
Abstract
Study Design:
Prospective cohort study.
Objective:
The lateral transpsoas access is a retroperitoneal approach for the lumbar spine to perform the lateral lumbar interbody fusion (LLIF), an intersomatic arthrodesis performed with a cage placed on the lateral borders of the epiphyseal ring. The procedure can be used to provide indirect decompression of the nervous structures through the discectomy and restoration of the disc height. The objective of the present study was to evaluate the indirect decompression following LLIF both with radiological and clinical parameters.
Methods:
Prospective clinical and radiological study in a single center with 20 patients diagnosed with 1- or 2-level degenerative lumbar stenosis. Radiological analysis on magnetic resonance imaging included foramen height, canal area, canal diameter, and disc height. Clinical outcomes included visual analogue scale (VAS) and Oswestry Disability Index (ODI) collected up to 12 months. Complications and reoperations were recorded.
Results:
In total, 25 levels were treated. No reoperation was required. Disc height was increased by an average of 25% (P < .001). The canal area increased from 109 to 149 mm2 (P < .001) and from 9.3 to 12.2 mm (P < .001) in anteroposterior diameter. The foramen area demonstrated the effect of indirect decompression on both sides (P < .001). The height of the foramen showed significant average increase of 2.8 mm (P < .001). The results from VAS and ODI questionnaires confirmed the clinical effect of indirect decompression.
Conclusion:
We observed that indirect decompression by the LLIF method is feasible both radiologically and clinically with a low rate of complications and reoperations.
Keywords
Introduction
The surgical treatment for degenerative lumbar spinal stenosis with posterior access with direct visualization of the neural elements are well established in the literature. 1,2 Direct decompression followed by interbody fusion has been accomplished with transforaminal lumbar interbody fusion (TLIF) or posterior lumbar interbody fusion (PLIF) techniques. 3,4 These techniques aim at the restoration of foraminal and discal heights, with insertion of intervertebral cage and fusion of the vertebral bodies associated with posterior fusion, due to the facetectomy of the posterior structures. 5 -7 However, these techniques require extensive muscular resection and longer hospital discharge time and involve greater blood loss and higher costs. 4
Less invasive techniques have been widely studied due to the more favorable clinical outcomes when compared with traditional techniques, such as the need not to remove the posterior elements of the support and the rapid recovery of the patient and shorter hospitalization time. 5,8 -10 Lateral lumbar interbody fusion (LLIF) has been evaluated in the past decade with benefits and clinical outcomes favorable to patients, with adequate complication rates and results on pain and quality of life. 3,4,11 -14
The basis of LLIF to treat acquired lumbar stenosis is to achieve indirect decompression of the neural structures with the restoration of anatomical corridors followed by wide discectomy, gain of disc height and ligamentotaxis. 13,15 Clinical studies have shown significant improvement of complains related to the stenosis. 13,16 The primary objective of the study was to evaluate the success of clinical and radiological outcomes of indirect minimally invasive decompression surgery with lateral lumbar arthrodesis technique.
Materials and Methods
Study Design
Prospective case series clinical and radiological study was carried out in the Spine Pathology Clinic of the Instituto de Ortopedia e Traumatologia in the HC-FMUSP hospital, with enrollment interval between November 2014 to January 2017. The study protocol was approved by independent research and ethics committee. All patients included signed an informed consent form.
Casuistic
Inclusion Criteria
Following were the inclusion criteria: skeletally maturate patients of both genders; aged 18 years or older but not older than 70 years; both clinical and radiological diagnosis of central and/or lumbar foraminal stenosis due to degenerative disc disease and/or spondylolisthesis less than or equal to grade II in 1, 2, or 3 consecutive lumbar levels; unsuccessful conservative care for at least 6 months; ASIA (American Spinal Injury Association) I or II.
Exclusion Criteria
Following were the exclusion criteria: previous fusion at the index level; degenerative joint disease, that prevents the indirect sliding/decompression; sagittal mismatch (pelvic incidence – lumbar lordosis) greater than 10°; clinically compromised vertebral bodies; spinal tumor; osteopenia, osteoporosis or osteomalacia, active local or systemic infection; rheumatoid arthritis or other autoimmune disease; pregnant or interested in becoming pregnant during the study period; mentally incapacitated patients; reluctant or unfit to comply with the follow-up protocol.
Surgery
The patients underwent LLIF technique with the transpsoas approach as described before. 13 The side of approach was chosen case by case according to lumbar and retroperitoneal anatomy of the patient. A single surgeon with advanced learning curve 17 performed all procedures. The interbody fusion was performed using polyetheretherketone 10° lordotic cages (CoRoent XL, NuVasive, Inc, San Diego, CA). The surgical technique used aims to place the cages in an anterior position of the interbody space (2 anterior thirds of the disc space). Lateral procedures were carried out with neuromonitoring (Neurovision, NuVasive, Inc, San Diego, CA). All cases received posterior supplementation with pedicular pedicle screws with less invasive approach (Wiltse or percutaneous technique).
Clinical Outcomes
The incidence of device failures, insufficient decompression, and need of reoperation at the index level were collected. Postoperative complications were also recorded, as well as any reduction of strength of the psoas muscle or any plexopathy. Patients answered the Oswestry Disability Index (ODI) 18 and the visual analogue scale (VAS) questionnaires to assess the perception of subjective pain radiated to the lower limbs and axial back pain. The patient-reported outcomes were collected in the preoperative period and after surgery at 6 weeks, 3 months, 6 months, and 12 months. Minimum clinically important difference (MCID) 19 was used as thresholds to measure the effect of clinical treatment for ODI (12.8 points), and VAS back pain (1.2 points) and VAS leg pain (1.6 points).
Radiological Outcomes
Simple radiographs (anteroposterior [AP] neutral, lateral in flexion, lateral in neutral and lateral in extension) were performed before surgery and at different postoperative periods to control the status of the construction: 6 weeks, 3 months, 6 months, and 12 months. Magnetic resonance imaging (MRI) exams of the lumbar spine were performed at baseline and at 3 months postoperatively for measurement of different radiographic parameters: (1) anterior and posterior disc height, (2) right and left foramen heights, (3) anteroposterior diameter of the spinal canal, and (4) area of the spinal canal. Radiological assessments were done using the digital visualization system iSite-Philips. Two evaluators independently evaluated the radiological parameters. The discrepancies were resolved by consensus.
Statistical Analysis
The normality of the data was evaluated by the Shapiro-Wilk test. Parametric variables were analyzed using the 2-tailed Student’s t test and nonparametric variables with the Mann-Whitney and Wilcoxon tests (P < .05), or Spearman, with a significance level of 5%. Data analysis was performed on IBM SPSS version 20 software. The following method was used to calculate the percentage method of expansion: final gain (in percentage) = (postoperative value – preoperative value)/(preoperative value).
Results
Baseline Clinical and Demographic Characteristics
Twenty patients were enrolled and 19 reached final follow-up (95% retention). Baseline data is shown in Table 1. Thirteen women (65%) and 7 men (35%), with mean age of 57.8 years (SD = 11.9, range 32-79 years), underwent lateral arthrodesis with the LLIF technique Twenty-five stenosis levels were treated in the 20 patients involved in this study, where 16 patients had surgery in 1 level (80%), 3 patients had 2 levels operated (15%), and 1 patient had 3 levels of surgery (5%). The most common level was the L4-L5, with 76% of the total, followed by L3-L4 (16%), and finally L2-L3 (8%). The mean coronal Cobb angle was 7° (SD = 5°). In 18 patients, there was supplementation with bilateral transpedicular fixation (90%), 1 patient with unilateral fixation (5%), and 1 patient without fixation (5%). Average length of stay was 2 days (range 1-3 days).
Results of Nuclear Magnetic Resonance Measurements With Pre- and Postsurgical Values.a
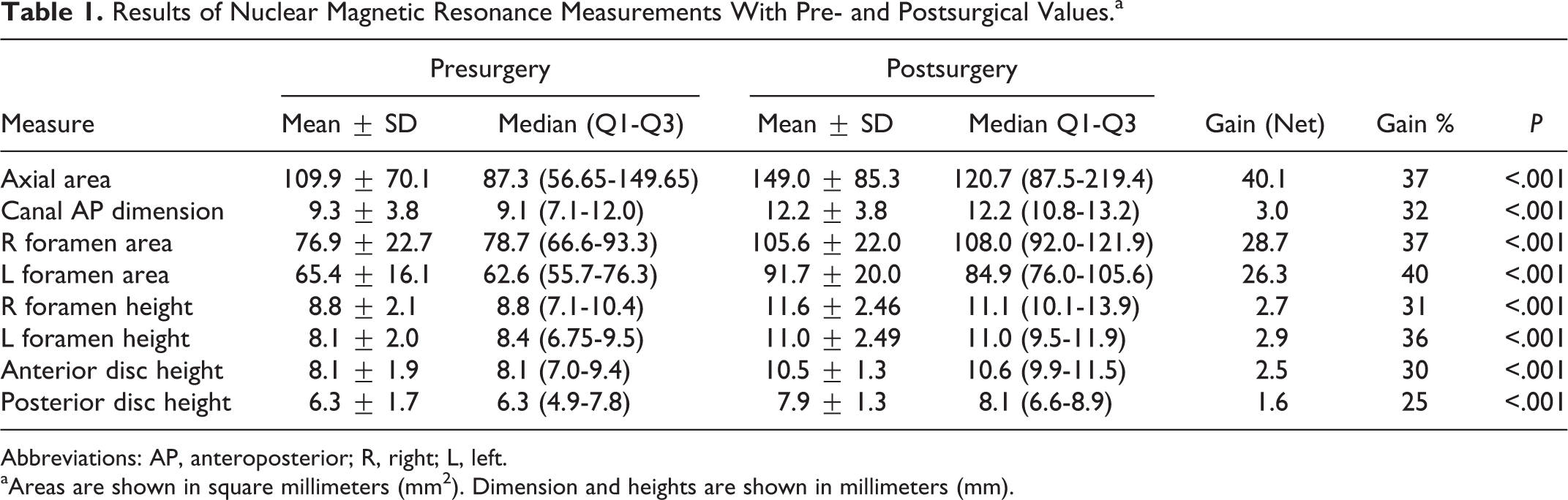
Abbreviations: AP, anteroposterior; R, right; L, left.
aAreas are shown in square millimeters (mm2). Dimension and heights are shown in millimeters (mm).
Complications
Surgical procedures occurred without complications. One case (5%) experienced a non-serious cutaneous reaction to the neuromonitoring electrodes, the surgery was then staged for further posterior supplementation. There was no case of restenosis. At the postoperative consultation (between 7 and 10 days after surgery) no patient presented psoas weakness. By the end of the study, no patient required revision surgery.
Radiological Results
The radiological results are shown in Table 1. Following discectomy and cage insertion, it was possible to testify that the increase in disc height, using both anterior and posterior values. The anterior disc height had a 2.5-mm increase (30%) and the posterior disc height gained 1.6 mm (25% increase). As a consequence of disc height restoration, the results showed a 37% increase in the mean spinal canal area, a 32% increase in the anteroposterior width of the vertebral canal, a 37% increase in the right foramen area, a 40% increase in the left foramen area, a 31% increase in the right foramen height, and a 36% increase in the left foramen height. Up to 12 months follow-up, there was no case that evolved with cage/pedicle screw loosening or cage subsidence.
The radiological results of a case are shown in Figures 1 to 6.
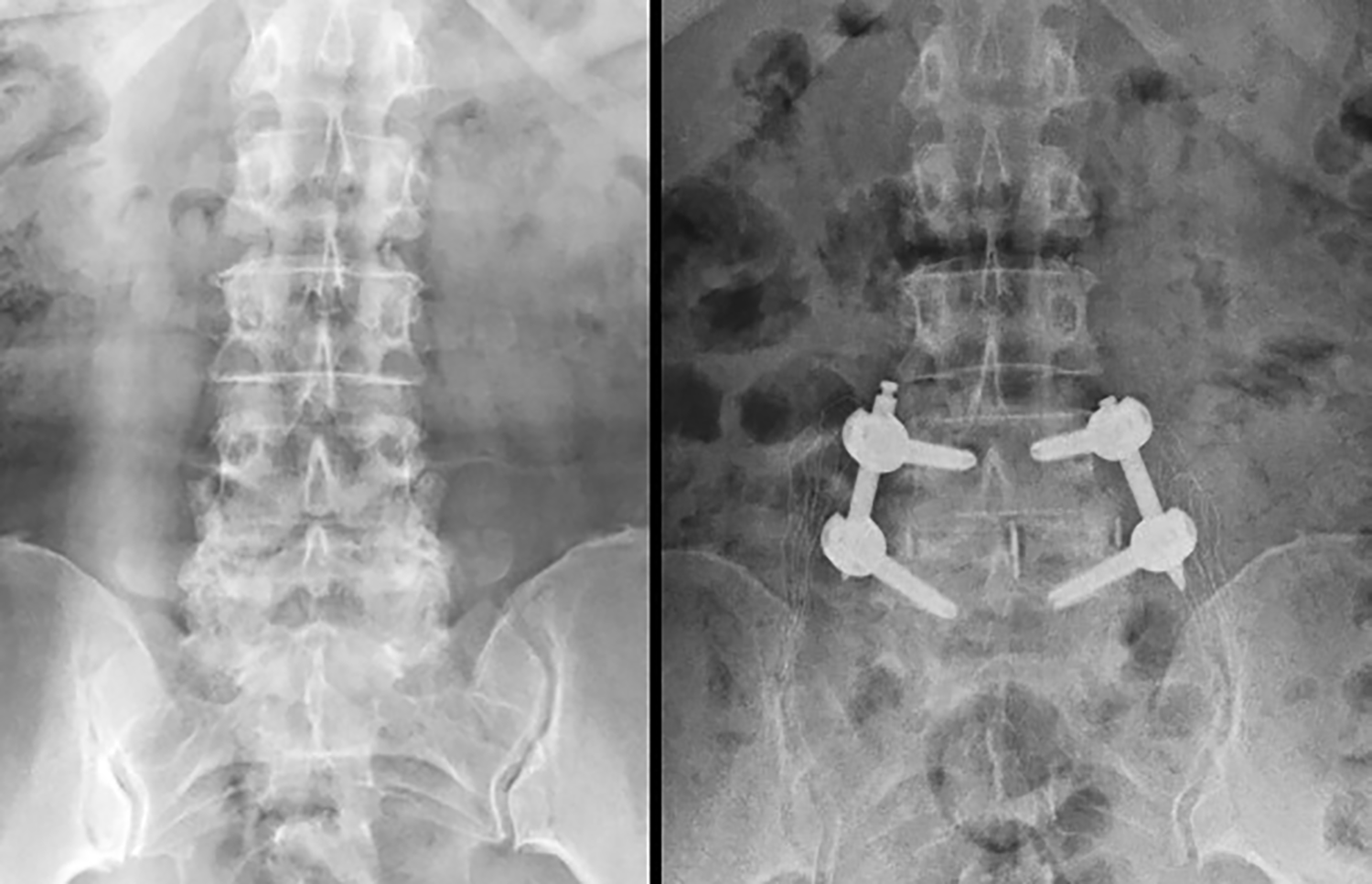
Case example. Preoperative (left) and postoperative (right) anteroposterior radiographs.

Case example. Radiography profiles in preoperative (left) and postoperative (right).
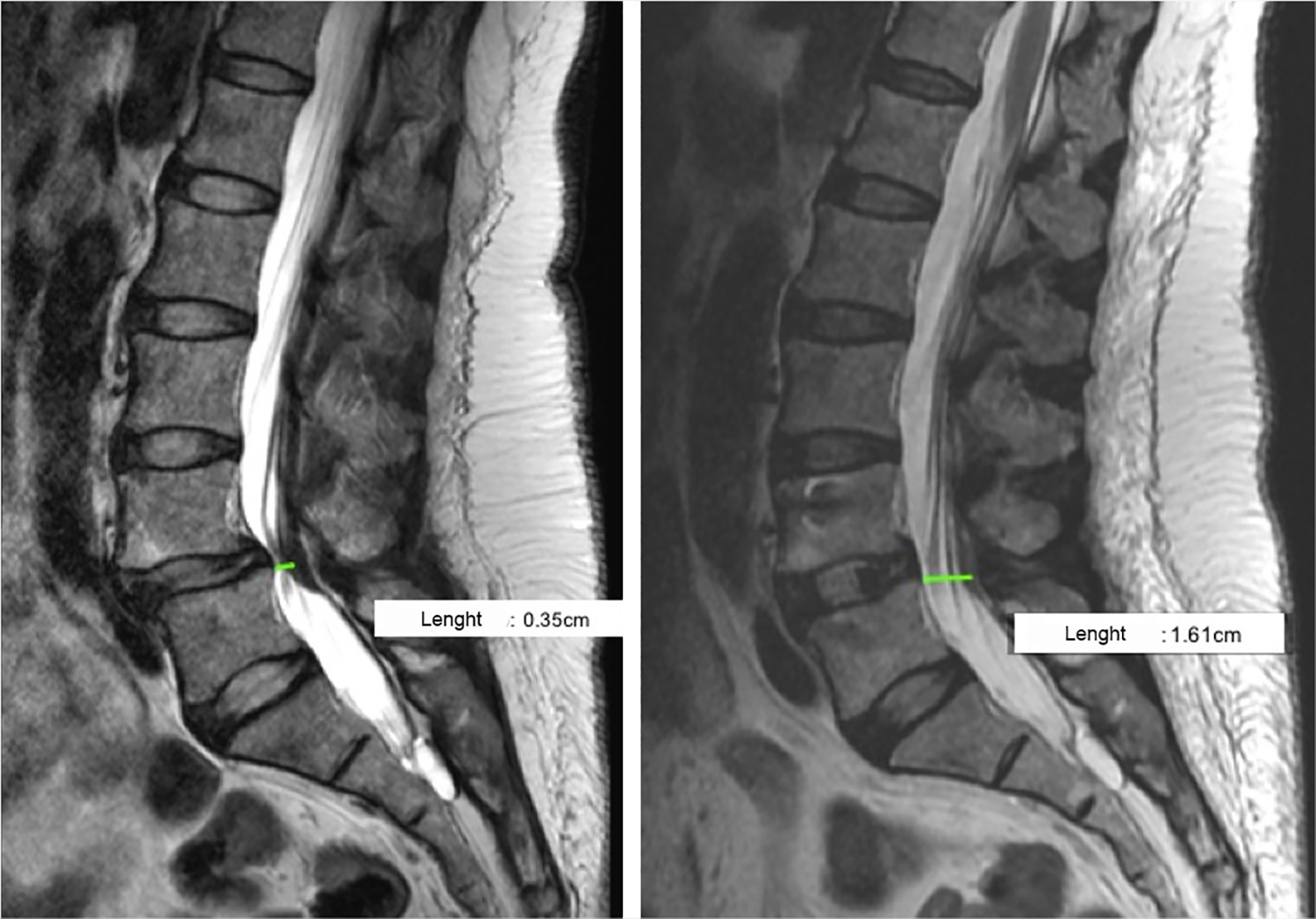
Length (anteroposterior) of the spinal canal. Left (pre): 6.06 mm. Right (post): 12.2 mm.
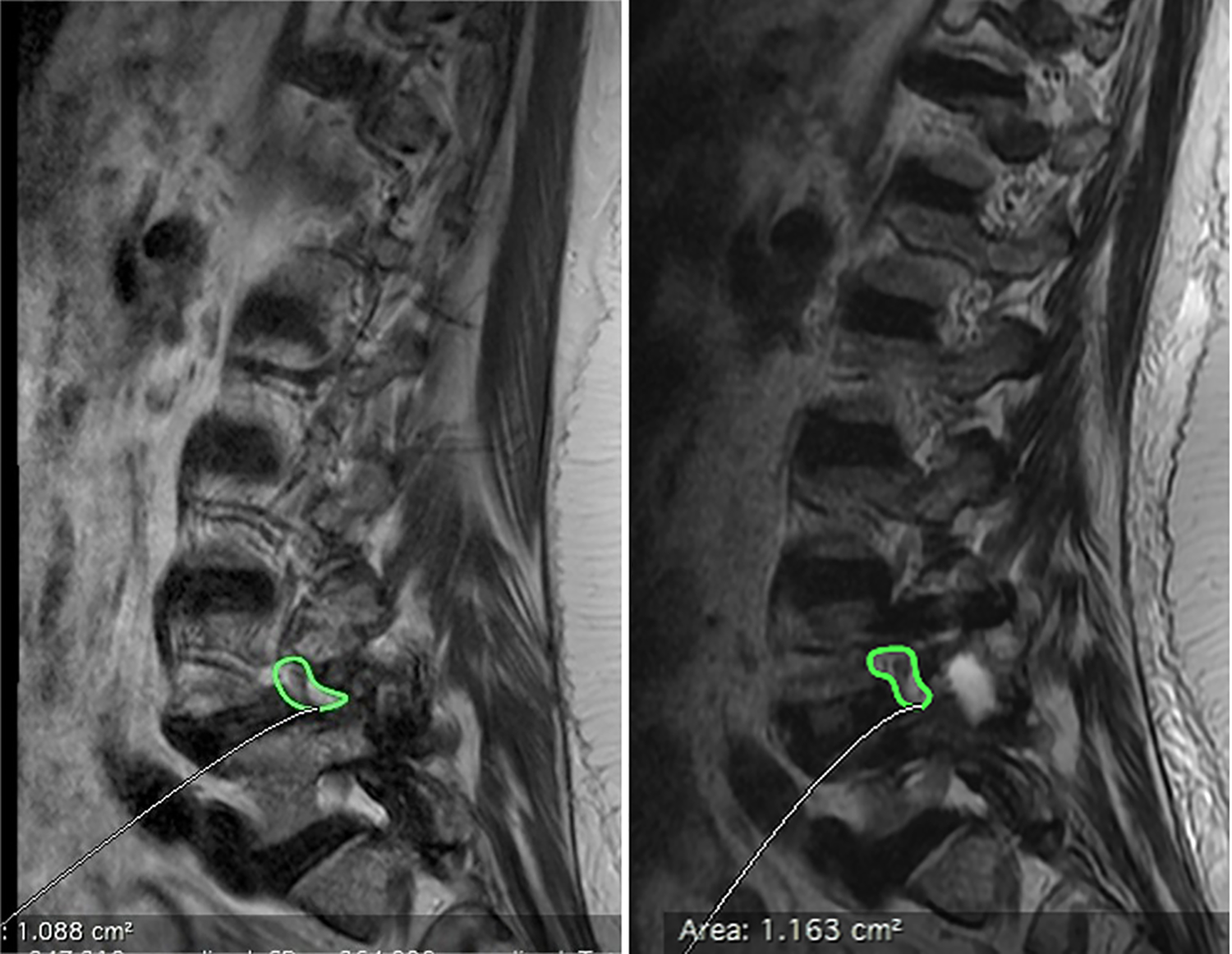
Foramen area: Left (presurgery): 1.088 cm2. Right (postsurgery): 1.163 cm2.

Height of the foramen. Left (presurgery): 7.3 mm. Right (postsurgery): 15.1 mm.
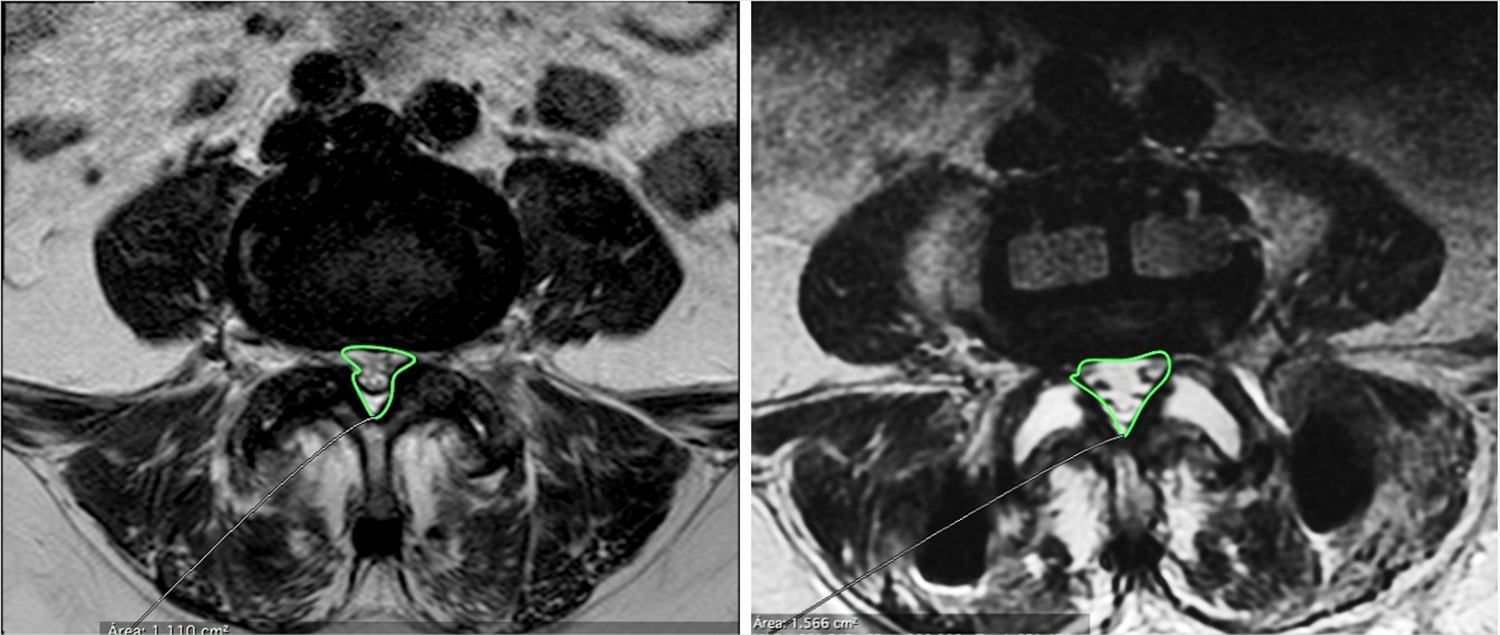
Canal area. Left (presurgery): 1.110 cm2. Right (postsurgery) 1.566 cm2.
Clinical Outcomes
The results of the clinical outcomes throughout the follow-up period are shown in Figure 7. At the first postsurgical follow-up, 6 weeks, it was already possible to detect improvement in the average pain levels, both for irradiated pain (7 to 3, P < .001) and for low back pain (8 to 3, P < .001). In the same manner, both 3- and 6-month assessment showed statistically significant improvements compared with the baseline. After 12 months, pain reduction was maintained in the lower limb (7 to 1, P < .001) and in the lumbar region (8 to 2, P < .001). At final follow-up, all patients (100%) had reached at least the MCID value for ODI. For VAS back and leg pain respectively, 95% and 90% patients have reported clinical results superior to MCID values.
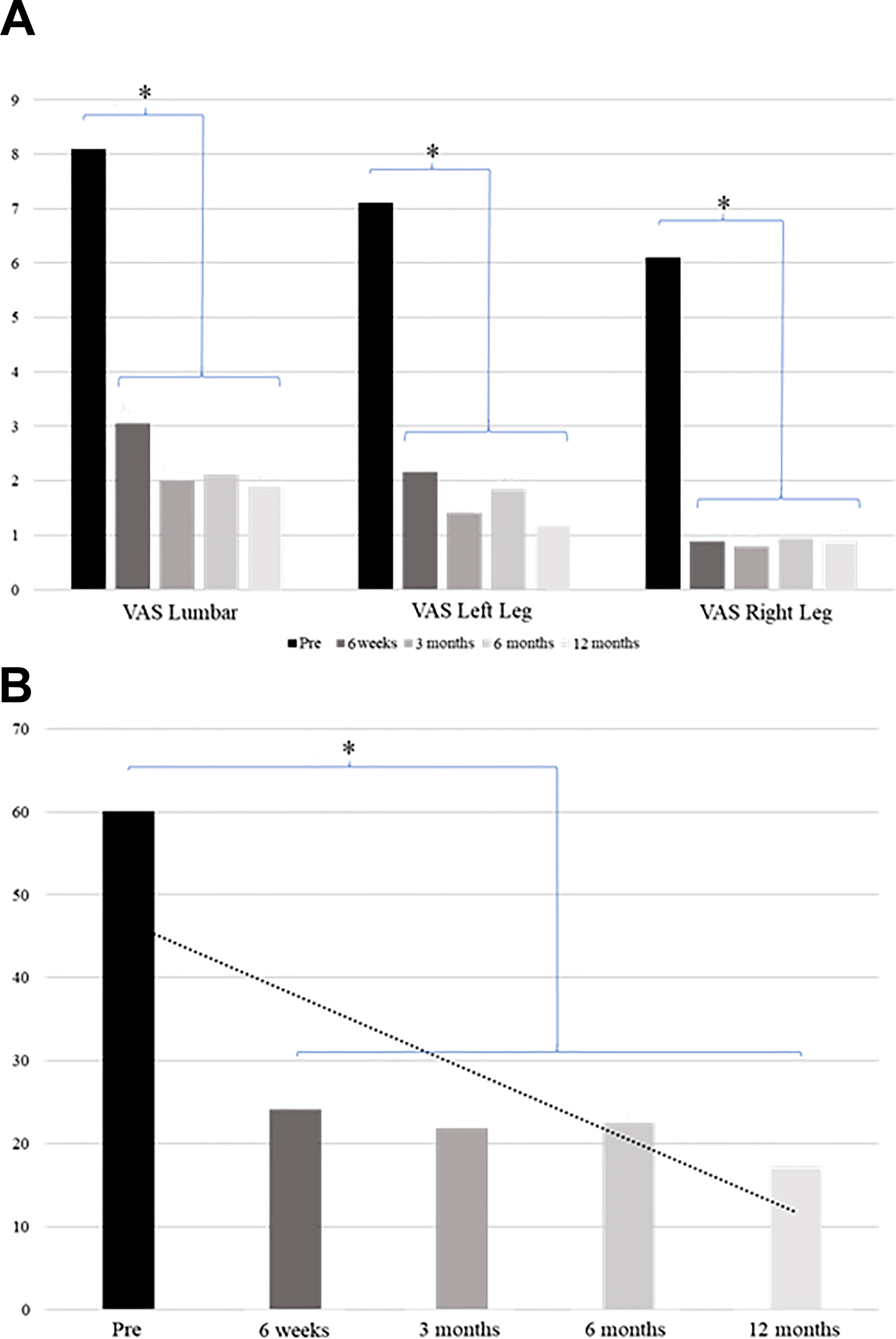
Clinical outcomes. (A) Mean values of the visual analogue scale (VAS) for pain evaluation between the preoperative period, 6 weeks after surgery and at 3, 6, and 12 months after surgery. All postoperative points were statistically lower (P < .01) than baseline (preoperative). (B) Mean values of the physical impairment assessed by the Oswestry Disability Index (ODI) between the preoperative periods, 6 weeks after surgery and at 3, 6, and 12 months postoperatively. *P < .001.
In addition to the decrease in pain, there was a decrease in the physical impairment of approximately 60% compared with baseline soon at the first postoperative evaluation. There was a significant improvement in all postoperative periods in the reduction of physical impairment compared with the preoperative evaluation (60 to 24 after 6 weeks, P < .001).
Discussion
The present study showed that it is possible to restore the foramen and vertebral canal dimensions with the minimally invasive LLIF transpsoas technique, without the need of posterior posterolateral fusion in cases of lumbar degenerative stenosis. This indirect decompression showed clinical results of pain relief and improvement in physical function, with low reoperation rate in the medium term.
It was possible to observe that discectomy and cage insertion by a minimally invasive LLIF technique allowed the gain of canal size and foramen at levels similar to those already observed in other studies with indirect lateral decompression. 20 -23 This indirect decompression showed clinical results of pain relief and physical impairment with low reoperation rate. Similar to other works with this surgical approach, the restoration of disc and foraminal height observed in the resonance images allowed the treatment of stenosis symptoms, with a significant improvement above 60% in the perception of low back pain and between 70% and 85% improvement in the in the lower and upper limbs, respectively. 20,21 It is very important to remind that the criteria for case selection, once the indirect decompression only restores “physiological” corridors instead of creating new ones as it can be achieved with direct decompression.
The results of the patient-reported outcomes confirmed the clinical effect of radiological decompression indirectly demonstrated. In this study, significant improvement was observed in radiological signs, physical evaluation, and pain assessments in the short, medium, and long terms, with maintenance of results over the study period. 20 -23 Rodgers et al 24 showed that 90% of the patients were satisfied or very satisfied with the results obtained after lateral access surgery. Ozgur et al 13 showed a reduction of the ODI score to 39% of the preoperative cohort of 62 patients.
Comparing studies that evaluated lateral and posterior surgery, authors show lower disk height loss after 24 months of surgery (P = .002), significantly increased areas and heights of the ipsilateral and contralateral foramen (P < .05) and a better result in physical disability (ODI) and pain (VAS), with a decrease in back pain of 59% (95% CI 6.9-2.8), a decrease in pain in the lower limbs of 56% (95% CI 7.1-3.1), increased quality of life assessed by the Short Form–36 questionnaire of 40% (95% CI 30.9-43.2; P < .001). 15,25 -28
Other authors in similar studies also found favorable radiological results with the decompression of the lateral access, with increase of the intervertebral disc height, increase of the central canal diameter and increase of the height and lateral foramen area. 20 This data is compatible with those found in this study and demonstrate the potential of this surgery in significant improvement of postoperative symptoms, with benefits in reducing pain and increasing the physical capacity of patients evaluated in different parameters and scales. 12,24,26
In this study, the group studied had acquired stenosis with or without limited olisthesis without severe rotation of the vertebrae (mean Cobb angle 7°). However, other authors 24,29,30 have observed that the indirect decompression by the lateral interbody fusion can occur in cases with mild degenerative lumbar scoliosis.
This study has some limitations that should be pointed out: The study design itself carries the limitation of the lack of comparison, limited number of cases enrolled, and short follow-up. Radiological assessment was not blind regarding if the image was pre- or postoperative. In addition, due to limited statistical power, it was not possible to establish a correlation between radiological parameters of indirect decompression and patient reported outcomes. Larger studies and longer follow-up should be performed to overcome these drawbacks.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.