
Abstract
Study Design
Retrospective cohort study.
Objectives
Obesity and metabolic syndrome have become a common comorbidity among patients undergoing spine surgery. This study aimed to evaluate 30-day postoperative outcomes following cervical laminoplasty, stratified by BMI categories and the presence of metabolic syndrome.
Methods
This study utilized the 2007-2022 ACS-NSQIP database. Patients who underwent cervical laminoplasty were identified and categorized into six BMI groups, according to the World Health Organization guidelines, and based on the presence of metabolic syndrome. The primary outcome was the 30-day occurrence of at least one complication (excluding blood transfusions). Secondary outcomes included rates of complications, hospital length of stay, and total operative time.
Results
A total of 2261 patients were analyzed, including 21 underweight, 510 normal-weight, 782 pre-obese, 565 class I obese, 249 class II obese, and 134 class III obese individuals. The cohort consisted of only 244 individuals with metabolic syndrome. Class II obesity (coefficient 23.585, 95% CI 10.815-36.355; P < 0.001) and class III obesity (coefficient 20.096, 95% CI 4.712-35.479; P = 0.011) were independently associated with longer operative times. Metabolic syndrome was an independent risk factor for deep incisional SSI (OR 3.25, 95% CI 1.07-9.80, P = 0.037), postoperative pneumonia (OR 4.17, 95% CI 1.63-10.63, P = 0.003), and prolonged hospitalization (OR 1.68, 95% CI 1.17-2.41, P = 0.005).
Conclusions
Patients with metabolic syndrome face an increased risk of adverse outcomes after cervical laminoplasty. Implementing preoperative preventive interventions may help mitigate complications and associated costs in these patients. Furthermore, preoperative weight loss in class II-III obese patients may help decrease operative time and associated costs.
Keywords
Introduction
Overweight and obesity have emerged as global health concerns, with a consistently increasing prevalence and burden observed worldwide in recent decades.1,2 In the United States, obesity has reached an epidemic status, while studies have projected that nearly half of the adult population will be affected by obesity by 2030.3,4 Obesity in adults has been associated with a wide array of complications, including: (1) Psychiatric conditions such as depression and anxiety, (2) metabolic disorders such as cardiovascular disease and type II diabetes mellitus (DM), and (3) mechanical consequences, including osteoarthritis.5–8 Obesity is a recognized risk factor for unfavorable postoperative outcomes across various spinal procedures, leading to complications such as infection, wound complications, incidental durotomy, readmission, and increased health care costs.7,9,10
Metabolic syndrome refers to a combination of major medical conditions, including insulin resistance, obesity, and hypertension, which collectively heighten the risk of cardiovascular disease and related complications.11,12 The prevalence of metabolic syndrome among the adult population of the United States has risen approximately 26% from 1988-1994 to 2007-2012.13,14 Previous studies have identified several contributing risk factors, including physical inactivity and dietary shifts, that play a role in its development.15,16 Metabolic syndrome has been shown to influence postoperative outcomes across various surgical interventions significantly.17,18 In lumbar spine surgery, it is particularly relevant as a predictor of poorer perioperative outcomes. 19 Existing studies have linked the condition to prolonged hospital stays, higher health care utilization and costs, and greater rates of major postoperative complications in spine surgeries, such as posterior lumbar spinal fusion.19-21 Regarding cervical spine surgery, investigations into the effects of metabolic syndrome are even scarcer. To date, only two studies have specifically examined its impact on patients undergoing procedures of the cervical spine, including anterior cervical discectomy and fusion and cervical disc replacement.20,21 As life expectancy rises and metabolic syndrome has been increasingly associated with spinal osteoarthritis, the number of affected patients requiring surgery for degenerative spinal disorders is expected to grow. 22
Laminoplasty is an established surgical technique utilized for treating cervical spine degenerative conditions. This procedure expands the spinal canal while preserving the posterior tension band, potentially mitigating the biomechanical drawbacks commonly associated with laminectomy. 23 Although prior literature has investigated the impact of body mass index (BMI) and metabolic syndrome on cervical and lumbar spine procedures,10,20,21,24,25 comprehensive large-scale database studies focusing specifically on cervical laminoplasty remain lacking. While some smaller, institutional retrospective studies have examined the outcomes of cervical laminoplasty,26-29 their limited sample sizes impede the identification and comparison of significant but rare adverse events, such as pulmonary thromboembolism or myocardial infarction (MI), stratified by BMI. Additionally, these studies have not categorized patients based on the severity of obesity or underweight status and presence or absence of metabolic syndrome, despite evidence suggesting that unfavorable outcomes may be significantly more prevalent in underweight and morbidly obese patients, along with patients with metabolic syndrome, undergoing cervical spine surgery.20,21,24 Evaluating the role of BMI and metabolic syndrome in the incidence of adverse outcomes following cervical laminoplasty is crucial for effective risk stratification, patient counseling, treatment planning, and implementing preventive measures for these complications.
The present study aimed to report 30-day postoperative outcomes for patients who underwent cervical laminoplasty, stratified by BMI category and the presence or absence of metabolic syndrome. We hypothesize that patients with increased BMI and with metabolic syndrome have an increased 30-day postoperative complication rate.
Methods
Data Source
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) is a multi-institutional initiative that prospectively collects more than 200 variables from de-identified surgical cases at over 700 institutions nationwide, in compliance with the Health Insurance Portability and Accountability Act. The data encompasses information on baseline characteristics, intraoperative factors, and outcomes related to morbidity and mortality within 30 days after surgical procedures. Participating sites undergo Inter-Rater Reliability (IRR) audits, and each institution employs certified Surgical Clinical Reviewers responsible for ensuring the quality of the data collected and sampling processes. 30 This program boasts an IRR disagreement rate of less than 2%. 31
Study Design
This retrospective cohort study utilized the ACS-NSQIP database from 2007 to 2022. Patients who underwent cervical laminoplasty were identified using Current Procedural Terminology (CPT) codes 63 050 (laminoplasty, cervical, with decompression of the spinal cord, two or more vertebral segments) and 63 051 (laminoplasty, cervical, with decompression of the spinal cord, two or more vertebral segments; With reconstruction of the posterior bony elements). This study did not require the approval of the institutional review board at the authors’ institution. The data used for this study are available upon reasonable request.
Exclusion Criteria
To focus on the routine adult patient treated with cervical laminoplasty, patients were excluded if they underwent any emergent or irrelevant concurrent surgeries, were being treated for non-degenerative spinal conditions, had end-stage organ diseases, or had missing demographic data. The complete list of the exclusion criteria is presented in Figure 1. Database variables investigated for the present study.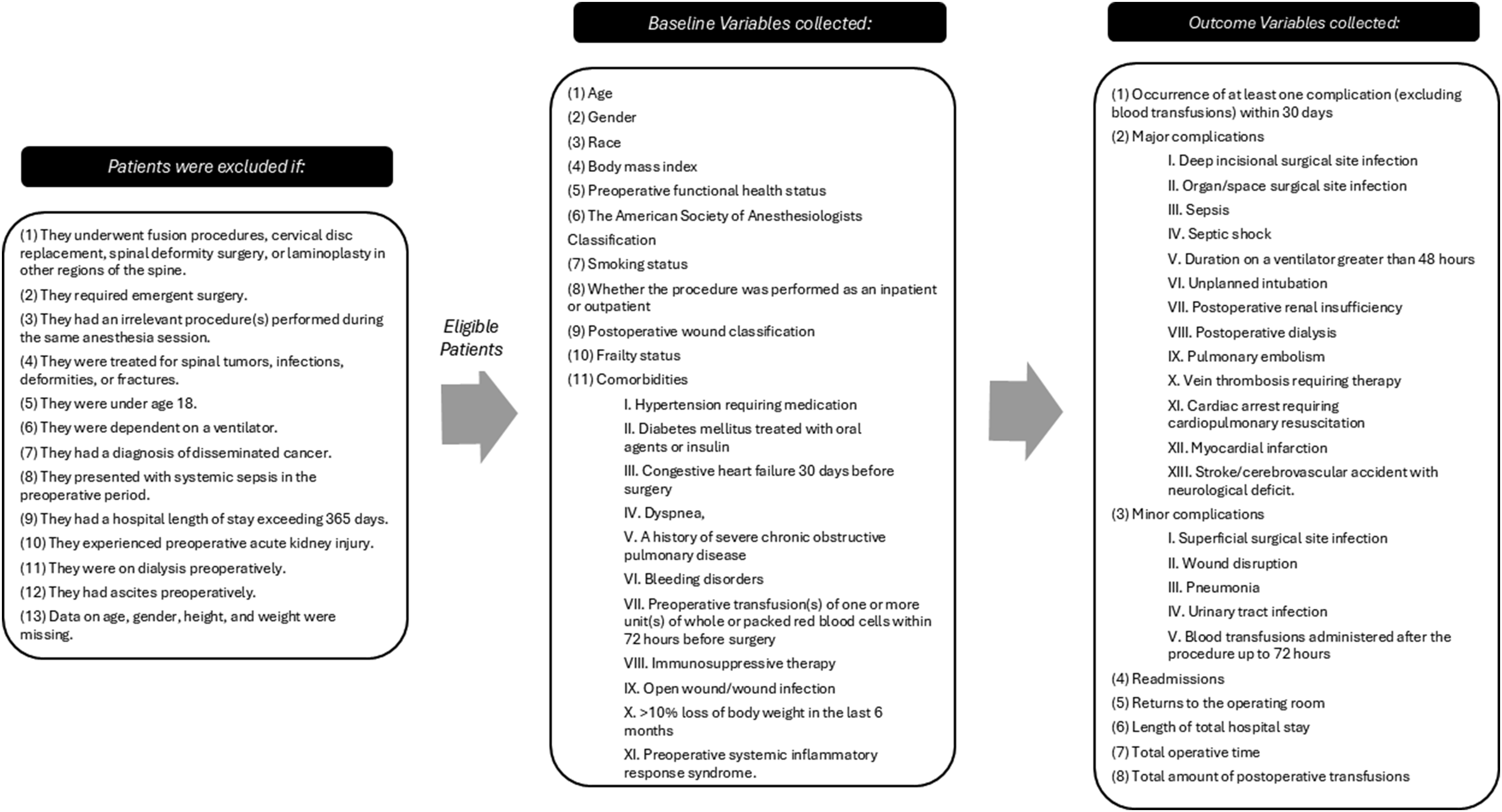
Baseline Variables
The BMI for the included patients was calculated based on their recorded height and weight using Quetelet’s index 32 and categorized according to the guidelines established by the World Health Organization (WHO). 33 The BMI categories were defined as follows: (1) Underweight (BMI < 18.5 kg/m2), (2) normal weight (18.5-24.9 kg/m2), pre-obese (25-29.9 kg/m2), class I obese (30-34.9 kg/m2), class II obese (35-39.9 kg/m2), and class III obese (≥40 kg/m2). Metabolic syndrome was defined based on established criteria used in previous ACS-NSQIP studies, requiring the presence of: (1) Hypertension requiring medication, (2) diabetes mellitus treated with oral agents or insulin, and (3) a BMI of 30 kg/m2 or higher.20,21 smoking status was defined as current smoking within the past year. The frailty status was determined using the modified Frailty Index (mFI-5), in accordance with the previous literature. 34 Other baseline variables collected are presented in Figure 1.
Outcome Variables
The primary outcome variable was the occurrence of at least 1 complication (excluding blood transfusions) within 30 days. The secondary outcome variables included: (1) major complications, (2) minor complications, (3) individual postoperative complications, (4) readmissions, (6) returns to the operating room, (7) length of total hospital stay, (8) total operative time, and (9) total amount of postoperative transfusions. The complete list of postoperative complication variables is presented in Figure 1. The length of total hospital stay was classified into two categories: (1) Regular and (2) extended. An extended length of total hospital stay was defined as 1 that exceeded the 80th percentile among the study population for the procedure, which was set at 5 days.
Statistical Analysis
Descriptive statistics were presented as frequencies and percentages or means and standard deviations. Methods used for univariate analysis included the χ2 test or Fisher’s Exact Test for categorical variables, and the independent samples t test or Mann-Whitney U-test for continuous variables. Baseline variables with a P < 0.2 in the univariate analysis were included in the multivariate analysis. To evaluate the independent correlation between BMI category and metabolic syndrome with categorical outcome variables, multivariate logistic regression models were employed, adjusting for other baseline variables. Multivariate linear regression models were utilized to assess the independent association of BMI category and metabolic syndrome with continuous outcome variables to account for other baseline variables. Normal-weight patients, defined as having a BMI between 18.5 and 24.9 kg/m2, were set as the reference group in the multivariate analyses for BMI. As diabetes mellitus treated with oral agents or insulin, hypertension requiring medication, and BMI were components utilized to define metabolic syndrome, they were omitted from the multivariate regression models for metabolic syndrome. Coefficients and odds ratios (ORs) with 95% confidence intervals (CIs) were computed. Data analysis was conducted using RStudio version 4.4.2 (R Foundation). All tests were two-tailed, with statistical significance defined as a P < 0.05.
Results
Participants
A total of 4792 patients were identified in the 2007-2022 ACS-NSQIP database. Of these, 2531 patients were excluded due to concurrent operative procedures (n = 2331), emergent surgery (n = 65), ineligible pathologies (n = 65), preoperative dialysis (n = 22), disseminated cancer (n = 6), preoperative acute kidney injury (n = 4), dependence on a ventilator (n = 2), preoperative systemic sepsis (n = 2), and missing data regarding age, gender, height, or weight (n = 34). Notably, none of the patients were under the age of 18, had a hospital length of stay (LOS) exceeding 365 days, presented with preoperative ascites, or had missing data regarding hypertension or DM. Consequently, a total of 2261 patients were included and analyzed in this study (Figure 2). Flow diagram illustrating the patient selection process for this study.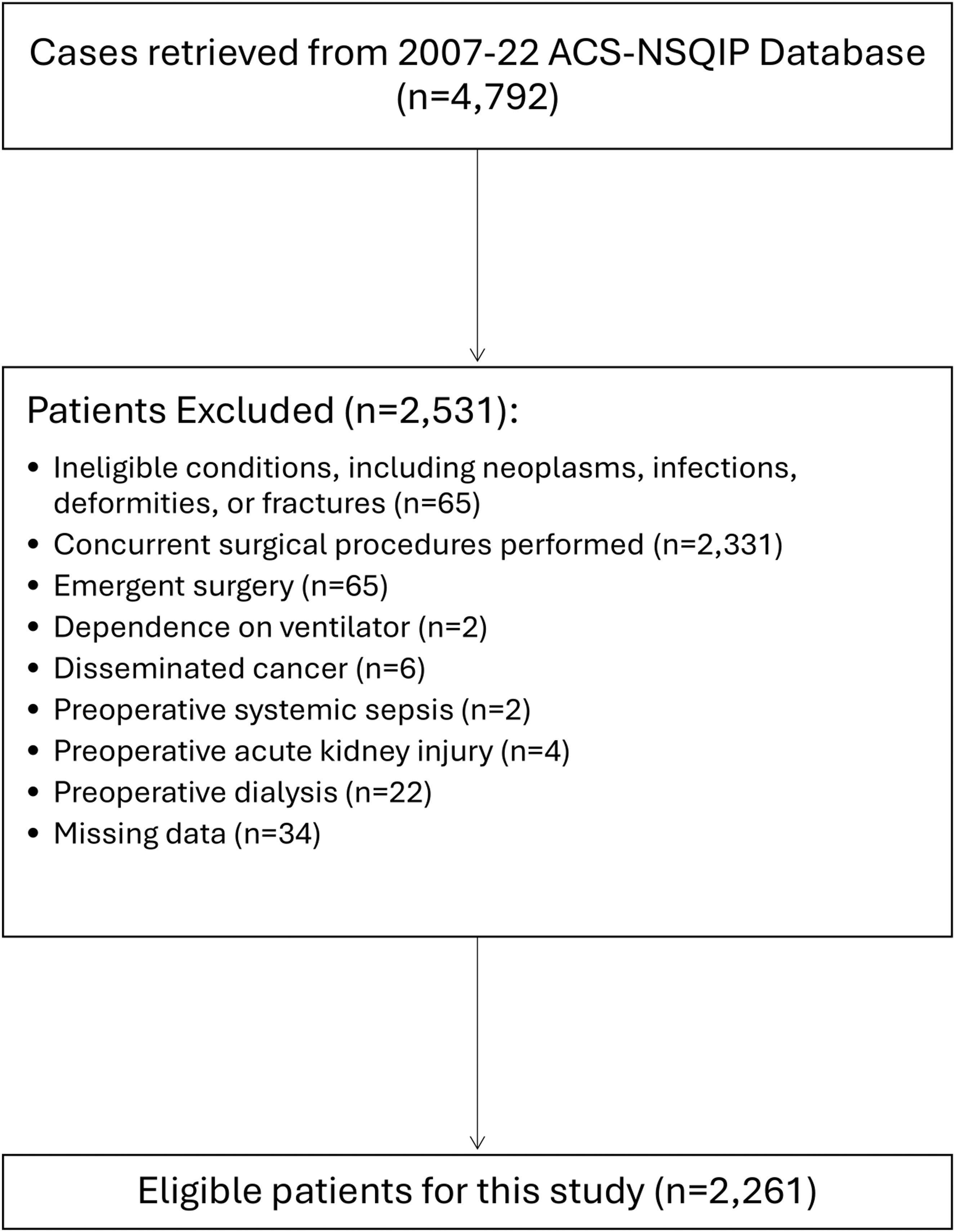
Baseline Variables
Baseline Characteristics of Included Patients Across Different Body Mass Index Categories.
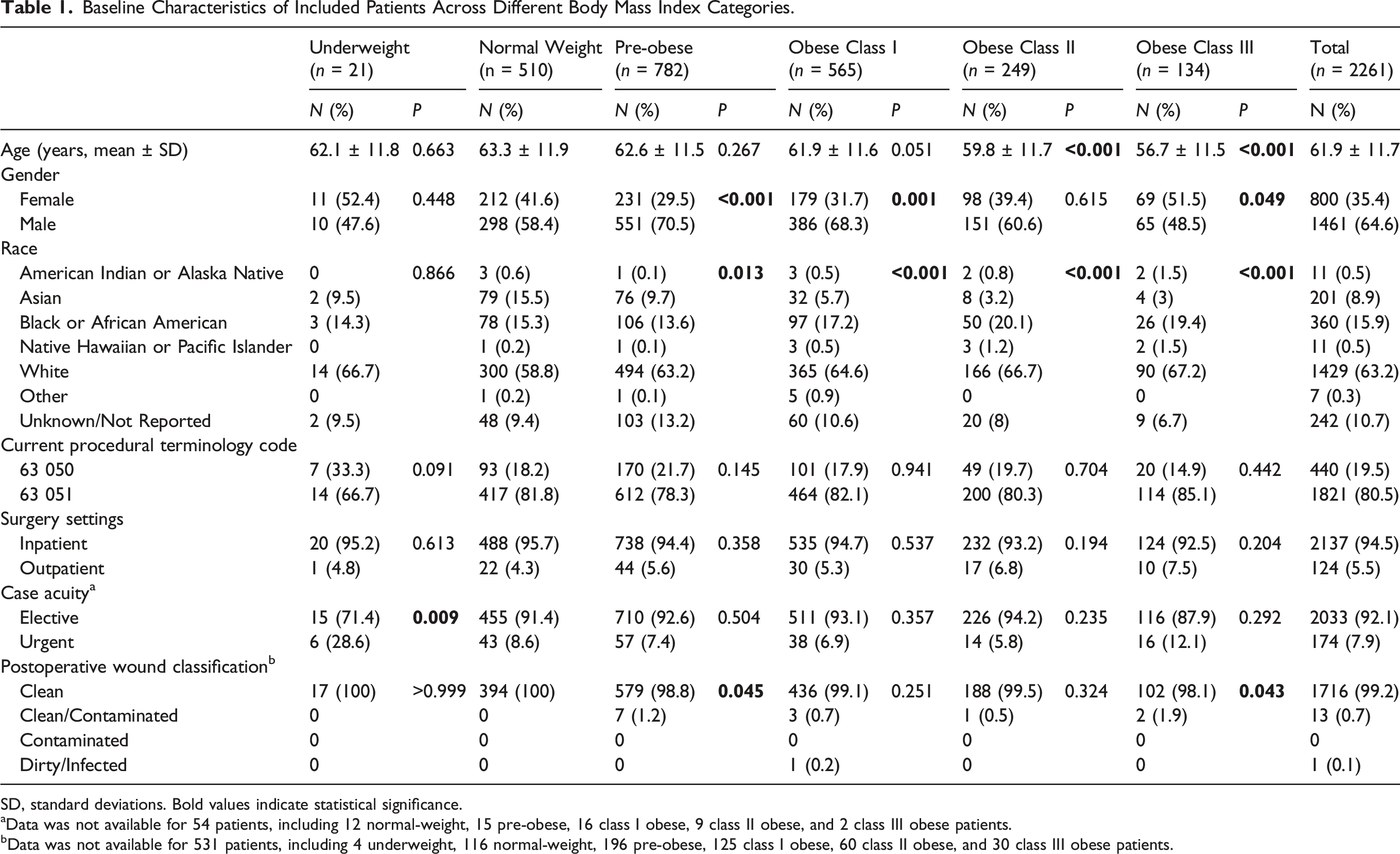
SD, standard deviations. Bold values indicate statistical significance.
aData was not available for 54 patients, including 12 normal-weight, 15 pre-obese, 16 class I obese, 9 class II obese, and 2 class III obese patients.
bData was not available for 531 patients, including 4 underweight, 116 normal-weight, 196 pre-obese, 125 class I obese, 60 class II obese, and 30 class III obese patients.
Baseline Variables of Patients Included in This Study with Regard to the Presence or Absence of Metabolic Syndrome.
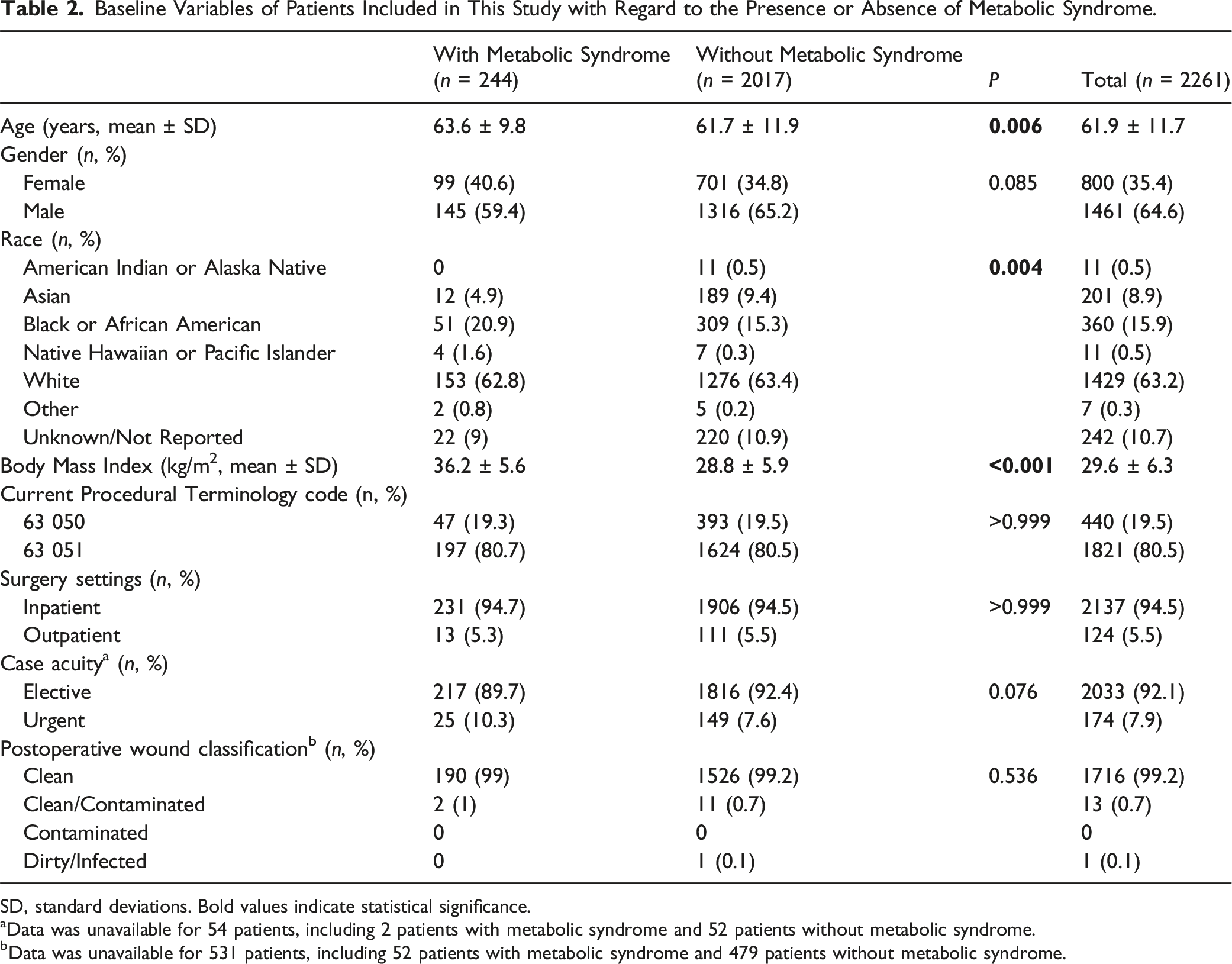
SD, standard deviations. Bold values indicate statistical significance.
aData was unavailable for 54 patients, including 2 patients with metabolic syndrome and 52 patients without metabolic syndrome.
bData was unavailable for 531 patients, including 52 patients with metabolic syndrome and 479 patients without metabolic syndrome.
Univariate Analysis
Outcome Variables of the Study Across Different Body Mass Index Categories.
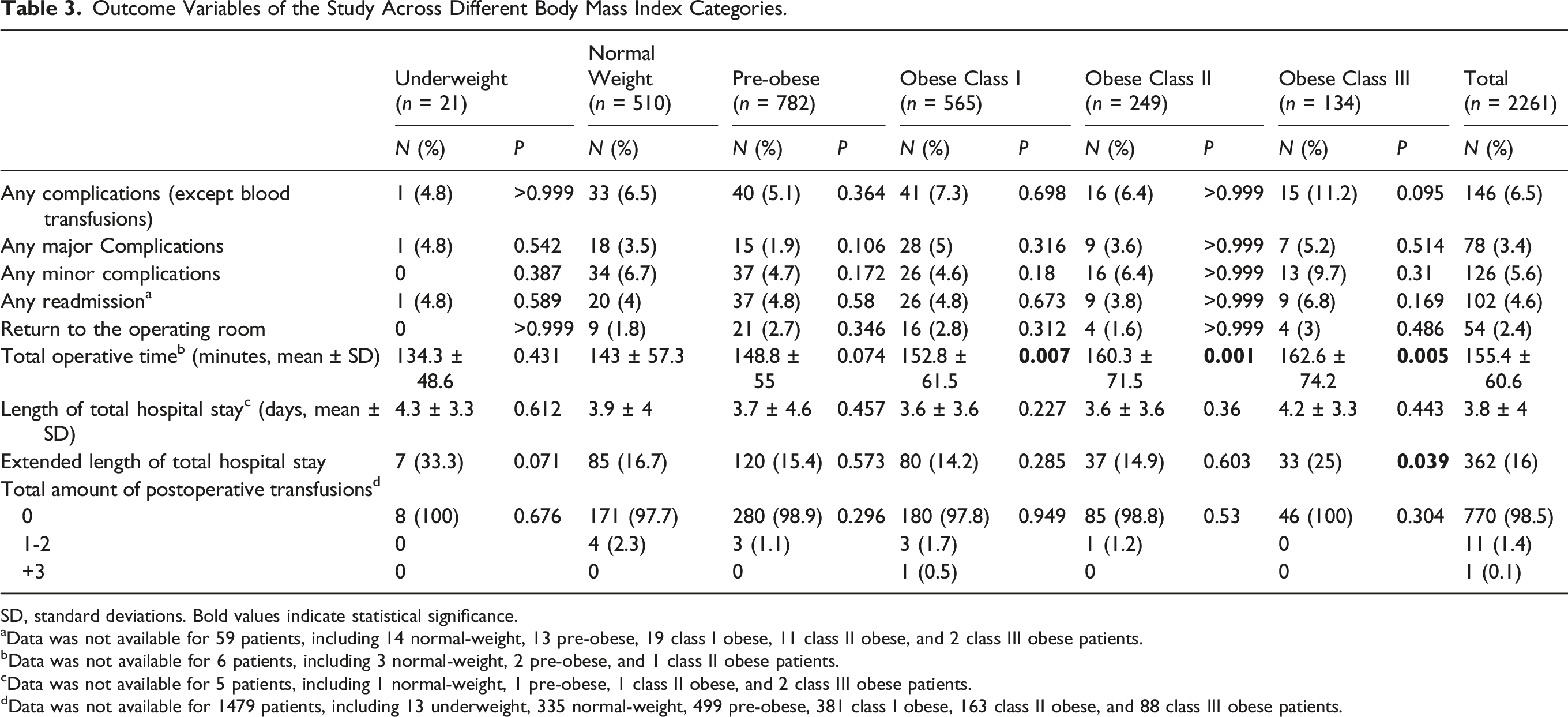
SD, standard deviations. Bold values indicate statistical significance.
aData was not available for 59 patients, including 14 normal-weight, 13 pre-obese, 19 class I obese, 11 class II obese, and 2 class III obese patients.
bData was not available for 6 patients, including 3 normal-weight, 2 pre-obese, and 1 class II obese patients.
cData was not available for 5 patients, including 1 normal-weight, 1 pre-obese, 1 class II obese, and 2 class III obese patients.
dData was not available for 1479 patients, including 13 underweight, 335 normal-weight, 499 pre-obese, 381 class I obese, 163 class II obese, and 88 class III obese patients.
Outcomes of Patients Included in This Study with Regard to the Presence or Absence of Metabolic Syndrome.
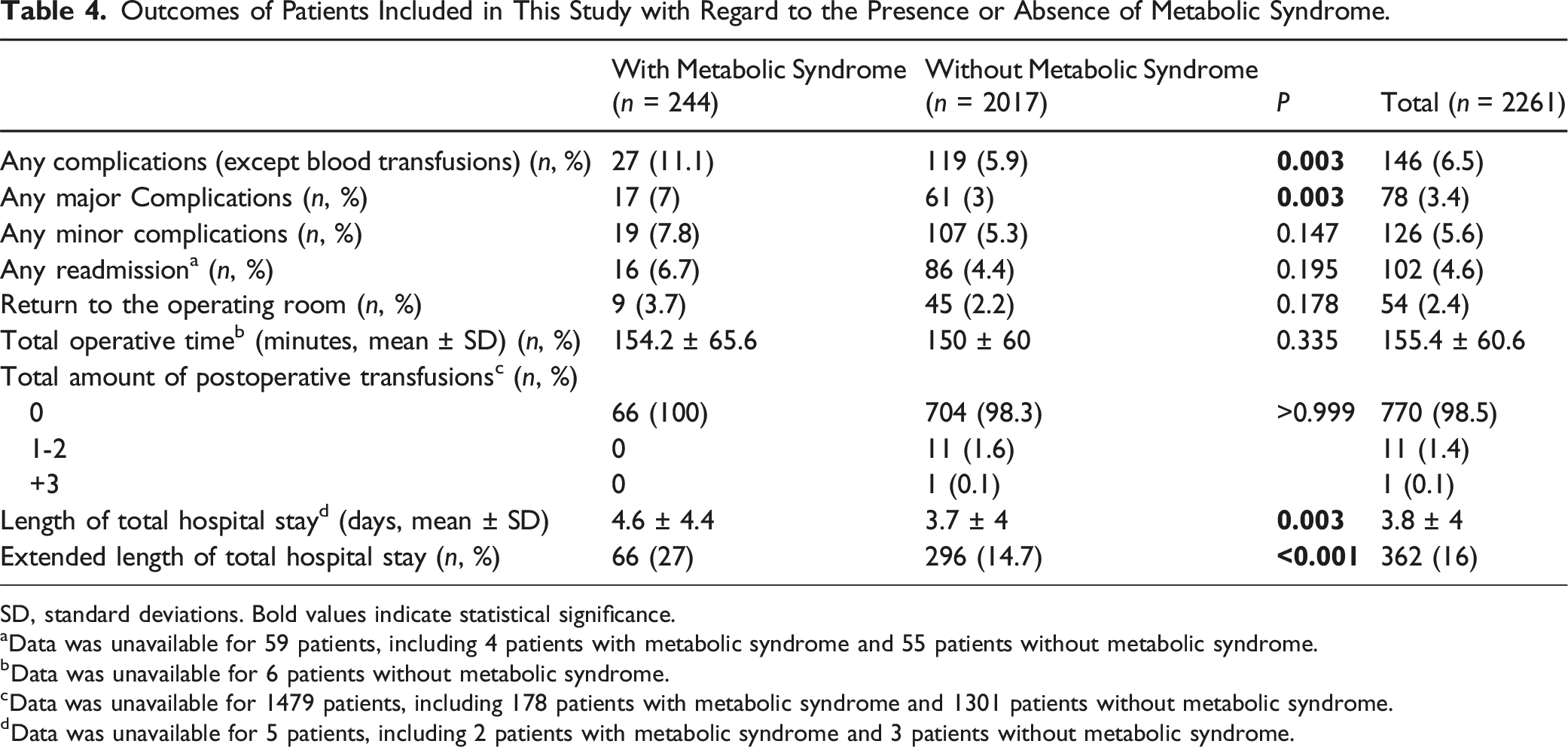
SD, standard deviations. Bold values indicate statistical significance.
aData was unavailable for 59 patients, including 4 patients with metabolic syndrome and 55 patients without metabolic syndrome.
bData was unavailable for 6 patients without metabolic syndrome.
cData was unavailable for 1479 patients, including 178 patients with metabolic syndrome and 1301 patients without metabolic syndrome.
dData was unavailable for 5 patients, including 2 patients with metabolic syndrome and 3 patients without metabolic syndrome.
Multivariate Analysis
Regression Analysis of the Association of Different Body Mass Index Categories With Study Outcomes.
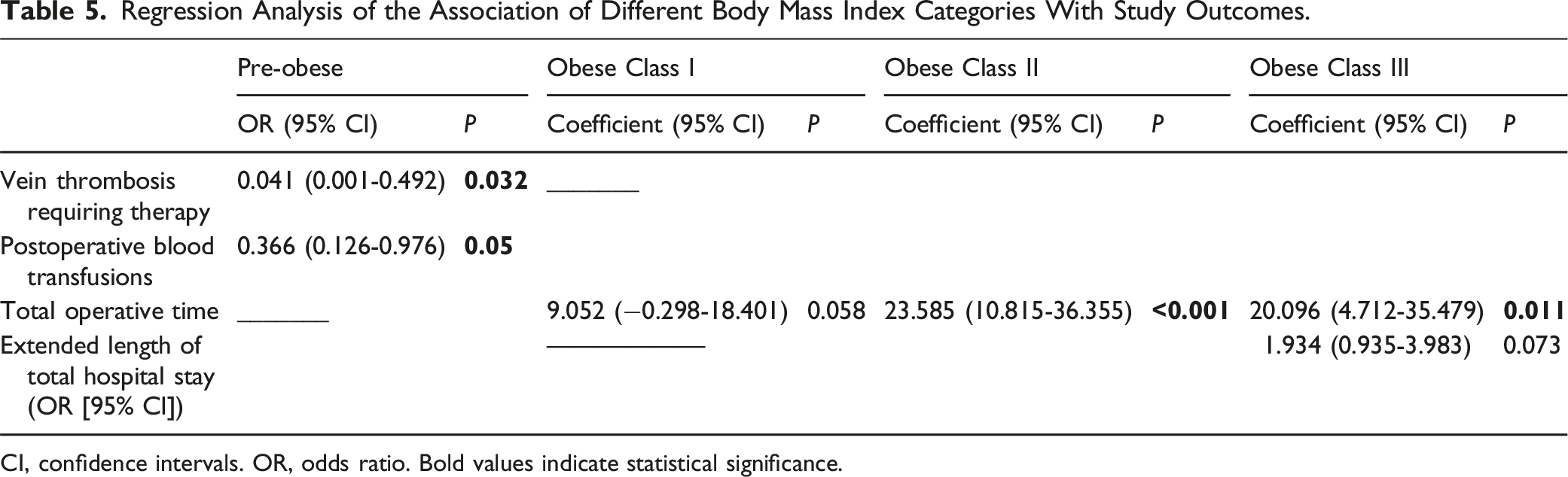
CI, confidence intervals. OR, odds ratio. Bold values indicate statistical significance.
Regression Analysis of the Association of Metabolic Syndrome With Study Outcomes.
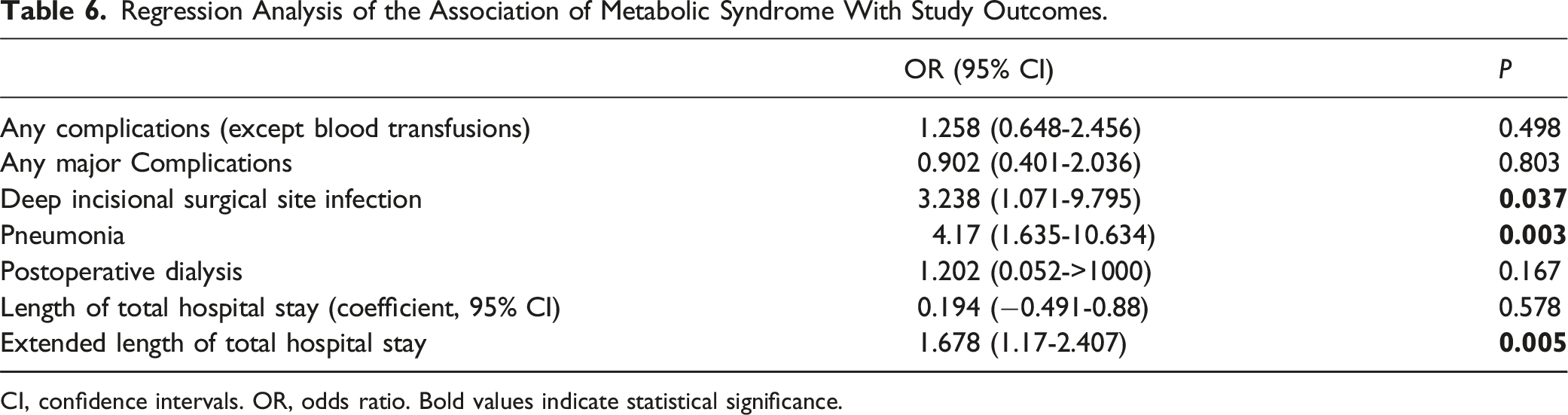
CI, confidence intervals. OR, odds ratio. Bold values indicate statistical significance.
Discussion
Summary of Findings
In this retrospective cohort of 2261 patients who underwent cervical laminoplasty, the overall complication rates, as well as the rates of major and minor complications, were similar among underweight, pre-obese, and class I-III obese patients when compared to those with normal weight. Furthermore, both the overweight groups and the underweight patients demonstrated comparable rates of individual complications documented in the ACS-NSQIP database. The length of total hospital stay, alongside readmission and reoperation rates, did not exhibit significant differences between normal-weight and all non-normal-weight groups. However, after adjusting for confounding variables in regression analysis, class II and III obesity were independently associated with longer operative times.
On the other hand, patients with metabolic syndrome had significantly higher overall and major complication rates compared to those without. Particularly, these patients experienced significantly higher rates of deep incisional SSI, postoperative pneumonia, and the need for postoperative dialysis. Furthermore, patients with metabolic syndrome had significantly longer hospital stays and faced a significantly higher risk of extended hospital length of stay. However, no significant differences were observed between the groups in terms of 30-day minor complications rates, readmission rates, reoperations, or total operative time. After adjusting for confounders, metabolic syndrome was independently associated with deep incisional SSI, postoperative pneumonia, and prolonged hospital stays.
Operative Times
While pre-obesity and obesity either had no impact or appeared to offer some protection against postoperative complications, class II-III obesity was independently associated with prolonged operative times, consistent with a previous single-center study. 29 This may be due to extended setup times with additional challenges in patient positioning and increased neck thickness in obese individuals. In posterior cervical spine procedures, excess adipose tissue necessitates more extensive dissection, retraction, and manipulation, thereby rendering surgical exposure and wound closure more challenging. These factors contribute to longer operative times and often necessitate larger incisions and extensive soft tissue dissection. Prior literature has highlighted the significance of minimizing operative time to reduce postoperative complications. 35 Although this study did not directly assess hospitalization costs, operative time can serve as an indirect indicator, suggesting that class II-III obesity may lead to higher surgical expenses. This finding aligns with previous findings showing that class III obese patients incurred greater total charges for spine surgeries compared to those with normal weight. 36
Postoperative Complications
Existing literature has demonstrated the detrimental effects of metabolic syndrome on cervical spine surgeries, particularly its association with an increased risk of SSIs. 20 In our study, metabolic syndrome was independently correlated with higher rates of deep incisional SSIs and postoperative pneumonia. The link between metabolic syndrome and SSIs may be attributed to diabetes-related vascular complications, which impair blood flow and delay wound healing, thereby elevating infection risks.37,38 Similarly, obesity has been correlated with poor postoperative wound healing, likely due to vascular insufficiencies and elevated oxidative stress. 20 Additionally, excessive subcutaneous fat in the posterior cervical spine necessitates prolonged and forceful retraction during surgery to optimize surgical site visualization, leading to tissue necrosis and increased exposure of subcutaneous tissue to environmental contaminants.39,40 Collectively, these comorbidities may synergistically heighten the SSI susceptibility. The relationship between metabolic syndrome and pulmonary complications, including pneumonia, has been well-documented as well.19,41,42
In addition to cervical spine surgery, metabolic syndrome has been recognized as a risk factor for adverse outcomes not only in lumbar spine surgeries19,42 but also in adult spinal deformity procedures. 43 Although metabolic syndrome is a relatively recent medical classification, its individual components, such as diabetes mellitus, 44 are well-established risk factors for poor cervical spine surgery outcomes. However, metabolic syndrome itself may represent a distinct and independent risk factor beyond its individual components. 45 For instance, a study by Lovecchio et al. 39 examined metabolic syndrome’s impact on lumbar spine surgery outcomes while adjusting for obesity. Their findings indicated that patients with metabolic syndrome exhibited increased wound complication rates, readmissions, and extended hospital stays compared to obese patients alone. This suggests that metabolic syndrome may involve more than just obesity; it encompasses immune dysfunction and chronic low-grade inflammation, linked by hormonal mediators, which possibly contributes to an increased susceptibility to infections.39,46,47 This postulation is consistent with the findings of our study, exhibiting notable differences in complication rates between patients with obesity and metabolic syndrome.
Limitations
This study was a retrospective observational analysis based on prospectively collected data. Therefore, it was unable to establish causal relationships and was susceptible to selection bias, treatment bias, and potential confounders. The ACS-NSQIP database, while extensive, has inherent limitations, including a predefined set of variables and a follow-up period restricted to 30 days. This brief follow-up may overlook the assessment of mid- and long-term complications, which should be considered when evaluating the risks associated with cervical laminoplasty. Moreover, the ACS-NSQIP database does not collect information on the pain severity, spinal pathology severity, spinal alignment, disability levels, utilized surgical techniques (eg, “open door” vs “double door”, along with multiple muscle sparing approaches 48 ), severity of complications, laminoplasty-specific variables (eg, neurologic deficits, characteristics of implants, number of operated vertebral segments, or functional outcomes), and preventative measures (eg, preoperative antibiotic administration or medication dosages). The absence of radiographic data further restricts analysis, requiring reliance solely on CPT codes.
Implications for Future Studies
Future multi-institutional prospective studies should leverage databases with extended postoperative follow-up periods to capture potential complications that may arise in the long term. These studies should utilize more detailed and specific datasets, incorporating technical surgical factors and laminoplasty-related variables, to further validate the findings of this study.
Conclusion
This study analyzed 2261 patients who underwent cervical laminoplasty for degenerative conditions using a multi-institutional, nationwide database, assessing clinical outcomes across different BMI categories and between those with and without metabolic syndrome. The findings revealed no significant differences in overall, minor, or major complication rates, hospital LOS, readmission rates, or reoperation rates among underweight and overweight patients compared to those with normal BMI within the 30-day postoperative follow-up period after adjusting for confounding variables. These results suggest that extreme BMI levels may not necessarily be associated with a higher rate of unfavorable perioperative outcomes after cervical laminoplasty, in contrast to many other cervical spine procedures. However, class II-III obesity was independently associated with prolonged operative times. Therefore, even modest weight loss in the preoperative window, such as lowering BMI by one classification, may help decrease operative time in class II-III obese patients, potentially mitigating associated surgical risks and costs. However, it is essential that future prospective studies evaluate the feasibility and efficacy of this preventive measure, given that many patients likely received laminoplasty for cervical myelopathy. Additionally, although the risks remain acceptable, the findings indicated that metabolic syndrome is independently associated with adverse perioperative outcomes, including a higher incidence of deep incisional SSI, pneumonia, and extended hospital stays. Given these findings, preoperative strategies such as strict serum glucose control and optimal hypertension management may help lower surgical risks and associated costs. Surgeons should anticipate these complications in patients with metabolic syndrome and implement stringent infection-prevention protocols. This information can aid physicians in counseling patients with different BMI categories or patients with metabolic syndrome who are candidates for cervical laminoplasty.
Supplemental Material
Supplemental Material - The Impact of Body Mass Index and Metabolic Syndrome on Perioperative Outcomes Following Cervical Laminoplasty
Supplemental Material for The Impact of Body Mass Index and Metabolic Syndrome on Perioperative Outcomes Following Cervical Laminoplasty by Ataollah Shahbandi, Pegah Ghamasaee, Abdul Mounnem Yassin Kassab, and Saman Shabani in Global Spine Journal
Footnotes
Author contributions
AS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft. PG: Writing – review & editing. AMYK: Writing – review & editing. SS: Conceptualization, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors report no conflict of interest or funding source. American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) and the hospitals participating in the ACS NSQIP are the sources of the data used herein; They have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Data used in this study is available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.