
Abstract
Study Design
Cross-sectional study.
Objectives
Normative data describing the relationship between spinopelvic and femoroacetabular alignment is not thoroughly described in the literature; we aimed to explore potential associations in healthy young adults.
Methods
Volunteers with no hip or spine pathology were recruited for this study (N = 395.) Full body EOS scans were used to obtain 3D reconstructions of participants’ acetabula and femurs. Associations between femoroacetabular parameters (acetabular anteversion (AA), acetabular inclination (AI), femoral version (FV)) and spinopelvic parameters (pelvic incidence (PI), pelvic tilt (PT), lumbar lordosis (LL)) were tested using multiple linear regression analyses.
Results
We included 395 healthy volunteers (mean age 28.90 ± 5.1; 57% female; mean BMI 24.8 ± 4.2). Linear regression analysis demonstrated that AA is associated with PI, PT, age, sex and weight (R2 = 0.381). AI is largely conserved across participants, but associated with FV, PT, age, height and weight (R2 = 0.0949).
Conclusion
We identified that normative relationships exist between acetabular orientation and spinopelvic parameters; however there remains residual variability in AA that is not comprehensively predicted by spinopelvic parameters alone. This knowledge provides the foundation for understanding changing alignment with normal aging and compensatory mechanisms. This will ultimately help guide restoration of pre-degenerative acetabular orientation in THA and spinopelvic alignment in spinal fusion in order to optimize patient care and reduce the need for revision surgery.
Background
Spinopelvic alignment is commonly defined by pelvic incidence (PI), a morphologic, non-positional parameter that describes the position of the sacrum within the pelvis and forms the basis for the alignment of the mobile spine. The PI has an intimate, morphologic relationship to the lumbar spine and together with LL, spinopelvic parameters can be used to describe patterns of overall sagittal plane alignment using Roussouly morphotype. Roussouly morphotype characterizes variation in sagittal spinopelvic alignment as follows: Type 1 has low sacral slope (SS, <35°), with short LL, Type 2 has low SS (<35°) and straight LL, Type 3 (most common morphotype) has SS between 35 and 45° and more prominent LL, and type 4 has high SS (>45°) and more prominent LL. 1 PI to LL mismatch of greater than 11° is considered sagittal malalignment at risk of severe disability in the spinal deformity population, but PI-LL relationships in normal populations have not been comprehensively described. 2 Increasing PT can help compensate for mismatches between PI and LL, allowing the patient to remain within the cone of economy and minimize energy expenditure 3 while mobilizing. Additional compensatory mechanisms include maximizing hip extension, sometimes to the point of pseudo-flexion developing. This causes difficulty in determining the pre-compensatory alignment of the acetabulum (acetabular anteversion (AA) and acetabular inclination (AI)), which has implications for surgical planning in spine deformity patients who have concomitant hip osteoarthritis.
Spinopelvic alignment is also important to consider in patients with symptomatic femoroacetabular impingement (FAI). 4 Femoral pathology including FAI and abnormal femoral torsion have been postulated to contribute to low backpain, 5 and patients with stiff spine deformities have been observed to have increased femoral retroversion. 6
Better understanding of normal spinopelvic alignment is key for care of all patients where the hip-spine relationship may contribute to pain and dysfunction. Previous study of normal pelves demonstrate some correlation between proximal femoral and acetabular alignment, but no consistent relationships have been identified. 7 Understanding the relationship that acetabular orientation has with spinopelvic alignment could help guide the process. There is currently a lack of evidence on this topic and normative relationships have yet to be described
The goal of this study was to explore potential associations between spinopelvic and femoroacetabular parameters in healthy young adults to establish normative alignment relationships prior to the onset of degeneration and deformity. We hypothesized that significant associations would be present, with possible differences according to sex.
Methods
Study Design
Written informed consent was obtained from each participant. The study was approved by the institutions Conjoint Health Research Ethics Board at the University of Calgary (Approval REB19-1912). A single-center, cross-sectional study of healthy individuals between the age of 20 and 39 years-old was carried out. Between March 2018 and March 2021, 500 participants were recruited to obtain simultaneous, orthogonal, biplanar radiographs of the entire skeleton using stereoradiographic 2D EOS imaging (Paris, France). 8 Basic health and demographic information was collected. All participants completed Oswestry Disability Index (ODI) questionnaire prior to imaging. Each participant’s height and weight were measured at the time of presentation for imaging. This study was approved by the local Conjoint Health Research Ethics Board (REB17-1800) and by the Provincial Health Services Research Department to allow access to participant specific data.
Exclusion Criteria and Participant Demographics.
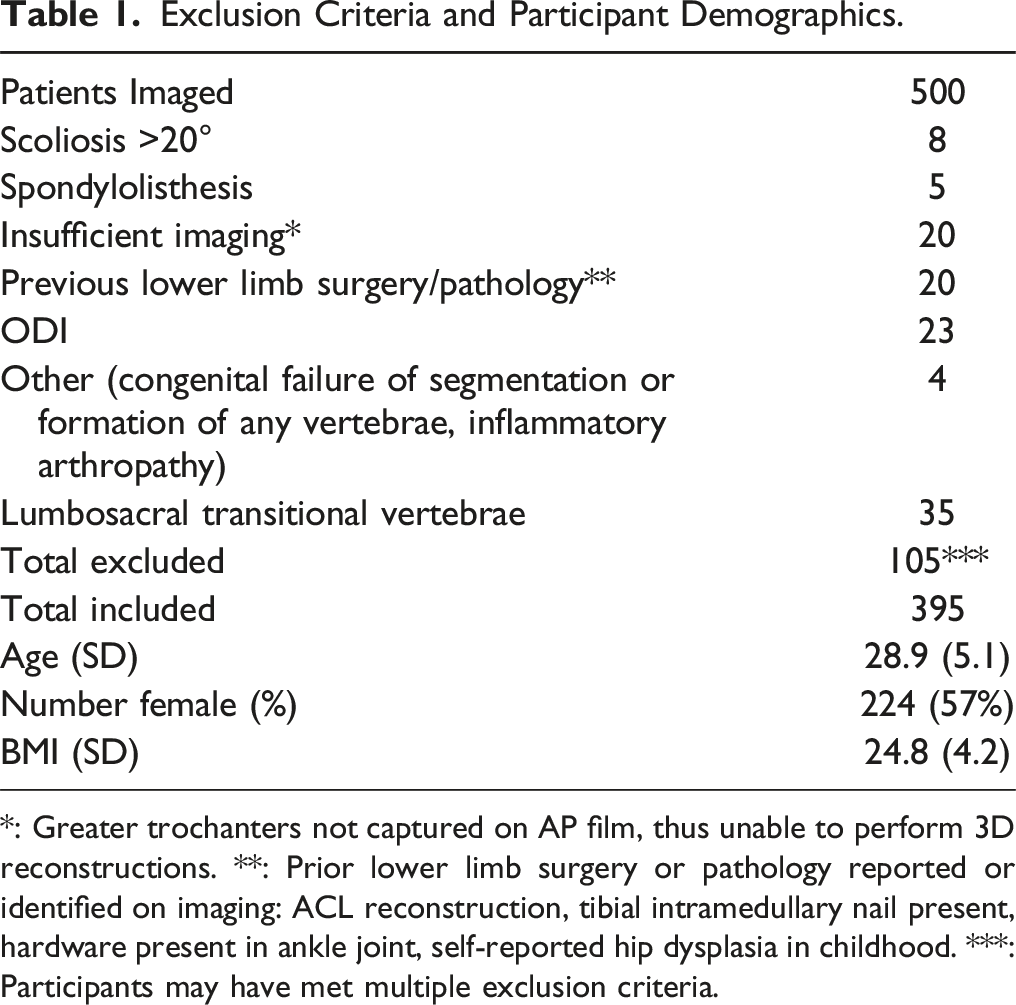
*: Greater trochanters not captured on AP film, thus unable to perform 3D reconstructions. **: Prior lower limb surgery or pathology reported or identified on imaging: ACL reconstruction, tibial intramedullary nail present, hardware present in ankle joint, self-reported hip dysplasia in childhood. ***: Participants may have met multiple exclusion criteria.
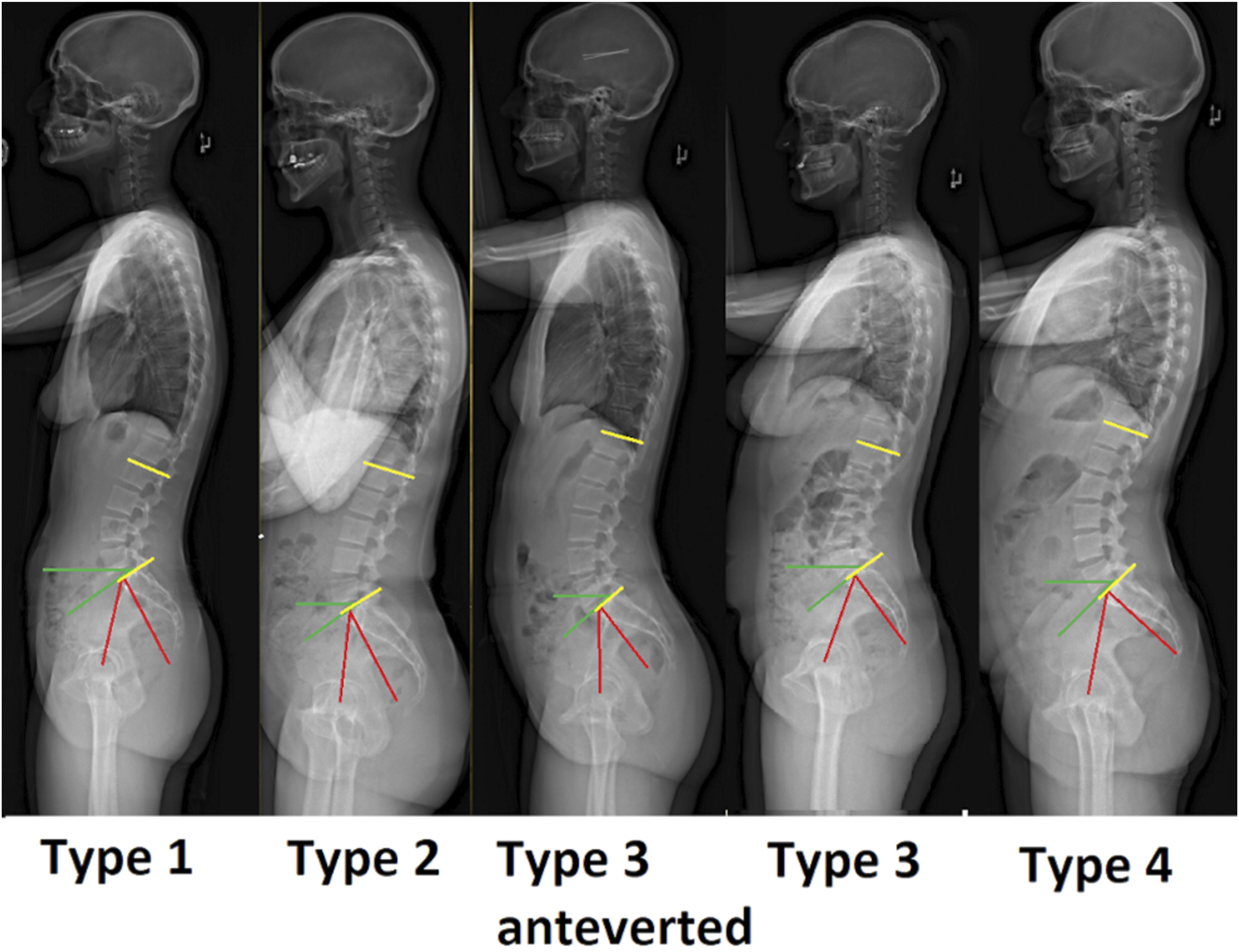
Representative images demonstrating each Roussouly morphotype from the current study cohort. Red: pelvic incidence (PI). Green: sacral slope (SS). Yellow: lumbar lordosis (LL).
Imaging Protocol
Images were obtained under standardized conditions; subjects were instructed to stand without leaning on any support structures, with the feet parallel in an offset double-leg-stance with both knees extended and the patellae pointing forward. Arms were raised to ensure the hands were outside the field of view. Images were obtained from the top of the skull to the ankle joint; if a participant was too tall, images were coned to include the external auditory meatus down to ankle joint. Acquired images were stored on the Keops web application (SMAIO, France). Images were initially segmented using Keops semi-automated software and accuracy of each point was confirmed manually
12
(Figure 2). For the purposes of this study, parameters from the Keops image analysis used were lumbar lordosis from L1-S1 and Roussouly morphotype. Sample sagittal (A) and coronal (B) Keops semi-automated image segmentation showing user-defined anatomic landmarks.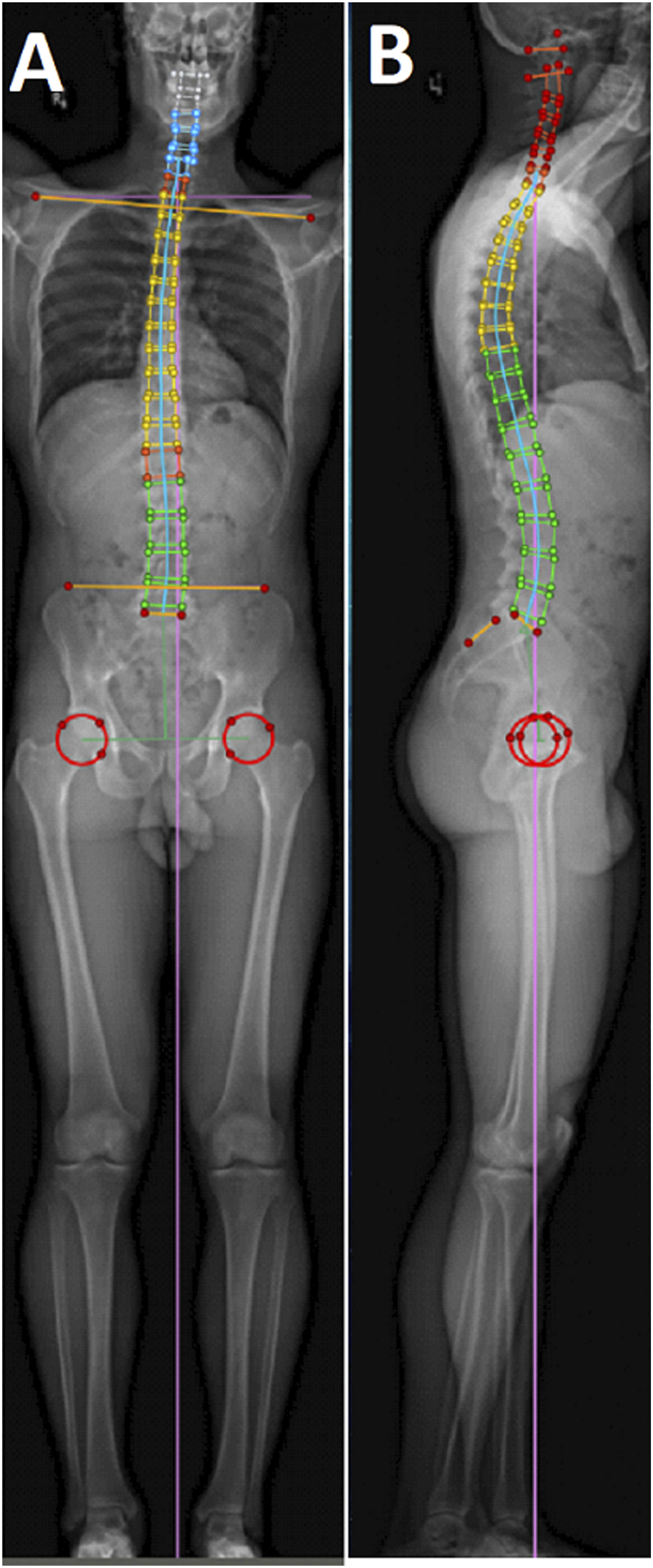
Three-Dimensional Reconstruction
3D reconstructions of the pelvis, acetabulum, and lower extremities were rendered by EOS with sterEOS 3D software (EOS Imaging, Paris, France, Figure 3A). The model generated automated measurements of pelvic incidence (PI), sacral slope (SS), pelvic tilt (PT), acetabular anteversion (AA), acetabular inclination (AI), femoral version (FV), and femoral neck-shaft angle (NSA) using a previously validated technique
12
Figure 3B (adapted from Refs. 13,14). For this study, AA and AI in the “patient vertical plane” (PVP) were used and were measurements of anatomic AA (defined by EOS as angle between a line orthogonal to the acetabular axis and the intersection line of the acetabular cup plane and the patients axial plane) and radiographic AI (acetabular axis angle with the longitudinal plane through the acetabulum).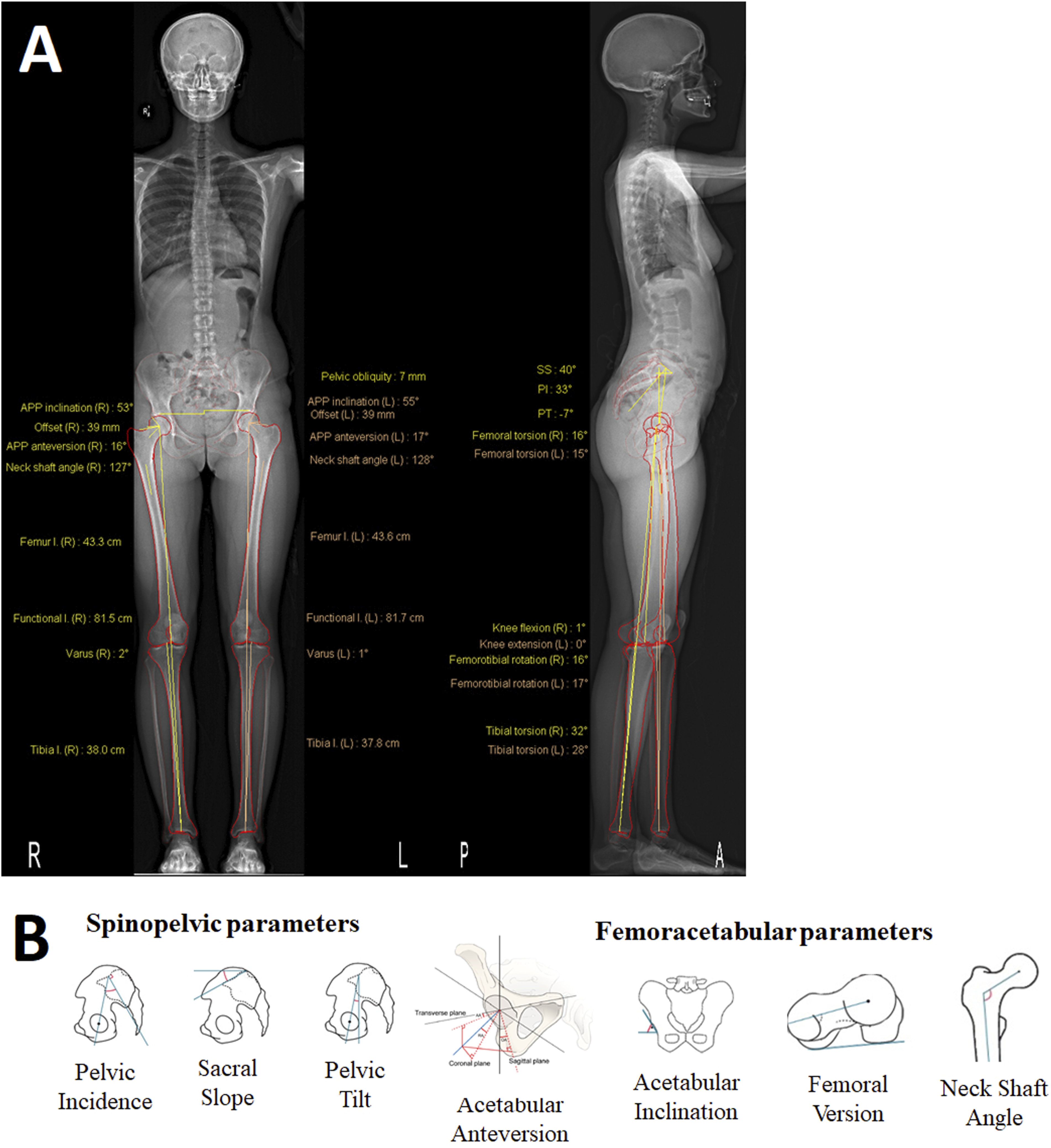
Statistical Analysis
Statistical analysis was performed using SPSS (IBM Corp., Chicago, USA, version 28.0.0.0.) All variables are presented as mean (SD). Unpaired Student t-tests were used to compare parameters between female and male subjects. One-way between subjects ANOVA was used to compare parameters between Roussouly morphotypes followed by Tukey post-hoc testing if a significant main effect was found. Bilateral parameters (left and right sides of one individual) were compared using paired t-tests. AA and AI were statistically significantly different between sides, however left and right values for each participant were averaged for subsequent analysis, due to the small absolute numerical difference. Unadjusted and adjusted associations between acetabular orientation and anthropomorphic, spinopelvic and femoroacetabular parameters were tested for using univariate and multiple linear regression analyses, respectively; all spinopelvic and femoroacetabular variables, age, and sex were initially included. Variables were sequentially removed to obtain the best fit model, as determined by the highest adjusted R2 value, with consideration of clinical relevance and unadjusted relationships between parameters and AA or AI. The model was also tested with outliers (defined as those below (Q1 – 1.5 × IQR) or above (Q3 + 1.5 × IQR) removed. 15 All tests of significance were 2-tailed and P-values <.05 were considered significant.
Results
Summary of Parameters
Average Spinopelvic and Femoroacetabular Parameters for Population and by Sex.
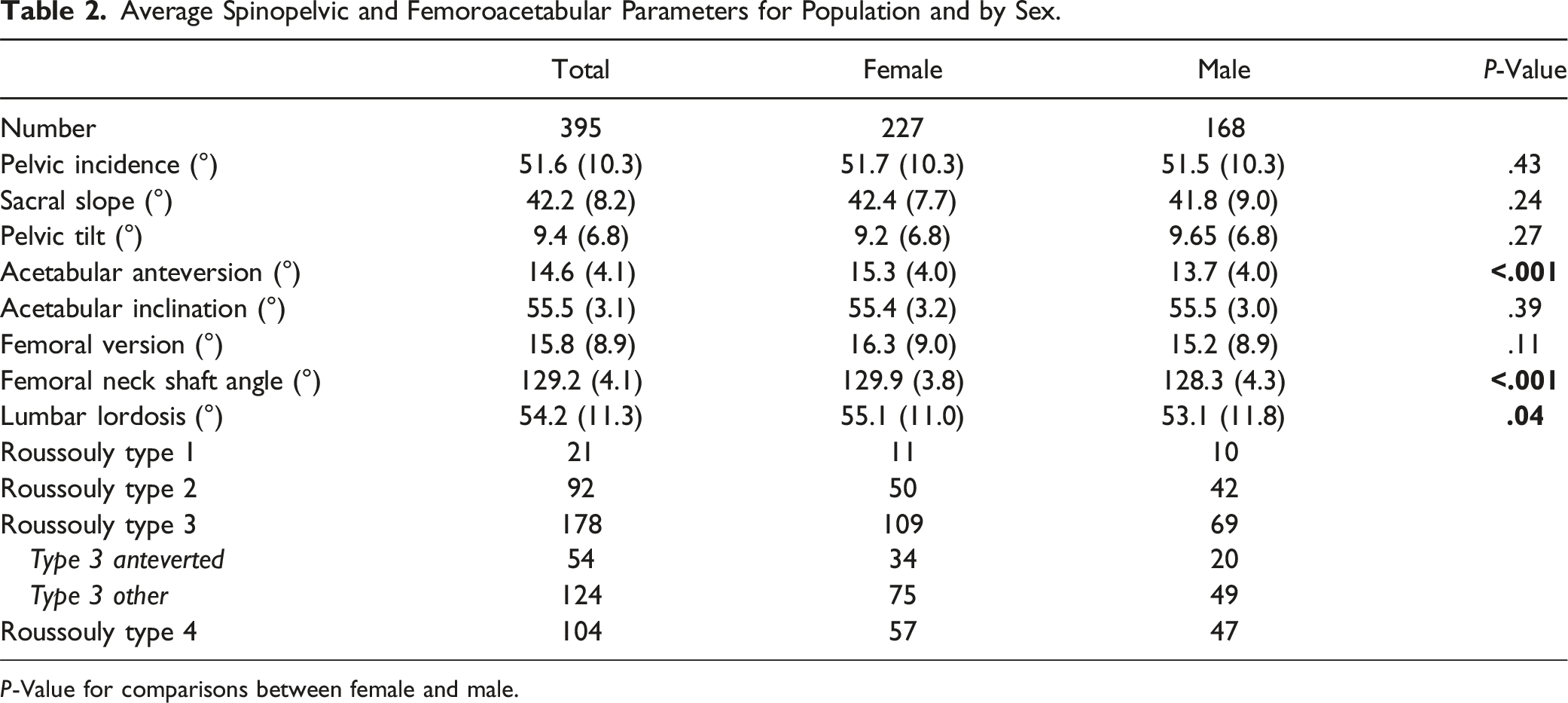
P-Value for comparisons between female and male.
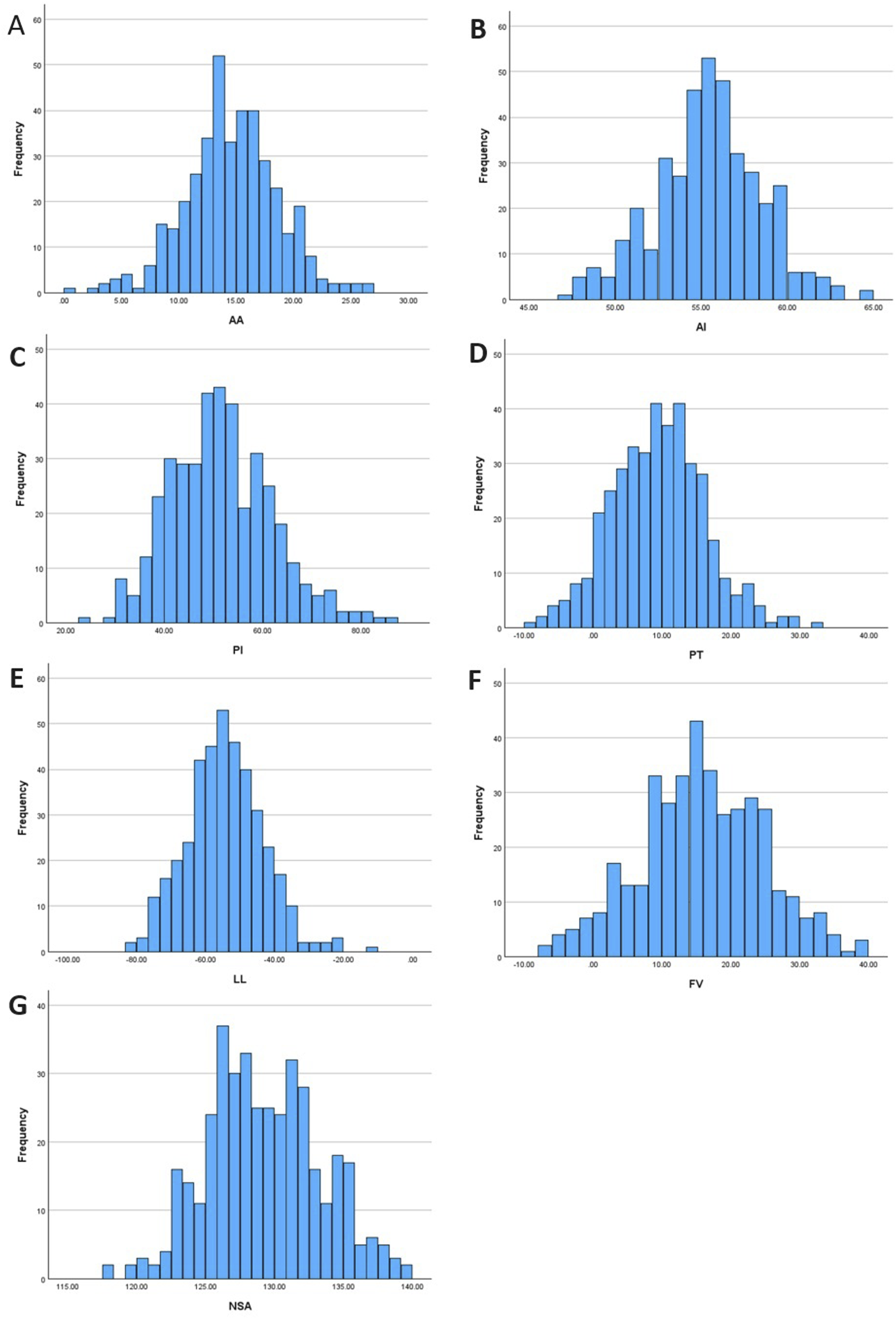
Confirmation of normally distributed data for key parameters. (A) Acetabular anteversion (AA), (B) Acetabular inclination (AI), (C) Pelvic incidence (PI), (D) Pelvic tilt (PT), (E) Lumbar lordosis (LL), (F) Femoral version (FV).
To test for bilateral differences, the paired t test found that AA was significantly higher on the left side (mean difference 0.56°, P < .001), while AI was significantly higher on the right side (mean difference 0.66°, P < .001). Distributions in differences are shown below (Figure 5). NSA and FV showed no significant difference between sides (P = .22, .06 respectively). Right vs left AI (A) and AA (B) difference in degrees.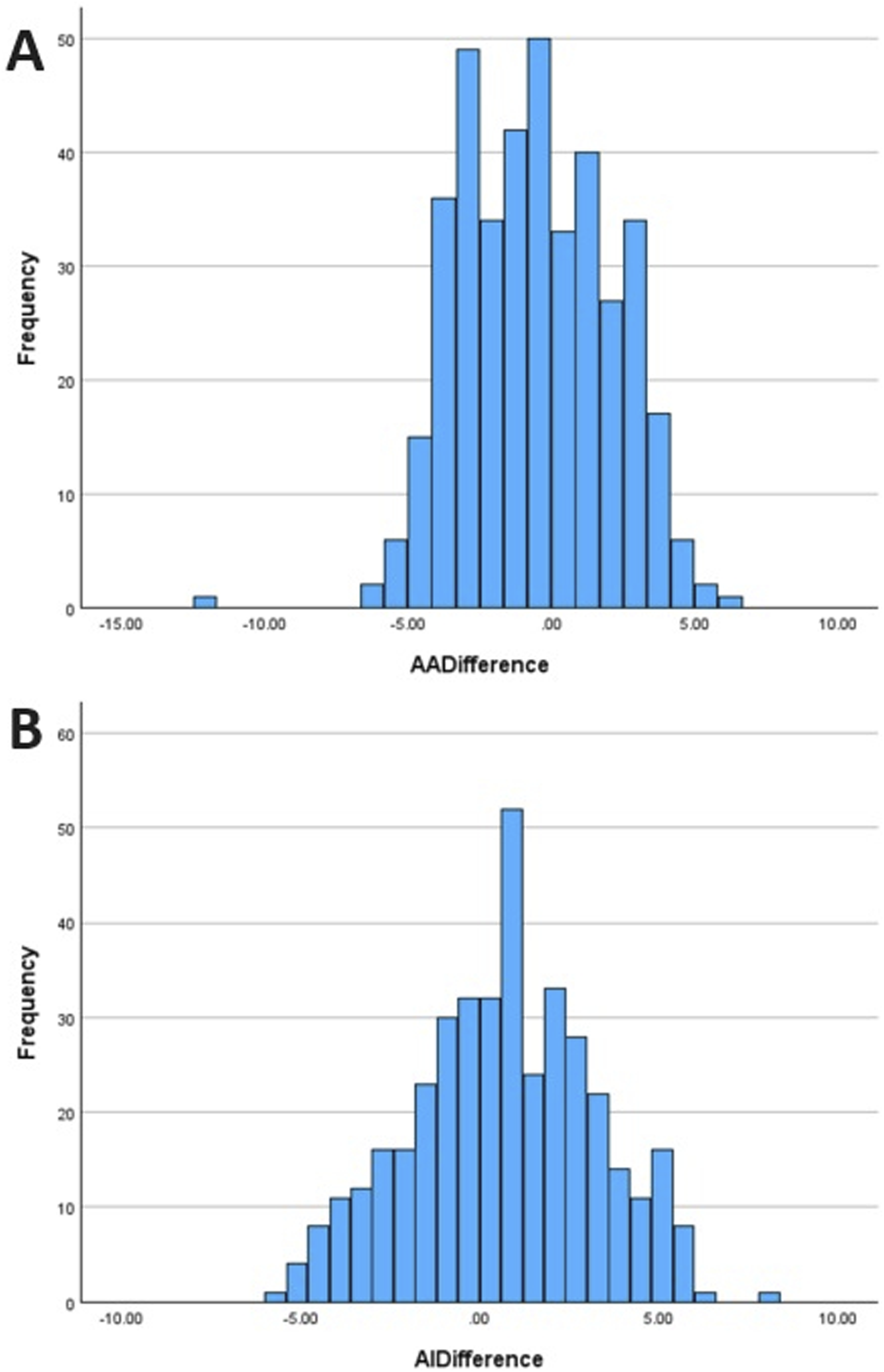
Regression Analysis
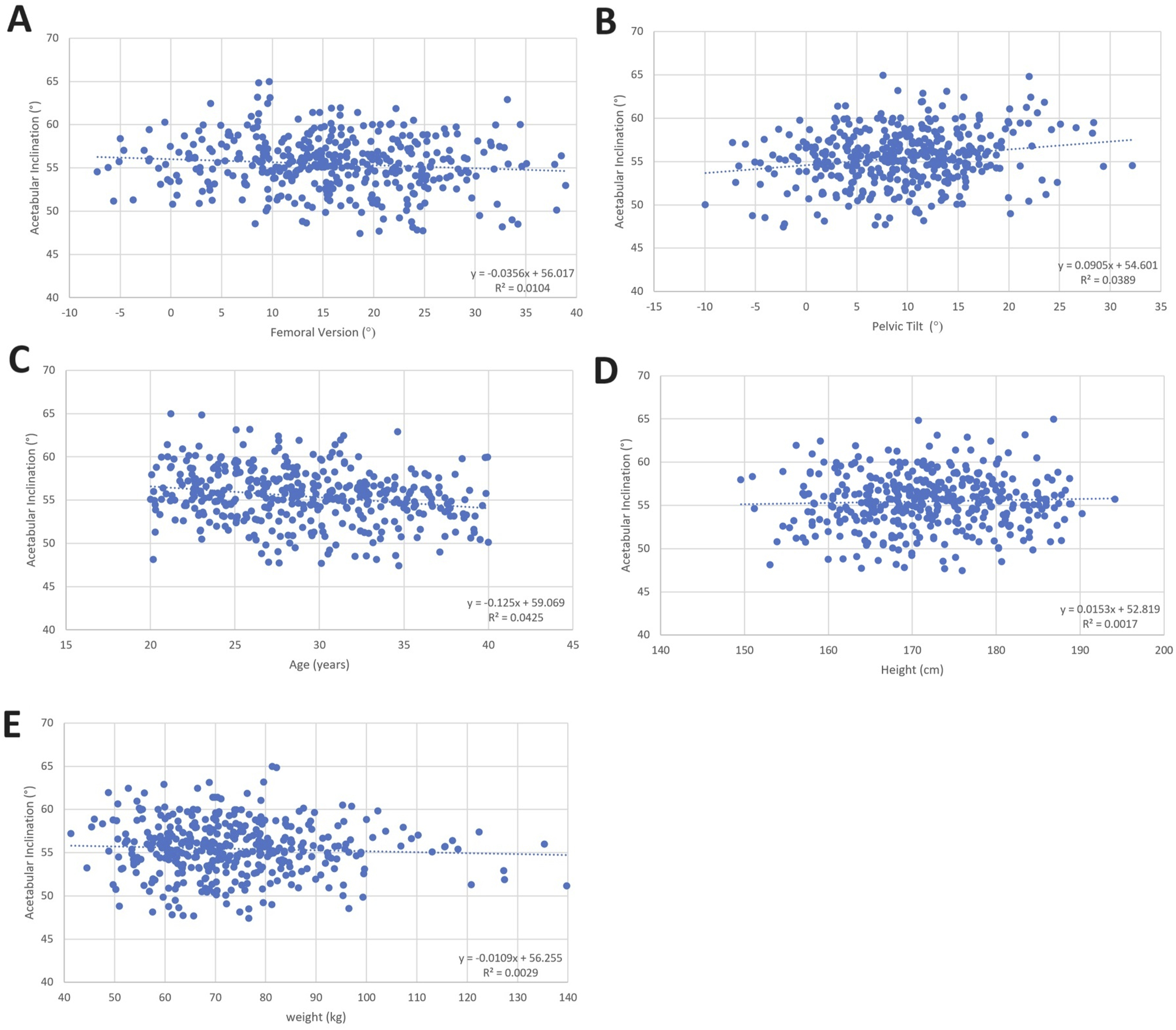
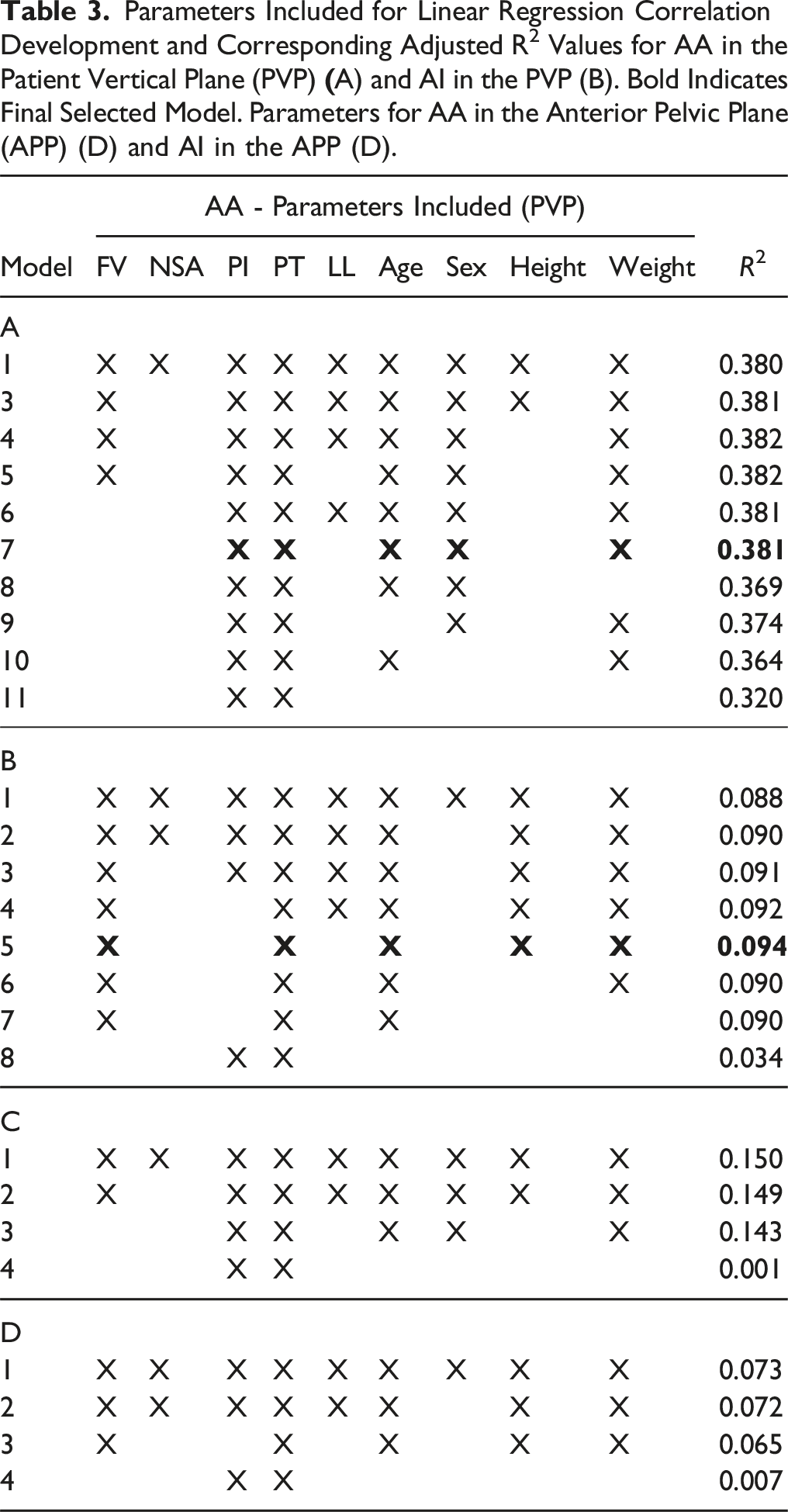
For visual clarity, unadjusted linear relationships of the significant associations from the regression analysis are shown for AA (Figure 6) and AI (Figure 7). A summary of the linear regression model development for correlation of AA and AI and spinopelvic and femoroacetabular parameters is shown in Tables 3A and 3B below. Unadjusted comparisons for AA and AI as a function of parameters omitted from final model shown in Appendix Figures 9 and 10 respectively. When the analysis was repeated with AA and AI obtained in the anterior pelvic plane (APP, N = 370 due to some images having the anterior superior iliac spine excluded), the R2 values decreased significantly (Tables 3C and 3D). Unadjusted comparisons showing significant associations of acetabular anteversion (AA) in final regression model. (A) AA vs PI, (B) AA vs PT, (C) AA vs age, (D) AA vs weight. Line of best fit and linear equation shown inset. Unadjusted comparisons showing significant associations of acetabular inclination (AI) based on final regression model. (A) AI vs FV, (B) AI vs PT, (C) AI vs age, (D) AI vs height, (E) AI vs weight. Line of best fit and linear equation shown inset. Parameters Included for Linear Regression Correlation Development and Corresponding Adjusted R2 Values for AA in the Patient Vertical Plane (PVP) 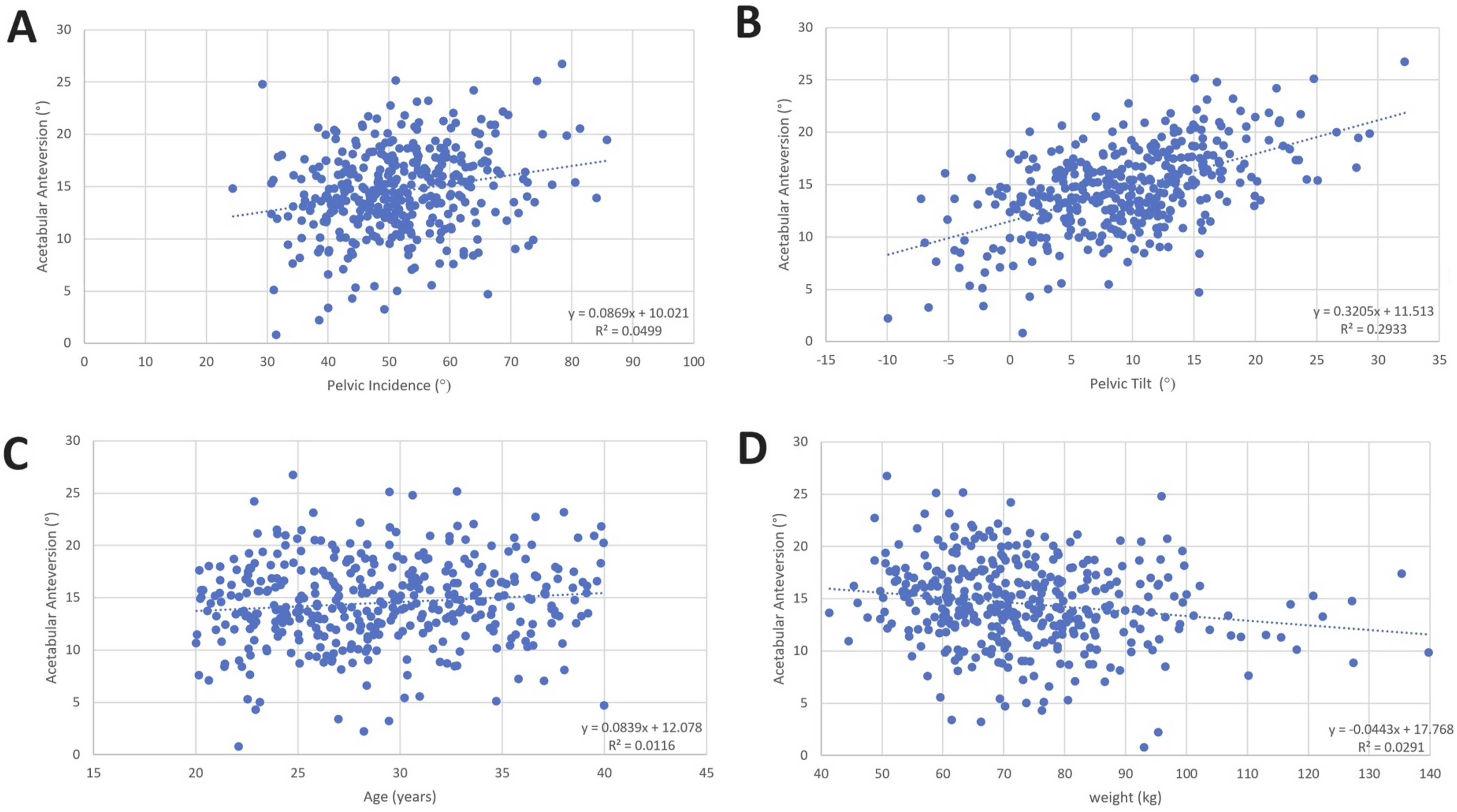
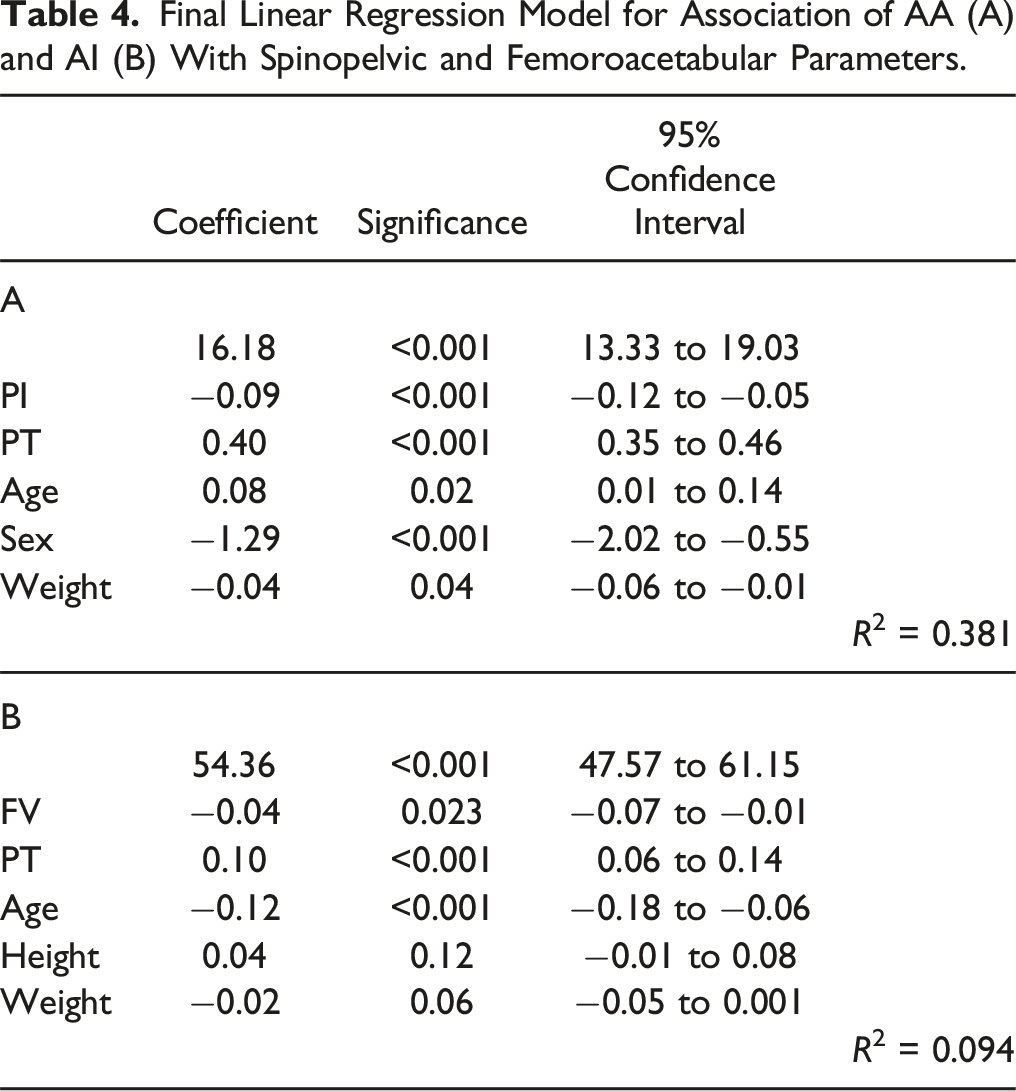
Final Linear Regression Model for Association of AA (A) and AI (B) With Spinopelvic and Femoroacetabular Parameters.
Discussion
We performed a cross-sectional study to explore relationships between spinopelvic and femoroacetabular parameters in young, healthy adults with no prior hip or spine pathology. We found that acetabular anteversion (AA) was associated with pelvic incidence (PI), pelvic tilt (PT), age, sex, height and weight, which suggests that spinopelvic and anthropometric parameters are important factors in relation to acetabular orientation. However, variability in AA is not completely explained by the spinopelvic measurements used here, suggesting that there are other factors (bony or positional) contributing to acetabular alignment that remain to be elucidated. Acetabular inclination (AI) was weakly associated with femoral version (FV), PT, age, height and weight, which suggests that acetabular orientation in the coronal plane is more highly conserved across anthropomorphic and spinopelvic/femoroacetabular variables. This insight into the spinopelvic/femoroacetabular relationship in a young healthy population is important as it provides knowledge of baseline alignment prior to degeneration or development of deformity and will be useful for improved planning of surgical deformity correction or alignment planning.
Strengths and Limitations
This study presents the largest database of young healthy individuals reported to date in the literature to our knowledge. Screening on study intake, and radiographic review for exclusion of prior lower limb or spine pathology ensures that this cohort truly represents normal anatomy and maximizes accuracy of correlations between spinopelvic and femoroacetabular parameters, prior to confounding contributions from any degenerative pathology and resulting compensatory mechanisms. While the correlations identified using this large dataset are statistically significant and provide insight into important relationships, the magnitude of correlations is small. This likely reflects the complexity of these anatomic/functional relationships.
Three-dimensional EOS reconstruction is an established method for assessment of spinopelvic and femoroacetabular parameters. Furthermore, Keops software has been shown to be an accurate methodology for measuring alignment in the coronal and sagittal planes. 12 Images for the current study were obtained in a single, upright stance, although PT is known to be positional. 16 Future work using this technology could include assessment of normal spinopelvic mobility. In this study, measurement of participants’ acetabular orientation in the “patient vertical plane” (PVP - vertical plane passing through centers of both acetabulae 13 ) were used for analysis, not the anterior pelvic plane (APP – plane through bilateral anterior superior iliac spines (ASIS) and pubic symphysis). APP tilt (more commonly used in the hip literature) and PT (more commonly used in the spine literature) are strongly correlated with each other. 17 Thus, using the AA measured in the PVP allows assessment of spinopelvic alignment in the sagittal plane to be assessed by PT alone, not confounded by the APP already having taken sagittal tilt of the pelvis into account; we believe that this explains why the results presented in the APP demonstrate weaker relationships in this study, as the tilt of the pelvis is already accounted for when the APP is used. Furthermore, from a clinical applicability standpoint 18 reliability of the APP to provide a reference for AA has been questioned, 19 and errors in identifying bony landmarks can significantly alter definition of the APP 20 Finally, anatomic measurements of AA as reported here (angle between acetabular axis and coronal plane) differ from the operative definition of anteversion (angle between longitudinal axis of patient and acetabular axis projected onto the sagittal plane) used by surgeons during THA. This underscores the importance of clearly defining the plane from which the acetabular orientation is measured.
Relation to Prior Literature
This study demonstrated a statistically significant difference in AA (0.56°) and AI (0.66°) between left and right sides. As this numerical difference was small, results were pooled such that correlations per overall patient could be obtained. This differs from previous, smaller studies where no statistically significant difference between right and left acetabular parameters was observed13,21; however numerical differences between AA and AI from side to side were similar to those observed in this study.13,22 The lower AA observed for Type 3 anteverted Roussouly morphotype participants compared to those with other Type 3 morphotypes observed here is consistent with low pelvic tilt decreasing acetabular anteversion (see Figure 6), as theoretically more anterior femoral head coverage would be required with, for example, negative pelvic tilt. Numerical values for spinopelvic parameters obtained here are within ranges of previously reported normal ranges,23-25 including values obtained for young asymptomatic patients in Korea using EOS. 26 Values for femoroacetabular parameters are also within previously published ranges. 27 Females have been reported to have higher anteversion than males, as again demonstrated in this study.13,22,28,29 The incidence of lumbosacral transitional vertebrae identified here (7%) is within the wide previously reported range of 3.3-35.6%. 30
The relationship demonstrated here between AA and spinopelvic parameters significantly extends prior relationships identified in previous significantly smaller studies. A previous CT study of 115 normal pelves in a US population demonstrated relationships between AA and FV, NSA, and gender. 7 CT studies in Asia (200 normal pelves) and France (150 normal pelves) demonstrated no relationship between acetabular orientation and spinopelvic parameters.21,31 A CT study including 36 normal hips in the UK demonstrated a decrease (as opposed to the increase seen in this study) in AA with increasing PT; similar to this study the AI was more highly conserved across a range of PT. 32 A German CT study of 138 patients demonstrated increasing AA with increasing PT. 33 A US magnetic resonance arthrogram (MRA) study in 89 patients being imaged due to hip pain demonstrated no correlation between acetabular sagittal orientation and SS, and weak correlations with PI and PT. 34 A study of CTs obtained for non-orthopaedic clinical indications in the US (N = 164, average age 59) identified a weak inverse correlation between the sacroacetabular angle 35 (a parameter representing sagittal acetabular orientation) and PI, as observed in the present study. They also identified that a decreased PI was associated with a more horizontal acetabular orientation, consistent with the result of the present study. 35 Finally, a Canadian study using CT measurements of acetabular morphology and spinopelvic parameters in 195 asymptomatic hips identified, consistent with the current study, that functional acetabular version was moderately associated with PT. 25 The relationship between AA and participant weight is novel. Acetabular anteversion decreased with increasing weight, with no relationship between proximal femoral parameters FV and NSA. Further study is required to determine the underlying mechanism of this relationship; it is possible that abdominal obesity causes anterior shift and decreased AA compensates for this. The influence of obesity on sagittal balance affects many THA and spinal deformity patients, thus it may also be important to consider body anthropomorphic parameters when planning THA or spinal fusion.
Discrepancy between this study and previously reported results is likely multifactorial. The discussed above studies used supine CT and MRA, and images were usually obtained for unrelated medical indications. Whole body EOS imaging has an advantage over these modalities as it is performed in the upright position and can therefore be used for planning realignment. In addition, it is relatively radiation sparing. 8 Furthermore, the age of patients included in the above-cited studies ranged from under 18 to over 70. It is possible that changes in alignment with age contribute to the discrepancy observed here, as PT increases and LL decreases with age. 36 Understanding changes in these relationships with aging will be key to determining appropriate acetabular component alignment in THA based on age and spinopelvic alignment. Previous studies have also included a wide range of ethnic groups, and it has previously been demonstrated that acetabular morphology can vary significantly by ethnicity 37 ; 73% of participants in this study self-reported as Caucasian. Finally, obesity has been shown to alter compensatory mechanisms in patients with sagittal spinopelvic imbalance. 38 BMI was not reported in the above-mentioned studies. The present study includes patients with a high-normal BMI (average 24.9) and demonstrates that both height and weight are factors in determination of acetabular orientation, with AA decreasing with increasing weight, while coronal orientation (AI) increases slightly with increasing height and decreases slightly with decreasing weight.
Clinical Applications
This study has implications for clinical practice in both Spine and Arthroplasty subspecialties, where better understanding of the interplay of anatomic factors can potentially contribute to improved surgical planning. Knowledge of normal spinopelvic/femoroacetabular alignment could help minimize THA dislocation rates in patients with concomitant hip and spine pathology, as discussed above. More recent investigations have suggested modified “safe zones” of acetabular orientation for adult spinal deformity patients with high PT. 39 Furthermore, understanding normative alignment may help future identification and understanding of risks to adjacent joins in malalignment and compensation; for example, the postulated risk of increased hip OA with pelvic retroversion in adult spinal deformity 40 Knowledge of normative alignment can also be used in assessment of patients with femoroacetabular impingement and other hip pathology. There are multiple factors remaining to be elucidated in defining the relationship between spinopelvic and femoroacetabular alignment. Changes in alignment with aging are a crucial next step and recalling the current cohort of subjects for future EOS imaging/analysis will enable the first longitudinal study of its kind. Extending this work to interrogate spinopelvic/femoroacetabular relationships in patients with degenerative hip or spine pathology, or patients who have undergone THA or spinal fusion will enable evaluation of predictive models of compensation. Stratifying participants by ethnicity and evaluating the effect of lumbosacral transitional vertebrae on the demonstrated relationships will help extend application of these results to a wider population. Extension of the current methodology to evaluate individualized spinopelvic mobility would further enhance prediction of appropriate acetabular positioning for a given patient.
Conclusion
This study presents relationships between spinopelvic and femoroacetabular parameters in the largest cohort of young, healthy individuals to date in the literature. Relationships between AA and PI and PT exist, but these spinopelvic alignment parameters do not fully explain variability in AA; further research is needed to elucidate morphologic and positional parameters to more comprehensively predict the alignment of the acetabular based on lumbopelvic alignment. This knowledge provides the foundation for future work pursuing the understanding of normal aging, changing alignment with degeneration, and compensatory mechanisms. Ultimately these normative data provide baseline alignment parameters and may help guide appropriate selection of acetabular orientation in THA and spinopelvic alignment in spinal fusion, improving patient care and reducing the need for revision surgery.
Supplemental Material
Supplemental Material - Normative Relationships Between Spinopelvic Alignment and Femoroacetabular Orientation: A Cross-Sectional Study
Supplemental Material for Normative Relationships Between Spinopelvic Alignment and Femoroacetabular Orientation: A Cross-Sectional study by Taryn Ludwig, Jonathan Bourget-Murray, Sarup Sridharan, Ariana Frederick, Victoria Smith, Kelly Johnston, Nathan Evaniew, Brent Edwards, Michael Asmussen, and Fred Nicholls in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Fraternal Order of the Eagles, Alberta Spine Foundation, Section of Orthopaedic Surgery, McCaig Institute for Bone and Joint Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.