
Abstract
Study Design
Retrospective analysis.
Objective
To investigate the relationship of T10-pelvic angle (T10PA) with conventional sagittal parameters and legacy alignment schemes.
Summary of Background Data
T10PA is a newly introduced sagittal parameter to predict the development of proximal junctional kyphosis (PJK). However, its relationship with conventional sagittal parameters and legacy alignment schemes remains unknown.
Methods
Patients with fusion from the pelvis to the upper-instrumented vertebra at or above the T10 were included. Based on the 6-week T10PA, the patients were divided into 3 groups as follows: undercorrection, functional alignment, and overcorrection. Conventional sagittal parameters and alignment status based on the Schwab’s pelvic incidence (PI)–lumbar lordosis (LL) modifiers and age-adjusted PI–LL were compared according to the T10PA groups. The PJK rates were compared among the alignment schemes.
Results
Overall, 219 patients were enrolled in this study. At 6 weeks postoperatively, 33.3%, 37.0%, and 29.7% of the patients demonstrated undercorrection, functional alignment, and overcorrection relative to the T10PA, respectively. Conventional sagittal parameters significantly differed according to the T10PA groups. Linear regression analysis revealed that T10PA was significantly affected by PI (β = .562) and LL (β = − .411). The correction statuses of the Schwab’s PI–LL modifiers and age-adjusted PI–LL were significantly differentiated between the T10PA correction groups. However, only 32.9% of patients with functional alignment relative to T10PA belonged to matched correction category for the age-adjusted PI–LL. Overcorrection relative to age-adjusted PI–LL and T10PA significantly increased PJK risks.
Conclusion
T10PA significantly correlated with conventional sagittal parameters, particularly PI and LL. Although the T10PA correction status correlated with that of the legacy alignment schemes, a notable discrepancy in the optimal correction was observed between the T10PA and age-adjusted PI–LL schemes. Overcorrection relative to T10PA and age-adjusted PI–LL should be avoided to mitigate PJK development.
Introduction
Proximal junctional kyphosis (PJK), a common mechanical complication following adult spinal deformity (ASD) surgery. It is a broad radiographic term referring to the development of junctional kyphosis at the upper end of an instrumented construct, which may lead to poor clinical outcomes.1,2 Although PJK has a multifactorial etiology, its occurrence is significantly associated with postoperative sagittal alignment.3-7 To define the “optimal alignment,” several alignment targets have been proposed, including the Scoliosis Research Society (SRS)–Schwab classification and age-adjusted alignment, as a patient-specific approach.8,9 These established alignment schemes have been validated in follow-up studies for their effectiveness in improving clinical outcomes and/or preventing PJK.10-13
Recently, the International Spine Study Group (ISSG) introduced a new sagittal parameter, the T10-pelvic angle (T10PA). 14 T10PA is a modification of the T1-pelvic angle (TPA), utilizing a component angle of TPA within the fusion. Since its introduction in 2014, TPA has been recognized as a useful perioperative planning parameter because it remains unaffected by patient posture. 15 However, TPA inevitably includes a component of the unfused thoracic spine unless the fusion extends to T1. Consequently, intraoperatively measured TPA may not always be reproducible postoperatively due to changes in the alignment of the unfused thoracic spine from a prone intraoperative position to a standing postoperative position. Additionally, intraoperative measurement of TPA requires a specialized long cassette that extends from the hips to T1. In contrast, T10PA is measured entirely within the fusion (if the fusion extends to at least T10) and can be measured intraoperatively using a conventional cassette. The first study introducing T10PA reported that achieving optimal correction relative to the T10PA target improved clinical outcomes by reducing PJK rates. Given that T10PA differs from conventional spinopelvic parameters and that established alignment schemes have already demonstrated their clinical efficacy in predicting PJK, it is important to assess the relationship between T10PA and traditional sagittal parameters to better understand its characteristics.
Therefore, this study aims to investigate the relationship between T10PA and conventional sagittal parameters and legacy alignment schemes in ASD surgery. Additionally, we examine PJK rates based on correction status according to each alignment scheme.
Materials and Methods
This study was approved by the institutional review board, and the requirement for informed consent was waived due to its retrospective nature.
Study Cohort
This retrospective study analyzed prospectively collected data from a single institution’s ASD database. The study cohort included consecutive patients who underwent corrective surgery between 2014 and 2022 for degenerative-type ASD using either a lateral approach or three-column osteotomy. ASD was defined by at least one of the following criteria: C7-sagittal vertical axis (C7–SVA) ≥5 cm, pelvic incidence (PI)–lumbar lordosis (LL) ≥10°, pelvic tilt (PT) ≥20°, or coronal Cobb angle ≥30°. Since this study primarily focused on T10PA, we included only patients who underwent fusion from the pelvis to an upper instrumented vertebra (UIV) at T10 or above. Pelvic fixation was performed using conventional iliac screws in all cases. The minimum follow-up period was 2 years postoperatively. Patients were excluded if they lacked appropriate radiographic data or had syndromic, neuromuscular, inflammatory, or other pathological conditions unrelated to degenerative ASD.
Data Collection and Radiographic Analysis
Baseline patient characteristics and surgical variables were recorded, including age, sex, American Society of Anesthesiologists (ASA) grade, T-score, body mass index (BMI), history of prior fusion surgery, lateral lumbar interbody fusion (LLIF), pedicle subtraction osteotomy (PSO), and the total number of fused levels.
Radiographic parameters were obtained from standing full-length lateral spine radiographs. Measurements were taken preoperatively and 6 weeks postoperatively and included PI, LL, PI–LL, sacral slope (SS), PT, thoracic kyphosis (TK), TPA, and C7–SVA. The risk of PJK development was assessed based on the correction status in 6-week postoperative radiographs. For patients who developed PJK within 6 weeks postoperatively, pre-discharge radiographs (taken prior to PJK development) were used for analysis.
Postoperative T10PA was measured as the angle between the line connecting the center of the T10 vertebral body to the hip center and the line connecting the hip center to the midpoint of the S1 upper endplate (Figure 1A). Previously reported data were used to define PI- and age-adjusted T10PA targets (Supplemental Table 1).
14
According to the original article, when the offset between the target and current T10PAs was within ±3.5°, the correction was considered functionally aligned relative to T10PA.
14
Based on these criteria, patients were divided into 3 groups: overcorrection (OC) (>3.5°), functional alignment correction (FC) (±3.5° from the target T10PA), and undercorrection (UC) (<−3.5°) (Figure 1B). Additionally, lordosis distribution index (LDI) was calculated on postoperative radiographs using the following equation: LDI (%) = (L4 − S1 lordosis)/(L1 − S1 lordosis) × 100. (A) Measurement of the T10 pelvic angle (T10PA). (B) Description of functional alignment, undercorrection, and overcorrection of T10PA.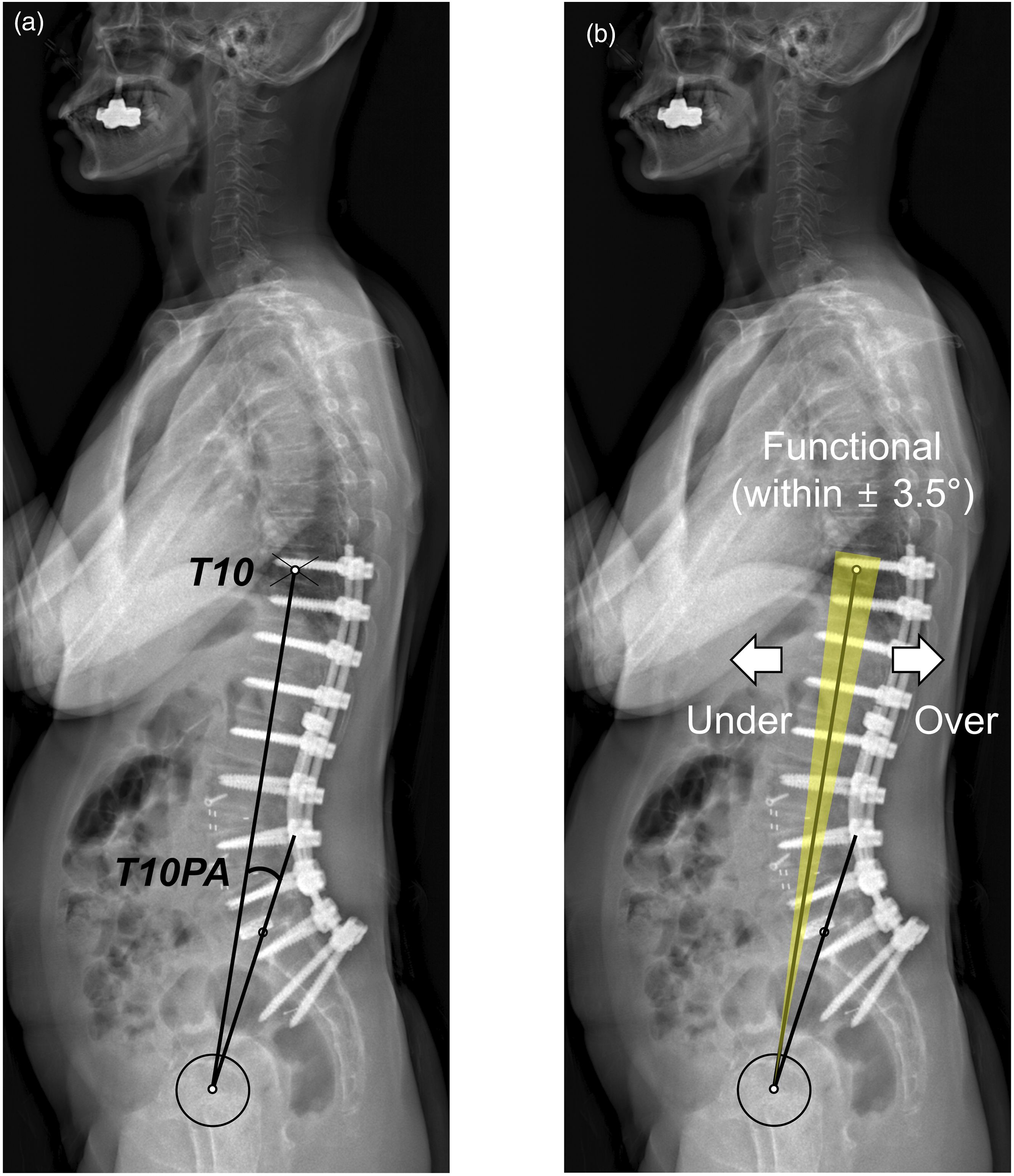
For legacy alignment schemes, we evaluated the PI–LL modifier of the SRS-Schwab classification and age-adjusted PI–LL based on 6-week postoperative radiographs. To compare T10PA, which remains unaffected by posture, only the PI–LL components of the Schwab criteria and age-adjusted alignment were included, excluding the positional components of PT, TPA, and SVA. The SRS-Schwab PI–LL modifiers were classified as 0 (PI–LL <10°), + (PI–LL within 10 – 20°), and ++ (PI–LL >20°). The age-adjusted PI–LL target was calculated using a previously reported equation: PI − LL = (age − 55)/2 + 3. 13 Matched correction relative to the age-adjusted alignment target indicated current values within a ±10-year range from the calculated ideal target. UC and OC indicated values greater than a +10-year limit and values less than a −10-year limit, respectively. PJK was defined as a proximal junctional angle (PJA) ≥20°. 16
Statistical Analysis
Descriptive statistics were used to present baseline demographic data and surgical variables. A paired t test was conducted to compare preoperative and 6-week postoperative sagittal parameters. One-way analysis of variance (ANOVA) was used to compare T10PA offsets and conventional sagittal parameters among the T10PA alignment groups. Pearson’s correlation test was used to assess the relationships between T10PA and conventional sagittal parameters, including PI, LL, LDI, PI–LL, and PT. Linear regression analysis was performed to examine the relationship between T10PA and intraoperatively measurable sagittal parameters (PI, LL, PI–LL, and LDI). Due to multicollinearity, PI–LL was excluded from the final model. Chi-square tests were conducted to analyze various aspects of the study. First, we examined the relationship between the correction status of the T10PA group and those of the SRS-Schwab PI–LL modifier and age-adjusted PI–LL. Next, we assessed the differences in PJK rates based on correction status across the 3 alignment schemes: the SRS-Schwab PI–LL modifier, age-adjusted PI–LL, and T10PA groups. Finally, we compared PJK rates according to the presence or absence of OC components in both the age-adjusted PI–LL and T10PA groups. All statistical analyses were conducted using SPSS (version 29.0.2.0; IBM Corp., Armonk, NY, USA). Statistical significance was set at P < .05.
Results
Study Population
Baseline Demographic, Surgical, and Perioperative Radiographic Data.
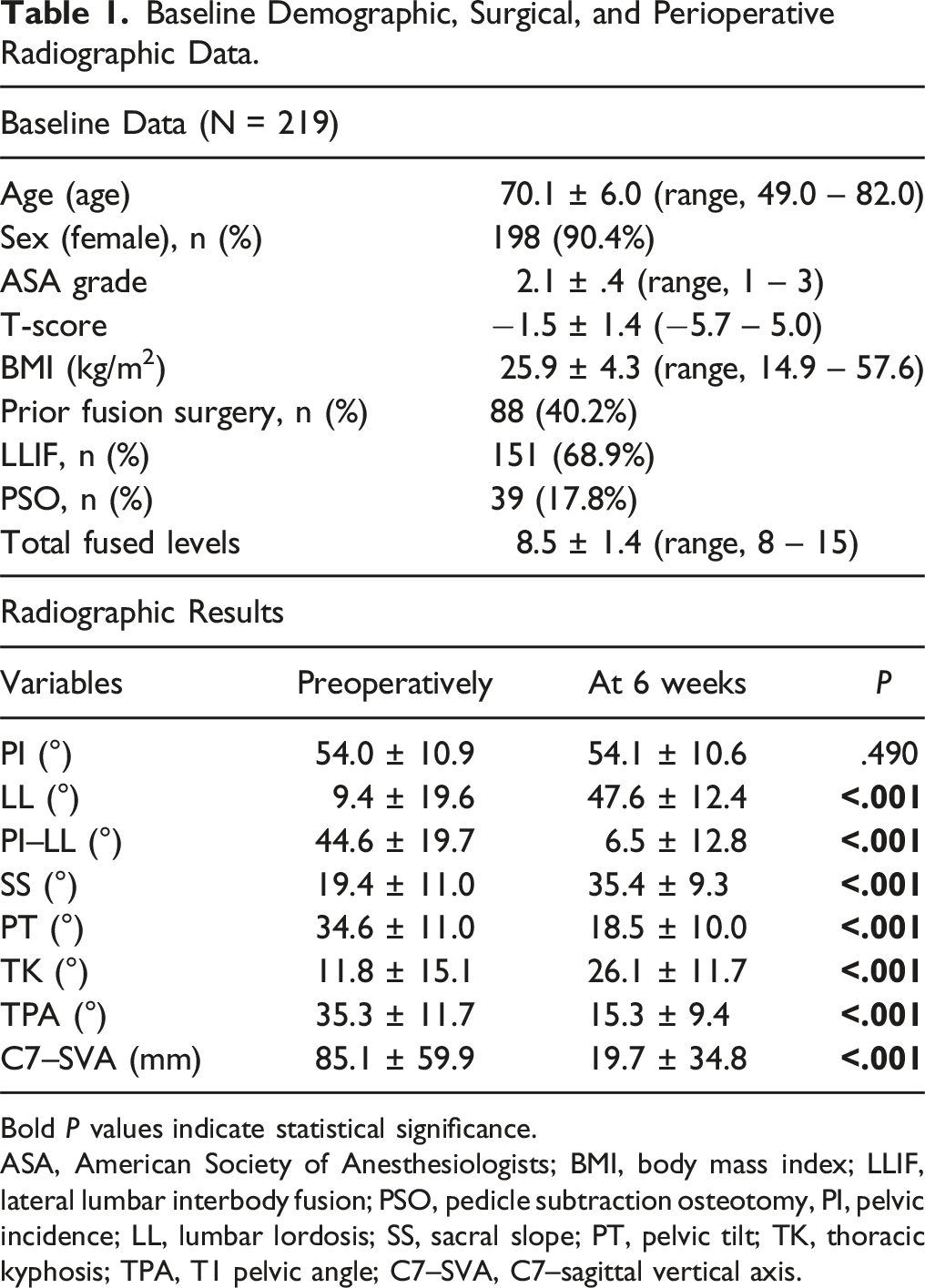
Bold P values indicate statistical significance.
ASA, American Society of Anesthesiologists; BMI, body mass index; LLIF, lateral lumbar interbody fusion; PSO, pedicle subtraction osteotomy, PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; TPA, T1 pelvic angle; C7–SVA, C7–sagittal vertical axis.
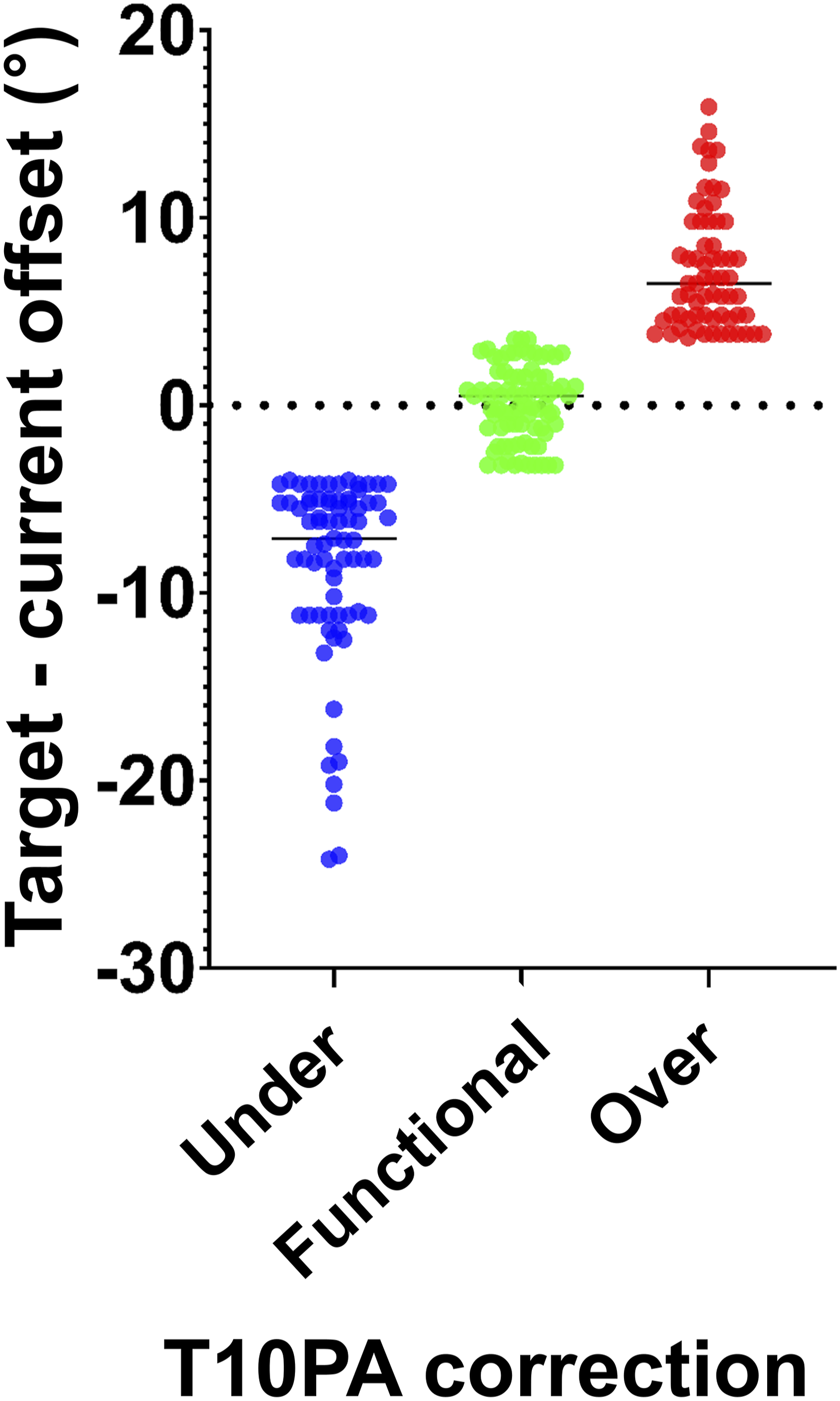
Comparison of T10-pelvic angle (T10PA) offsets between target and current T10PA values among T10PA correction groups.
Relationship Between T10PA and Conventional Sagittal Parameters
Comparison of Conventional Sagittal Parameters According to T10PA Correction Groups at 6 Weeks Postoperatively.
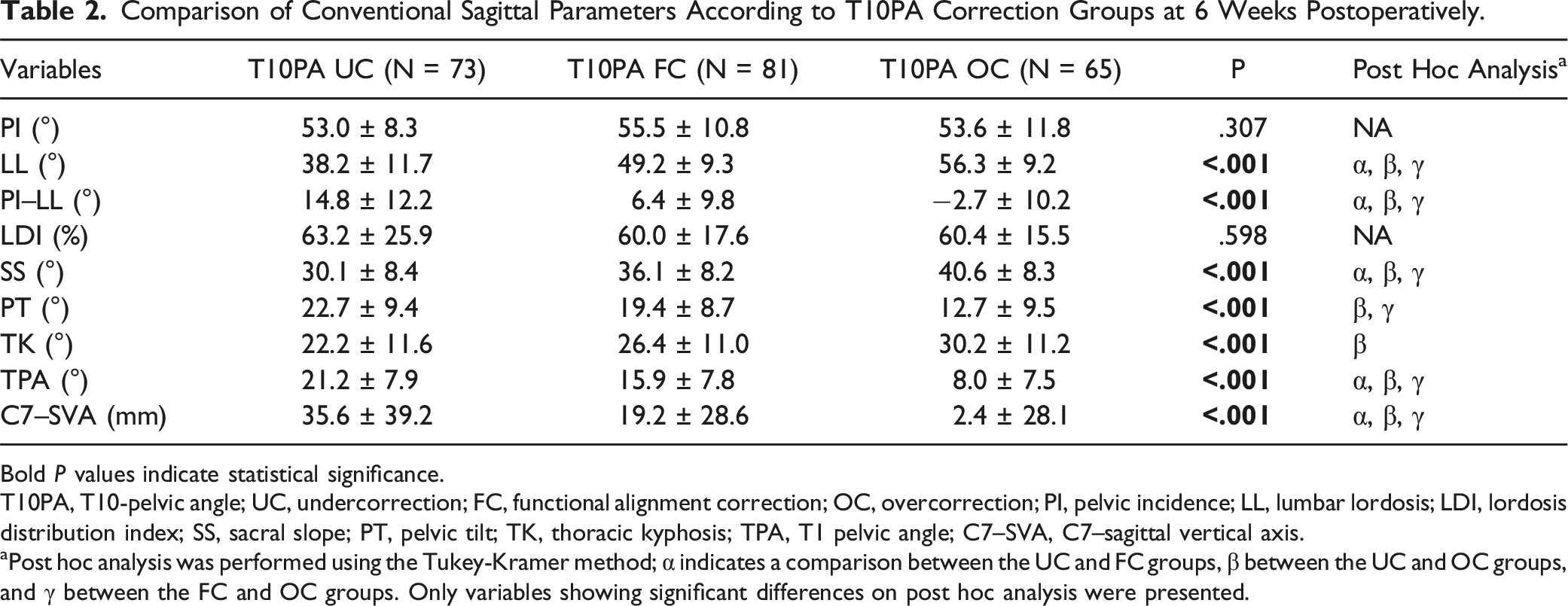
Bold P values indicate statistical significance.
T10PA, T10-pelvic angle; UC, undercorrection; FC, functional alignment correction; OC, overcorrection; PI, pelvic incidence; LL, lumbar lordosis; LDI, lordosis distribution index; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; TPA, T1 pelvic angle; C7–SVA, C7–sagittal vertical axis.
aPost hoc analysis was performed using the Tukey-Kramer method; α indicates a comparison between the UC and FC groups, β between the UC and OC groups, and γ between the FC and OC groups. Only variables showing significant differences on post hoc analysis were presented.
Pearson’s correlation analysis showed that T10PA had a strong correlation with PI–LL (r = .764) and PT (r = .719), a moderate correlation with PI (r = .504), a weak correlation with LL (r = −.352), and a very weak correlation with LDI (r = −.056) (Figure 3). Linear regression analysis was conducted to identify the factors influencing T10PA using intraoperatively measurable parameters, including PI, LL, PI–LL, and LDI. Due to multicollinearity, PI–LL was excluded from the final model. The resulting predictive equation was: T10PA = −.728 + .562 × PI − .411 × LL (R2 = .618). Scatter plots showing the correlation T10PA and (A) PI (r = .504), (B) LL (r = −.352), (C) LDI (r = −.056), (D) PI–LL (r = .764), and (E) PT (r = .719). T10PA, T10-pelvic angle; PI, pelvic incidence; LL, lumbar lordosis; LDI, lordosis distribution index; PI–LL, pelvic incidence–lumbar lordosis; PT, pelvic tilt.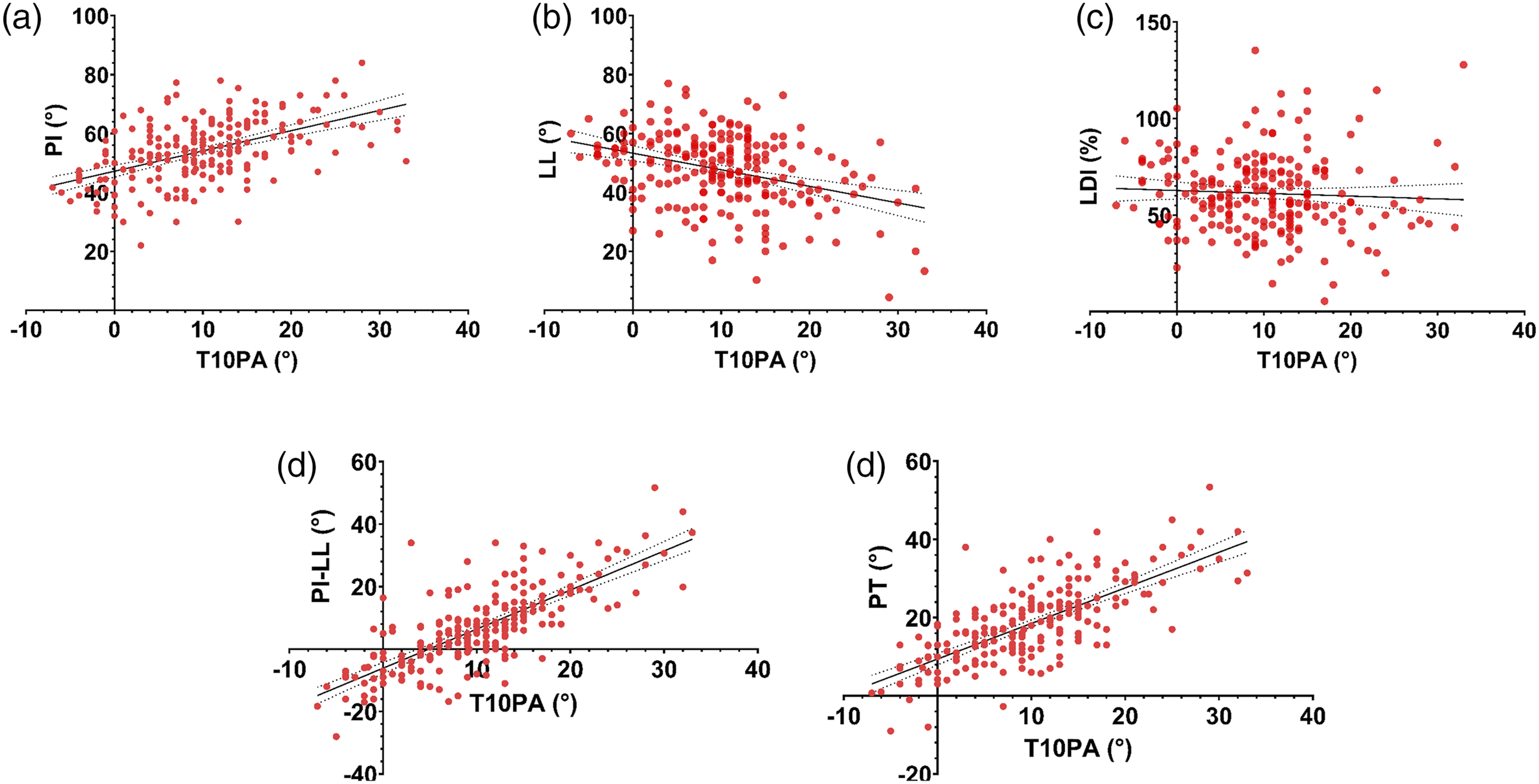
Relationship of T10PA Correction Status With Legacy Alignment Schemes
Comparison of Postoperative Correction Status Relative to the Legacy Alignment Schemes According to T10PA Correction Groups.
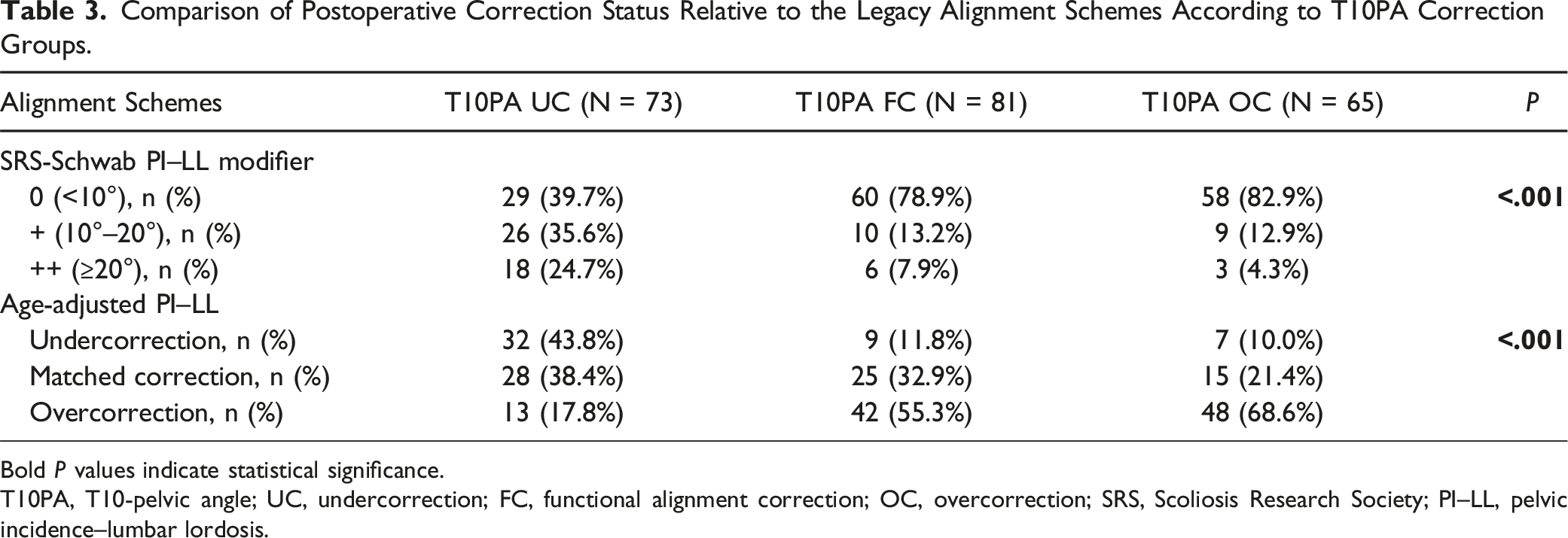
Bold P values indicate statistical significance.
T10PA, T10-pelvic angle; UC, undercorrection; FC, functional alignment correction; OC, overcorrection; SRS, Scoliosis Research Society; PI–LL, pelvic incidence–lumbar lordosis.
PJK Rates According to Alignment Schemes
Comparison of PJK Rates According to Correction Status of Three Alignment Schemes.
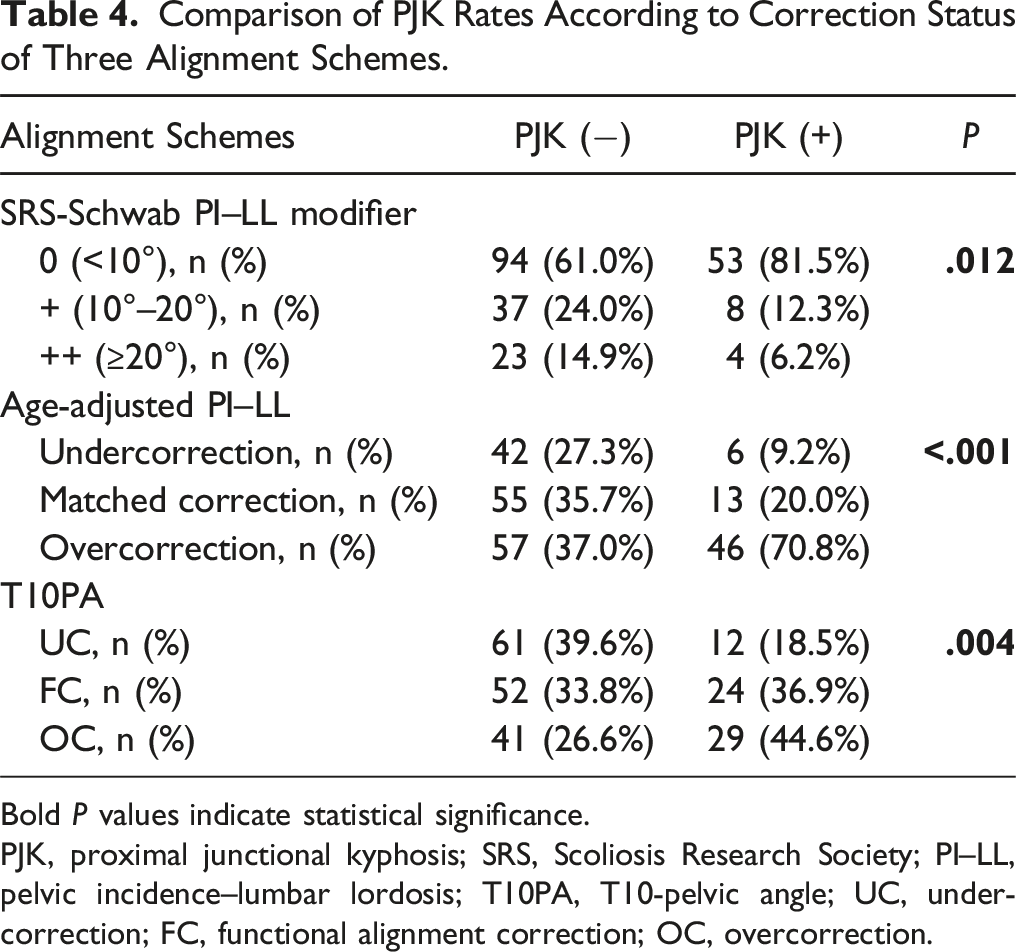
Bold P values indicate statistical significance.
PJK, proximal junctional kyphosis; SRS, Scoliosis Research Society; PI–LL, pelvic incidence–lumbar lordosis; T10PA, T10-pelvic angle; UC, undercorrection; FC, functional alignment correction; OC, overcorrection.
Stratified PJK Risks According to the Presence of Overcorrection Components in Age-Adjusted PI–LL and T10PA Groups.
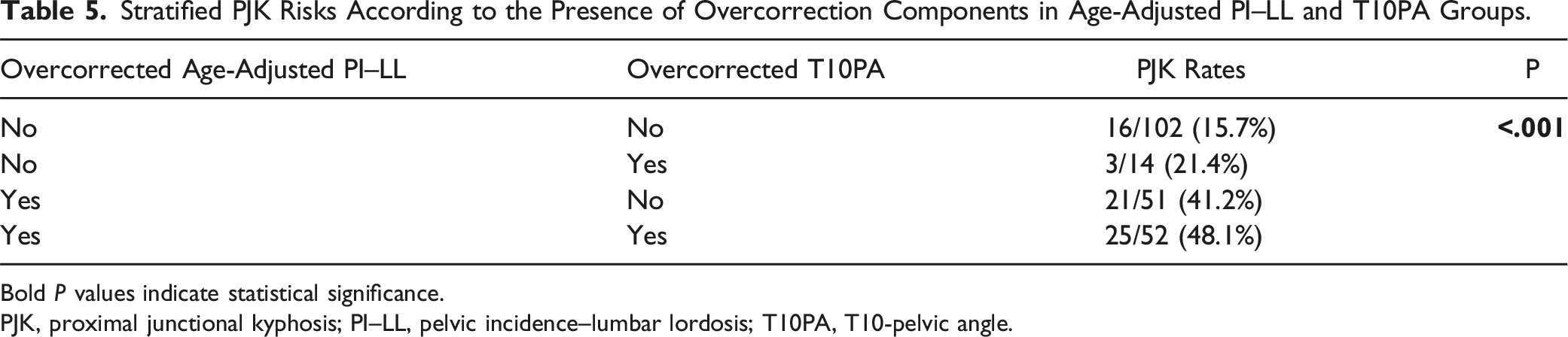
Bold P values indicate statistical significance.
PJK, proximal junctional kyphosis; PI–LL, pelvic incidence–lumbar lordosis; T10PA, T10-pelvic angle.
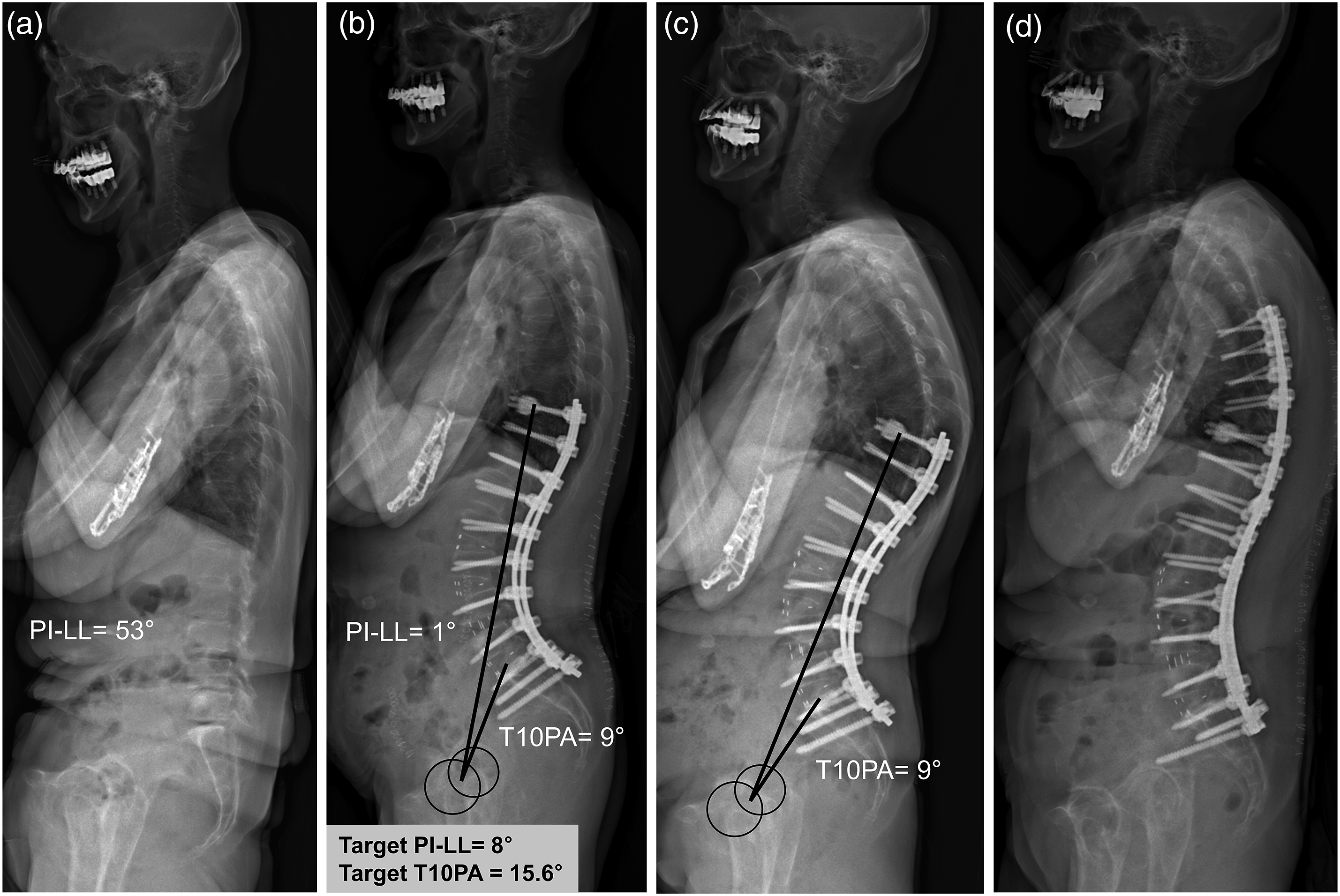
Case example of a 75-year-old woman. (A) Preoperative radiograph showing severe flatback deformity with PI–LL of 53°. (B) After T10-to-pelvic fusion, sagittal malalignment was corrected with PI–LL and T10PA of 1° and 9°, respectively. Based on the calculated alignment targets, both PI–LL and T10PA were overcorrected. (C) PJK developed at 6 weeks postoperatively. Note that T10PA did not change despite the development of PJK. (D) Revision surgery was performed because of aggravating axial pain. PI–LL, pelvic incidence–lumbar lordosis; PJK, proximal junctional kyphosis; T10PA, T10-pelvic angle.
Discussion
The primary goal of sagittal realignment surgery is to restore sagittal balance, maximize the cone of economy, and ultimately improve pain and disability. 17 With the increasing emphasis on patient-specific surgical planning, correction strategies are shifting toward a more individualized approach that considers both PI and age. The SRS-Schwab PI–LL modifier (only PI-based) and age-adjusted PI–LL (age- and PI-based) are widely used alignment schemes that guide optimal LL correction. While the SRS-Schwab criteria were initially developed to improve clinical outcomes, age-adjusted alignment was introduced to minimize the risk of PJK.10,18
T10PA was introduced by the ISSG as a novel parameter incorporating patient-reported outcome scores, pelvic incidence, and age. 14 This parameter demonstrated significant correlations with the physical component score (r = −.284), PI (r = .533), and age (r = .308). Using decision tree analysis, ISSG established T10PA thresholds to define optimal functional alignment, with a range extending 3.5° above and below the target value. Since T10PA represents the component angle of TPA within the fused segment, it enables the assessment of spinopelvic alignment independently of the unfused thoracic spine (Figure 4B). Additionally, unlike TPA, T10PA is an anatomical angle that remains unaffected by PJK occurrence (Figure 4C). Because this angle remains consistent between prone and standing radiographs, it offers the advantage of being reliably measured intraoperatively. Given these advantages in ASD surgery, establishing a method to achieve optimal T10PA during surgery requires further investigation into its relationship with conventional sagittal parameters and alignment schemes.
In this study, we found a significant association between crude T10PA (unadjusted for age and pelvic incidence) and conventional sagittal parameters, including PI, LL, PI–LL, and PT (Figure 3). However, LDI showed the weakest correlation with T10PA. Linear regression analysis indicated that T10PA was significantly influenced by PI (β = .562) and LL (β = −.411), suggesting that optimal T10PA can be effectively achieved intraoperatively. Although T10PA is linearly correlated with PI–LL, it has distinct characteristics compared to the traditional PI–LL concept. First, it incorporates multiple anatomical components, including pelvic shape (strongly correlated with PI), pelvic position (strongly correlated with PT), and lumbar lordosis (strongly correlated with LL), making the T10 position a complex interplay of these factors. Second, unlike PI–LL, which only accounts for alignment below L1, T10PA also reflects alignment above L1. Given the importance of maintaining adequate rod contour in the proximal part of the construct (ie, above L1) for PJK prevention, 19 T10PA provides a more comprehensive assessment of sagittal spinal alignment. Even when T10PA correction was categorized based on pelvic incidence and age, similar trends to crude T10PA were observed: smaller T10PA values were associated with greater sagittal correction, except for PI and LDI (Table 2). The lack of variation in PI among the T10PA groups is likely due to PI already being factored into the T10PA correction classification.
Regarding categorized alignment schemes, the SRS-Schwab PI–LL modifiers and age-adjusted PI–LL categories showed significant differences among the T10PA correction groups (Table 3). However, there were discrepancies in correction status between these alignment schemes. Among patients with FC relative to T10PA, 78.9% had an SRS-Schwab PI–LL modifier of 0, whereas only 32.9% met the criteria for matched correction based on age-adjusted PI–LL. This discrepancy suggests that the criteria used to define optimal correction may vary depending on the alignment scheme applied, as these classifications serve distinct roles. Regarding PJK risk, consistent with previous studies,6,7,14,18 we found that OC increased PJK rates across all 3 alignment schemes: the SRS-Schwab PI–LL modifier, age-adjusted PI–LL, and T10PA correction groups (Table 4). Although PI–LL <10° in the SRS-Schwab classification was associated with a higher risk of PJK in this study, the clinical significance of maintaining PI–LL >10° as a preventive measure remains uncertain, particularly given that undercorrection has been linked to poorer clinical outcomes in several studies.10,20 Furthermore, as shown in Table 4, the relationship between undercorrection and PJK risk varied depending on the alignment scheme applied, suggesting that a single universal threshold for undercorrection may not be appropriate. Therefore, a more nuanced approach that considers both age-adjusted PI–LL and T10PA may be preferable for achieving optimal sagittal alignment while minimizing the risk of PJK. Given their distinct characteristics, it remains unclear which of these alignment schemes is superior in predicting PJK occurrence. Instead, we propose that a combined approach using both schemes may enhance PJK risk prediction (Table 5). To minimize PJK development, avoiding OC in both age-adjusted PI–LL and T10PA appears to be the most effective strategy. Developing an integrated targeting system that incorporates multiple alignment schemes may provide a more comprehensive framework for PJK prevention and surgical planning.
This study has several limitations. First, as a retrospective analysis conducted at a single institution, the possibility of selection bias or missing data cannot be entirely ruled out. Second, the recently introduced sagittal age-adjusted score (SAAS) by the ISSG, which incorporates age-adjusted PI–LL, PT, and TPA, 21 was not included. SAAS contains non-fixed-angle components such as PT and TPA, and its effectiveness in improving clinical outcomes and preventing PJK has not yet been fully validated. Third, other classification schemes, including the Roussouly classification and the global alignment and proportion (GAP) score, were not included. The Roussouly classification provides insights into sagittal spinal morphology by categorizing different alignment patterns. While it helps characterize intrinsic lumbar shape, it does not directly quantify the magnitude of lordosis correction, which was an important consideration in our study. Similarly, the GAP score accounts for unfused spine motion and positional parameters, making it less applicable to our analysis. For these reasons, these classification methods were not incorporated into this study. However, further research is needed to compare them with T10PA and their impact on postoperative sagittal alignment, PNR, and PJK.
Conclusion
T10PA showed a significant correlation with conventional sagittal parameters, particularly PI and LL. While its correction status aligned with legacy alignment schemes, a notable discrepancy was observed between the optimal correction targets of T10PA and age-adjusted PI–LL. To minimize the risk of PJK, OC in both T10PA and age-adjusted PI–LL should be avoided.
Supplemental Material
Supplemental Material - Relationship of T10-Pelvic Angle With Conventional Sagittal Parameters and Legacy Alignment Schemes in Adult Spinal Deformity Surgery
Supplemental Material for Relationship of T10-Pelvic Angle With Conventional Sagittal Parameters and Legacy Alignment Schemes in Adult Spinal Deformity Surgery by Se-Jun Park, Hyun-Jun Kim, Jin-Sung Park, Dong-Ho Kang, Minwook Kang, Kyunghun Jung, and Chong-Suh Lee in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.