
Abstract
Study Design
Systematic Review.
Objective
To describe the historical classifications of thoracolumbar injuries and their evolution into the AO Spine Thoracolumbar Injury Classification System.
Methods
A systematic review of MEDLINE, EMBASE and Cochrane Databases was performed in keeping with Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.
Results
445 articles were crystallized to 14 included studies. Simple categorization systems offered by Bohler or Watson-Jones merely identify fracture morphology. Holdsworth and Denis conveyed a sense of the stability of injuries by noting columns of stability, but still failed to take into consideration important factors such as neurological status or specific integrity of key stabilizing structures. The AO Spine Thoracolumbar Injury Classification System provides 3 hierarchical categories: type A consisting of compression type injuries, type B composed of distraction injuries and the unstable type C comprising displacement injuries. This communicates the severity of the fracture to clinicians and, with the addition of modifiers, can be synthesised into a scoring system to guide management. This classification is based upon biomechanical stability and increasing likelihood of clinicians offering operative rather than non-operative intervention as fracture severity escalates.
Conclusions
A combination of evaluating fracture morphology, integrity of the posterior ligamentous complex and neurological status of the patient in the context of individual patient modifiers is integral to guide surgical decision making. The AO Thoracolumbar Injury Classification System accounts for all of the aforementioned and is the derivative and advancement on existing historical systems. Further nuanced development of scoring systems to guide operative or non-operative management is still required.
Introduction
The thoracic spine demonstrates the primary curvature of kyphosis due to the wedge shape of the vertebral bodies and intervertebral discs. 1 Thoracic discs are also proportionately shorter in relation to vertebral height when compared to discs within the cervical and lumbar regions. 2 The thoracic region is unique given it derives support from the rib cage, which biomechanically increases the load bearing capacity of the spine by up to 3 times through articulation of the vertebral bodies with the rib heads. 3 Panjabi et al highlighted that applying the same load without the stabilizing thoracic cage results in greater flexion and extension. 4 Watkins et al further investigated this to find the thoracic cage contributed to 40% of the thoracic spine’s stability in flexion and extension, 35% in lateral movement and 31% with axial rotation. 5
In addition, the facet joints also protect the thoracic region against extreme axial rotation and to some degree against translation due to their sagittal orientation. 6 Indeed, the lower thoracic facet joints are increasingly angled in the sagittal plane and resemble those in the lumbar spine. 7 The stability of the thoracic spine is also reliant upon the ligamentous structures including the anterior longitudinal ligament (ALL) extending from C1 to the sacrum. 6 The ALL is thickest where it is firmly attached to the vertebral bodies. 8 In contrast, the multi-layered posterior longitudinal ligament is much thinner over the vertebral body and attaches to the intervertebral discs. 6 These structures are supplemented by capsular ligaments, intertransverse ligaments, and interspinous and supraspinous ligaments (which limit hyperflexion), as well as the paraspinal musculature. 9 All of these anatomical structures must be taken into consideration when attempting to develop a reliable clinically applicable spine trauma classification system.
Increasing biomechanical understanding of the translational vector forces that result in specific fracture morphology patterns has been reflected in the development of early classification systems. Historical systems such as the simple Watson-Jones classification included 4 basic morphologies that evolved into the now well-known Denis three-column theory, allowing clinicians to understand degrees of stability from the classification alone. Despite this, there still remains a lack of a universally accepted thoracolumbar injury classification which logically categorizes fractures into a gradated stepwise fashion to form the basis of an accepted treatment algorithm.10-12
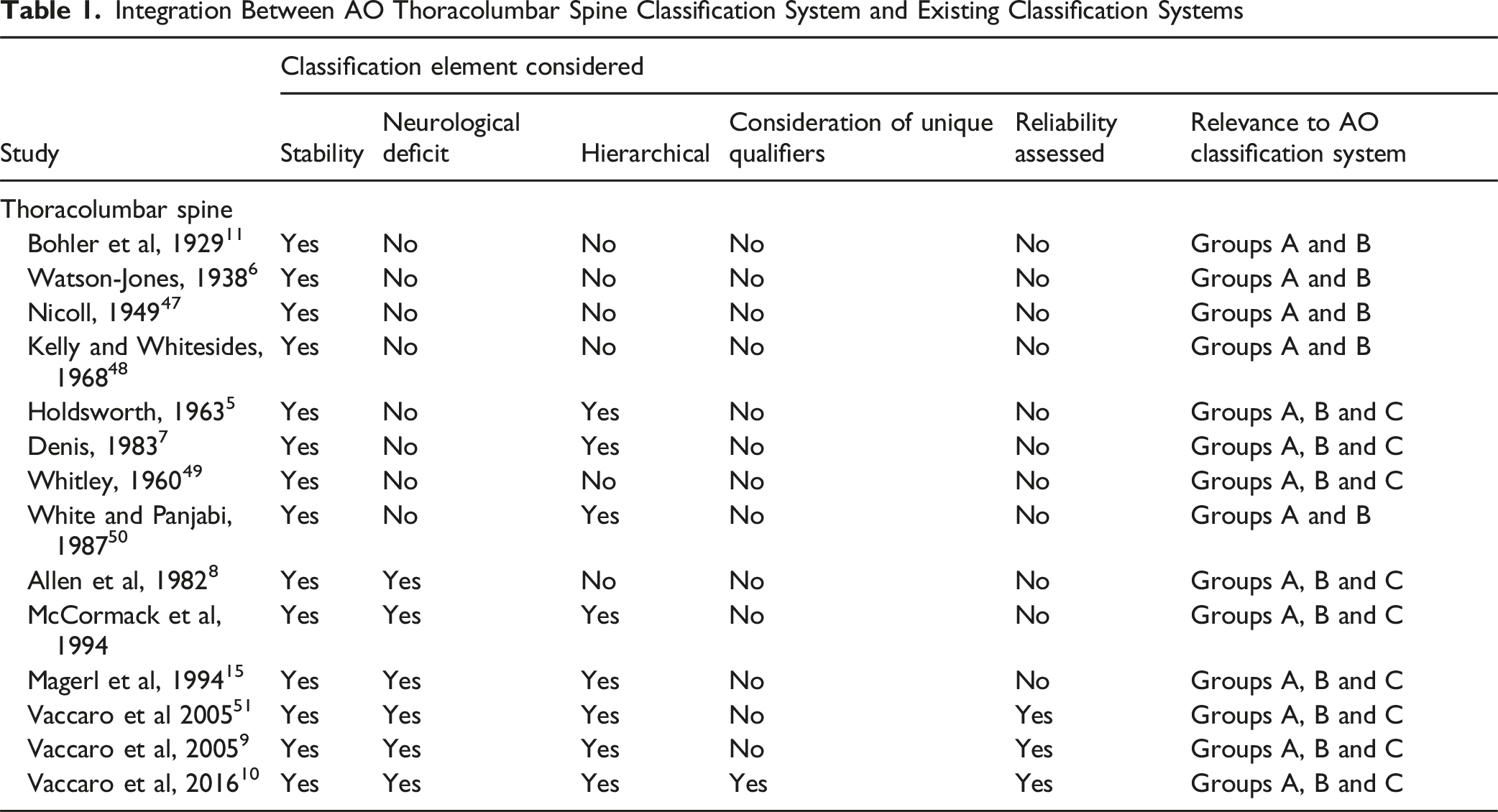
Integration Between AO Thoracolumbar Spine Classification System and Existing Classification Systems
Methods
Search and Eligibility Criteria
The authors conducted a systematic electronic search of the Medline, EMBASE and Cochrane Database of Systematic Reviews from their date of inception to August 2024 was conducted in keeping with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Databases were queried with the proceeding terms combined with Boolean operators: ‘thoracolumbar’ and ‘injur*’, or ‘classification’, or ‘system’ and ‘fracture’. Only studies examining human subjects in the language English or with available English translations were included. No registered review protocol exists for this study.
Inclusion and Exclusion Criteria
Eligible abstracts were checked by 2 authors (B.T.S.K and J.W.T), before appropriate articles for full-text examination were scrutinized. Bibliographies of included studies were also interrogated for further eligible articles. Discrepancies were discussed until consensus attained. Inclusion criteria were defined as: (1) Any form of article, whether randomised or non-randomised controlled trials, cohort study, case series, case report or review article which proposed a new classification system that was defined as a method of grading fractures upon a rational basis with 2 or more categories (2) Any article which added a new category to an established classification system (3) Human Subjects.
Study Selection and Data Extraction
Extraction of data into a preformatted spreadsheet was performed independently by 1 author (B.T.S.K) and cross-checked by another (J.W.T) in accordance with the Cochrane Handbook for Systematic Reviews. 1 No authors were contacted for further unpublished data.
Appraisal and Synthesis of Results
The Risk Of Bias In Non-Randomized Studies of Interventions (ROBINS-I) tool and Murad et al instrument was applied for included non-randomized studies and case studies or case reports respectively.2,3 Study quality was independently assessed by 2 authors (B.T.S.K and J.W.T) with consensus attained following discussion. The ‘Robvis’ tool was utilised to generate the traffic light plot in accordance with Cochrane recommendations. 4
Results
Study Selection
The primary search retrieved 1088 articles which was condensed to 445 manuscripts after duplicates were removed (Supplemental Figure 1). 43 studies satisfied the criteria for full-text assessment for eligibility once screening was concluded. Fourteen studies were eventually deemed suitable for qualitative analysis in the systematic review (Table 1). 29 articles were excluded with 21 lacking a proposed grading scheme contained within a publication and the remaining 8 articles being incomplete reviews.
Study Quality
Risk of Bias Assessment of Included Case Series and Case Report Studies Assessed by the Tool Developed by Murad et al. 52
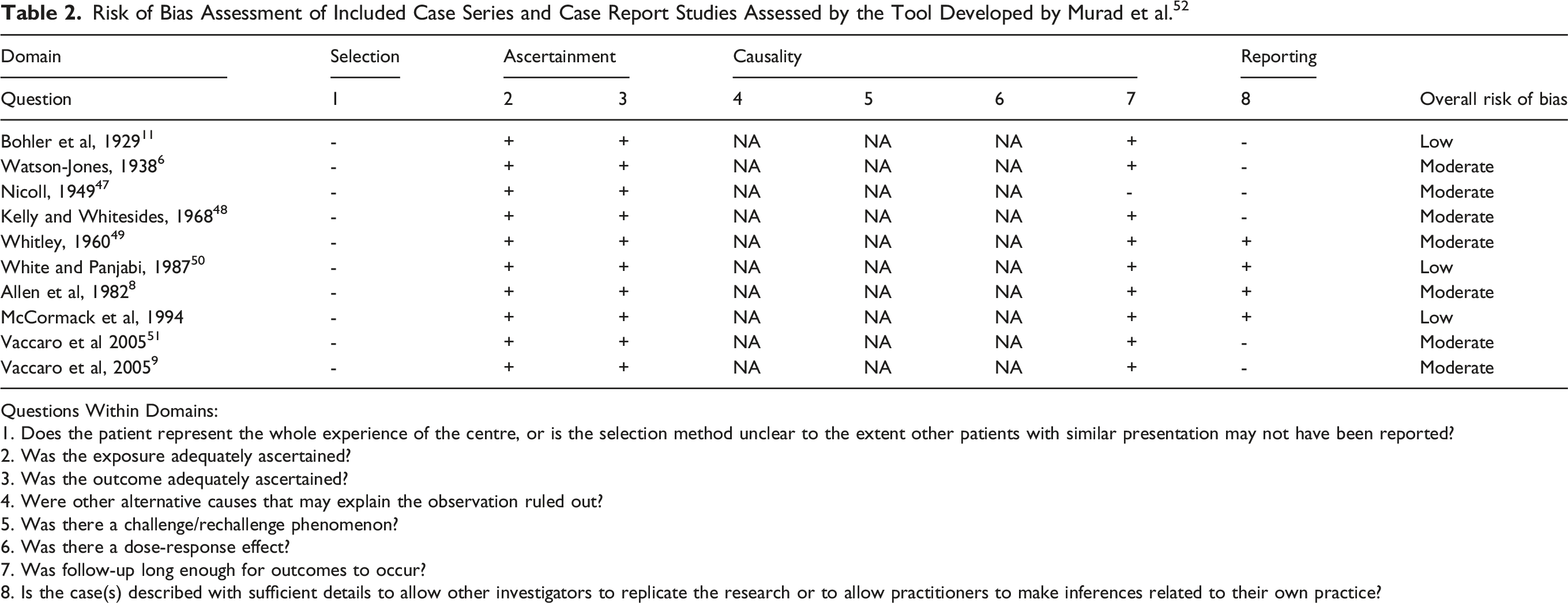
Questions Within Domains:
1. Does the patient represent the whole experience of the centre, or is the selection method unclear to the extent other patients with similar presentation may not have been reported?
2. Was the exposure adequately ascertained?
3. Was the outcome adequately ascertained?
4. Were other alternative causes that may explain the observation ruled out?
5. Was there a challenge/rechallenge phenomenon?
6. Was there a dose-response effect?
7. Was follow-up long enough for outcomes to occur?
8. Is the case(s) described with sufficient details to allow other investigators to replicate the research or to allow practitioners to make inferences related to their own practice?
Classification Systems
Fourteen discrete classification systems were identified which chronicled the evolution of the biomechanical and clinical understanding of thoracolumbar fractures over time. This ranged from the basic vector of force systems proffered by Watson-Jones to the two-column model of Holdsworth et al.5,6 Denis et al expounded upon this and championed the renowned 3 column model of spinal injuries. 7 More than this, Allen et al doubled the number of categories with 6 mechanistic classes of thoracolumbar injuries being recognized but yet notably this scheme was still devoid of translation into a hierarchial scoring system to guide clinical decision making. 8 Vaccaro et al resolved this by establishing the universal AO Thoracolumbar Injury Classification System and Thoracolumbar Injury Classification and Severity Score.9,10
Discussion
Historical Classification Systems
Bohler proposed the first classification system in 1929. 11 This was further developed by Watson-Jones in 1938 who described 4 basic morphologies: simple wedge fracture, comminuted fracture, fracture dislocation and hyperextension injuries.6,12 Wilke et al identified the biomechanical significance of this given the thoracic spinal ligaments have a strong stabilizing role and are thicker in this region than the cervical or lumbar spine. 13 This was followed by a two-column model offered by Holdsworth et al, which was further developed by Denis et al into the famous 3 column model still referenced today.5,7 The anterior column consists of the anterior two-thirds of the vertebral body and disc as well as the ALL, whilst the middle column includes the posterior one-third of the vertebral body and disc with the PLL. Finally, the posterior column includes the posterior elements structures. A criticism levelled against the model proposed by Denis et al was its focus on clinical simplicity whilst ignoring biomechanics. 7 For example, Yoganandan et al argued instability is a continuum rather than a dichotomy and partial injuries to the disc and ligaments may still result in instability. 14
The Denis model was a useful bedside clinical rule for clinicians who could quickly estimate whether an injury was stable or unstable based on whether 2 or more columns were involved, but a more reliable and validated treatment algorithm was required. 7 The primary shortcoming was implying instability based upon middle column injury, suggesting all burst fractures were inherently unstable. Eventually, in 1994, Magerl proposed what would become the basis for the novel AO Spine thoracolumbar injury classification system. 15 Type A fractures consisted of compression injuries, type B were distraction injuries and type C were rotational injuries.15,16 Each of the 3 groups was in turn divided into 3 subgroups. The schemes provided the most comprehensive description of patterns of fractures, but has less emphasis on their prognostic value. This has led to limited applicability in everyday practice and poor reliability. 15
Importantly, the Magerl system was consistent with biomechanical principles. In the type A category, compression fractures were a result of pure axial forces close to the weight-bearing axis producing endplate deformities. 17 Sances et al found that isolated thoracolumbar specimens failed with forces of 800N to 5100N. 18 The forces required varied according to the posture of the specimen which included degree of flexion as well as the length of the spine tested. 18 In contrast, Willen et al subjected vertebral preparations with surrounding discs, facet joints and ligaments to an instant axial dynamic force and found initial fracturing at an average force of 8000N. 19 Comminution of the vertebral body with retropulsed fragments into the spinal canal and the classic burst fracture occurred with 11000N. 19 Interestingly, the variation in forces required between biomechanical experiments is typical of differing experimental conditions. The age of the specimens also likely played a role with all of the specimens in the study by Willen et al being less than 40 years. 19
Translating this into the clinical environment, surgeons often agree upon the conservative management of stable simple compression fractures and the operative management of clearly translated and rotational injuries. As an area of equipoise though remains the contemporary management of thoracolumbar burst fractures without neurological deficit which remains controversial.20-22 Additionally, radiographic outcomes do not necessarily correlate with superior clinical outcomes alone. 23 Some authors argue that stabilization should be performed even in the absence of neurological deficit to mitigate the risk of post-traumatic kyphotic deformity.24,25 This has been countered by other authors who have found no correlation between radiological kyphotic progression and clinical outcomes.26-31 It is likely that the correct management lies in between these two extremes and each individual patient must be evaluated.
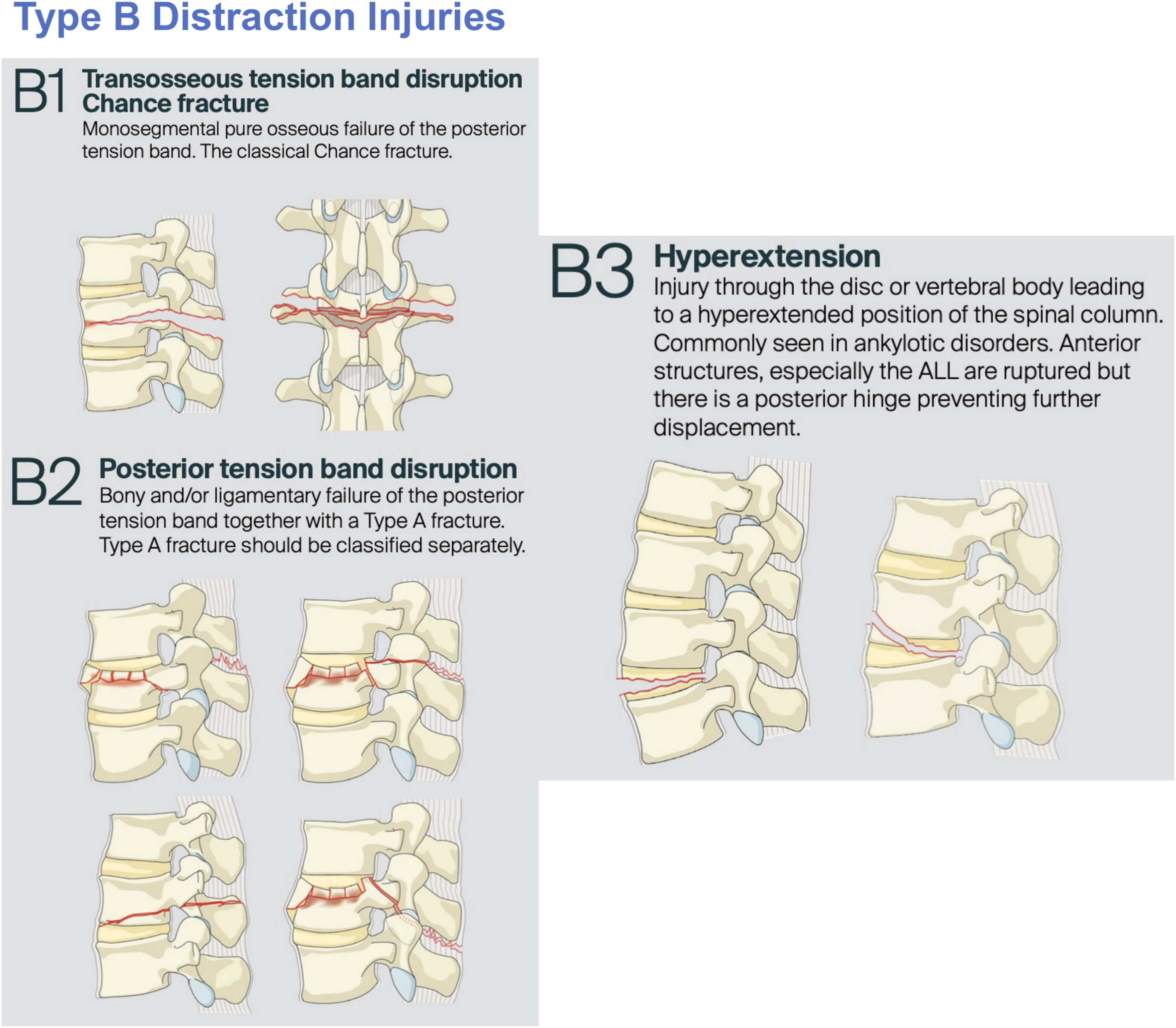
There exists a clear preference for operative management of type B injuries compared to type A injuries which is in keeping with the AO Spine system.9,10 These distraction injuries were investigated by Panjabi et al in 1981. 32 This in vitro study defined the functional spinal unit as two vertebrae connected by soft tissue and loaded 19 individual samples until failure. 32 Crucially, they determined that the spine was most likely to fail in posterior injury with loads causing flexion, in line with B1 or B2 injuries, whilst anterior injury failed with loads causing extension consistent with B3 injuries. 10 It was when all ligaments anterior to and including the posterior longitudinal ligament were transected did the functional spinal unit become unstable. 32 Strikingly, the thoracolumbar junction is the most common site of these flexion-distraction injuries or ‘seat belt’ fractures. 33
This was explained by White et al who found there were more degrees of sagittal plane motion in the more caudal thoracic spine, with 4° in the upper thoracic spine, 6° in the middle segments and up to 12° in the lower portion at T11/12 and T12/L1. 34 This is similar to the findings of Wilke et al with the thoracic spine possessing the highest range of motion between 10 and 12° in the upper and middle thoracic spine, and between 7 and 8° in the lower thoracic spine (T10-T12). 35 The biomechanical basis for this is both the absence of the stabilizing thoracic cage and also that the T11 and T12 vertebrae are unique in having their inferior articular facets oriented in the sagittal direction similar the lumbar spine. 36 Our multicenter study investigated the use of a modifier to indicate that there may be indeterminate ligamentous injury. Unsurprisingly, and consistent with the biomechanical literature, this increased the chance of operative management when comparing type B and C injuries to type A3/A4 injuries (OR 39.19, 95% CI 20.84-73.69, P < 0.01 vs OR 27.72, 95% CI 14.68-52.33, P < 0.01).37-40
Evolving from a simple classification system, Vaccaro et al aimed to provide clinicians with a treatment recommendation using a validated algorithm.9,41,42 This was the thoracolumbar injury classification and severity score (TLICS) followed by the thoracolumbar AO Spine Injury Score (TL AO SIS). This more detailed scoring system acknowledged that not all burst fractures should be weighed equally. 43 In fact, a complete A4 burst fracture is weighted 5 points whilst an incomplete A3 burst fracture is awarded only 3 points. 43 In other words, a complete burst fracture is now closer in severity to a type B tension band injury than it is to a simple single endplate fracture. 43 In comparison to the TLICS, Nagi et al confirmed that the TL AO SIS aligned more closely with real world treatment recommendations (88.6% vs 85.7%). 44
A final consideration in future classification systems is that the level of the fracture should also be considered. As explored in our previous subaxial cervical spine study, cervicothoracic junctional injuries were perceived by clinicians as more severe. 45 Edmondston et al found the motion segment T11/2 was found to have the greatest motion in all 6 degrees of freedom. 13 Furthermore, the compressive load increases experienced in the lower thoracic spine were greater than those in the upper thoracic spine, with 9% at T1 33% at T8 and 47% at T12, for instance. 13 Furthermore, the compressive load increases in the lower thoracic spine being only 9% at T1, increasing to 33% at T8 and 47% at T12. 13 This spine loading pattern explains the location of vertebral fractures being preferentially in the mid-thoracic and thoracolumbar regions.
Maiman et al also identified a tendency for different vertebral body fracture lines across the spine with transverse fracture lines being common from T1-T8, and oblique fracture patterns from T9-T12. 36 Future thoracolumbar injury classification systems should also take into consideration the level of the injured segment as biomechanical studies often do.
AO Spine Thoracolumbar Injury Classification System
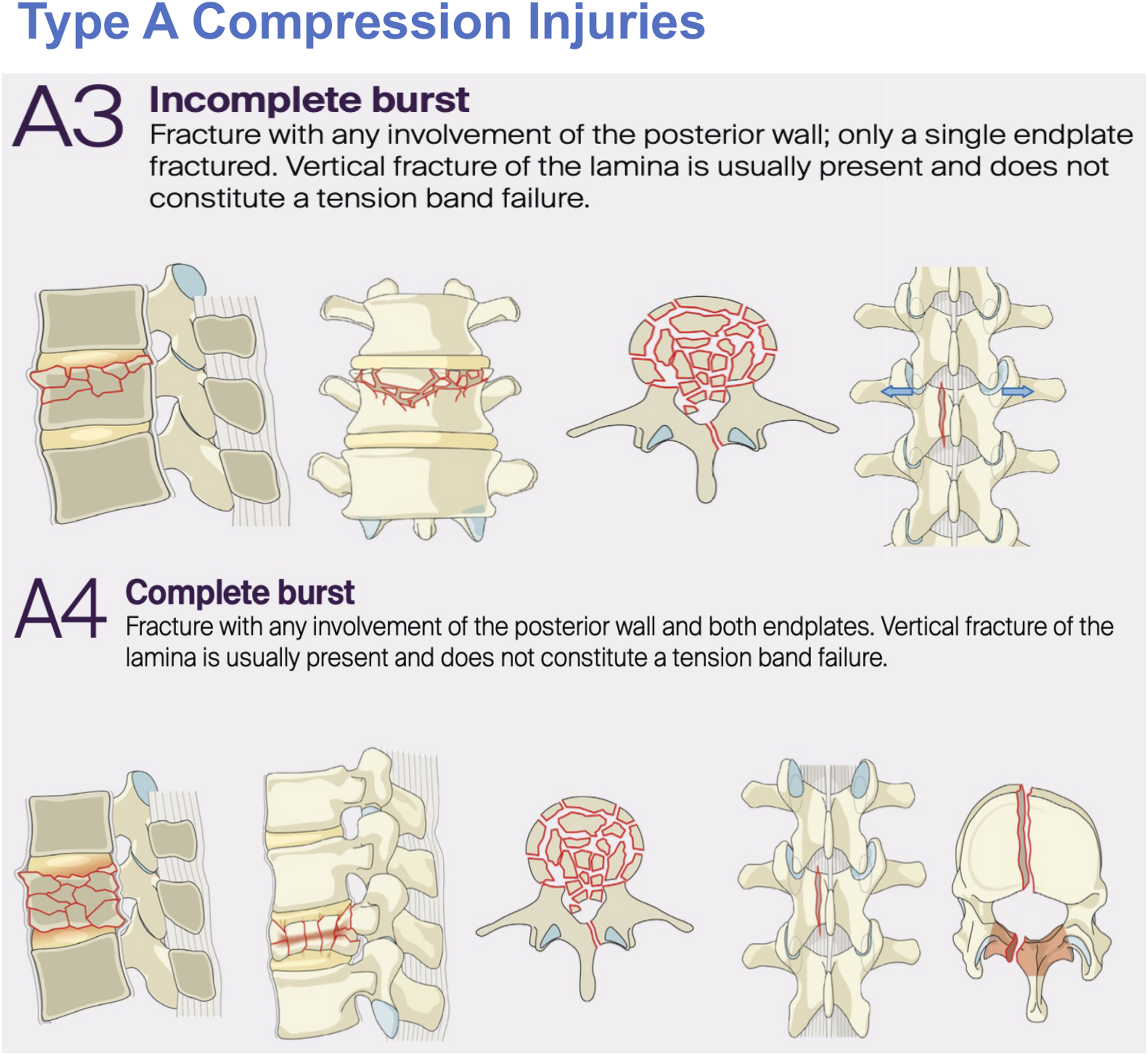
Our novel research with AO Spine in developing a universally applicable thoracolumbar injury classification system is based on a sound understanding of the biomechanics of the spine. The findings of previous studies validated the AO Spine Thoracolumbar Injury Classification system by demonstrating a stepwise statistically significant increase in the rate of operative management (P < 0.001) as fracture severity progressed from type A0/A1/A2 (Figure 1), to type A3/A4 (Figure 2) then type B1/B2 (Figure 3) and type C injuries (Figure 4).
46
There was excellent correlation between recommended expert management and the real-world treatment of each category of injury: A0/A1/A2 (OR 1.09, 95% CI 0.70-1.69, P = 0.71), A3/4 (OR 1.62, 95% CI 0.98-2.66, P = 0.58) and B1/B2/C (1.00, 95% CI 0.87-1.14, P = 0.99).
46
This study also addressed the crucial area of thoracolumbar burst fractures, for which there is often clinical disagreement.
46
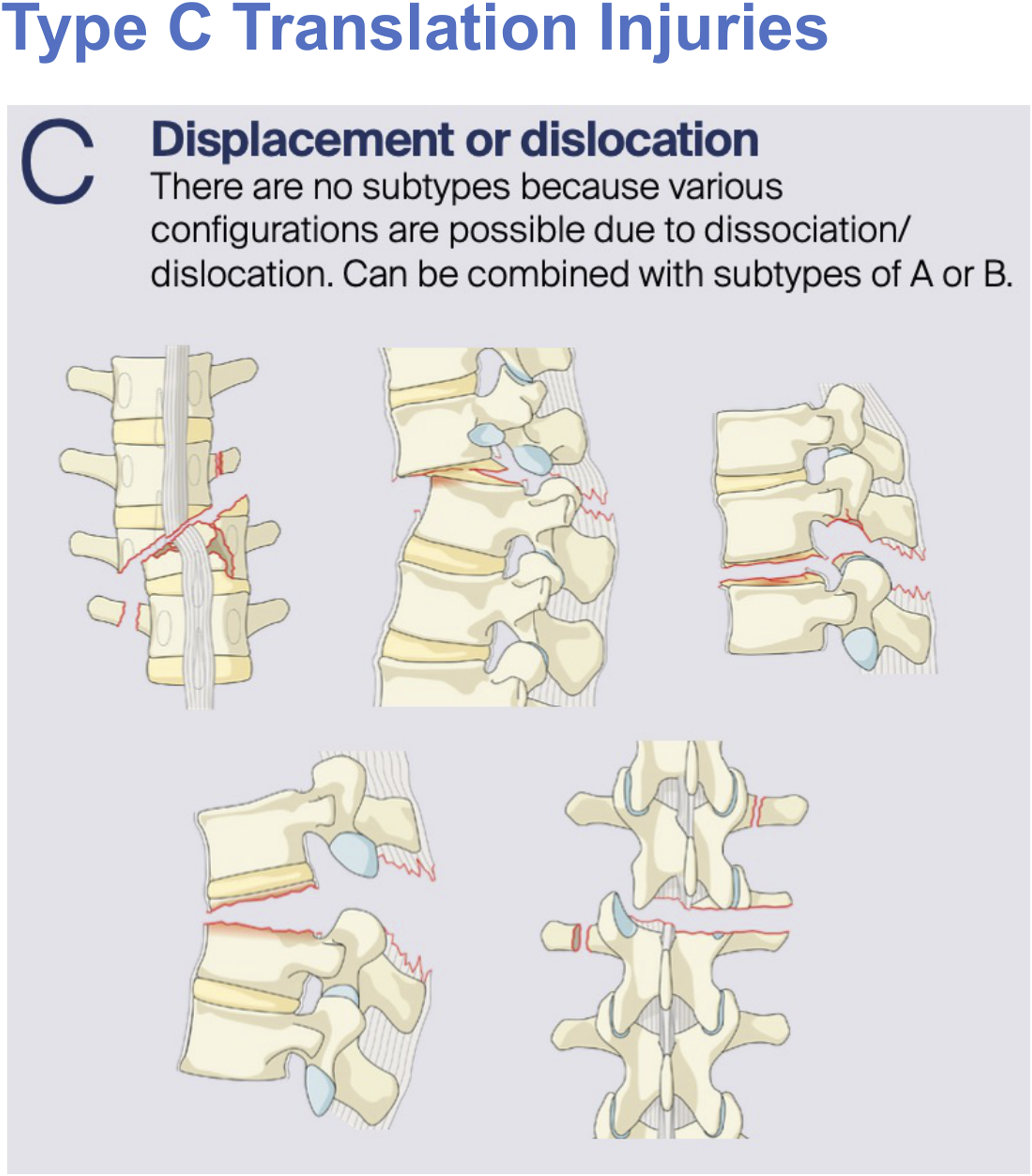
Most commonly occurring at the junction of the relatively rigid kyphotic thoracic spine and more mobile lordotic lumbar spine, these fractures have the potential to cause devastating neurological sequelae. Type A Compression Injuries Ranging From A0 Minor Non-structural Injuries, to A1 Wedge-Compression Fractures and Finally A2 Pincer Fractures Type A Fractures including From Single Endplate Involving A3 Incomplete Burst Fractures to Dual Endplate A4 Complete Burst Fractures Type B Fractures Constituting B1 Transosseous Tension Band Chance Fractures, B2 Posterior Tension Band Disruption Ligamentous Injuries and Finally B3 Hyperextension Injuries Type C Translation Injuries Representing the Most Unstable of Thoracolumbar Burst Injuries and Usually Requiring Surgical Fixation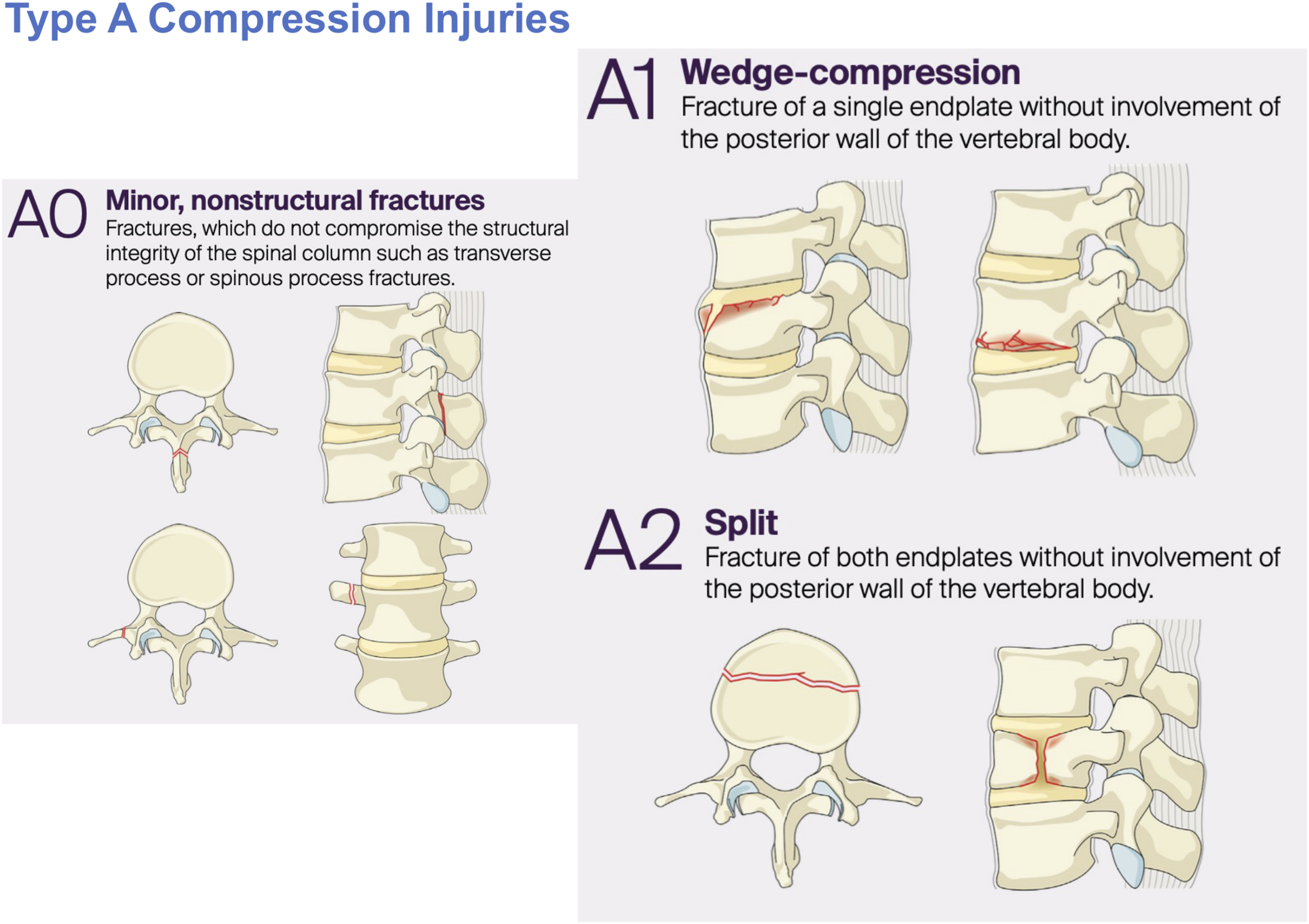
Existing classifications are pooled from a diverse range of international centers which in turn confers excellent external validity. Crucially, the AO Spine system provides a novel alternative to this assortment of disjointed systems in the TL AO SIS with its advancement and hierarchical nature based upon historical classifications (Table 1). Limitations historical systems are the somewhat arbitrary classifications proposed such as a simple fracture morphology by Watson-Jones rather than that derived from a biomechanical framework as Holdsworth et al or Denis et al later proposed.5-7 Whilst this TL AO SIS also provides a useful hierarchy of fracture classification, clinicians are still required to determine appropriate operative fixation strategies ranging from anterior or posterior approaches to short or long segment fixation. This is only partially addressed in the current system with modifiers such as ossifying bone disease suggestive of long segment constructs whilst lack of complicating factors or non-junctional levels may be appropriate for shorter segment constructs. 9
What is reassuring however is that that international expert consensus supported the current TL AO SIS.
46
Indeed, there was a stepwise increase in the rate of surgical stabilization rather than conservative management as the category escalated from type A to type B and type C. Furthermore, thoracolumbar A4 complete burst fractures are also perceived as more likely to require fixation than the A3 incomplete burst fracture morphology (68.2% vs 30.9%, P < 0.001).
46
Finally, our clinically based study determined that a modifier indicating indeterminate ligamentous injury increased the rate of operative management when comparing type B and C injuries to type A3/A4 injuries (OR 39.19, 95% CI 20.84-73.69, P < 0.01 vs OR 27.72, 95% CI 14.68-52.33, P < 0.01).
46
This is consistent with the previously discussed literature. In light of this, our study concluded that this AO Spine classification introduces fractures in a rational hierarchical manner which correlates with real world management decisions (Figure 5).
46
Thoracolumbar Injury Classification System Treatment Algorithm Based Upon a Flowchart Initially Based Upon Injury Morphology, Then Anterior or Posterior Tension Band Involvement and Finally the Specific Subtype. Neurological Status and Modifiers May Also be Taken Into Consideration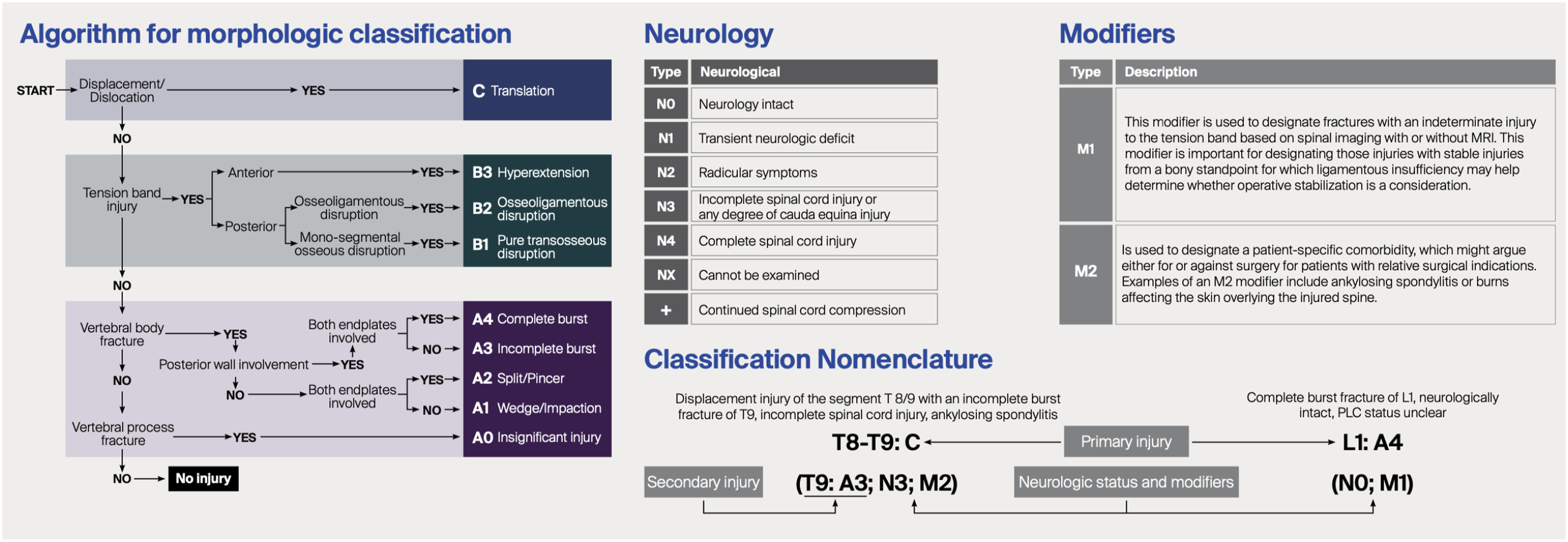
Conclusions
The AO Thoracolumbar Injury Classification System is a celebration of existing historical schemes and advances our understanding of trauma to this important region. Despite success in its validation and translation into a scoring system to communicate whether injuries require operative or non-operative management, further development in appreciating the nuances of these complex injuries is still required. The management of burst fractures in neurologically intact patients remains an area of clinical equipoise which demands further research.
Supplemental Material
Supplemental Material - Thoracolumbar Fractures: Historical Systems and Advancements With the AO Spine Classification
Supplemental Material for Thoracolumbar Fractures: Historical Systems and Advancements With the AO Spine Classification by Barry Ting Sheen Kweh, Alexander R. Vaccaro, Gregory Schroeder, Jose A Canseco, Maximilian Reinhold, Mohamed Aly, Sebastian Bigdon, Mohammad El-Skarkawi, Richard J. Bransford, Andrei Fernandes Joaquim, Harvinder Singh Chhabra, Emiliano Vialle, Rishi M. Kanna, Charlotte Dandurand, Cumhur Öner, and Jin Wee Teein Global Spine Journal
Footnotes
Acknowledgements
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma, a focused group of international Trauma experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research.
ORCID iDs
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine, AO Network Clinical Research through the AO Spine Knowledge Forum Trauma.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.