
Abstract
Study Design
Systematic review and meta-analysis.
Objective
To evaluate the timing of anticoagulation in acute spinal trauma, specifically assessing the efficacy and safety of early (<48 hours) vs delayed administration for chemical venous thromboembolism prophylaxis.
Methods
A systematic search of Medline, EMBASE, Web of Science, and Cochrane was conducted through February 2023 for studies comparing early vs delayed anticoagulation in acute spinal trauma patients. Studies reporting deep vein thrombosis (DVT), pulmonary embolism (PE), major bleeding, and mortality were included. Three reviewers independently screened and extracted data. Risk of bias was assessed using MINORS and the Newcastle-Ottawa Scale. The protocol was registered on PROSPERO (CRD42023397717).
Results
Five studies, comprising a total of 13,110 patients, compared anticoagulant administration within 48 hours of trauma vs after 48 hours, reporting DVT and PE as outcomes. Early administration was associated with significantly lower odds of DVT (OR: 0.20 [95% CI: 0.17-0.25], P = .0001, I 2 = 34%) and PE (OR: 0.46 [95% CI: 0.34-0.62], P = .0001, I 2 = 0%). Four studies evaluated major bleeding as an outcome and found slightly lower odds with early initiation, though the association was not statistically significant (OR: 0.85 [95% CI: 0.66-1.09], P = .1992). Similarly, 4 studies assessed mortality, with results that were also nonsignificant.
Conclusions
The current evidence indicates that early initiation of chemical anticoagulation within 48 hours of injury in spine trauma patients is associated with favorable outcomes in preventing thromboembolic complications, without significantly increasing the risk of bleeding or mortality.
Keywords
Introduction
The American College of Chest Physicians’ Evidence-Based Clinical Practice Guidelines underscore that patients with acute spinal trauma, particularly those with concomitant spinal cord injury (SCI), are at the highest risk for suffering a deep vein thrombosis (DVT).1-3
Reports on the incidence of venous thromboembolism (VTE) following SCI vary depending on study populations and definitions. While earlier work suggested that, under conditions of impaired venous return and hypercoagulability, deep vein thrombosis (DVT) could occur in up to 49% to 100% of cases within the first 12 weeks after acute spinal cord injury - with peak incidence observed during the first 2 weeks post-injury - more contemporary studies indicate lower rates of symptomatic events. 4 For example, Piran et al (2016) reported a symptomatic VTE incidence of 11% in SCI patients. 5 Similarly, Godat et al (2023) reported thrombotic events in 9.6% of SCI patients, consisting of 8.7% DVT and 0.9% pulmonary embolism (PE). 6
In contrast, estimates of symptomatic DVT rates were documented between 5% and 26%7,8 in patients without SCI. Nevertheless, contemporary data on the prevalence of venous thromboembolism (VTE) in patients with nonoperative spinal trauma without SCI remains controversial. Avila et al analyzed the Healthcare Cost and Utilization Project’s Nationwide Readmissions Database (NRD), identifying 41,337 patients with acute nonoperative spinal fractures, and found that approximately 8% developed symptomatic VTE, DVT, or pulmonary embolism (PE) within 6 months post-injury. 9 However, this incidence rate likely underestimates the true thromboembolic burden, as only symptomatic patients are generally readmitted, and the analysis does not account for the substantial number of patients who were already on anticoagulation therapy.
Despite the thromboembolic burden in patients with acute spinal trauma with and without SCI, heterogeneity exists in VTE prophylaxis practice patterns among surgeons. For example, in Ploumis et al’s survey on thromboprophylaxis in spinal trauma, no mechanical or chemical prophylaxis was routinely used preoperatively by ∼75% of surgeons.10-12 This observation is consistent with more recent data, which continue to demonstrate considerable variability in both the prescription and timing of VTE prophylaxis in trauma patients overall.6,13
One possible explanation for the variability in practice patterns and reluctance to utilize VTE chemoprophylaxis in the early stages of injury is the increased risk of major hematologic complications.14,15 However, studies by Kim et al in 206 operatively fixed patients following spine fractures and Zeeshan M et al in 3,556 patients following operative spine trauma, reported no difference in bleeding or neurologic complications in patients receiving chemoprophylaxis regardless of the timepoint of initiation.16,17 A clear discordance exists between what is considered safe in the literature and current practice patterns, likely stemming from a scarcity of aggregate evidence, a lack of high-quality studies, and variability in the type of anticoagulation, timing of administration, and the delineation of appropriate patient populations that would benefit from prophylaxis within the literature.
This systematic review and meta-analysis aimed to synthesize contemporary evidence on the timing of anticoagulation in spinal trauma. Specifically, it evaluated whether early (<48 hours) VTE prophylaxis is warranted and whether efficacy or safety differences exist between early and late administration of chemoprophylaxis.
Methods
A systematic review of hematologic complications associated with anticoagulation following spinal trauma was conducted in adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al). 18 A professional medical librarian conducted a comprehensive search of Medline (OVID), EMBASE (Elsevier), Web of Science Core Collection (Clarivate), and Cochrane Central Register of Controlled Trials (Wiley) from 12/22/2022 to 2/6/2023. The search was restricted to English and foreign-language papers with available English translations. Databases were queried for studies addressing spinal injuries, fractures, and trauma in conjunction with anticoagulation strategies.
Inclusion and Exclusion Criteria
Inclusion criteria were defined as follows: peer-reviewed articles evaluating the timing of anticoagulation following nonoperative or operative spinal trauma, written in English, with ≥10 patients. Included studies had to provide comparisons between early (<48 hours) and delayed (>48 hours) anticoagulation initiation and focus on adult populations with a minimum of a 30-day follow-up.
Exclusion criteria included case reports, studies with fewer than 10 patients, pediatric populations, non-comparable interventions, prophylaxis-only studies, or studies lacking safety outcomes.
Identified studies were processed using screening software, with duplicates removed. MA and DY screened titles and abstracts to assess eligibility; full texts of articles passing initial screening were subsequently reviewed by MA, DY, KM, and SM. Disagreements during the review process were resolved by consensus. Screening was performed using Covidence (Veritas Health Innovation), a systematic review management software.
Peer-reviewed articles comparing the timing of chemoprophylaxis for thromboembolic prevention in acute spinal trauma were included. The target population comprised adults with a minimum 30-day follow-up. While the acute spine trauma period was defined as within 90 days of injury, all included studies ultimately focused on patients within 30 days post-trauma.
Outcomes
The outcomes of interest were DVT, PE, major bleeding (i.e., hemoglobin decrease of ≥2 g/dL, transfusion of ≥2 units, retroperitoneal, intracranial, epidural, or other intraspinal bleeding, or any bleeding requiring cessation of treatment, consistent with previously published definitions of major bleeding), and all-cause mortality. 19
Methodologic Quality
This study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al). 18 The Methodological Index for Non-Randomized Studies (MINORS) was used to evaluate the quality of retrospective, nonrandomized observational studies. The study design was documented a priori and registered on PROSPERO (CRD42023397717).
Statistical Analysis
This study aimed to compare early vs delayed administration of chemoprophylaxis following spine trauma. Given the limited literature and direct comparisons on this topic, a 48 hours cut-off was used based on findings from existing studies. Studies using alternative time cut-offs were discussed but excluded from the meta-analysis. A meta-analysis was performed only if more than 2 studies were available for each comparison of interest. Categorical study characteristics were summarized using counts and percentages. The effect of timing on outcomes was evaluated using odds ratios (ORs), with outcomes pooled using the Mantel-Haenszel method in a fixed-effect model. Forest plots were generated to summarize the findings, and funnel plots to assess the presence of publication bias. A sensitivity analysis was conducted to assess the robustness of the synthesized meta-analysis results by excluding from the analysis one study at a time. Statistical heterogeneity was assessed using the I 2 and Tau2 statistics. All analyses were performed using R version 4.2.3 (R Core Team, Vienna, Austria) with the meta package version 6.5- 0.
Results
The systematic review identified 2,948 records through multi-database searches: OVID MEDLINE (n = 680), Embase (n = 1,375), Web of Science (n = 819), and Cochrane (n = 74). A detailed search strategy is available in Supplemental Digital Content 1. After removing 1,000 duplicates, 1,948 unique records remained for screening. Of these, 1,845 were excluded based on titles and abstracts, leaving 103 full-text articles for further assessment.
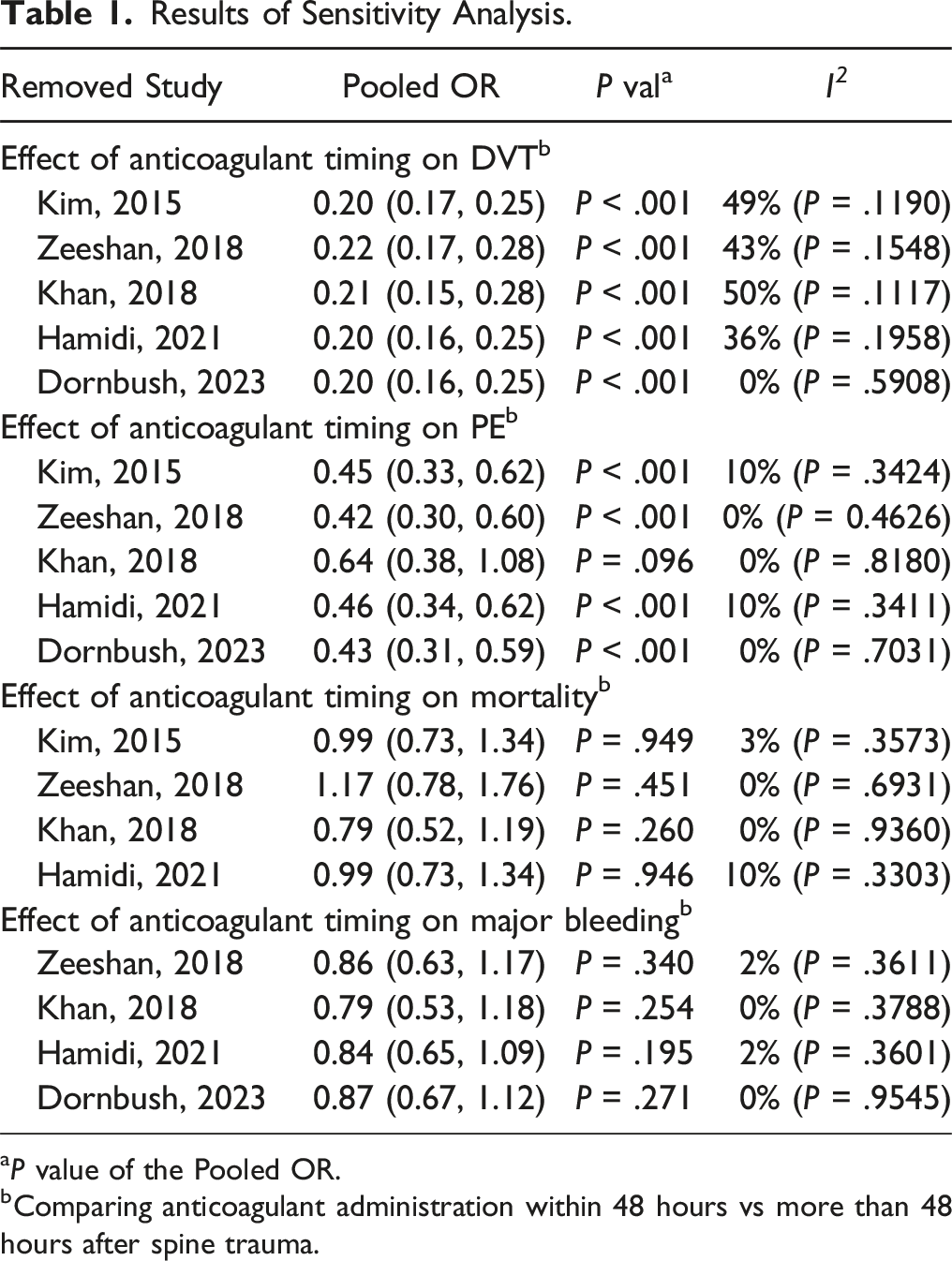
During the full-text review, 94 articles were excluded for the following reasons: 30 involved the wrong patient population, 12 had inappropriate study designs, 12 did not report relevant outcomes, 17 used an incorrect comparator, seven involved a different intervention, and 16 focused solely on efficacy without addressing safety. Ultimately, 9 studies met the inclusion criteria, of which 5 were included in the final analysis Figure 1. Table 1 shows the sensitivity analysis results conducted to ensure the robustness of the meta-analysis results. Selection of studies. Results of Sensitivity Analysis. aP value of the Pooled OR. bComparing anticoagulant administration within 48 hours vs more than 48 hours after spine trauma.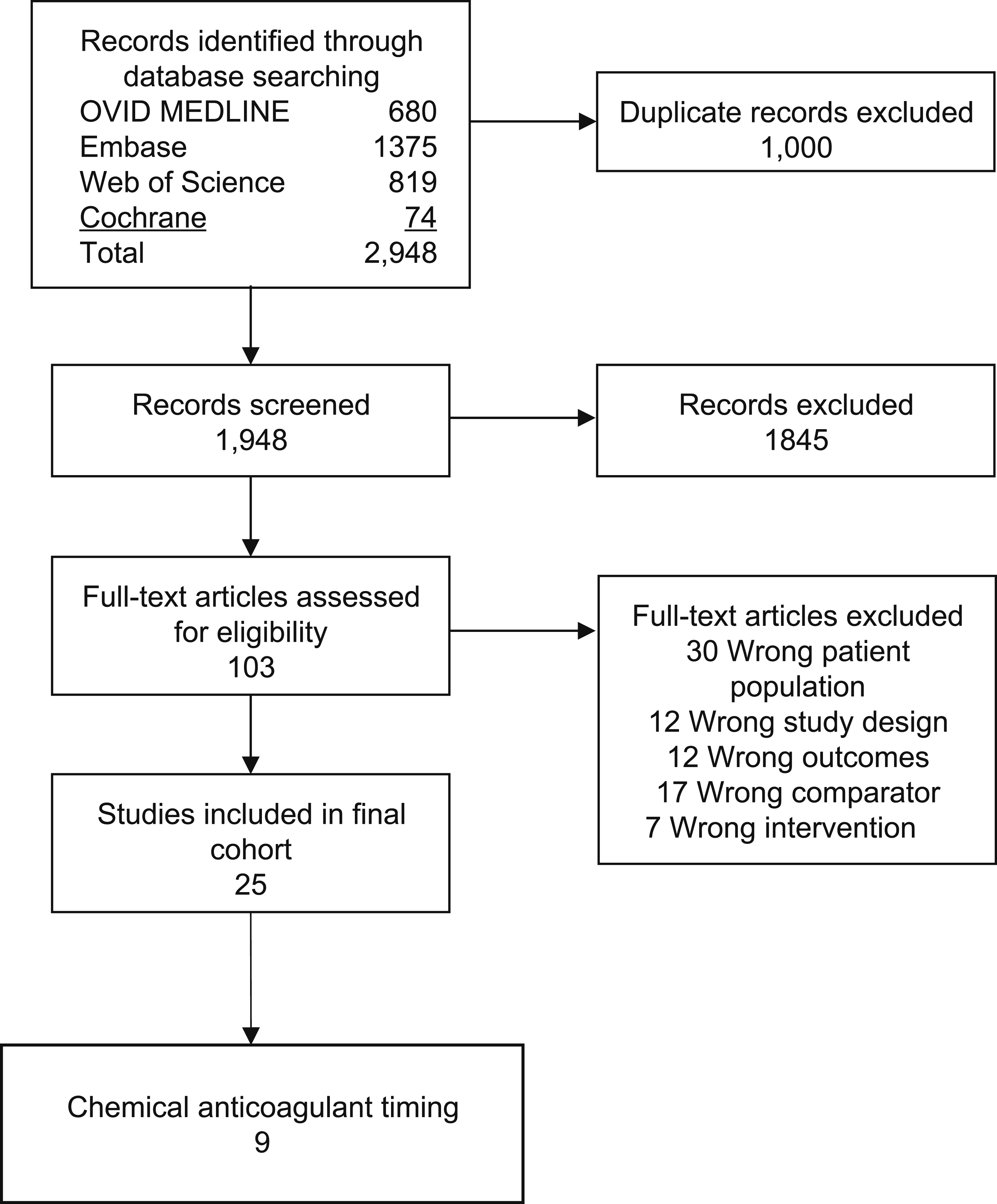
In the methodological evaluation using the MINORS assessment, all included studies scored between 16 and 17, reflecting a moderate to high overall methodological quality (Supplemental Digital Content 2). 20 The overall level of evidence for this systematic review was rated as 2 according to the Oxford Centre for Evidence-Based Medicine 2011 levels of evidence. 21
Administration of Chemical Anticoagulation Within 48 hours of Spine Trauma is Associated with Lower DVT & PE Incidence Compared to Administration After 48 hours
First, we analyzed the impact of administering chemical anticoagulation within 48 hours of spinal trauma compared to initiation beyond 48 hours on DVT incidence (Figure 2). This meta-analysis included 5 studies, encompassing 6,617 patients in the “early anticoagulation administration” group and 6493 in the “late anticoagulation administration” group. Khan et al (2018) contributed the largest weight (60.6%), followed by Zeeshan et al (2018) with 35.3%.16,22 Smaller contributions came from studies such as Dornbush (2023), Hamidi (2021), and Kim (2015), with weights of 0.2%, 3.0%, and 0.9%, respectively.17,23,24 The pooled odds ratio (OR) was 0.20 (95% CI: 0.17-0.25), indicating significantly lower odds of DVT in the early anticoagulation cohort than those receiving anticoagulation after 48 hours. Heterogeneity assessment showed a Tau2 of <0.0001, an I
2
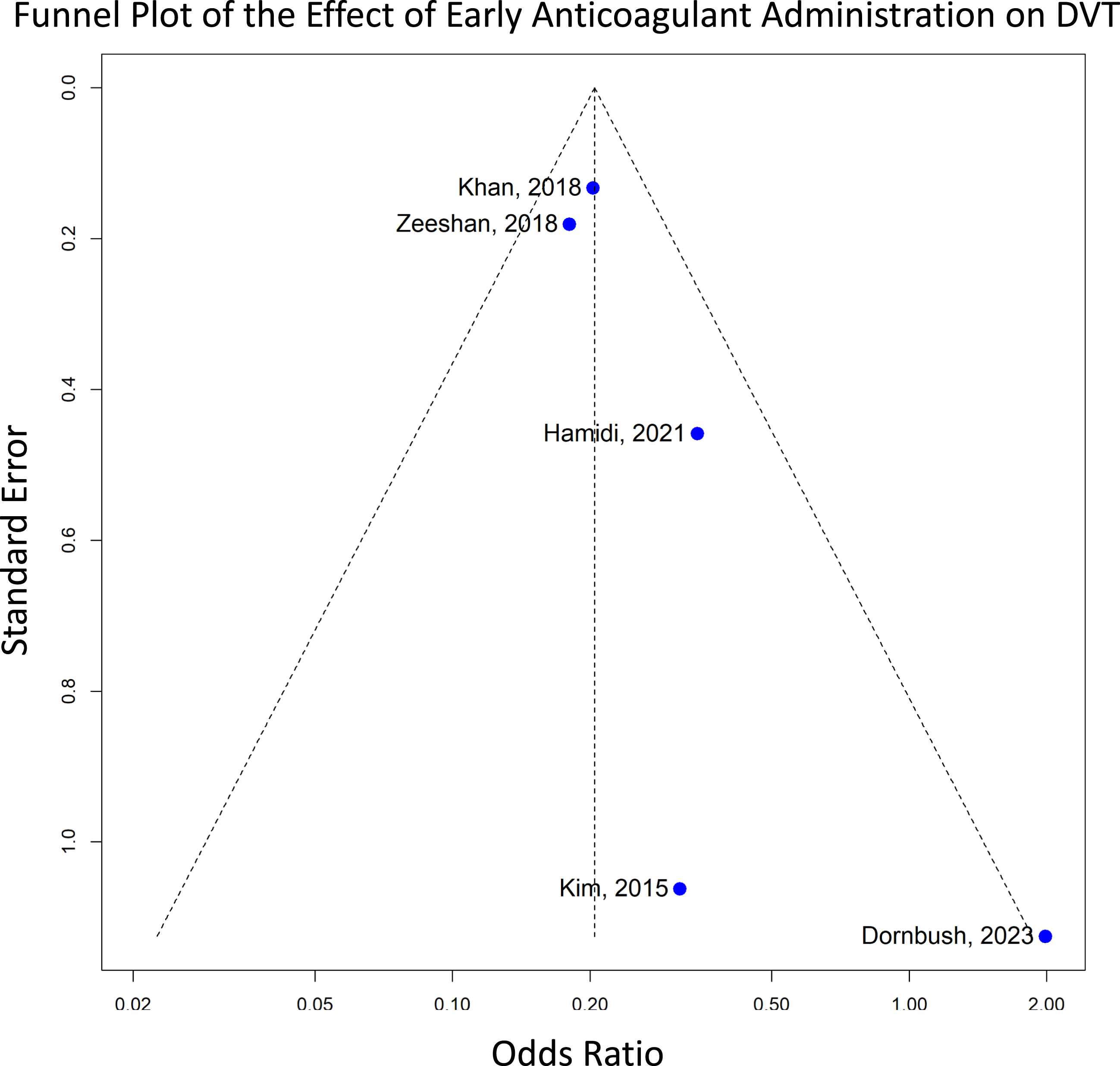
of 34%, and a Chi2 of 6.02 (df = 4, P = .20), indicating low to moderate heterogeneity. The funnel plot revealed an asymmetrical distribution, suggesting potential publication bias or small-study effects. Larger studies, such as Khan (2018) and Zeeshan (2018), aligned closely with the pooled effect size and had small Standard Errors, while smaller studies, like Kim (2015), exhibited larger Standard Errors (Figure 3).16,17,22 Forest plot for deep vein thrombosis (DVT), showing the effect sizes of included studies and the overall pooled estimate with their corresponding confidence intervals, comparing anticoagulation initiation within 48 hours (early) vs after 48 hours (late). Funnel plot assessing publication bias for DVT, where asymmetry suggests potential publication bias in the included studies.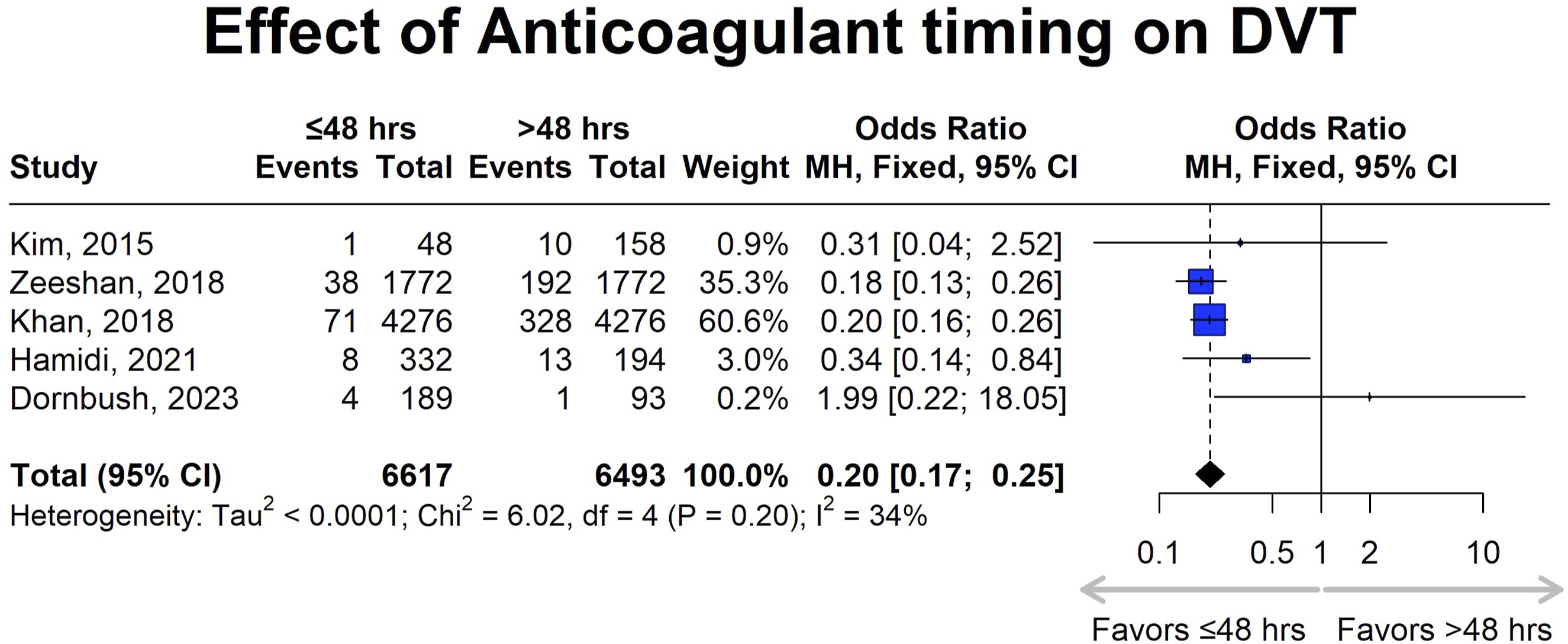
Consistent with the findings from the DVT analysis, early administration of chemical anticoagulation was associated with a significantly reduced risk of pulmonary embolism compared to delayed initiation (OR: 0.46 [95% CI: 0.34-0.62]). Heterogeneity analysis yielded a Tau2 of 0.0450, Chi2 of 3.39 (df = 4, P = .50), and an I
2
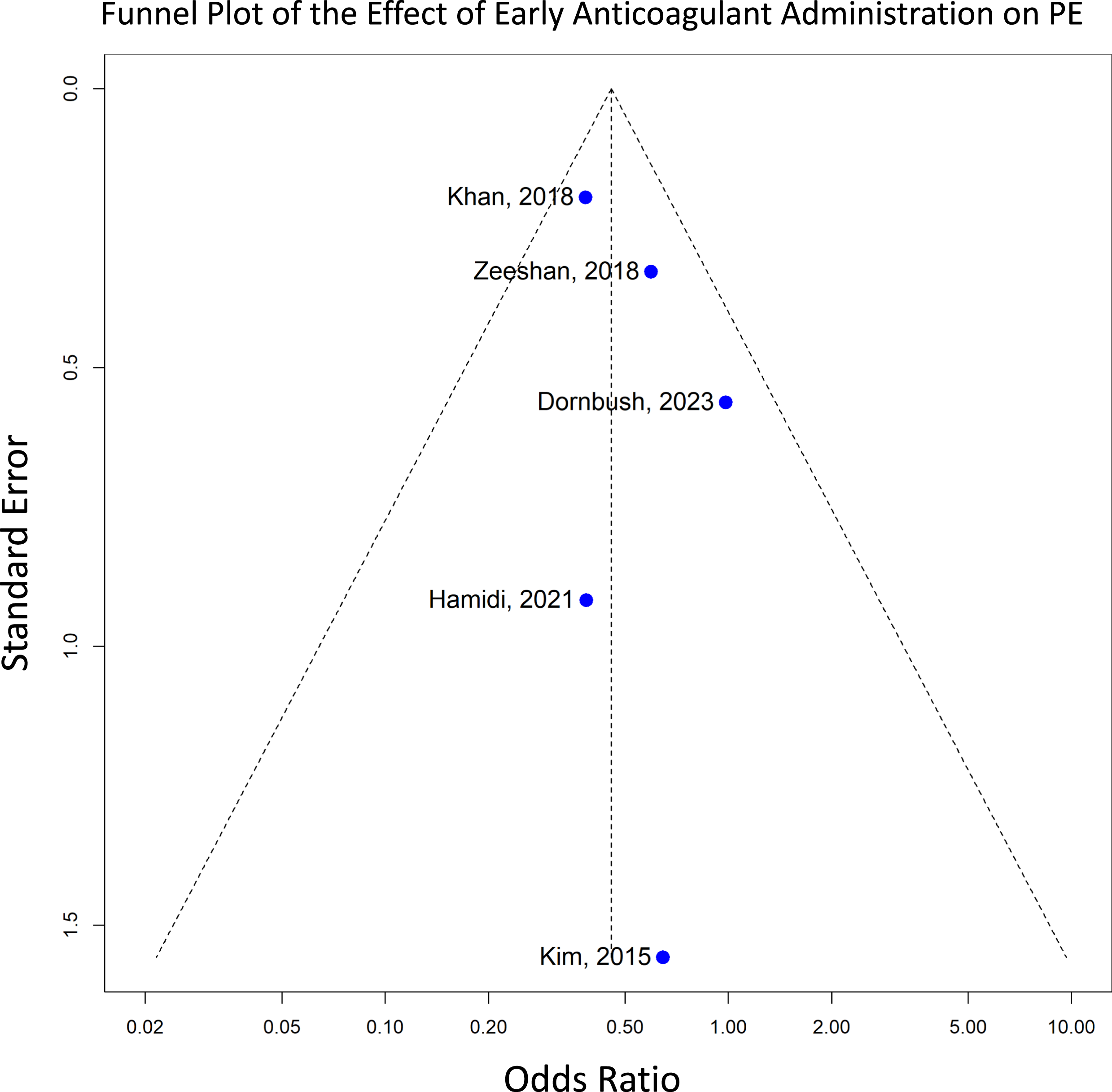
of 0%, indicating low heterogeneity and consistency across the included studies (Figure 4). The accompanying funnel plot illustrates study distribution, with larger studies such as Khan et al. (2018) having smaller Standard Errors, while the placement of the studies within the 95% Confidence Interval of the pooled effect suggests minimal publication bias (Figure 5).
22
Forest plot for pulmonary embolism (PE), showing the effect sizes of included studies and the overall pooled estimate with their corresponding confidence intervals, comparing anticoagulation initiation within 48 hours (early) vs after 48 hours (late). Funnel plot assessing publication bias for PE, helping to identify any potential publication bias.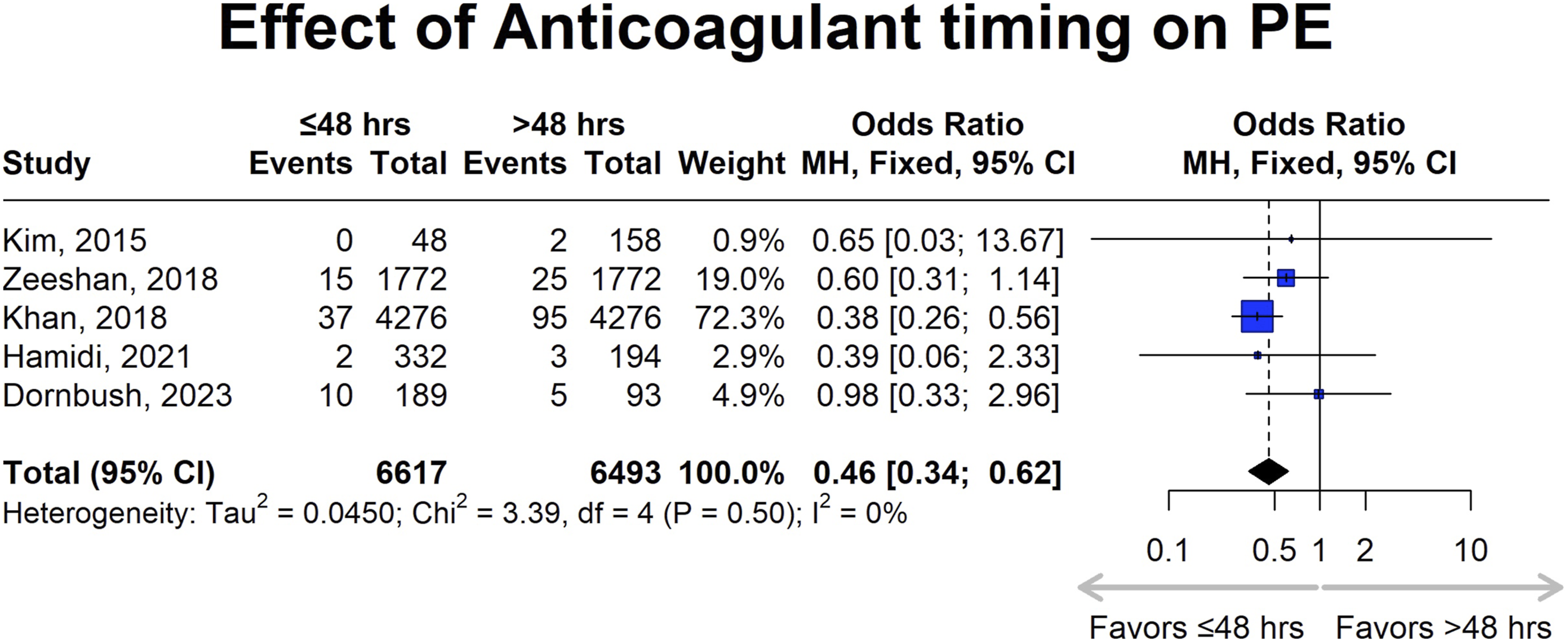
Four studies compared early vs late initiation of chemical anticoagulation but were not eligible for inclusion in the meta-analysis due to differing definitions of primary outcomes (i.e., studying venous thromboembolism (VTE) rather than DVT) or time points (i.e., 72 hours rather than 48 hours) used for comparison.6,25-27 For instance, Godat et al analyzed 343 patients with spinal cord injury (SCI) and found that the VTE rate was 7.1% when prophylaxis was initiated within 48 hours, compared to 12.1% when started later (P = .119). 6 After adjusting for risk factor differences, initiation within 48 hours was independently associated with a lower risk of VTE (OR: 0.45 [95% CI: 0.101-0.978]; P = .044). Similarly, Taghlabi et al reported a significantly higher VTE incidence when anticoagulation was initiated 72 hours post-trauma compared to early administration (30% vs 4.4%; P < .0001), 25 comparable to findings from earlier studies.
Meta-Analysis of Anticoagulation and Clinical Outcomes
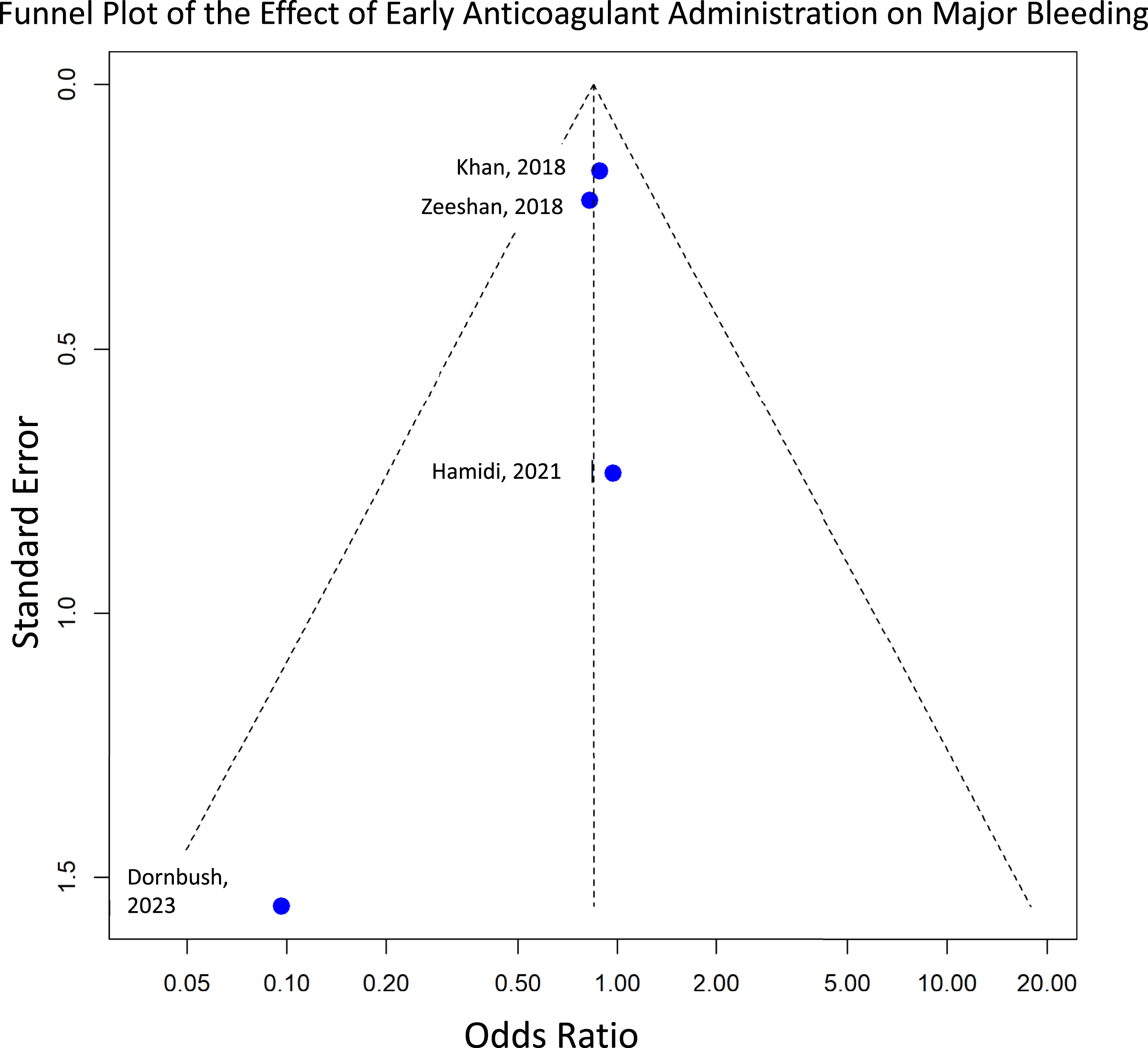
The safety assessment focused on the incidence of major bleeding and all-cause mortality between early and delayed initiation of chemical anticoagulation following spine trauma. The analysis for major bleeding included 4 studies and indicated no statistically significant difference in the odds of major bleeding by the timing of anticoagulation administration (OR: 0.85 [95% CI: 0.66-1.09]; P = .1992) (Figure 6). The funnel plot shows an asymmetric distribution of studies, which could indicate potential publication bias or heterogeneity, especially since smaller studies with higher standard errors tend to show a stronger effect size in the direction of a protective effect (Figure 7). Forest plot for major bleeding, showing the effect sizes of included studies and the overall pooled estimate, comparing anticoagulation initiation within 48 hours (early) vs after 48 hours (late), with confidence intervals indicating statistical significance. Funnel plot visually assessing publication bias for major bleeding.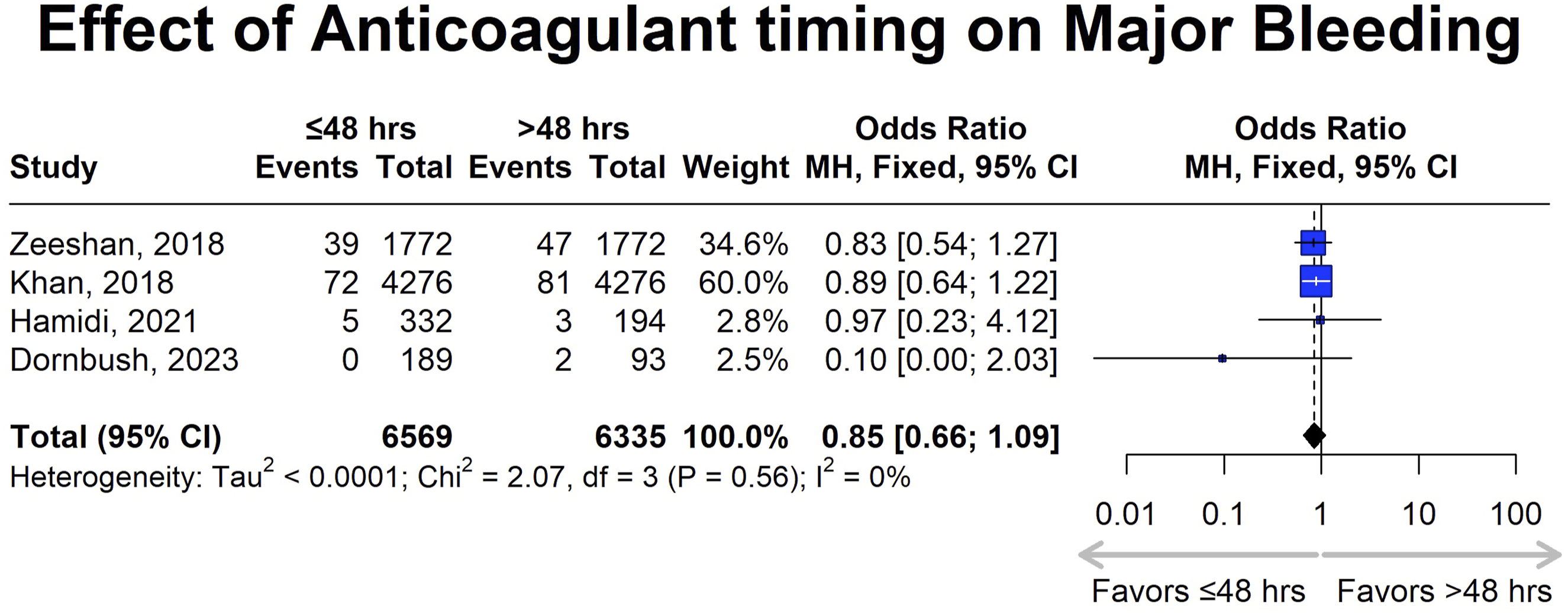
The analysis of all-cause mortality included 6,428 patients in the early anticoagulant initiation cohort and 6,400 in the delayed anticoagulant initiation cohort. Zeeshan et al (2018) and Khan et al (2018) contributed most of the weight, at 51.2% and 42.7%, respectively, with smaller contributions from Hamidi et al (2021) at 4.3% and Kim et al (2015) at 1.9% (Figure 8).16,17,22,24 Forest plot for mortality, showing the effect sizes of included studies and the overall pooled estimate with their corresponding confidence intervals, comparing anticoagulation initiation within 48 hours (early) vs after 48 hours (late), with confidence intervals indicating statistical significance.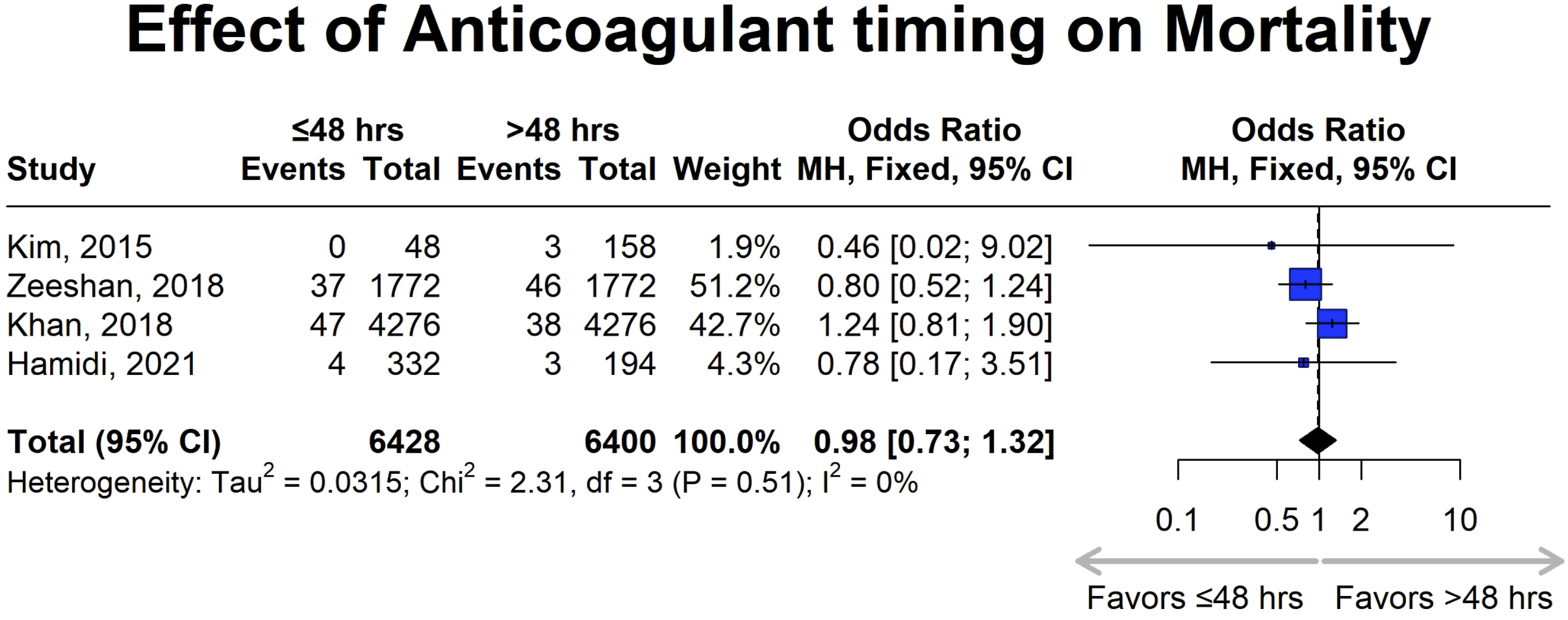
The pooled odds ratio (OR) was 0.98 (95% CI: 0.73-1.32), indicating no significant difference in all-cause mortality between early and delayed anticoagulation administration. Heterogeneity analysis showed a Tau
2
of 0.0315, Chi2 of 2.31 (df = 3, P = .51), and an I
2
of 0%, indicating low variability across studies. The near-symmetric funnel plot and lack of studies with high effect sizes and standard errors suggest a minimal risk of publication bias (Figure 9). A summary of the pooled results of the entire meta-analysis is presented in Table 2. Funnel plot assessing publication bias for mortality, where asymmetry may suggest potential bias in the included studies. Summary of the pooled results of the entire meta-analysis; the pooled OR corresponds to comparing early (within 48 hours of spine trauma) vs late timing (after 48 hours of spine trauma) of chemoprophylaxis administration.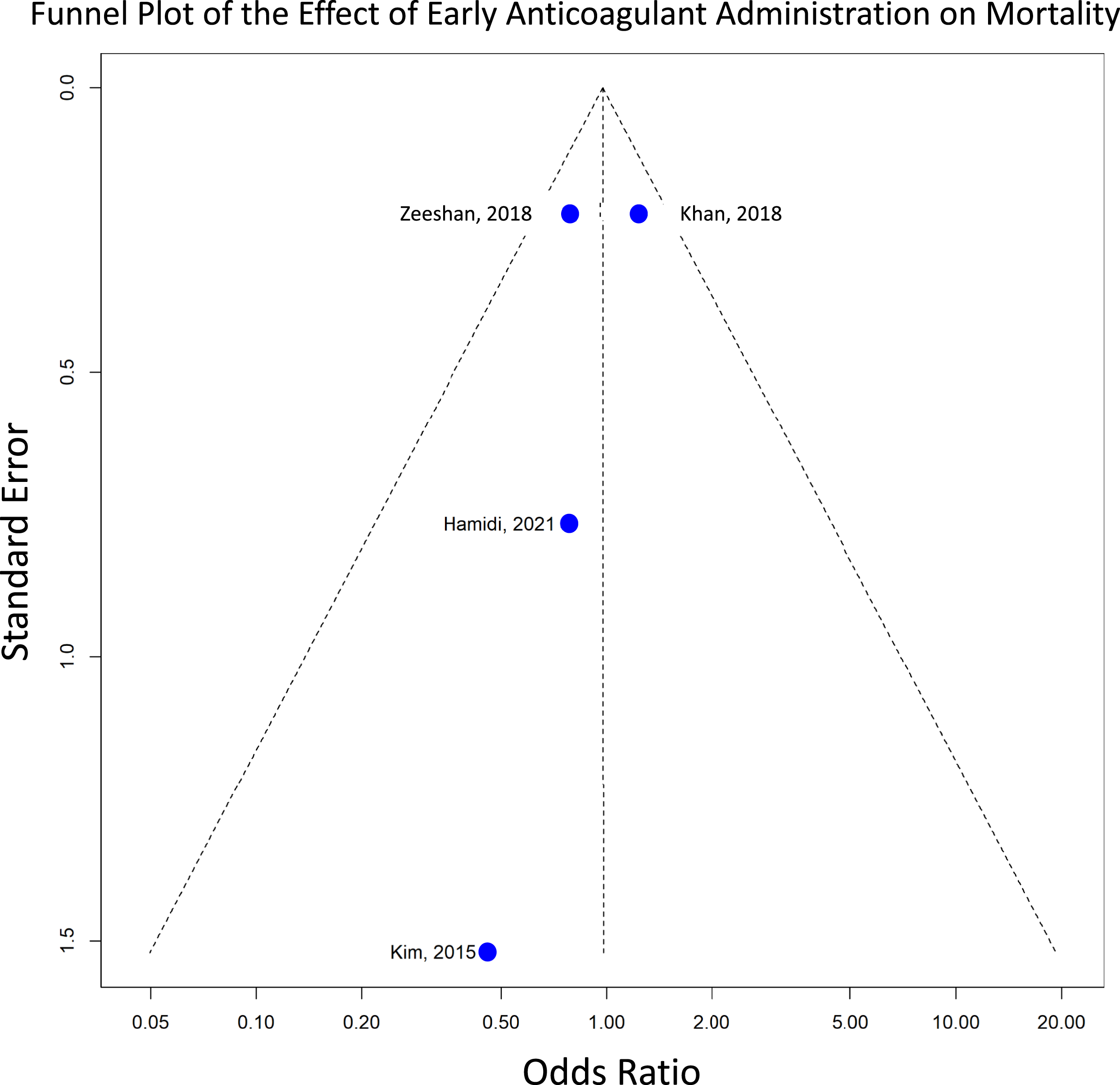

Discussion
This systematic review and meta-analysis, encompassing 9 studies, highlights 2 key findings: in spine trauma, the administration of chemical anticoagulation within 48 hours is associated with a significantly lower incidence of DVT and PE compared to initiation after 48 hours; there are no significant differences in the odds of major bleeding and all-cause mortality between early vs late chemoprophylaxis administration. While no statistically significant difference was observed for bleeding or mortality, it is important to recognize that this analysis may be underpowered due to the relatively small number of included studies reporting these outcomes. Therefore, the absence of statistical significance should be interpreted cautiously, and further large-scale, well-powered studies specifically designed to assess these endpoints are warranted. Despite the prevalence of spine trauma, research disproportionately focuses on operative cases, with limited data on outcomes in nonoperative populations. The latter is neither systematically tracked nor adequately studied despite the comparable incidence of medical complications. For instance, a systematic review by Ghobrial et al reported near-identical rates of pulmonary, thromboembolic, cardiac, and gastrointestinal complications between operative and nonoperative groups. 28 When integrated with existing literature on operative populations, the data presented here suggest that both nonoperative and operative spine trauma patients may benefit from chemoprophylaxis initiated within 48-72 hours of injury.
Supporting this assertion, prospective data from 1,425 patients with traumatic brain injuries (TBI) or spinal injuries collected from 2010 to 2014 demonstrated a significant association between delayed initiation of chemical VTE prophylaxis and increased VTE risk. Tracy et al found that patients who developed VTE had a longer time to prophylaxis initiation (6.7 ± 4.9 days vs 4.7 ± 4.9 days, P < .001). Each 1-day delay in initiating prophylaxis was associated with a significant increase in VTE risk (OR: 1.055, P < .001). 29 Interestingly, among this heterogeneous population, patients with isolated spinal injuries (similar to the population presented here) received prophylaxis significantly earlier and had a markedly reduced VTE rate (4.4% vs 10.4%, P < .0001) compared to the overall TBI group. 23 Similarly, in an operative population, Taghlabi et al (2022) reported that early administration of VTE prophylaxis (≤72 hours postoperatively) was associated with a significantly lower VTE rate (4.4%) compared to late initiation (30%). 25
Although no studies directly compare various timepoints, early (within 48 hours) but not immediate (<24 hours) chemoprophylaxis appears to strike an optimal balance between efficacy and safety. Lambrechts et al (2024) investigated outcomes in 8,704 patients receiving either immediate subcutaneous heparin or chemoprophylaxis initiated on postoperative day (POD) 1 or 2. The study found that immediate chemoprophylaxis did not significantly reduce the risk of VTE (HR: 1.18, P = .436), but it was a significant independent predictor of unplanned reoperation for hematoma. 30 The authors intuitively concluded that delaying chemoprophylaxis allows for physiologic coagulation of minor residual bleeding, which may not be fully addressed intraoperatively.
While the efficacy of chemoprophylaxis is well established, this study adds to the growing body of evidence supporting the safety of chemoprophylaxis, despite theoretical concerns about catastrophic epidural hematoma. The prevalence of epidural hematoma in patients with spinal fractures is reported to be less than 1%,31-33 with some studies citing rates as low as 0.19%, unaffected by the administration of chemoprophylaxis. 34 Most recently, a 2024 systematic review and meta-analysis showed that the overall pooled incidence of epidural hematoma was 0.4%, without difference between patients that did and did not receive chemoprophylaxis. 35 Moreover, while the risk of iatrogenic complications is significant, Nerelius et al compared 113 patients who required evacuation of an epidural hematoma with 19,527 patients who did not. Both groups demonstrated significant improvement across all PROMs, with no significant differences between the groups. 36 In contrast, while specific validation in spine patients is lacking, orthopedic literature demonstrates that DVT during periods of relative immobilization significantly impacts long-term functional and patient-reported outcomes, persisting several years post-surgery. 37
Overall, consensus on the timing of anticoagulation remains elusive, which this study hopes to help clarify. As recently as 2023, a modified Delphi clinical recommendations paper suggested stratified initiation of VTE chemoprophylaxis: low-risk patients on POD 5, medium-risk patients on POD 3 to 4, and high-risk patients on POD 1 to 2. 38 Survey-based studies further underscore this variability. Among orthopedic and neurosurgical spine surgeons, 22% identified 48 hours as the appropriate initiation time, but preferences varied significantly, with 12% favoring initiation within 24 hours, 15% at 24 hours, 13% at 72 hours, and 10% at 96 hours.26,39
Clinical Recommendations
Given the available evidence, early initiation of chemical VTE prophylaxis within 48 hours appears beneficial for both operative and nonoperative spine trauma patients, as thromboembolic complications are comparably common in these groups. Nevertheless, prophylaxis should be individualized, with careful attention to patient selection and risk stratification. In particular, clinicians should assess bleeding risk and closely monitor patients during anticoagulation to ensure safety.
Limitations
Our review encompassed studies of varying quality, with few high-quality randomized controlled trials; consequently, recommendations rely on the best available evidence, including retrospective studies prone to small sample sizes and selection bias. A formal quantitative analysis of bias was not conducted, as only 5 studies were included in the meta-analysis. Due to the small number of studies, such an analysis would not have been meaningful. Data on nonoperative spinal trauma are particularly limited, focusing primarily on patients with adequate follow-up, which constrains the ability to make robust recommendations for this group. Furthermore, the absence of comparative studies assessing specific initiation time points complicates the delineation of an optimal window to balance efficacy and safety. As such, the findings primarily highlight differences observed within and beyond 48 hours of anticoagulation initiation. In two of the included studies (Kim et al, 2015 and Dornbush et al, 2023), neurological impairment was documented using the ASIA classification (A-E), while the other studies primarily recorded the extent of injury using the Spine Abbreviated Injury Scale (AIS) or the Injury Severity Score (ISS).17,23 The inconsistent use of these classifications represents a further limitation of the analysis. The majority of the included studies examined patients who underwent surgical stabilisation of their spinal injury. Given that the indication, timing, and strategy of VTE prophylaxis may differ between surgical and non-surgical patients, the results of this meta-analysis should be interpreted primarily in the context of surgically treated patients, while the applicability to non-surgical cases is limited.
Conclusion
This systematic review and meta-analysis provide compelling evidence that initiating chemical anticoagulation within 48 hours of spinal trauma significantly reduces the risk of DVT and PE with no evidence of increasing major bleeding or all-cause mortality. While current practice patterns reflect hesitancy in early anticoagulation due to concerns about hematologic complications, our findings suggest that timely prophylaxis offers substantial benefits without compromising patient safety. The study also underscores the need for standardized guidelines to bridge the gap between existing evidence and clinical practice, particularly for nonoperative spinal trauma patients who remain understudied. Future research should focus on refining optimal anticoagulation timing through prospective trials and expanding investigations into nonoperative populations to enhance evidence-based recommendations.
Supplemental Material
Supplemental Material - Timing of Chemical Anticoagulant Administration in Spine Trauma and its Impact on VTE, Bleeding, and Mortality: A Systematic Review and Meta-Analysis
Supplemental Material for Timing of Chemical Anticoagulant Administration in Spine Trauma and its Impact on VTE, Bleeding, and Mortality: A Systematic Review and Meta-Analysis by Sarthak Mohanty, Hanna von Riegen, Michael Akodu, Elizabeth Oginni, Diana Yeritsyan, Kaveh Momenzadeh, Anne Fladger, Mario Keko, Michael McTague, Ara Nazarian, Jason L. Pittman, and Sapan D. Gandhi in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.G. reports paid consultancy with Johnson&Johnson and Qmetis. J.P. declares the following affiliations: DePuy Consultant, BrainLab Consultant, ZSFab Consultant, Amplify Speaker, ROMTech Stock.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
This study is based on previously published studies. All data used in this study were extracted from publicly available sources cited in the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.