
Abstract
Study Design
Scoping review.
Objective
To review the literature on complications related to uniportal and unilateral biportal endoscopic techniques for lumbar spinal stenosis, identify areas needing further clarification, and enhance the understanding of these techniques.
Methodology
A scoping review was conducted in September 2024 across five databases (Google Scholar, Medline, Embase, PubMed, and Web of Science) on complications related to uniportal and unilateral biportal interlaminar endoscopic decompression for lumbar spinal stenosis. Descriptive characteristics, trends, and regional distribution of studies were summarized. Study types, findings, and complications for each technique were tabulated. A comparison of complication rates was performed between the two techniques to assess their relative safety and outcomes.
Results
A total of 38 studies involving 2426 patients (17 Uniportal, 17 Biportal, 4 comparing both) were analyzed, with L4-L5 being the most common level operated. The overall complication rate was 2.7% for uniportal and 2.2% for biportal, with reporting inconsistencies noted. Persistent symptoms after surgical decompression were more common in the uniportal group (P = 0.003), while postoperative headaches were higher in the biportal group (P = 0.007). However, the number of studies reporting these complications was limited.
Conclusion
Both uniportal and unilateral biportal endoscopic techniques are effective for lumbar spinal canal decompression, with no significant difference in complication rates. However, inconsistent reporting across studies limits meaningful meta-analyses. Future research should standardize the reporting of complications to ensure more reliable results and improve research quality.
Keywords
Introduction
Endoscopic spine surgery has emerged as one of the preferred minimally invasive approaches for treating various spinal pathologies, predominantly of degenerative etiology. 1 A few decades ago, open surgery was the gold standard for treating most spinal ailments. However, in the 1980s, Kambin and Hijikata made the first attempts at endoscopic spine procedures, laying the foundation for modern minimally invasive spine surgery.2,3 However, the breakthrough happened in the 1990s, when Kambin 4 reported the safe triangle through the neural foramen, enabling a transforaminal approach to reach the disc space. Later years, saw endoscopic arrival in a much familiar interlaminar approach. The primary advantage of these procedures is their ability to preserve the integrity of spinal soft tissue and bony structures through precise targeting.5-7 In addition, endoscopy offers a lower risk of complications, minimized blood loss, and expedited postoperative recovery, making it a viable option for degenerative pathologies such as degenerative disc disease and lumbar spinal stenosis.8,9
Over the years, uniportal and unilateral biportal endoscopic (UBE) techniques have been described extensively in the literature, each with its learning curve.10,11 Proponents of uniportal endoscopy suggest it is the least invasive surgical strategy, with decompressive procedures performed through a single surgical incision. However, biportal endoscopic surgeons argue that adding an additional incision improves the maneuverability of surgical instruments and reduces the learning curve.12,13 Practically, the indication for surgery, surgical expertise, and experience of the surgeon dictates the need for either of these procedures. However, it is not without complications, that one can master these techniques and perform effectively. Minimizing these complications in endoscopic technique is crucial in optimizing patient outcomes. 14 Especially in pathologies like lumbar spinal stenosis, chances of dural tear, and nerve root injury could be higher as bilateral decompression has to be performed from a unilateral approach using over-the-top interlaminar endoscopic approach.10,15,16 However, the literature on the complications of endoscopic decompression for lumbar spinal stenosis is variable and inconsistent between uniportal and biportal techniques. Hence, we performed a scoping review of the available literature, to assess the lacuna, identify the knowledge gaps, and investigate for further improvements in understanding the complications in endoscopic decompression of lumbar spinal stenosis.
Materials and Methods
Design
This scoping review was conducted in accordance with the Joanna Briggs Institute (JBI) scoping review guidelines, 17 and reported following the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) framework. 18 In keeping with the nature of scoping reviews, where formal quality appraisal is typically not performed, the selection of studies was intentionally broad, encompassing a range of study types and sample sizes. Although distinct from systematic reviews in objective, we employed a systematic approach to literature search, study selection, and data extraction to ensure methodological rigor. Our primary objective was to survey the available evidence, identify key concepts and research gaps, and provide contextual insights to help readers critically assess and interpret the existing data, thereby mapping the breadth of existing knowledge and also capturing the evolving landscape.
Eligibility Criteria
Only original studies published in English and in full-text format were eligible if they: (i) included patients with lumbar spinal stenosis who underwent endoscopic decompression using either the uniportal or UBE technique, (ii) involved an interlaminar approach, including over-the-top decompression, and (iii) reported complications during the procedure, defined as any adverse event or undesirable outcome occurring during or after surgery. Studies were excluded if they: (i) did not report any data on complications, (ii) used the transforaminal uniportal technique, (iii) used the paraspinal biportal technique, (iv) performed only unilateral decompression or discectomy without over-the-top decompression, or (v) were case reports. This stringent selection criterion was applied to facilitate a comparison of complications associated with the commonly practiced uniportal and unilateral biportal endoscopic techniques.
Identification and Selection of Studies
A comprehensive search strategy was developed using a combination of keywords, subject headings, and phrases. Searches were conducted on September 15, 2024, across five databases: Google Scholar, Medline (Ovid), Embase (Ovid), PubMed, and Web of Science. A search string customized for the specific search engines was employed, incorporating keywords such as “lumbar spine,” “spinal stenosis,” “endoscopic surgery,” “uniportal,” “unilateral biportal,” “over-the-top decompression,” and “postoperative complications.” Searches were limited to the English language only and duplicates were removed before extracting articles for screening of titles and abstracts. Screening was performed by two independent researchers, and in case of disparity, the help of a third reviewer was sought to facilitate consensus. Following title and abstract screening, full-text review was performed by two independent reviewers to identify the final list of studies to be included in the research.
Data Extraction and Analysis
Data extraction was carried out by the same two reviewers who performed the full-text screening. For each included study, general information such as study design, country of conduct, and sample size was collected. This information summarizes the descriptive characteristics of all included studies, including study type, trends over time, and regional distribution. Additionally, two tables compile the included studies: one on the uniportal endoscopic technique and the other on the biportal endoscopic technique. Each table provides details on the study type, main findings, and conclusions, with a specific focus on complications.
Identification of Eligible Studies
Our search and screening process is presented in Figure 1 (Figure 1). In summary, 428 records were initially identified, and after removing duplicates, 212 article titles and abstracts were screened for eligibility. A total of 114 articles were shortlisted for full-text review, and 38 studies met the inclusion criteria. These 38 studies assessed a total of 2426 patients. Complications reported in these studies were recorded, and statistical analysis was conducted using GraphPad Prism 9 (GraphPad Software Inc., San Diego, CA). Fisher’s Exact test was used to compare complication rates between the uniportal and biportal techniques, with a P-value <0.05 considered statistically significant. Screening and identification of eligible studies.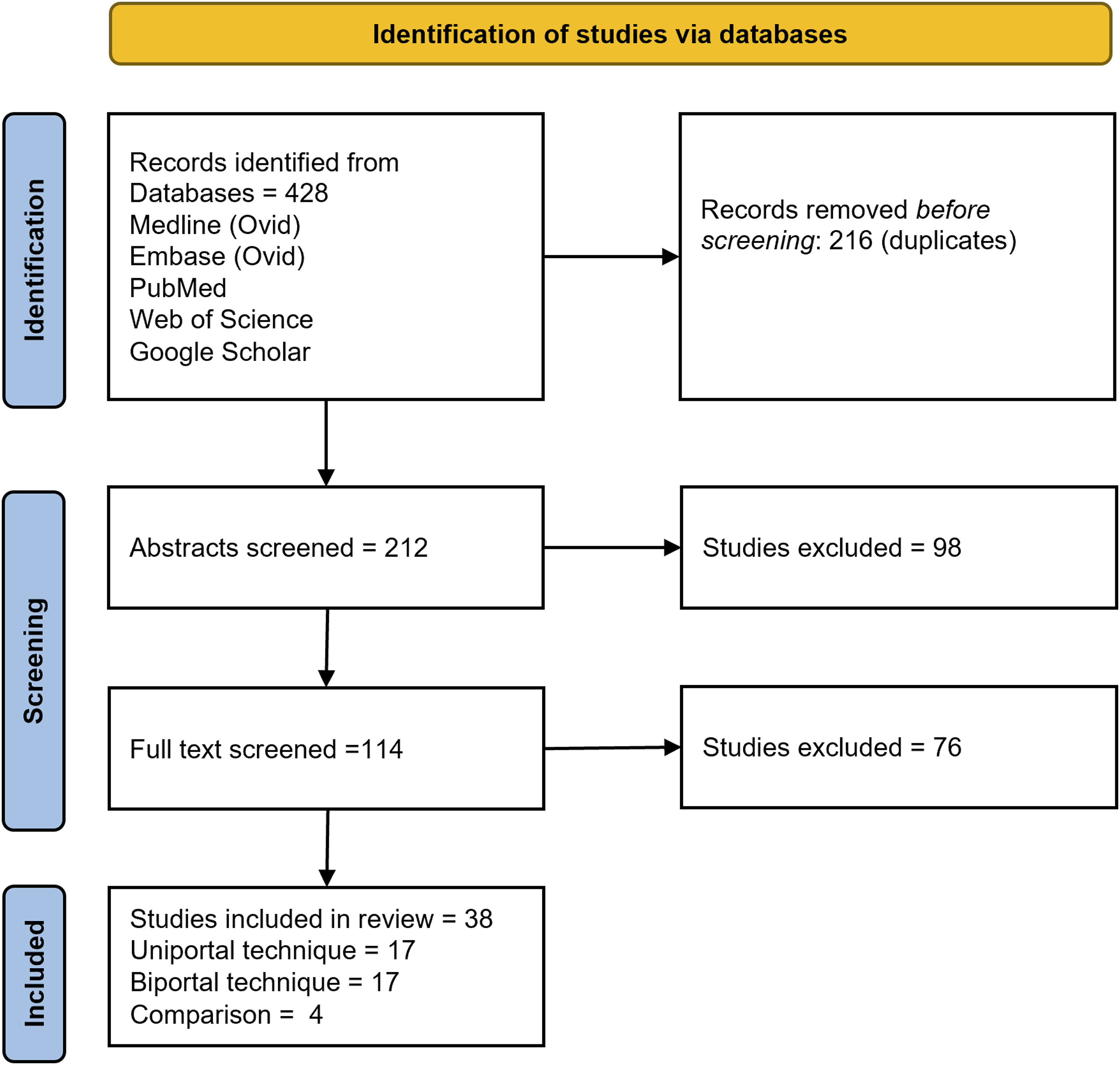
Results
Study Characteristics and Patient Demographics
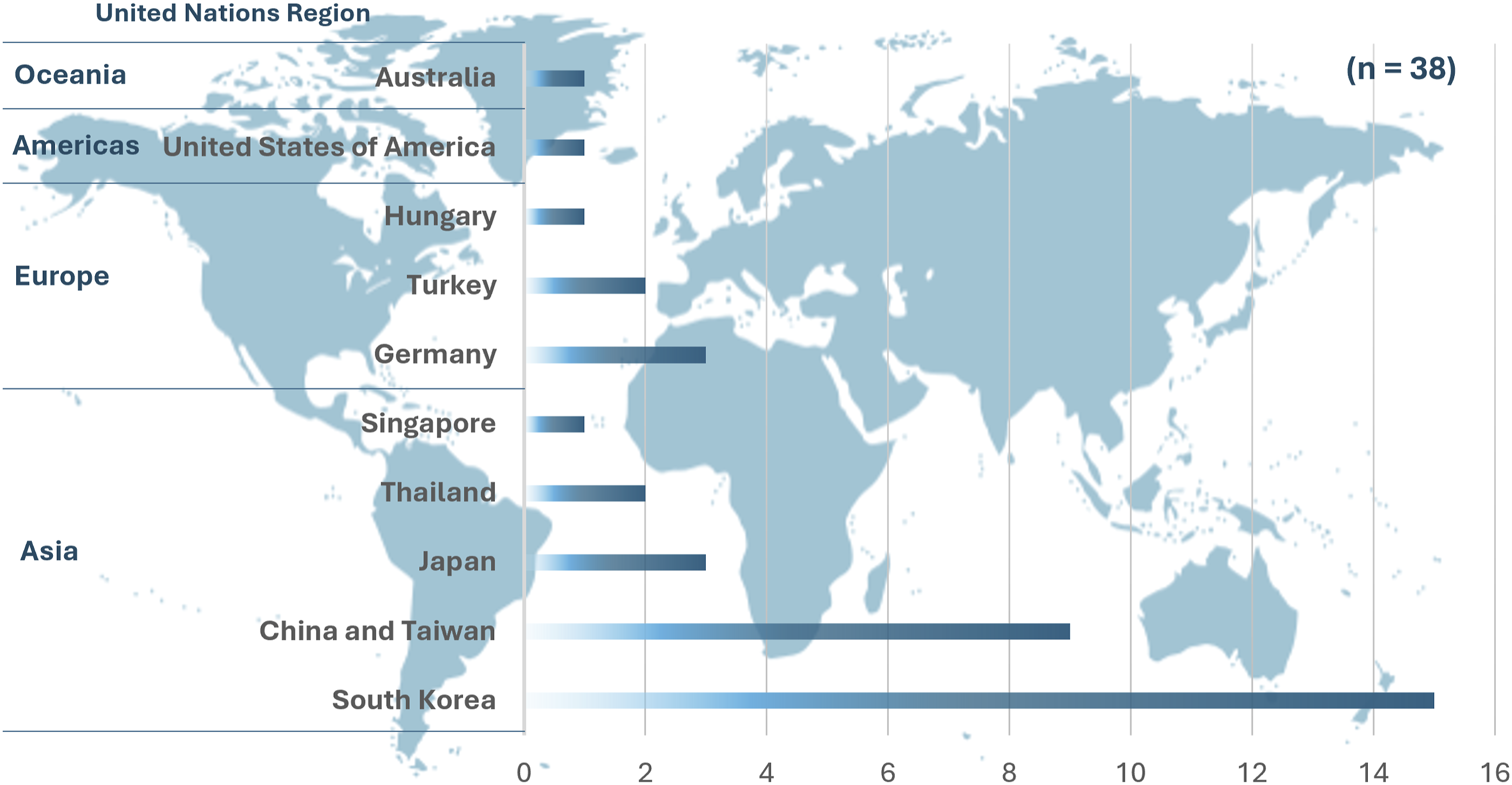
A total of 38 studies were included in our review, examining 2426 patients (Supplementary Table 1, 2). Of these, 17 studies focused on uniportal, 17 on biportal, and 4 compared uniportal and biportal endoscopic techniques. Among those, only one study was published between 2000 and 2010, while 37 studies were published after 2010 (Figure 2). The included studies were conducted in various countries from around the world and the geographical distribution of the included studies is categorized according to the United Nations regions (Figure 3). The majority of the publications are from Asia, including South Korea (15 studies), China and Taiwan (9 studies), Japan (3 studies), Thailand (2 studies), and Singapore (1 study). Europe contributed 6 studies, with Germany (3 studies), Turkey (2 studies), and Hungary (1 study). The Americas contributed 1 study from the United States of America, while Oceania contributed 1 study from Australia. The number of included studies on endoscopic decompression for lumbar spinal stenosis published each year. Regional distribution of articles according to United Nations regions.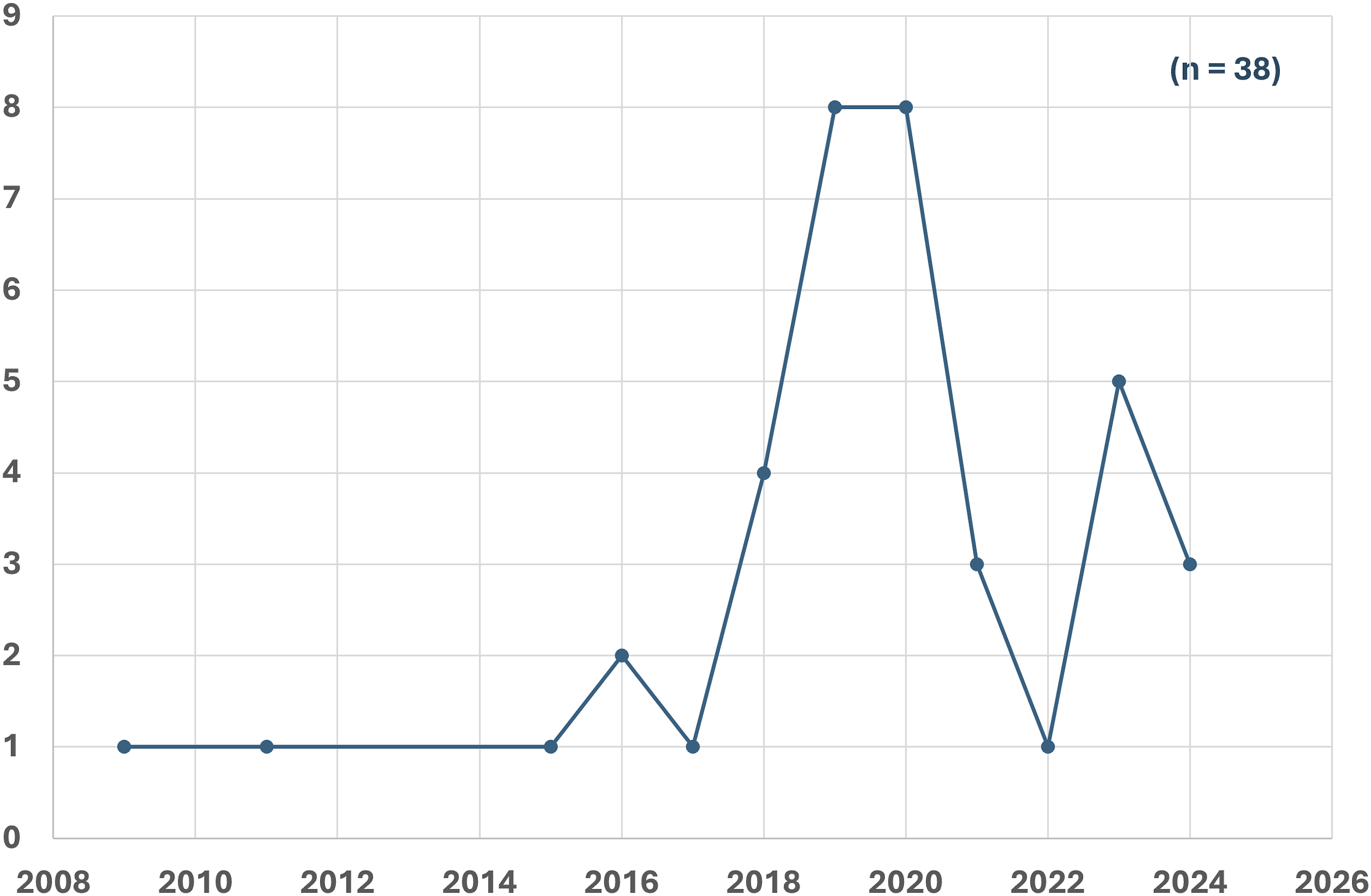
Overall, 20 studies were comparative, including 4 comparing uniportal vs biportal, 1 comparing biportal vs arthroscopic-assisted uniportal, 10 comparing endoscopic vs microscopic, 3 comparing endoscopic vs tubular, and 2 comparing endoscopic decompression vs fusion. Uniportal decompression was performed on 1309 patients, while 1211 patients underwent biportal decompression. Among the patients, 1051 were male and 1282 were female. However, one study by Reutten et al on uniportal endoscopic decompression did not report the gender distribution in their study population. The mean age of the population was 64.7 ± 7.9 years, and the average BMI was 25.8 kg/m².
Surgical Parameters
The most common level operated on was L4-L5 (1406 patients), followed by L5-S1 (474 patients), with 354 patients undergoing surgery at L3-L4, 64 at L2-L3, five at L1-L2, and one at T11-T12. Only twenty-two studies mentioned the site of stenosis as central or lateral recess stenosis. Regarding the endoscope used during surgical decompression, of the 38 studies, only 18 (7: Uniportal, 11: Biportal) reported on scope characteristics. The commonly used scope angles varied between 10° and 30° for uniportal endoscopy and 0° to 30° for biportal endoscopy. Data on saline dynamics and pressure were reported in only 11 studies (2: Uniportal, 9: Biportal), with pressure values ranging between 20 and 60. The mean follow-up period was 16 months.
Complications Reported
Intraoperative dural tears were reported in almost all studies, except for two (21: Uniportal; 19: Biportal). Overall, out of 2317 patients (1309: Uniportal; 1008: Biportal), 73 patients (41: Uniportal; 32: Biportal), or 3.2%, experienced a dural tear. Most of these cases were treated conservatively without repair. Two patients underwent endoscopic repair (one with vascular clipping), six patients were treated with dural patch substitutes, and in five cases, the procedure was converted to open surgery for repair (two of which involved muscle flap repair).
Sensory disturbance, dysaesthesia, or paraesthesia was reported in 12 studies (9: Uniportal; 3: Biportal). A total of 40 patients (35: Uniportal; 5: Biportal) out of 777 patients (656: Uniportal; 121: Biportal) (5.4%) experienced dysaesthesia. All reported dysesthesia was transient, and only three studies documented the duration of recovery: Xin et al (within 6 months), Lee et al (3 months), and Zhao et al (2-3 weeks).19-21 However, 15 patients (35.7%) required interventions, such as selective nerve root blocks or epidural steroid injections, during the follow-up period.
Post-operative motor deficits were reported in 9 studies (8: Uniportal; 1: Biportal). Among 798 patients (716: Uniportal; 82: Biportal), 15 patients (14: Uniportal; 1: Biportal), or 1.9%, experienced weakness after surgical decompression. This weakness was reported as transient in 13 patients (86.7%). However, the duration of recovery was only mentioned in two studies. In addition, nerve injury or cauda equina injury was reported in 20 studies (13: Uniportal; 7: Biportal), affecting 12 patients (6: Uniportal; 6: Biportal), or 0.8%, out of 1434 patients (978: Uniportal; 456: Biportal).
Persistent symptoms following decompression were reported in eleven studies (5: Uniportal; 6: Biportal). Among 876 patients, 36 patients (25: Uniportal; 11: Biportal; 4.1%) did not experience resolution of symptoms after surgery. Of these, 25 patients underwent reoperation. However, data regarding whether the persistent symptoms occurred on the side of docking the scope or the contralateral side (over the top) was not provided in any of these studies.
Post-operative hematoma was reported in 22 studies (10: Uniportal; 12: Biportal). Among the 1341 patients (791: Uniportal; 550: Biportal) included, 27 patients (16: Uniportal; 11: Biportal), or 2%, developed a symptomatic post-operative hematoma. Data on the management of the hematoma were reported in only nine cases, with 3 managed conservatively, 3 with endoscopic evacuation, and 3 with open evacuation.
Post-operative headaches were reported in 4 studies (1: Uniportal; 3: Biportal). Among 261 patients (127: Uniportal; 134: Biportal), 8 patients (3%) developed a post-operative headache, all of whom were in the biportal group. Dural tears were identified as a possible cause in three cases, and excess saline volume was reported in two cases. Although statistical significance was observed when comparing uniportal and biportal, the number of studies reporting these complications was not comparable.
Recurrence was reported in only two studies (one for uniportal and one for biportal). Overall, 14 patients (13: Uniportal; 1: Biportal) out of 149 patients (128: Uniportal; 21: Biportal) developed recurrence, which is 9.4% of the cases. Additionally, reoperation was reported in 21 studies (12: Uniportal; 9: Biportal). Among 1377 patients (988: Uniportal; 389: Biportal), 48 patients (38: Uniportal; 10: Biportal) underwent reoperation during the follow-up period. The causes for reoperation included foraminal stenosis, inadequate decompression, and hematoma. Of these, 9 patients underwent fusion, 10 patients had further decompression, and for 29 patients, no data regarding the revision surgery were provided in the studies.
Among other complications, post-operative surgical site infection (SSI) was reported in 26 studies (13: Uniportal; 13: Biportal). Among 1596 patients (860: Uniportal; 736: Biportal), only one patient (in the biportal group) developed SSI. However, data on the severity and management of the infection were not reported. Additionally, intra-operative breakage of the scope lens and conversion to micro decompression occurred in one patient who underwent uniportal endoscopic decompression. 22 Zhijun et al reported intraoperative spinal venous hypertension myelopathy in their study on patients undergoing uniportal endoscopy. 19 Here, three patients were reported with the complication and presented with a stiff neck, eye distention, and tinnitus. The symptoms improved by reducing the perfusion and intermittent short-stop processing. Drain tube trouble was reported by Yoshikane et al 23 in two patients undergoing uniportal endosopic decompression. Delayed wound healing was reported in three patients who underwent uniportal endoscopic decompression, and two of these patients underwent debridement under local anesthesia.24,25
Among all complications, persistent symptoms following decompression was more common in the uniportal endoscopy group, while the incidence of postoperative headache was higher in the biportal endoscopy group. The difference was statistically significant (P < 0.05) (Figure 4). However, the number of studies reporting these complications was limited, and the sample sizes for both groups were relatively small, which may reduce the significance of the results. All other complications were similar between the two groups. Pie charts showing the number of studies, patients, and complication rates for both uniportal and biportal endoscopic decompression along with statistical significance.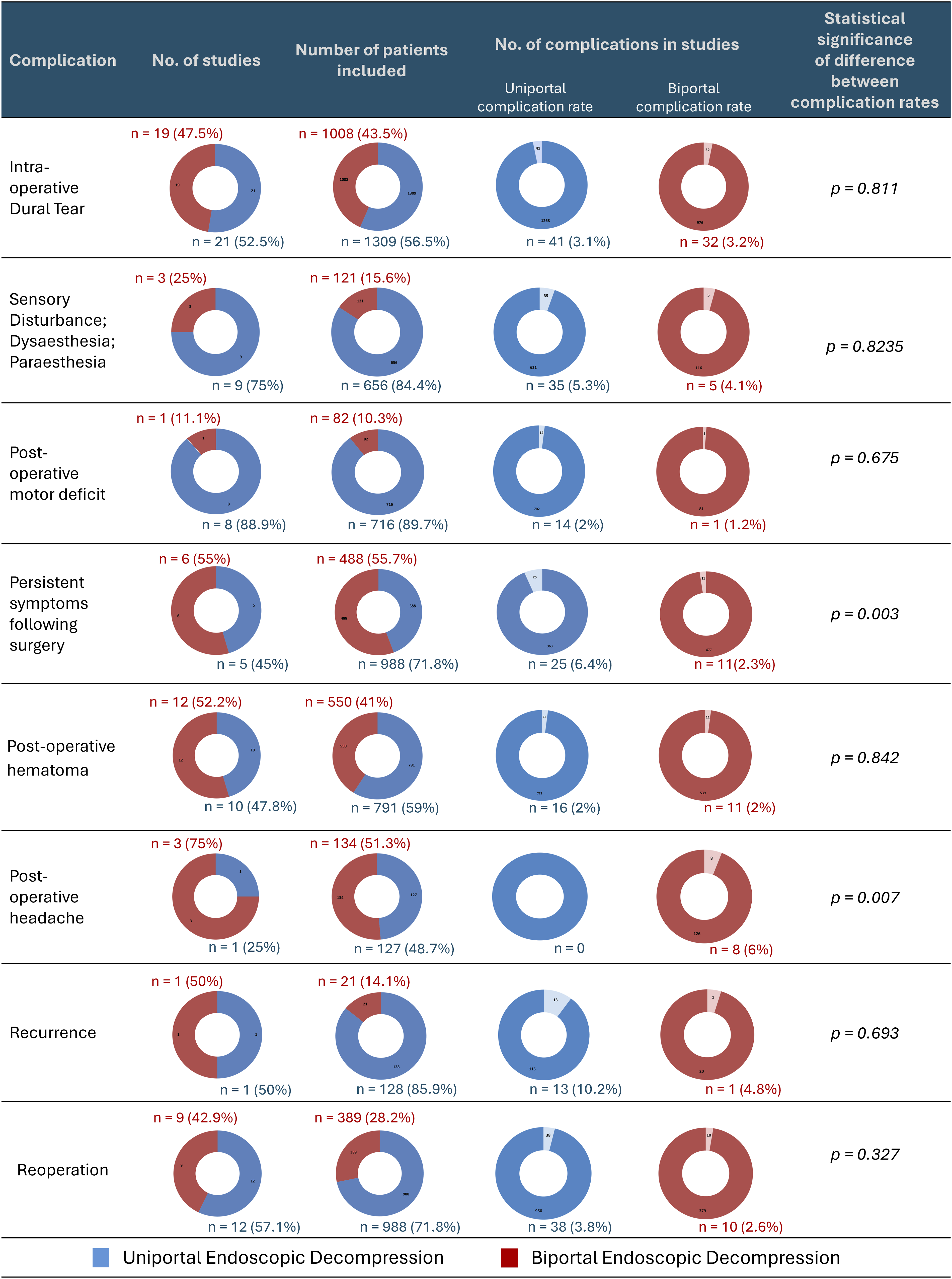
Discussion
Spinal endoscopy is a relatively new field compared to advancements in general surgical endoscopy or arthroscopy in orthopaedic surgery. However, its growth has been rapid. This is evident even when examining reported complications, as only two studies were published between 2000 and 2010, whereas 44 studies were published after 2010 among those selected for this review. While Asian studies have contributed the most to understanding complications, research has also emerged from a diverse range of countries. Among all complications, persistent symptoms after surgical decompression were more common in the uniportal group, whereas the incidence of postoperative headache was higher in the biportal group. These were the only two significantly different parameters comparing the two techniques; however, the number of studies reporting these complications was limited, and the sample size was relatively small. Hence, more studies are required to gain a clearer understanding of complications following these techniques. Moreover, authors need to report all complications, whether minor or major, to enable future meta-analyses to draw definitive conclusions.
Looking into the specifics, dural tear is the most reported complication in studies on both uniportal and biportal decompression for lumbar spinal stenosis. In endoscopic spine surgery, dural tears may go unnoticed intra-operatively due to the continuous flow of irrigation fluid in the surgical field, often becoming symptomatic only in the post-operative period. A meta-analysis by Wang et al 26 reported a 2.5% incidence of dural tears in patients undergoing endoscopic decompression for lumbar spinal stenosis, which is comparable to our study’s findings (3%). Several key factors contribute to dural tears in spinal endoscopy: (i) poor endoscopic visualization of the thecal sac and nerve roots due to inadequate hemostasis; (ii) midline dural fold formation caused by irrigation fluid pressure, increasing the risk of dural laceration during decompression; (iii) forceful removal of thick meningo-vertebral ligaments attached to the dura; (iv) entanglement of fibrous bands in the epidural space with a high-speed burr, leading to large dural lacerations. Additionally, in cases of severe stenosis, thick adhesions between the dura and the ligamentum flavum may further increase the risk of dural tears. 27 In such instances, the fluid inflow during the endoscopic procedure could aid in releasing adhesions below the flavum through a hydro-dissection effect. However, data on the size of these tears and the specific intra-operative steps leading to their occurrence are lacking in the studies. It is generally believed that small tears (<5 mm) can be managed conservatively without the need for further intervention.28,29 Other strategies reported include primary repair through the endoscope, the use of non-penetrating clips, muscle flaps, dural sealants, sealing with a collagen fibrin patch, and conversion to open surgery for repair.30-34 Overall, the success rate of managing these tears under endoscopy is high, regardless of the method used. This may be attributed to the tight space available for cerebrospinal fluid (CSF) accumulation, unlike in open spine surgeries.
Post-operative headache is a complication often associated with dural tears or meningeal irritation caused by the high pressure of saline used during endoscopic spine surgery. In our study, eight patients developed headaches postoperatively, all of whom were in the biportal endoscopy group. However, the number of studies reporting this complication was limited. Unlike uniportal surgery, biportal technique involves separate portals for saline inflow and outflow. If the outflow is obstructed or irregular, increased saline pressure can result in meningeal irritation. 35 We recommend improving the outflow by making a cruciate incision in the fascia during biportal endoscopic surgery and avoiding an increase in the height of the saline bag or pressure in the saline pump. Choi et al reported the incidence of seizures following percutaneous endoscopic lumbar discectomy and suggested that the saline pressure in the irrigation pump should be maintained below 30 mmHg to reduce the occurrence of neck pain, headaches, and seizures.36,37
Another aspect of discussion is post-operative hematoma. Since the endoscopic working space is narrow, there is a higher likelihood of hematoma formation at the surgical site. Oozing from cancellous bone can contribute to this hematoma formation. Moreover, when using pump-assisted saline inflow, continuous saline irrigation is maintained. Here, if the outflow of saline is impaired, the resulting increase in pressure within the surgical field can temporarily cover bleeding points, leading to intraoperative hemostasis. 38 Later, these sites may start to bleed contributing to the epidural hematoma. Hence, it is of utmost importance to secure proper hemostasis before wound closure. 39 For this reason, it is common for surgeons to use fibrin sealants for hemostasis in endoscopic spine surgeries. However, studies don’t include this information. Placing a drain at the surgical site helps to drain excessive irrigation fluid or any collection. However, Park et al, in their study, noted that improper positioning of the drain is one of the causes of post-operative hematoma.40,41 Yoshikane et al 23 also reported complications related to drain use in endoscopy. In both uniportal and biportal surgeries, the drain is placed under endoscopic view. However, once the endoscope is removed while securing the drain, there is always a possibility of the drain being withdrawn from the decompressed site. The overlapping paraspinal musculature may obstruct proper drainage of the hematoma, leading to post-operative symptoms. Therefore, utmost care must be taken during the placement of the drain tube in these patients.
Sensory-motor weakness is an important outcome in any spine surgery. In the context of endoscopic procedures, studies have shown that the risk of paresthesia is more common with the transforaminal technique compared to the interlaminar technique due to irritation of the exiting nerve root.42,43 Based on our assessment of the interlaminar technique, the overall incidence of paresthesia noted in our study was 5.2%. Most reports of paresthesia in the included studies have been transient, and the duration of the paresthesia was mentioned in only three studies.19-21 The common causes of paresthesia in endoscopic lumbar spine surgeries include manipulation and traction of the traversing nerve root, the use of a high-dosage radiofrequency (RF) probe near the nerve root, and aggressive adhesiolysis. Based on our experience, to reduce the risk of paresthesia, we suggest gradual and gentle mobilization of the traversing root using the scope retractor and intermittent release of traction of the nerve root. In cases that require additional disc removal, it is essential to rotate the endoscopic sleeve (uniportal) and scope retractor (unilateral biportal) only after securely placing them over the disc. When performing flavectomy, care should be taken to release the adhesions underneath the flavum using the Kerrison rongeur (uniportal) or a 90° broad RF probe (unilateral biportal) before removing the flavum, either piecemeal or en bloc. Additionally, when using an RF probe, the surgeon should be cautious and reduce the thermal energy dosage in the epidural space compared to working over the flavum. With regard to motor weakness, the overall incidence of post-operative motor weakness in the reported studies was 10%, with 13 cases being transient. While we could postulate that direct trauma to the nerve root from the RF probe, injury from the nerve root retractor and rongeurs, as well as significant post-operative hematoma, could contribute to motor weakness, no studies have identified the specific causes leading to post-operative motor deficits.
A major concern in spinal stenosis surgery is the persistence of symptoms, which can lead to a failed surgery. Based on our assessment, although the overall incidence of inadequate decompression or persistent symptoms was low, a higher occurrence was observed in the uniportal group compared to the biportal group, and this difference was statistically significant. However, the studies lacked data on whether the persistent symptoms occurred on the side of docking the scope or on the contralateral side (over the top). When operating through the endoscope, it is important to remember that the thecal sac is collapsed due to the saline pressure and water-based medium. Therefore, it is optimal to visualize the lateral margin of the traversing nerve roots and decompress at least 2-3 mm from the lateral margin of the root to ensure adequate decompression. Blurred vision due to bleeding and reduced saline flow pressure can also contribute to inadequate decompression. In lumbar spinal stenosis, the common site of bony compression is the medial and inferior part of the superior articular process, and adequate bony removal at the “J” point is crucial for visualizing the traversing nerve root. We recommend palpating the medial border of the pedicle to ensure the adequacy of decompression and to confirm that the nerve root is free from compression.
Although not everyone with persistent symptoms requires reoperation, some do, and the overall reoperation rate, as evidenced in this study, was 3.5%. Common causes for reoperation include foraminal stenosis, hematoma formation, and inadequate decompression. Based on our experience, post-operative instability, although not mentioned in any of the studies, is another important risk factor for reoperation. This could result from excessive drilling of the pars during laminectomy or significant violation of the facet joint. To prevent pars fractures, it is crucial to avoid drilling above the level of the free edge of the flavum. Additionally, a careful pre-operative assessment of the facet joint is essential. Any presence of facet tropism or abnormal sagittal facet orientation should alert the surgeon to the risk of post-operative instability. In such cases, a contralateral facet-sparing approach may be a safer surgical option. 44 Lastly, surgical site infections (SSI) must be discussed, though they are rare. The rarity of SSI is primarily due to the continuous inflow of saline, minimal soft tissue trauma, and shorter operation times associated with these procedures. In our study, only one case of infection was reported, while three patients experienced delayed wound healing and were treated with debridement under local anesthesia.
This review is the largest comparison of complications between uniportal and unilateral biportal endoscopic techniques for lumbar spinal stenosis to date. Our analysis indicates that the overall complication rates for both techniques are comparable. However, conducting a meta-analysis was challenging due to inconsistent data across studies, with key details such as scope characteristics and saline dynamics often omitted. Additionally, there is a lack of standardization in how complications are reported. To improve the understanding of complications associated with these techniques, we recommend implementing a standardized classification system that categorizes complications as major (eg, dural tear, dysesthesia/paresthesia, post-operative motor deficit, hematoma, persistent symptoms) and minor (eg, post-operative headache, SSI, delayed wound healing). Future studies should also provide detailed management strategies for these complications to better inform mitigation strategies. While no significant difference in complications was found between the two groups, the results may be influenced by inconsistent reporting practices across studies.
Limitations
Being a scoping review, this study aimed to provide a broad overview of literature rather than conduct a critical appraisal or quantitative synthesis. As such, no formal risk of bias assessment or rigorous statistical analysis was performed. Moreover, inconsistencies in the definition and reporting of complications across studies hinder meaningful data pooling and limit the ability to draw definitive conclusions. Consistent reporting across future studies would facilitate meta-analyses and allow a more robust head-to-head comparison of the two techniques. Additionally, given the evolving nature of endoscopic techniques and rapid advances in surgical practice, temporal variation across studies may have acted as a confounding factor. Nevertheless, the broad inclusion enabled us to capture the evolving landscape, map existing evidence, identify key concepts, and highlight areas for future research.
Conclusion
Both uniportal and unilateral biportal endoscopic interlaminar techniques are effective minimally invasive approaches for decompressing the lumbar spinal canal, with no significant difference in complication rates based on our assessment of the available data. However, the inconsistency in reporting complications across studies limits the ability to perform meaningful meta-analyses and draw definitive conclusions. To address this, future studies should follow a standardized protocol for reporting both major and minor complications. This will help ensure more reliable results and contribute to the overall improvement of research quality in this field.
Supplemental Material
Supplemental Material - Complications in Uniportal vs Unilateral Biportal Endoscopic Decompression for Lumbar Spinal Stenosis: A Scoping Review
Supplemental Material for Complications in Uniportal vs Unilateral Biportal Endoscopic Decompression for Lumbar Spinal Stenosis: A Scoping Review by Guna Pratheep Kalanchiam, Arun-Kumar Kaliya-Perumal, Lokesh Sampath, Elijah Tzen Hsuen Boey, and Jacob Yoong-Leong Oh in Global Spine Journal.
Footnotes
Author Contributions
All authors contributed to the conceptualization and design of the study. GPK, AKKP, and LS performed data curation. GPK, AKKP, LS, and ETHB conducted the formal analysis and investigation. GPK, AKKP, LS, and ETHB prepared the first draft of the manuscript. AKKP and JYLO reviewed and edited the manuscript for important intellectual content. All authors approved the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Data Availability Statement
The data used and analysed in the present study is provided within the article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.