability (YLDs) from 1990 to 2021 for the worldwild, America, China, and India were downloaded from the GBD database. Analytical methods including Joinpoint modeling, Bayesian Average Annual Percentage Change (BAPC) modeling, and decomposition analysis were applied to process the data.
Results
In 2021, the global incidence number of SCI was 574 502, with contributions from China (17.3%), India (15.57%), and America (7.9%). Based on YLDs number, the global burden of SCI was 4 566 237, with contributions from China (16.47%), India (13.22%), and America (6.79%). Women reached their peak SCI incidence number at older ages than men, although men had a higher overall burden. The Joinpoint model indicated that from 1990 to 2021, the AAPC of the SCI burden was negative globally, in America, China, and India, but China’s ASIR did not show a statistically significant change (95% CI included 0). Predictions from BAPC models suggest that global SCI ASIR and ASYR will continue to decline. Decomposition analysis indicates that population aging and size are major contributors to the increased SCI burden, while epidemiological changes mitigate its growth.
Conclusion
Nations need to design tailored public health policies to prevent SCI, enhance health management, and mitigate the alarming trends of SCI epidemiology according to their unique contexts.
Introduction
Spinal cord injury (SCI) represents a significant global health challenge, affecting not only patients’ physical function but also their mental health, social integration, and economic status. 1 The etiology of SCI is multifaceted, divided broadly into traumatic and non-traumatic categories. Traumatic SCI is commonly caused by high-energy events, including road accidents, Falls, sports-related injuries, and violent acts such as gunshot wounds or stabbings. Non-traumatic SCI may arise from conditions such as infections (eg, myelitis), tumors, spinal degenerative disorders, ischemia-reperfusion injury, or vascular abnormalities.2,3 These injuries may result in profound functional impairments, such as paraplegia, quadriplegia, bowel and bladder dysfunction, chronic pain, and autonomic nervous system dysfunction.4,5 Although progress has been made in SCI treatments, such as decompression surgery to reduce spinal cord pressure and medications to improve mean arterial pressure (MAP) against ischemia, there is currently no definitive cure. 6 Many patients survive the acute phase but suffer from long-term disability and diminished quality of life, particularly in low-resource settings where SCI care and rehabilitation remain challenging. 2
The Global Burden of Disease (GBD) initiative offers essential data for understanding and assessing the impact of SCI. GBD data reveals that in 2019, there were 20.6 million global SCI cases, marking a notable rise in prevalence and incidence since 1990. 7 The economic impact of SCI is especially significant in developed nations. In America, the yearly direct economic cost of SCI is estimated to exceed $9.7 billion, 8 with around 17 000 new cases annually, and lifetime treatment costs per patient ranging from $1.1 to $4.7 million. 9 In China, the average hospitalization cost for a patient with traumatic SCI is $11,500, with an average daily cost of $700. 10 These figures highlight the substantial socioeconomic burden imposed by SCI.
The GBD database, created by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, serves as a global health resource, offering reliable evidence for policymakers, public health professionals, researchers, and NGOs by collecting, analyzing, and modeling diverse epidemiological data. 11 The database is essential for comprehending the burden of diseases and their impacts, aiding in the development of health policies, resource distribution, and prevention strategies.
Using the GBD2021 database, this study evaluates the epidemiological characteristics of SCI in China, India, and America, representing three diverse contexts, and explores global trends. The selection of these three countries was based on their substantial differences in population scale, economic development levels, healthcare systems, and cultural and lifestyle characteristics. Furthermore, these countries exhibit significant diversity in the etiology of SCI. For example, in America, SCI is predominantly caused by traffic accidents and firearm injuries, whereas in China and India, it is often linked to labor-related high-energy trauma and insufficient workplace safety measures. 12 The comparison of SCI burden in these three countries helps uncover the epidemiological traits within varying socioeconomic contexts, offering key insights for public health policies, medical research, and global disease control strategies. This comparative analysis offers valuable guidance for enhancing the quality of life of SCI patients, improving resource distribution, and fostering international collaboration in health initiatives.
Methods
The data used in this study are sourced from the Global Burden of Disease database, which provides open access to disease burden data. Therefore, informed consent is not required for this study.
Data Sources
This study utilized the Global Health Data Exchange (GHDx) online query tool (https://ghdx.healthdata.org/gbd–results–tool) to extract SCI-related disease burden data from 204 countries globally between 1990 and 2021. The guidelines provided by the GBD 2021 study served as a scientific basis for data extraction and analysis, including data on SCI-related incidence, Years Lived with Disability (YLDs), and age-standardized rates (ASR). We downloaded and analyzed SCI data from four key regions: “Global,” “China,” “America,” and “India,” and further explored the epidemiological characteristics of SCI based on gender and age classifications. In the GBD database, SCI is categorized under the Level 1 cause “Injury,” which is further divided into three Level 2 causes: “Transport Injuries,” “Unintentional Injuries,” and “Self-harm and Interpersonal Violence.” Level 3 causes are further refined into 16 specific categories (Figure 2). This study systematically analyzed the trends in SCI burden and changes in its causal structure globally and in specific regions (China, America, and India) from 1990 to 2021 to better understand the primary factors influencing the SCI burden.
Statistical Analysis
To describe the epidemiology and disease burden of SCI, we used the number of incidence, age-standardized incidence rate (ASIR), number of YLDs, and age-standardized YLDs rate (ASYR). GBD 2021 utilized the DisMod-MR 2.1 statistical modeling tool to standardize global population and epidemiological data, with a 95% uncertainty interval (UI) to ensure the scientific rigor and consistency of estimates. In this study, Joinpoint regression analysis was employed to calculate the Annual Percentage Change (APC) and Average Annual Percent Change (AAPC) over the entire study period, along with their corresponding 95% confidence intervals (CI). Trends were determined based on the estimated AAPC and its 95% CI. If the AAPC estimate and its lower CI bound were greater than 0, it indicated a significant increasing trend; if the AAPC estimate and its upper CI bound were less than 0, it indicated a significant decreasing trend. If neither condition was met, it was considered that the ASR showed no significant change over time. To predict the disease burden of SCI from 2022 to 2035, we extended the APC model using Bayesian statistical methods (BAPC). The BAPC model integrates historical data patterns, uncertainty factors, and prior knowledge to improve prediction accuracy and robustness, effectively handling noise and ambiguities in the data. To more precisely assess the contributions of various factors to the SCI disease burden, decomposition analysis was applied, dividing the burden into three effects: aging effect, population size effect, and epidemiological effect. All data processing and analysis were conducted using R 4.4.1 software. During statistical calculations, strict attention was paid to data quality control and uncertainty assessment to ensure the scientific rigor and reproducibility of the results.
Results
Global Burden of SCI
According to GBD 2021 data, SCI poses a significant burden worldwide, with China, India, and America standing out. In 2021, the global incidence number of SCI reached 574 502 (440 219-757,445). Among 204 countries and regions, China ranked first with 99 363 (72 456-136,733), accounting for 17.3% of the global total; India followed with 89 419 (65 899-124,877), representing 15.57%; and America ranked third with 45 392 (33 651-62,224), accounting for 7.9% (Figure 1A). These figures demonstrate that SCI represents a substantial public health challenge in these three countries. Global Distribution of SCI Burden in 2021.(A) Incidence Number of SCI. (B) ASIR of SCI. (C) YLDs Number of SCI. (D) ASYR of SCI. YLDs, Years Lived With Disability; ASIR, Age-Standardized Incidence Rate; ASYR, Age-Standardized YLDs Rate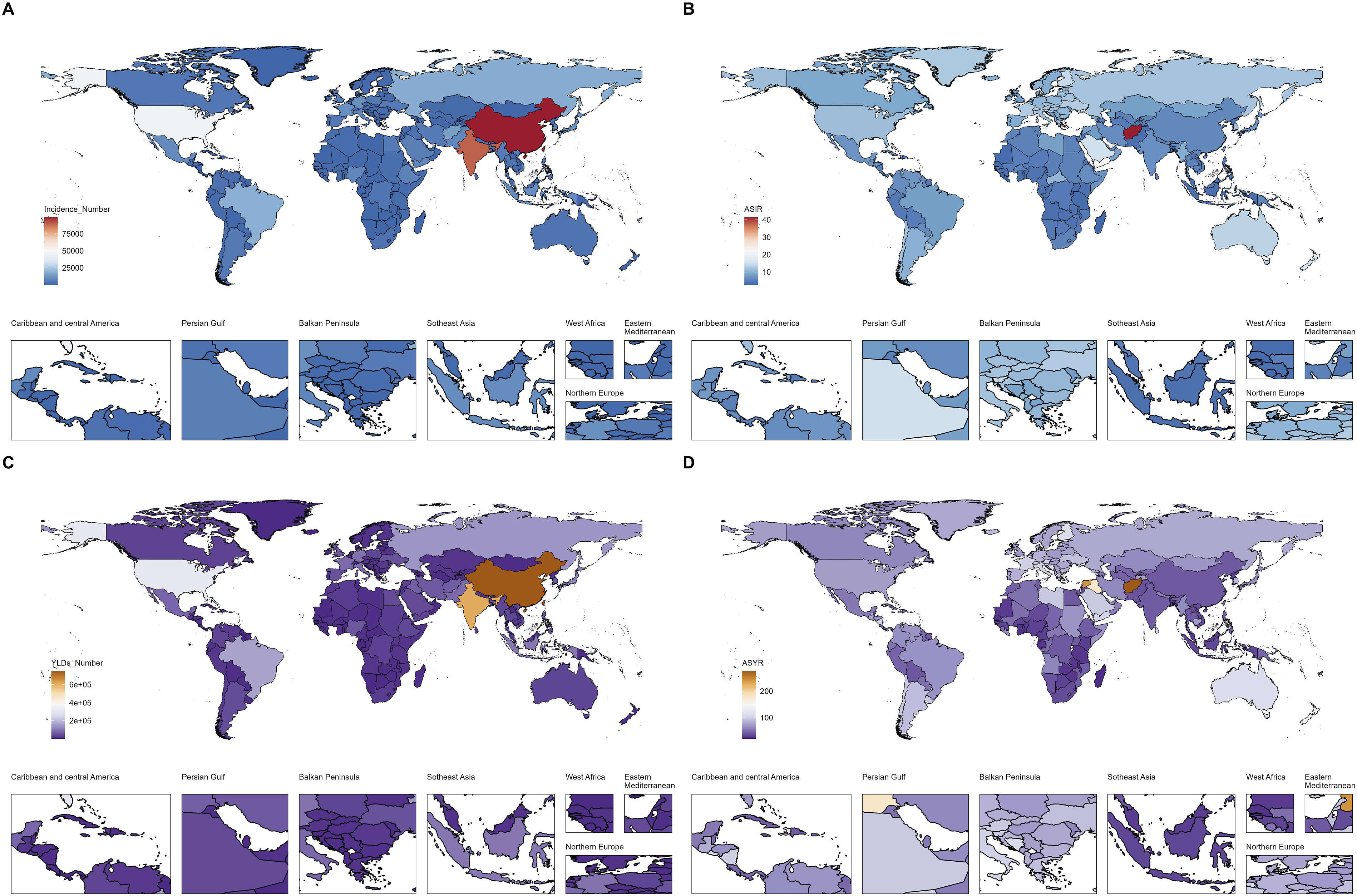
In terms of YLDs number, the global SCI burden in 2021 amounted to 4 566 237 (3 195 694-6,007 036), with China, India, and America showing particularly high burdens. Specifically, YLDs in China were 751 837 (533 035-983,599), accounting for 16.47% of the global total; in India, 603 723 (434 519-780,887), representing 13.22%; and in America, 310 242 (217 833-399,504), accounting for 6.79% (Figure 1C). The high YLDs number in these three countries further emphasize the profound impact of SCI on their healthcare systems and socioeconomic structures.
Analysis of ASIR and ASYR revealed regional differences in SCI burden. Globally, the ASIR was 7.12 (5.48-9.36), and the ASYR was 54.62 (38.2-71.97). Compared to the global average, America exhibited a particularly high burden, with an ASIR of 11.39 (8.88-14.99) and an ASYR of 72.7 (50.56-93.67). In contrast, China’s ASIR was 6.21 (4.65-8.4) and its ASYR was 41.61 (29.28-54.36); India’s ASIR was 6.73 (4.84-9.57), and its ASYR was 42.94 (31.04-55.34) (Figure 1B and D). The ASIR and ASYR in America were significantly higher than those in China and India, indicating a heavier disease burden of SCI in America.
Changes in the Causes of SCI 1990-2021
We analyzed the data for the number of SCI attributed to all level 3 causes in 1990 and 2021 across the globe, America, China, and India. In 1990, Falls were the leading cause of SCI, except in America, where the leading cause of SCI was Road Injuries and Falls were the secondary cause. Road Injuries were the secondary cause globally and in China, while the secondary cause of SCI in India was Conflict and Terrorism. It is still worth noting that, compared with the global ranking of SCI causes, Conflict and Terrorism in America and China were significantly lower in the ranking and were at the last position. In 2021, it was consistent that the top three causes of SCI were Falls, Road Injuries, and Interpersonal Violence, whether in America, China, India, or globally. Compared with the global ranking, it is worth noting that the ranking of Conflict and Terrorism in America and China still remained low, while India had improved in this regard compared with 1990. From 1990 to 2021, the main causes of SCI changed globally and in the key countries. Falls gradually became the main cause, with a significant increase in proportion, especially in India and China. In America, the proportions of Falls and Road Injuries were relatively balanced, but Falls gradually took the dominant position. These findings highlight the different priorities of SCI prevention and management in different countries and emphasize the importance of strengthening interventions against Falls and Road Injuries. (Figure 2). Distribution of Different Causes. (A) Causes’ Distribution of SCI Incidence in 1990. (B) Causes’ Distribution of SCI YLDs in 1990. (C) Causes’ Distribution of SCI Incidence in 2021. (D) Causes’ Distribution of SCI YLDs in 2021. YLDs, Years Lived With Disability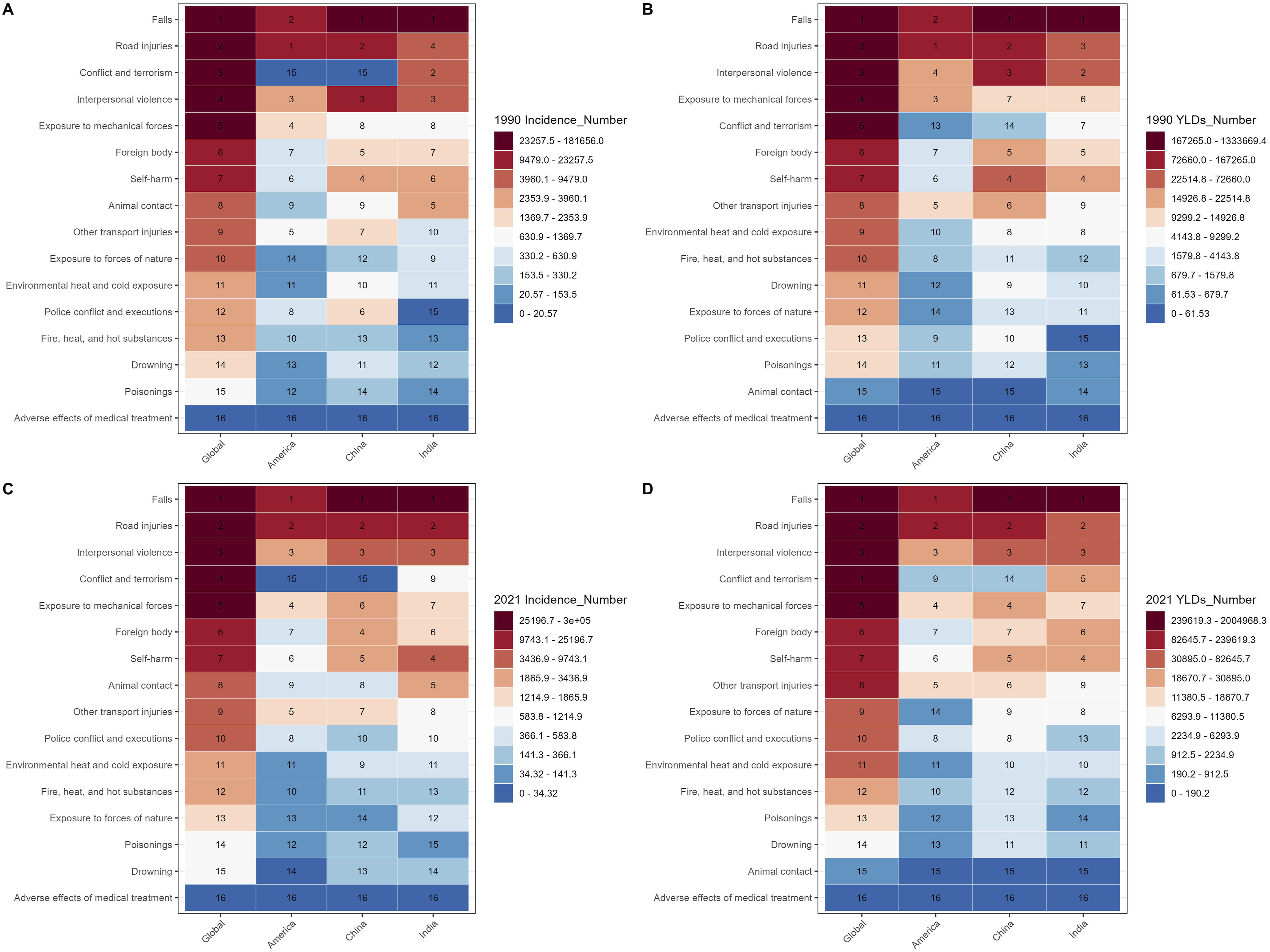
Distribution of SCI Burden Across Different Age Groups in 2021
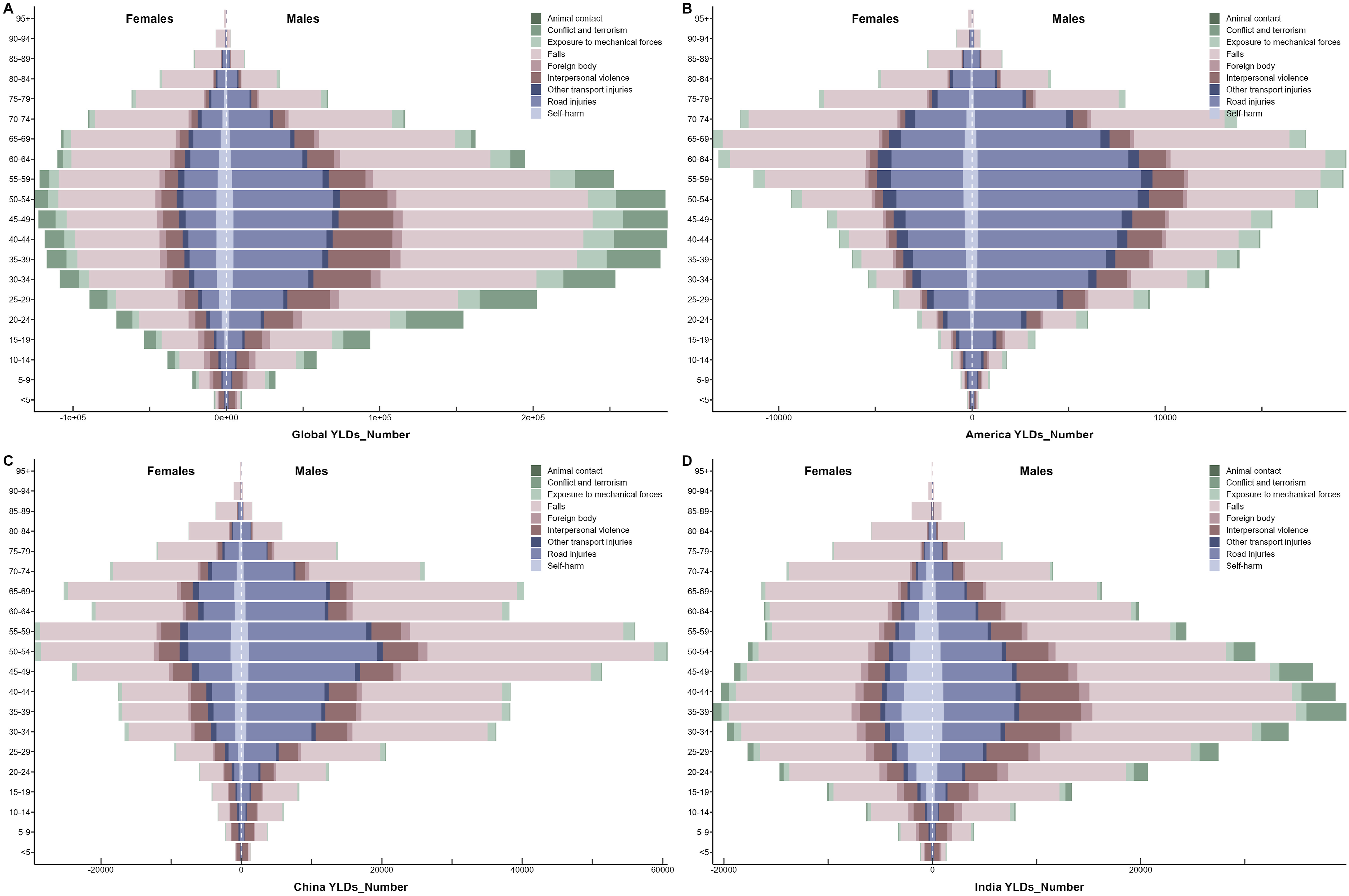
This study examined the differences in the burden of SCI in 2021 across different age groups and genders in the world, China, America, and India, measured by the number of incidence and YLDs. The analysis focused on the top five causes identified in Figures 2C and D, including Falls, Road Injuries, Conflict and Terrorism, Interpersonal Violence, Exposure to Mechanical Forces, Other Transport Injuries, Self-harm, Foreign Body, and Animal Contact.
In terms of incidence, it can be observed that the peak age of incidence in females is generally later than that in males, while globally and in India, the peak age of incidence in males tends to occur earlier (Figure 3). In terms of YLDs, it can be seen that the peak age group in America is higher than the global average for both males and females, the peak age in China is similar to the global average, while the peak age in India is lower than the global average (Figure 4). In terms of causes, it can be found that Falls have the highest proportion of incidence and YLDs across all age groups. For Falls, the peak age in males usually occurs in middle age, while in females, it occurs in old age. Road Injuries rank second in terms of incidence and YLDs. The peak age group of incidence in America is the youngest (Figures 3 and 4). Additionally, some other causes show unique characteristics in specific countries or genders. Globally, Conflict and Terrorism are particularly prominent among males aged 15-19. In India, Animal Contact and Self-harm among females require additional attention. Distribution of Incidence Number Due to SCI From Different Causes in 2021, Stratified by Gender and Age. (A) Globe. (B) The United States. (C) China. (D) India Distribution of YLDs Number Due to SCI From Different Causes in 2021, Stratified by Gender and Age. (A) Globe. (B) The United States. (C) China. (D) India. YLDs, Years Lived With Disability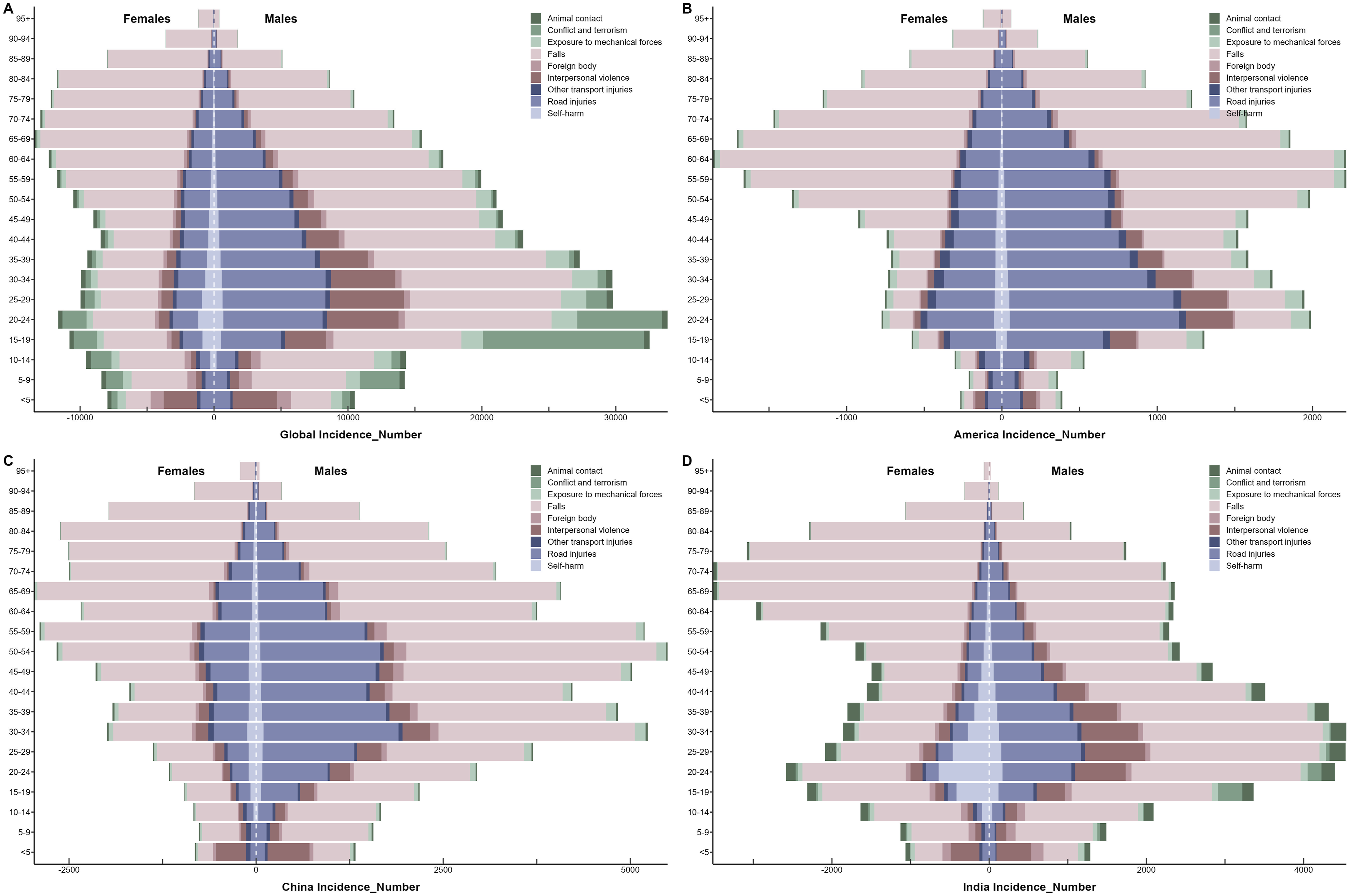
Joinpoint Regression Analysis of the Burden of SCI
AAPC of Incidence and YLDs Due to SCI and Its Causes in Global, America, China and India From 1990 to 2021
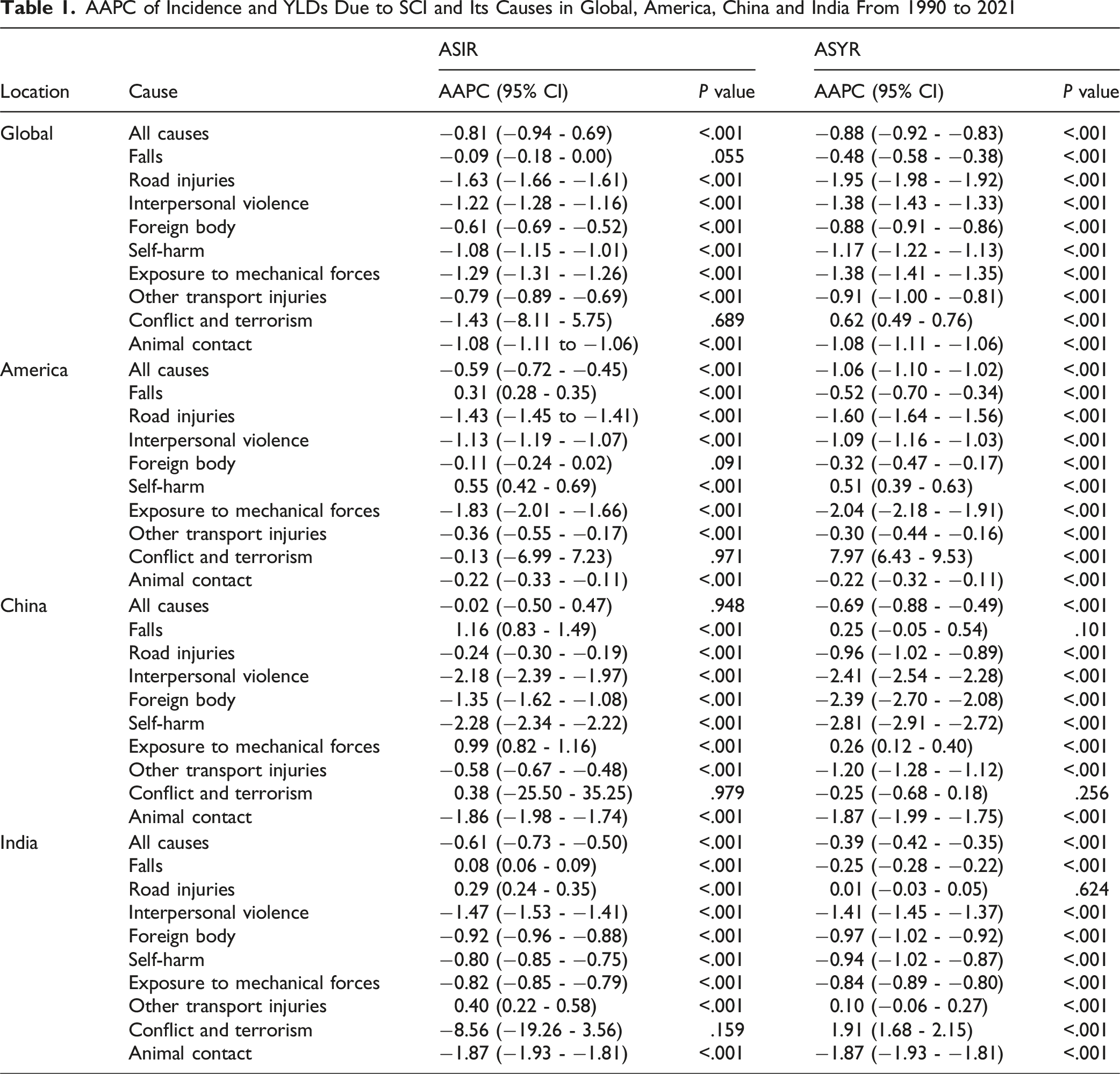
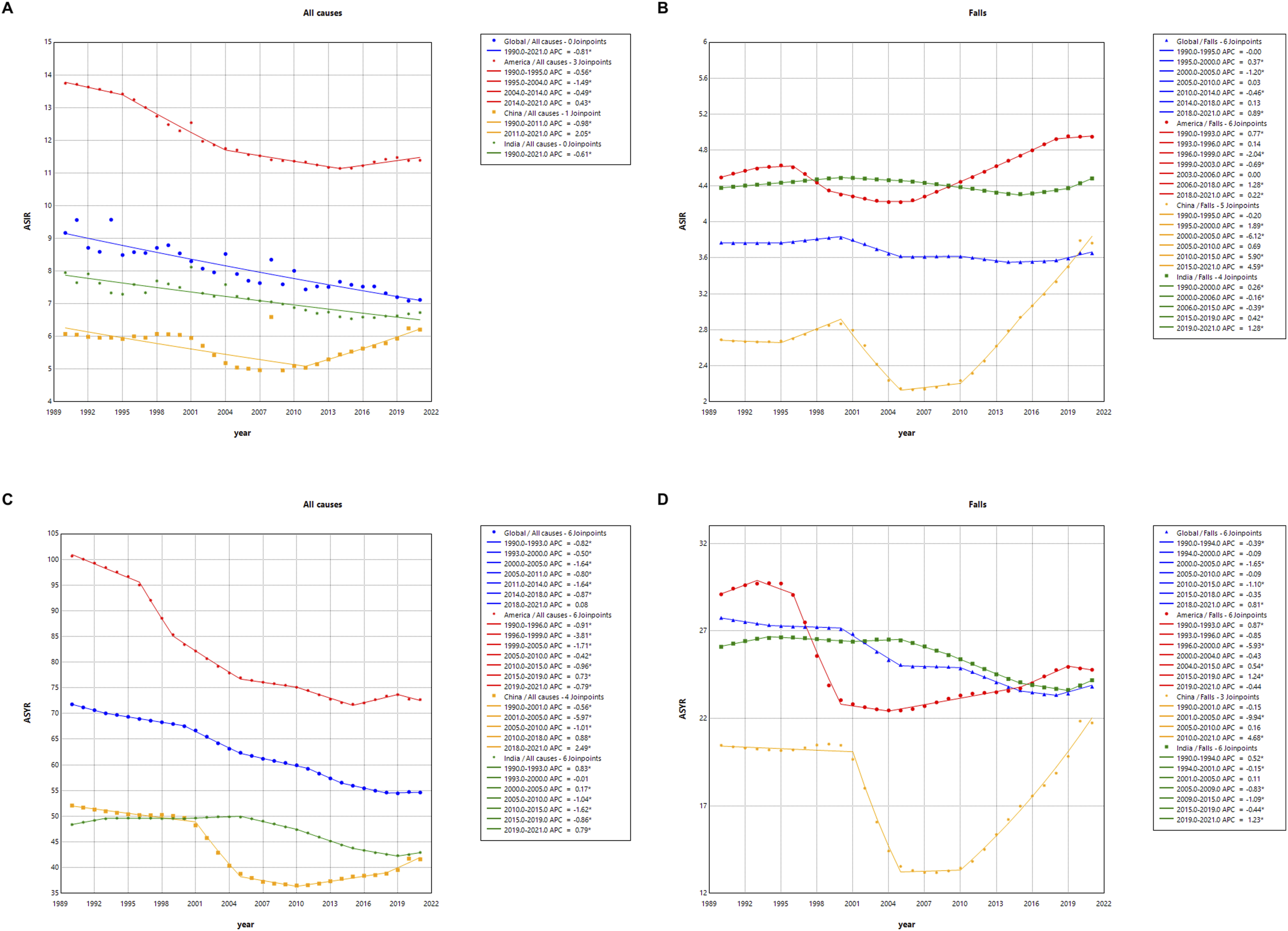
The APC in the ASIR and ASYR for SCI From 1990 to 2021. (A) ASIR Due to all Causes; (B) ASIR Due to Falls; (C) ASYR due to all Causes; (D) ASYR due to Falls. (*Indicates P-Values <.05, Denoting Statistically Significant Results)
SCI Development Forecast
The BAPC prediction model was used to forecast the future trends of SCI ASIR and ASYR from 2022 to 2035 in America, China, and India. The prediction results indicate that the ASIR and ASYR of SCI are expected to decline to varying degrees globally, as well as in America, China, and India. Additionally, it was observed that the ASIR and ASYR in America remain higher than the global average. Notably, the ASIR for Indian females is higher than the global level, and the prediction suggests that by 2035, the ASYR for Indian females will approach the global average (Figure 6). Disease Burden of SCI in Global, the United States, China and India (to 2035) Using BAPC Prediction Models: (A) ASIR Predicted by BAPC Model. (B) ASYR Predicted by BAPC Model. BAPC, Bayesian Mean Annual Percentage Change; ASIR, Age-Standardized Incidence Rate; ASYR, Age-Standardized YLDs Rate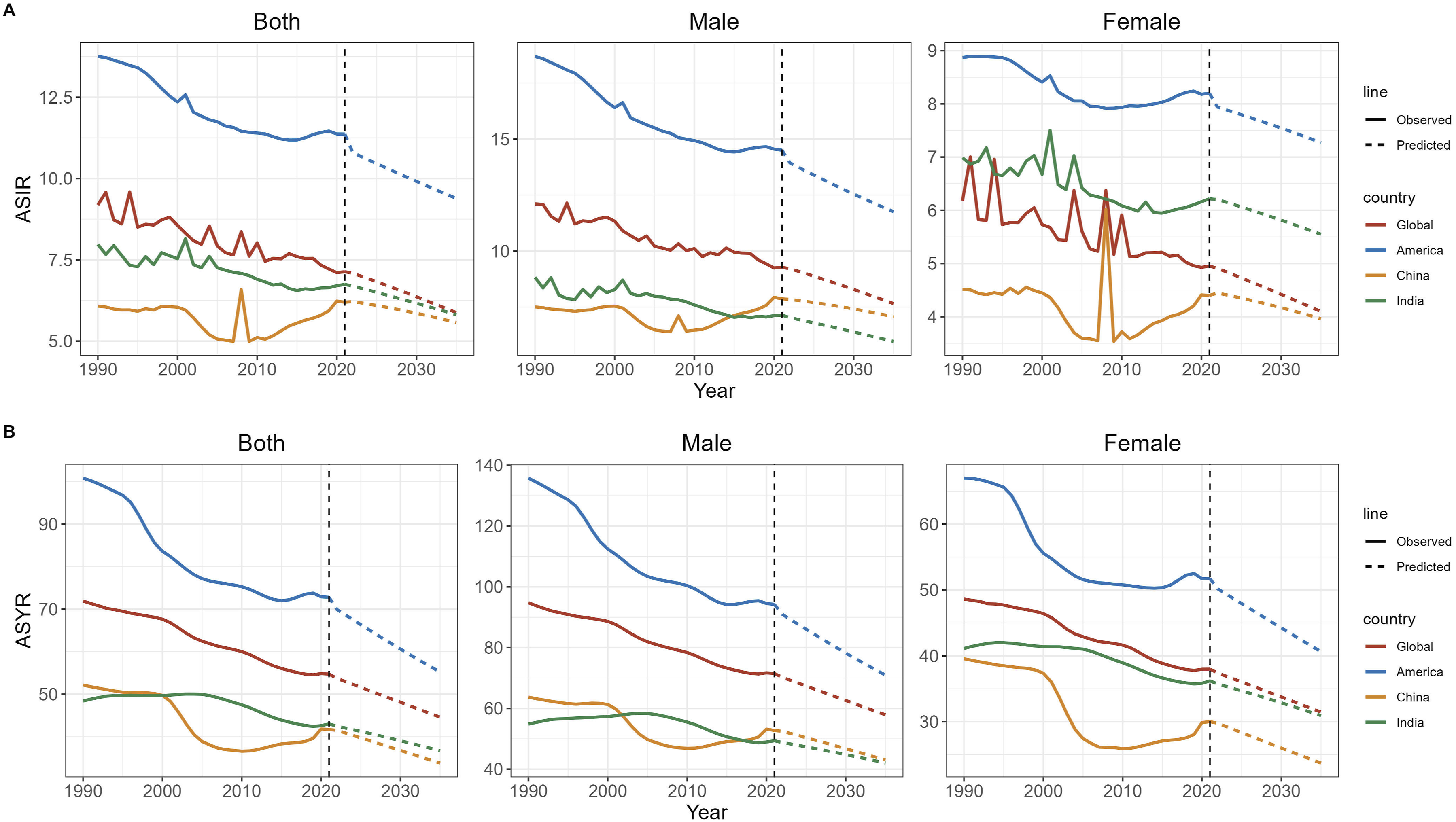
Decomposition Analysis
The study further conducted decomposition analysis to explore quantitative indicators of various factors influencing the number of incidence and YLDs from 1990 to 2021.
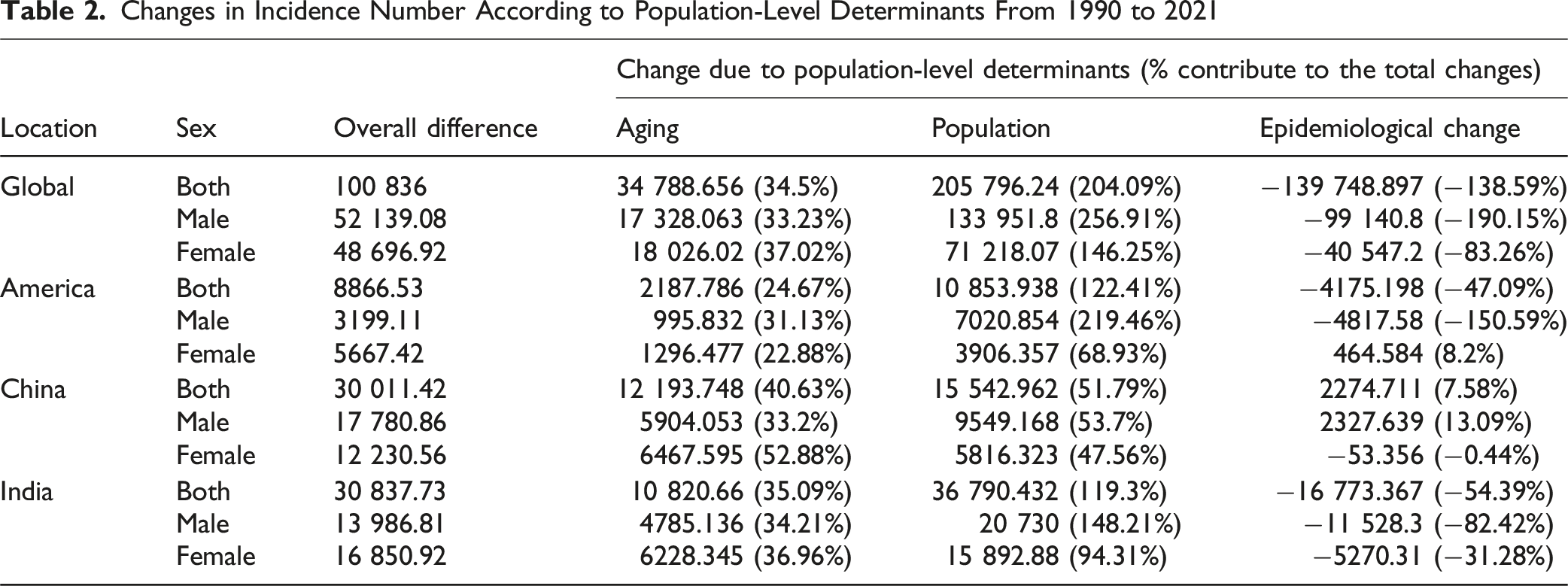
Regarding the number of incidence, from 1990 to 2021, the global SCI-related incidence increased significantly, reaching an additional 100 836 cases. This increase was decomposed into three aspects: aging, population growth, and epidemiological changes. The value attributed to aging was 34 788.656 (34.5%), to population growth was 205 796.24 (204.09%), and to epidemiological changes was −139,748.897 (−138.59%). Among America, China, and India, India experienced the largest increase, with aging and population growth accounting for 35.09% and 119.3% of the increase, respectively. Notably, the contribution of aging was most significant in China (40.63%), while the contribution of population growth was highest in America (122.41%). Globally, epidemiological changes showed a negative impact (−138.59%), with the most pronounced negative effect observed in India (−54.39%). The demographic and epidemiological impacts on incidence varied by gender across different national populations. In terms of the contribution of aging, Chinese females had the highest proportion (52.88%). For population growth, American males contributed the most (219.46%). Regarding epidemiological changes, American males experienced the highest negative impact (−150.59%) (Figure 7A and Table 2). Results of Decomposition Analysis of SCI: (A) Incidence of SCI. (B) YLDs of SCI Changes in Incidence Number According to Population-Level Determinants From 1990 to 2021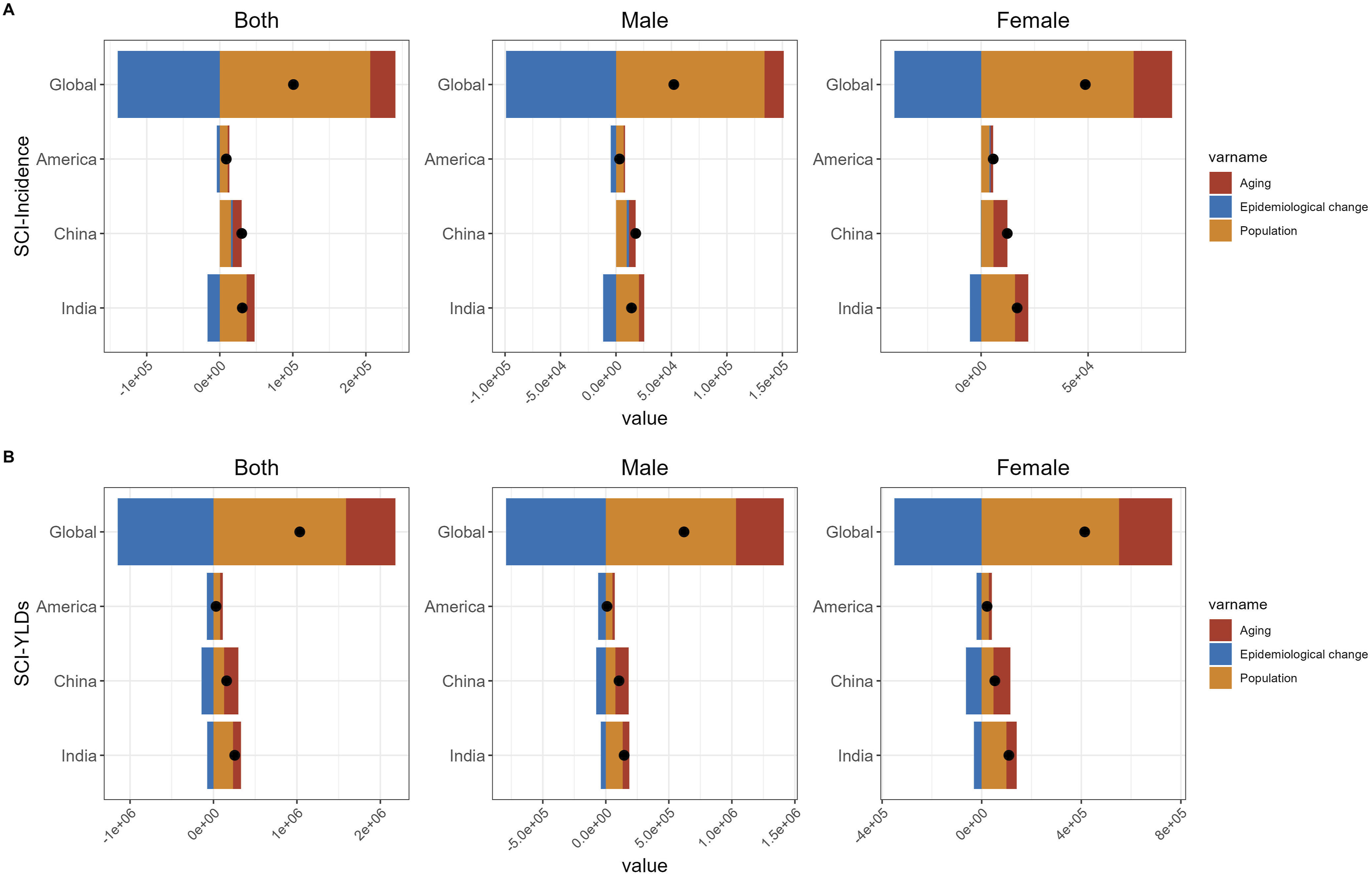
Changes in YLDs Number According to Population-Level Determinants From 1990 to 2021
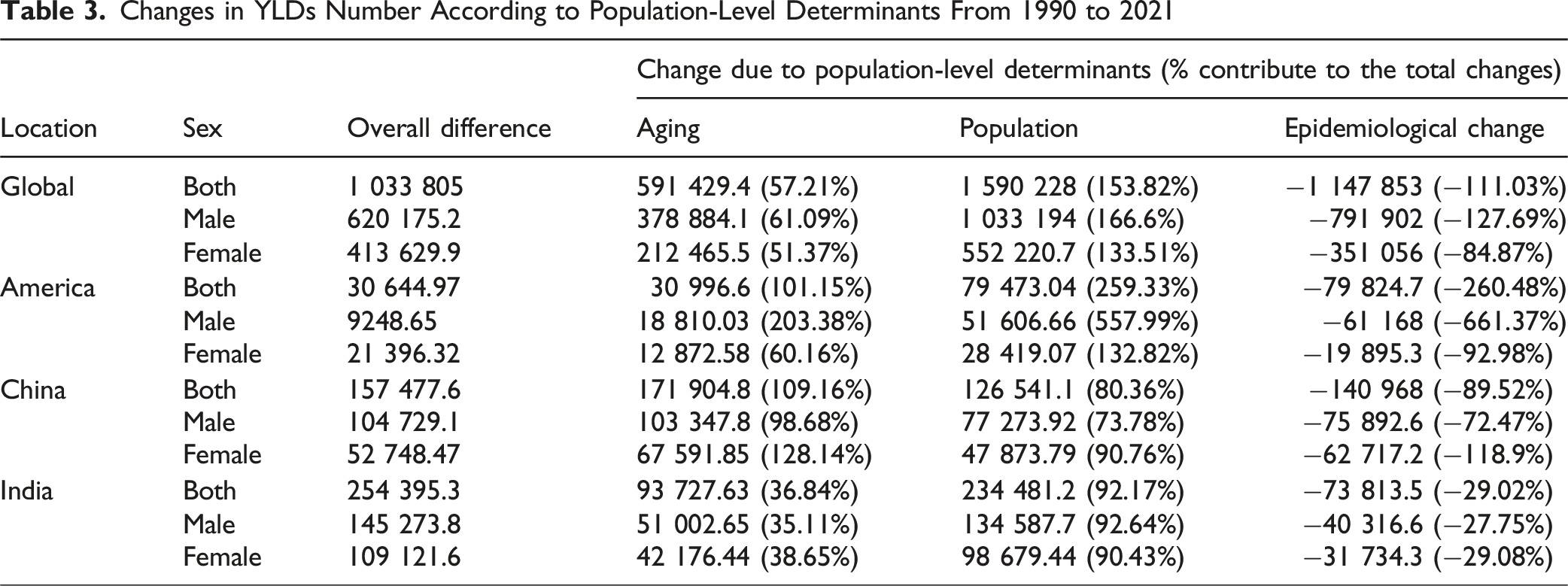
Overall, whether in terms of the number of incidence or YLDs, India exhibited the largest overall increase. Aging and population growth were the primary factors driving the increased SCI burden, with population aging having the most significant impact on China, particularly among females, and population growth having the greatest influence on America, especially among males.
Discussion
This study utilized the GBD database to conduct a comprehensive visualized analysis of the global burden of SCI. In 2021, SCI resulted in 574 502 incidence number globally, with China accounting for 17.3%, India for 15.57%, and America for 7.9%. Measured in terms of YLDs number, the global burden of SCI reached 4 566 237, with China contributing 16.47%, India 13.22%, and America 6.79%. Together, these three countries accounted for approximately 39% of the global SCI burden. Although both the AAPC results from 1990 to 2021 and the BAPC predictions for 2022 to 2035 indicate a declining trend in the SCI burden globally and in America, China, and India, the large number of SCI incidence and YLDs warrants increased attention from international health organizations. In summary, these findings indicate that China, India, and America bear the heaviest global burden of SCI. For regions with such high burdens, it is urgent to develop and implement effective prevention strategies and treatment measures, while also strengthening international cooperation to mitigate the global impact of SCI.
In the analysis of gender and age, we found that in 2021, the peak age group for SCI incidence among females occurred later than that of males. Previous studies have shown that although males overall experience more SCI, SCI incidence among females is higher in the 40+ age group. This phenomenon may be related to the longer life expectancy of females and postmenopausal health issues in later years, such as osteoporosis and falls.13,14 Conversely, males are more likely to engage in high-risk activities at a younger age, such as motorcycle accidents and working at heights. 15 We also observed that in India, the peak age for SCI incidence in males is younger, at 30-34 years. Studies suggest that the primary causes of SCI among young Indian males include engagement in high-risk occupations (such as construction, mining, and transportation) and sports activities. Additionally, traffic accidents and occupational hazards are the leading triggers of SCI in young males, closely tied to their socioeconomic roles and behaviors. 16 In terms of YLDs, regardless of gender, the peak age group in America was older than the global average, while China’s peak age group was similar to the global trend, and India’s was younger than the global average. This result may be attributed to the higher proportion of elderly individuals in the U.S. population and improved health management that extends the lifespan of older adults, resulting in more individuals experiencing SCI-related disabilities at an advanced age. Furthermore, the higher level of activity among the elderly in U.S. society may also contribute to this trend. 7 In China, the similarity of peak ages to the global average may be due to significant aging trends. However, unlike the U.S., middle-aged and older populations in China are more likely to engage in physical labor, resulting in YLD peaks aligning more closely with the global mean. 17 In India, the younger population proportion is larger, with a significant number of individuals engaged in high-risk labor such as construction and agriculture. Additionally, the limited availability of healthcare resources in India may lead to inadequate rehabilitation for younger patients, resulting in disabilities occurring at earlier stages of life. 13
Globally, Falls are one of the leading causes of SCI, particularly among individuals aged 60 and above. With global population aging, SCI related to falls is expected to continue increasing in the future. 18 In America, the incidence of fall-related SCI has risen rapidly, especially among individuals aged 65 and older. Studies have also found that limitations in medical intervention and rehabilitation services for the elderly may be significant factors contributing to severe disabilities. 19 In India, the high proportion of younger populations and widespread engagement in high-risk occupations (such as construction) are major contributors to SCI. Despite this, fall-related SCI among older adults in India is also showing an upward trend, 20 consistent with our findings. However, it is worth noting that the APC values for ASIR and ASYR in China from 2010 to 2021 were significantly higher than those in America and India, indicating a clear upward trend. This may be related to the accelerated population aging process in China after 2010. 21 At the same time, China’s economic development has fueled growth in sports activities, tourism, and industrial production, along with an increase in high-risk activities such as mountaineering, skiing, and adventure sports, leading to more cases of SCI. 10 Additionally, after 2010, China experienced rapid urbanization, with the development of high-risk industries such as construction and transportation, creating environments conducive to the occurrence of SCI. 22
This study revealed that in 1990, Road Injuries ranked first among the causes of SCI in America, reflecting issues related to transportation infrastructure and traffic accident management at the time. Over the years, improvements in traffic safety regulations, vehicle safety design, and road management significantly reduced traffic accidents, 23 as evidenced by the change in cause rankings in 2021. We also found that in the case of Road Injuries, the peak age group for incidence in America was the youngest, at 20-24 years. This could be attributed to the frequent engagement of young people in high-risk behaviors, including reckless driving, drunk driving, and driving while fatigued. Furthermore, this age group represents a critical period for learning to drive and beginning to drive independently, during which a lack of driving experience further increases the risks. Additionally, the complex transportation infrastructure and the culture of long-distance commuting in America expose young people to higher traffic-related risks.24,25 In India, we observed that in 1990, the SCI disease burden caused by Conflict and Terrorism and Interpersonal Violence was relatively high. This may be due to the country’s political instability, armed conflicts, and terrorist activities at the time, which often resulted in multiple types of trauma, including SCI, thereby increasing the disease burden. This situation had improved by 2021. We also found that the SCI-related ASIR for Indian females was higher than the global average, and predictions indicate that the ASYR for Indian females will approach the global level by 2035. Additionally, SCI disease burden caused by Self-harm in females requires special attention. Globally, among males aged 15-19 years, Conflict and Terrorism stood out as a cause of SCI. The susceptibility of adolescents (particularly males) is directly related to the frequency of violent events, especially in conflict zones where high exposure rates are observed. 26 Male adolescents are often at risk of direct involvement or passive entanglement in societal and conflict-related violence, such as recruitment as soldiers or being drawn into terrorist activities. The international community and relevant nations should enhance protective measures for adolescents, particularly males, in conflict-affected areas. This includes strengthening psychological interventions, reducing the likelihood of recruitment or involvement in terrorism, improving access to education and employment opportunities, and providing more nonviolent avenues for social participation for adolescents.
The decomposition analysis revealed that the improvement in SCI burden was primarily due to epidemiological changes. However, it was negatively impacted by population growth and aging. Population aging had the most significant impact on the disease burden in China, particularly among females, whereas population growth had the greatest influence in America, especially among males. Epidemiological changes, including advances in medical technology and improvements in the treatment of traumatic SCI, have significantly reduced the direct burden of the disease. 27 In America, population growth led to an increase in SCI incidence among young and middle-aged adults (particularly males), closely associated with occupational injuries and traffic accidents. 28 In China, the longer life expectancy of females and their physiological characteristics (such as decreased bone density) made them more susceptible to spinal cord trauma in the context of population aging. This phenomenon is particularly prominent given the aging process in China. 29 To address epidemiological changes, further improvements in prevention and medical intervention are needed. To mitigate the impact of population aging, the focus should be on chronic disease prevention and long-term care. Strengthened global health cooperation and the development of targeted public health policies are essential to reduce the burden of SCI.
The limitations of this study are similar to those of other GBD studies.30,31 The GBD database sources its data from medical records, surveys, and modeling estimates. However, in many low- and middle-income countries, SCI data collection may be incomplete, particularly for non-fatal cases caused by traffic accidents or Falls, potentially leading to an underestimation of the disease burden. Secondly, the GBD database’s risk attribution modeling may oversimplify the contribution of certain risk factors, failing to fully reflect the multifactorial impacts. Additionally, the GBD primarily focuses on the direct disease burden and does not adequately consider the indirect impacts of SCI, such as family caregiving burdens and losses in economic productivity. While the GBD database predicts future burden based on past disease patterns and data, it may fail to account for rapid advancements in medical technology and policy changes (eg, implementation of traffic safety measures), potentially leading to inaccuracies in forecasting the future trends of SCI burden.
Conclusions
This study conducted a comprehensive visualized analysis of SCI incidence and YLDs globally, as well as in America, China, and India, from 1990 to 2021. Over the past 30 years, despite significant reductions in SCI-related ASIR and ASYR due to changes in population and epidemiology, the disease burden measured by the number of SCI cases and YLDs has generally increased. The peak age group for SCI incidence among females occurred later than that of males, while the overall SCI burden was heavier for males than females. Falls were identified as the primary risk factor for SCI across all age groups. America should focus on addressing the SCI burden caused by population growth and road injuries. China needs to prioritize managing the SCI burden caused by population aging and falls, while India should pay special attention to the SCI burden among females. Relevant countries should develop targeted public health strategies tailored to their specific circumstances to prevent SCI and improve health management in order to tackle the upcoming challenges.
Footnotes
Acknowledgements
We sincerely appreciate the great work of GBD collaborators. In addition, this study was generously supported by Jingding Medical Tech, to whom we extend our sincere gratitude. We especially thank them for providing authorization and technical support for the JD_GBDR software. The team at Jingding Medical Tech offered invaluable assistance in data processing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Institutional Review Board Approval
The institutional ethics committee granted an exemption for this study, as it did not require approval, given that the data from the 2021 Global Burden of Disease (GBD) is publicly available. This study adhered to the guidelines for accurate and transparent health assessment reporting. Since publicly accessible data were used, Institutional Review Board approval was not required for this study.