
Abstract
Study Design
Retrospective cohort study.
Objectives
To evaluate the frequency, risk factors, and impact of incidental durotomy on adverse events and outcomes after TLIF with expandable interbody spacers.
Methods
We reviewed 433 consecutive patients treated by TLIF using expandable titanium interbody implants (ALTERA®, Globus Medical Inc) on 538 levels between December 2018 and September 2023. Patients with incidental durotomy (ID) and cerebrospinal fluid leakage were compared to patients without ID, focusing on patient-specific and surgery-related factors, adverse events, clinical outcomes (MacNab criteria), and radiological outcomes at discharge, 3, and 12 months.
Results
The ID rate was 9.0% (39/433 patients). Patients with ID had lower BMI (26.1 ± 5.2 vs 28.0 ± 5.3 kg/m2, P = .03), longer surgery duration (358 ± 132 vs 305 ± 128 minutes, P = .01), and extended hospital stays (14.7 ± 12.8 vs 10.9 ± 8.2 days, P < .01). More postoperative adverse events (51.3% vs 28.7%, P = .004) with higher severity (28.2% vs 13.2% moderate to severe, P = .019) occurred at discharge. No differences were found in outcomes at 3 or 12 months. ID patients showed higher risks for impaired wound healing (adjusted OR, 4.39; 95% CI, 1.90-10.2; P = .001) and pulmonary embolism (adjusted OR, 3.52; 95% CI, 1.13-10.9; P = .029).
Conclusions
Incidental durotomy was associated with longer surgery time, hospital stays, and increased early postoperative complications. While not affecting mid-to-long-term outcomes, ID increased risks for wound healing difficulties and pulmonary embolisms.
Introduction
Transforaminal lumbar interbody fusion (TLIF) is one of the most common surgical approaches, used for various spinal pathologies including degenerative conditions, deformity, trauma, tumor and infections. It allows for the restoration of both intervertebral and foraminal height, thereby directly or indirectly decompressing the exiting nerve root. 1 In recent years, TLIF procedures using expandable interbody spacers have become increasingly common. This trend is driven by growing awareness of the importance of sagittal alignment parameters and the rising popularity of minimally invasive approaches, which offer benefits such as reduced blood loss, less tissue trauma, and faster patient recovery. 1
Incidental durotomy (ID) with or without arachnoid injury and resulting leakage of cerebrospinal fluid (CSF) is one of the most frequently reported adverse events (AEs) in spine surgery, with an incidence ranging from 2% to more than 20%. 2 ID is concerning due to its potential impact on postoperative recovery and its significant economic burden, often resulting in increased length of surgical procedure and hospital stay. 3 If not managed adequately, ID may lead to wound healing disorders including infections, arachnoiditis, meningitis, pseudomeningocele formation, postural headaches, or new neurological deficits due to nerve entrapment in CSF cysts.2-4 Currently, there is no generally accepted, standardized treatment protocol for patients experiencing IDs.2,5,6
To date, no study has examined the rate of ID in large series employing expandable TLIF spacers. As collapsed expandable spacers may be introduced more gently into the disc space via a smaller access and with expansion in-situ, a lower rate of ID compared to TLIF with static interbody cages is theoretically conceivable. Moreover, the literature on risk factors and down-stream effects on patients experiencing ID after TLIF surgery is scarce. We hence set out to critically review our institutional series in this regard.
Methods
Study Setting and Population
This study was conducted at the Cantonal Hospital of St. Gallen, a major teaching hospital affiliated with the Medical School of the St. Gallen University, serving a population of approximately one million people. The Spine Center of Eastern Switzerland is comprised of twelve board-certified neuro- or orthopedic spine surgeons. In October 2018, we introduced the ALTERA® Expandable Integrated TLIF Spacer by Globus Medical Inc, PA, USA. TLIF procedures for this analysis were performed by all board-certified spine surgeons, as well as by residents and fellows under supervision.
Patient Identification and Selection
We identified patients in which an ALTERA® TLIF spacer was implanted by review of the purchasing records, as well as surgery schedules between October 2018 - September 2023. We included adult patients who underwent single- or multi-level lumbosacral TLIF surgery for degenerative, trauma, infection, tumor or deformity indication and who signed the institutional waiver for anonymized research. Patients undergoing TLIF surgery with either a static or another type of expandable interbody spacer were excluded, as the latter was found to frequently collapse during follow-up. 7
Data Collection
The electronic patient records were retrospectively reviewed in a standardized fashion. Baseline data collected included demographic variables like sex, age, body mass index (BMI; in kg/m2), smoking status (nonsmoker, smoker or former smoker), anesthesiologic risk (American Society of Anesthesiology (ASA) grading scale; grade 1-4), comorbidity (Charlson Comorbidity Index, CCI; stratified into very low (CCI 0), mild (CCI 1&2), moderate (CCI 3&4) and severe (CCI >4)), 8 and frailty (Canadian clinical frailty score; ranging from 1 (very fit) to 9 (terminally ill)). 9 In addition, the indication for surgery was determined (e.g. degenerative, trauma, infection, tumor or deformity).
Surgery-specific characteristics such as the level of the TLIF procedure (between T12/L1 and L5/S1), the number of fused segments (mono-/bisegmental or more segments), the type of spacer (8° vs 15° lordotic), the use of other additional fusion procedures during the same procedure (anterior lumbar interbody fusion (ALIF), (extreme) lateral lumbar interbody fusion (XLIF/LLIF), posterior lumbar interbody fusion (PLIF), or other), the use of cement-augmentation for pedicle screws, type of laminectomy (partial/complete), intraoperative release of the anterior longitudinal ligament (ALL), 10 the surgery duration (in minutes), and the estimated blood loss (EBL; in mL, estimated from suction drainage and bloody gauzes) were recorded as well.
Information on length of stay, occurrence and type of postoperative AEs was extracted from patient charts as well as follow-up clinical reports at 3 and at 12 months postoperative. AEs were classified according to their severity and impact using the Therapy-Disability-Neurology (TDN) scoring system. 11 Clinical outcomes were estimated from hospital reports and patient-reported outcome measures (PROMs), according to the Macnab criteria and graded as excellent, good, fair or poor. 12
Standing (lumbar, whole-spine or EOS, as available) x-ray and/or computed tomography (CT) scans obtained before hospital discharge as well as at 3 months and 12 months respectively were reviewed to assess for: the degree of posterolateral fusion (according to the classification by Lenke 13 ; definitely solid, possibly solid, probably not solid or definitely not solid), degree of intersomatic fusion (according to the Brantigan, Steffee & Fraser (BSF) classification 14 : pseudarthrosis, intermediate type and solid fusion), occurrence of cage subsidence (at discharge, at 3 months and at 12 months, respectively 15 ), and occurrence of cage collapse (at 12 months). Clinical pseudarthrosis was defined as new onset of axial or radicular pain weeks to months after fusion surgery after ruling out other causes of pain, 16 based on the clinical symptoms in combination with available imaging studies. In patients without unusual pain, reporting a favorable outcome and without signs of hardware failure on imaging, the diagnosis of pseudarthrosis was considered unlikely.
The following radiological parameters were obtained from reviewing standing lumbar, whole-spine or EOS x-ray studies, as available: segmental lordosis (SL), defined as the segmental sagittal Cobb angle (e.g., upper endplate of L2 vertebra to lower endplate of L3 vertebra for the L2-L3 segment), pelvic tilt (PT), pelvic incidence (PI), lumbar lordosis (LL), sacral slope (SS) and C7-sagittal vertebral axis (C7-SVA). Furthermore, the Roussouly type of spinal geometry as well as the patient-specific “ideal LL” were determined using a web-based application (https://www.spinebit.io/), which itself uses the formulas by Le Huec and the European Spine Study Group.17-19 From these measures, a PI-LL mismatch (PI minus LL) and an ideal-actual LL mismatch (ideal LL minus actual LL) were calculated.
Surgical Technique
The TLIF procedure involved pedicle screw placement first, followed by uni- or bilateral facetectomy. After meticulous discectomy the endplates were prepared, and trials were inserted. Severely collapsed segments were distracted with an intervertebral “Chiari” spreader. After choosing the appropriate spacer, it was filled with autologous and/or allogeneic bone graft, which was also inserted into the disc space. In its final position, spacers were expanded under serial fluoroscopic control. The posterior aspect of the disc space was then filled with bone graft and posterior compression was performed, as needed. The surgical approach was tailored to each patient’s specific pathology and symptoms. A typical case-example can be seen in Figure 1. Case Vignette of a 77-year-old osteoporotic female, suffering from bilateral L5 radicular symptoms due to a degenerative foraminal stenosis L5-S1 along with a segmental degeneration L4/L5 with disc bulging and recess stenosis. After exhausted conservative treatment, she was treated with posterior instrumented fusion from L4 to ilium with S2-ilioalar screws and TLIFs at L4/5 and L5/S1. The screws were cement-augmented as the bone quality was poor. In the preoperative a-p (A) and lateral (B) standing x-rays, the severe degeneration of the caudal lumbar segments (especially L4-S1) as well as the slight coronal deformity are shown (LL L1-S1 preoperatively: 49.3°). Her pelvic incidence was 56.6° (not shown in the figure). The patient suffered an intraoperative ID, which could be sutured, and a pulmonary embolism during the hospital stay. She had a favourable outcome with resolution of the radicular symptoms and no neurological deficits. In the postoperative a-p (C) and lateral (D) standing x-rays at the 1-year follow-up, the restoration of an adequate lordosis and of the sagittal and coronal profiles between L4-S1 is seen, despite cage subsidence at L4/5 (LL L1-S1 postoperatively: 61.2°).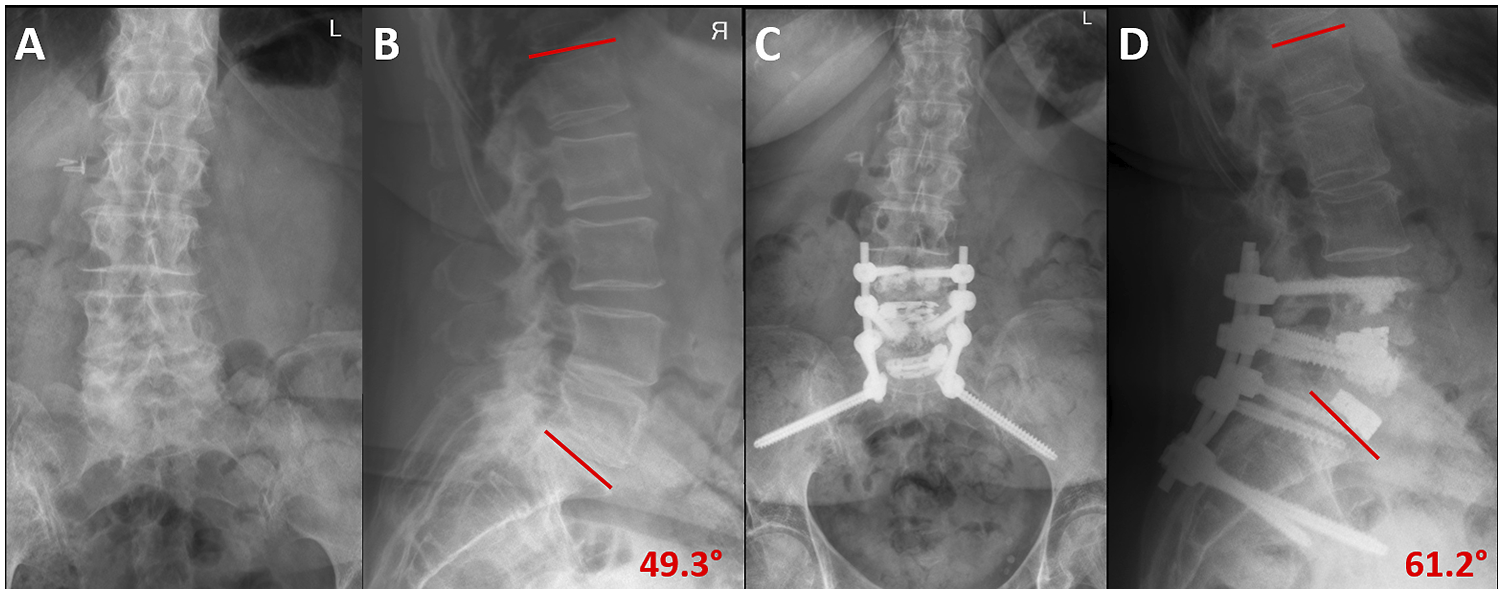
Study Groups & Statistical Analysis
Our main (independent) variable of interest was the occurrence of intraoperative ID with arachnoid injury and CSF leakage. Hence, patients experiencing “Incidental Durotomy” (ID) were considered the study group. A control group was built out of remaining patients with either no ID or a minor ID without arachnoid opening (‘No ID'). Our dependent variables of interest included demographic and surgical parameters, as well as radiological and clinical outcomes, as described above. Descriptive statistics were used to report means (including standard deviation (SD)), absolute and relative frequencies (count, percent) as well as 95% confidence intervals (CI). The cohorts were compared using independent samples t-tests for continuous variables or Pearson chi-square tests for categorical variables. Uni- and multivariable logistic regression models were built, calculating odds ratios (OR) and 95% CIs.
All statistical analyses were performed using Stata SE (StataCorp LLC, College Station, TX, USA) v18.0 software for Mac iOS. An alpha level of P < .05 was considered statistically significant.
Ethical Considerations
The study received approval from the institutional review board (IRB) of Eastern Switzerland (BASEC ID 2023-01343). The retrospective nature of the study allowed for a waiver of informed consent for the analysis and publication of anonymized patient data.
Results
Baseline Characteristics
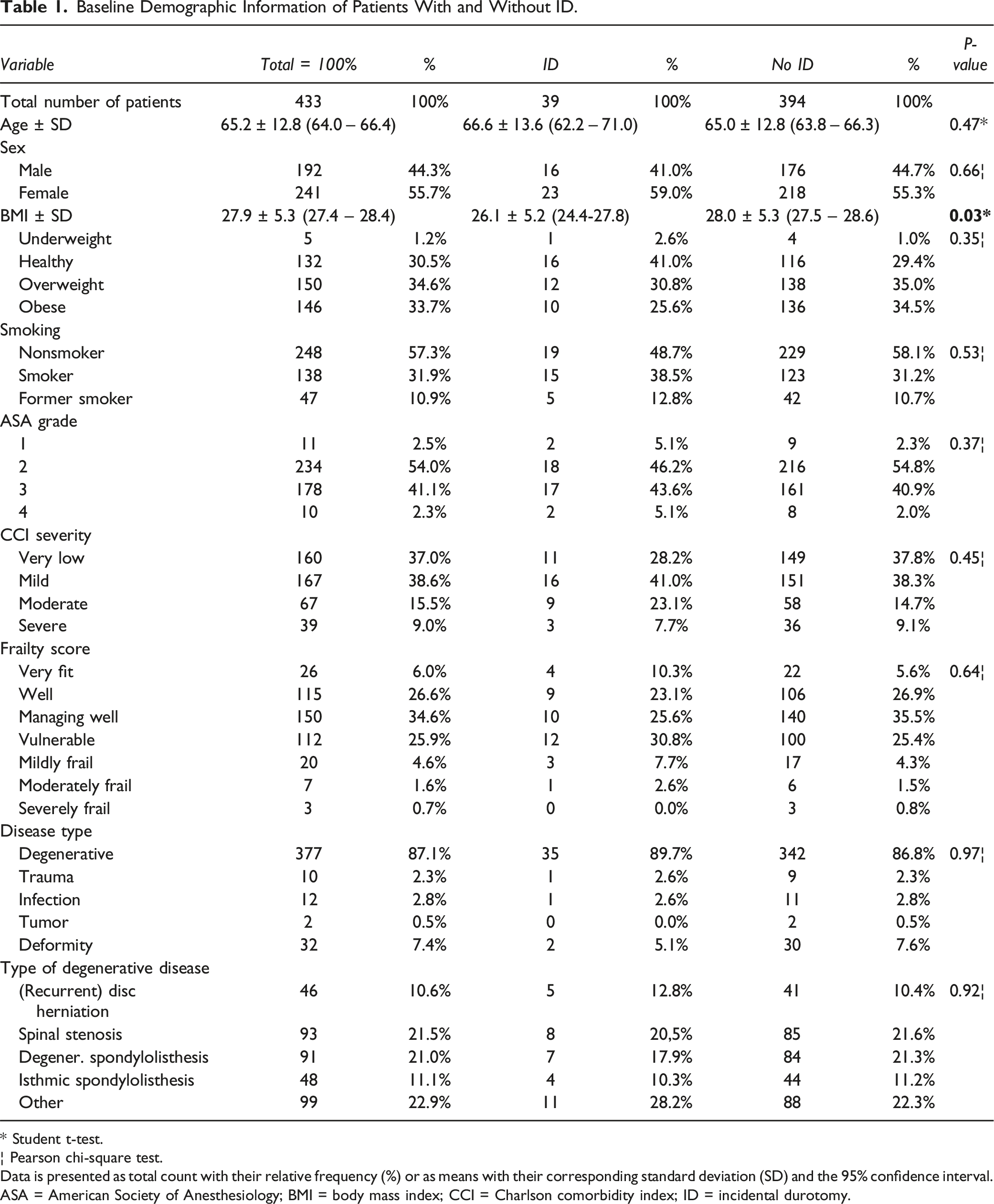
A total of n = 433 patients with expandable ALTERA® spacers implanted at 538 levels were considered eligible for the analysis, of which 39 patients (9.0%; 39 spacers implanted) experienced ID, while the remaining 394 patients (91.0%) were categorized as ‘No ID' control group. The mean age of the ID cohort was 66.6 years (SD 13.6), and 59% were female. About 56% of patients were overweight (BMI ≥ 25-30 kg/m2) or obese (BMI >30 kg/m2), about 51% were smokers or had a previous history of smoking and approximately 31% had moderate to severe comorbidities. The procedures were mostly performed for a degenerative pathology.
Baseline Demographic Information of Patients With and Without ID.
* Student t-test.
¦ Pearson chi-square test.
Data is presented as total count with their relative frequency (%) or as means with their corresponding standard deviation (SD) and the 95% confidence interval. ASA = American Society of Anesthesiology; BMI = body mass index; CCI = Charlson comorbidity index; ID = incidental durotomy.
Surgery-Related Characteristics
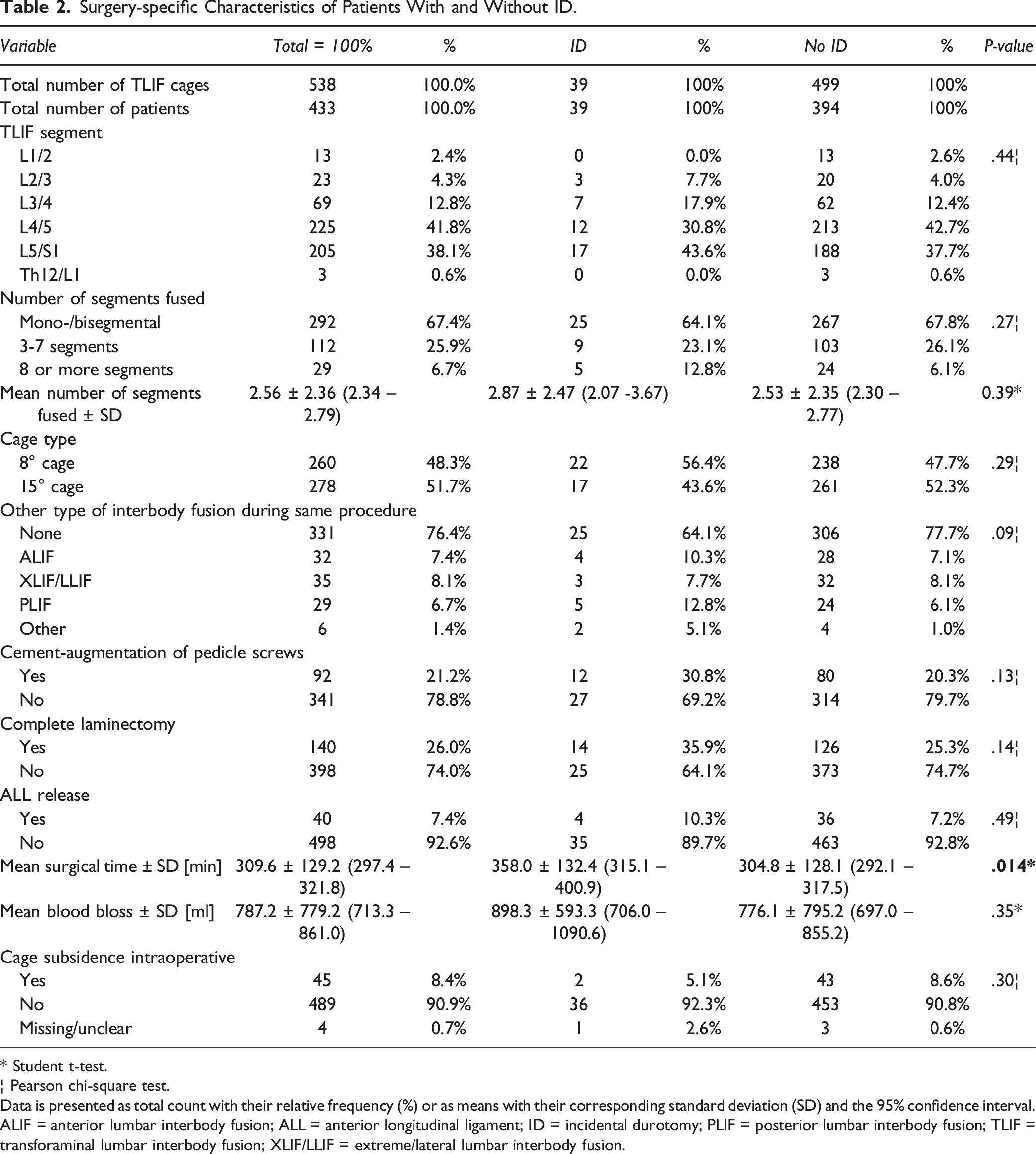
Surgery-specific Characteristics of Patients With and Without ID.
* Student t-test.
¦ Pearson chi-square test.
Data is presented as total count with their relative frequency (%) or as means with their corresponding standard deviation (SD) and the 95% confidence interval. ALIF = anterior lumbar interbody fusion; ALL = anterior longitudinal ligament; ID = incidental durotomy; PLIF = posterior lumbar interbody fusion; TLIF = transforaminal lumbar interbody fusion; XLIF/LLIF = extreme/lateral lumbar interbody fusion.
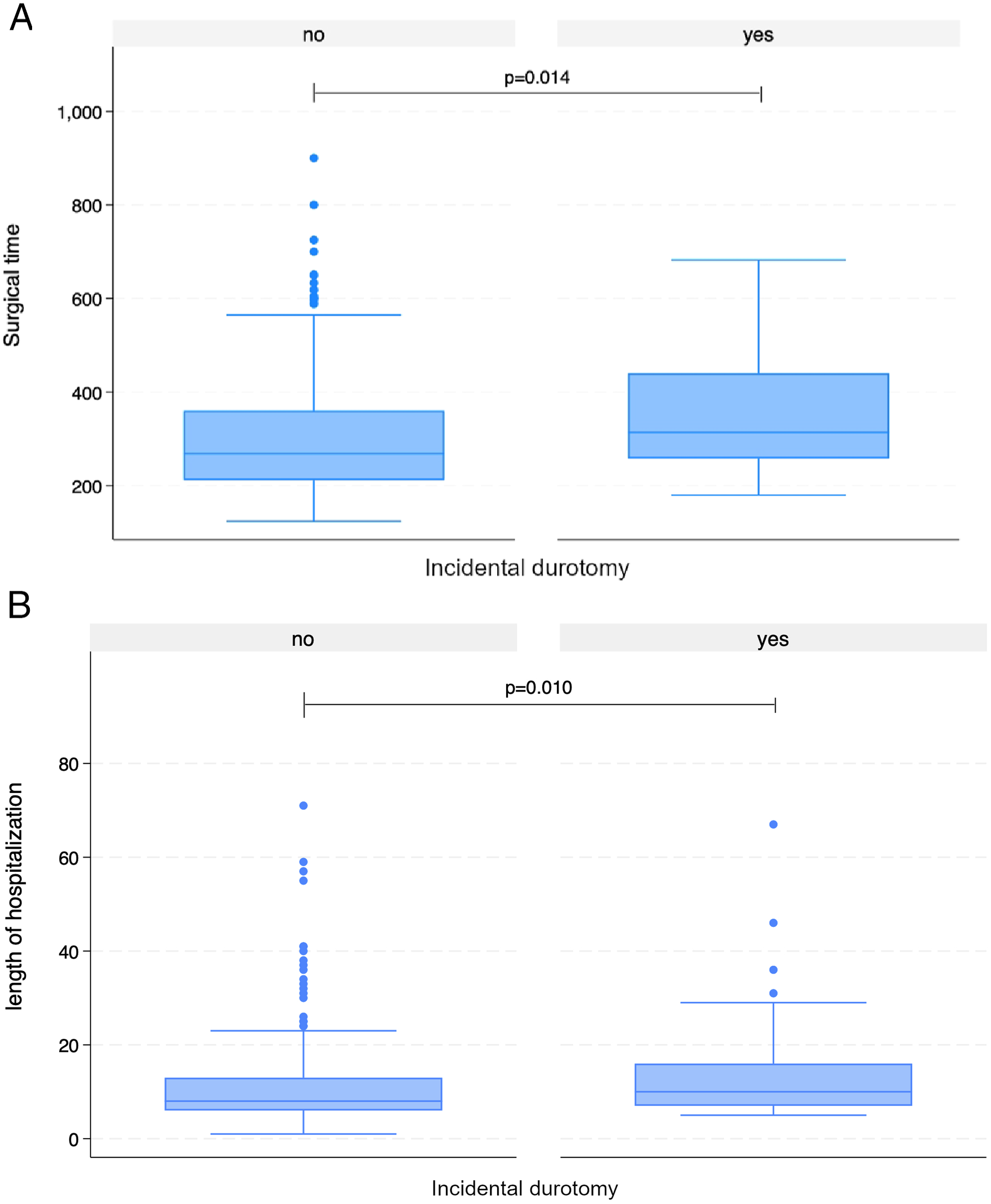
(A) Surgical time (in minutes) in patients with and without incidental durotomy (ID). Patients with ID had significantly longer surgeries (P = 0.014). (B) Length of hospital stay (in days) in patients with and without incidental durotomy (ID). Patients with ID had significantly extended hospital stays (P = 0.010).
AEs and Outcomes
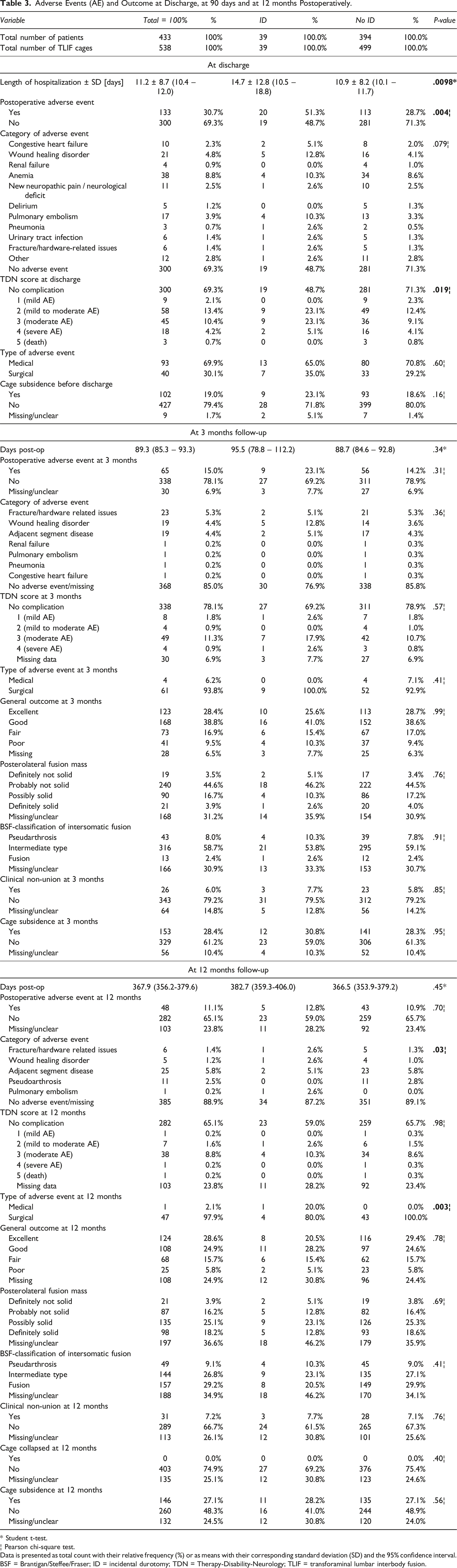
Length of stay (LOS) in patients with ID was approximately 3 days longer (14.7 ± 12.8 vs 10.9 ± 8.2 days, P = .010, Figure 2B) and they experienced more often postoperative AEs until discharge (51.3% vs 28.7%, P = .004), including wound healing disorders (12.8% vs 4.1%) and pulmonary embolisms (PEs; 10.3% vs 3.3%). The AEs were more severe on average, with a TDN score of 3 or more (i.e., moderate or severe) in more than a quarter of the patients with ID compared to 14% in patients without ID (P = .02).
Adverse Events (AE) and Outcome at Discharge, at 90 days and at 12 months Postoperatively.
* Student t-test.
¦ Pearson chi-square test.
Data is presented as total count with their relative frequency (%) or as means with their corresponding standard deviation (SD) and the 95% confidence interval. BSF = Brantigan/Steffee/Fraser; ID = incidental durotomy; TDN = Therapy-Disability-Neurology; TLIF = transforaminal lumbar interbody fusion.
Over the postoperative follow-up period, ten patients with (25.6%) and 31 patients without ID (7.9%) experienced wound healing issues (P < .001). In univariable analysis, patients with ID were four times as likely as patients without ID to experience wound healing disorders until 12 months (OR 4.04, 95% CI 1.80-9.04, P = .001). After adjusting the model for baseline differences in BMI and other types of interbody fusion, the model remained robust (adjusted OR 4.39, 95% CI 1.90-10.2, P = .001; Supplemental Table 1).
Until 12 months postoperative, five patients with (12.8%) and 14 patients without ID (3.6%) experienced a PE (P = .007). In univariable analysis, patients with ID were four times as likely as patients without ID to experience a PE until 12 months (OR 3.99, 95% CI 1.36-11.8, P = .012). After adjusting the model for baseline differences in BMI and other types of interbody fusion, the model remained robust (adjusted OR 3.52, 95% CI 1.13-10.9, P = .029; Supplemental Table 2).
Radiological Parameters
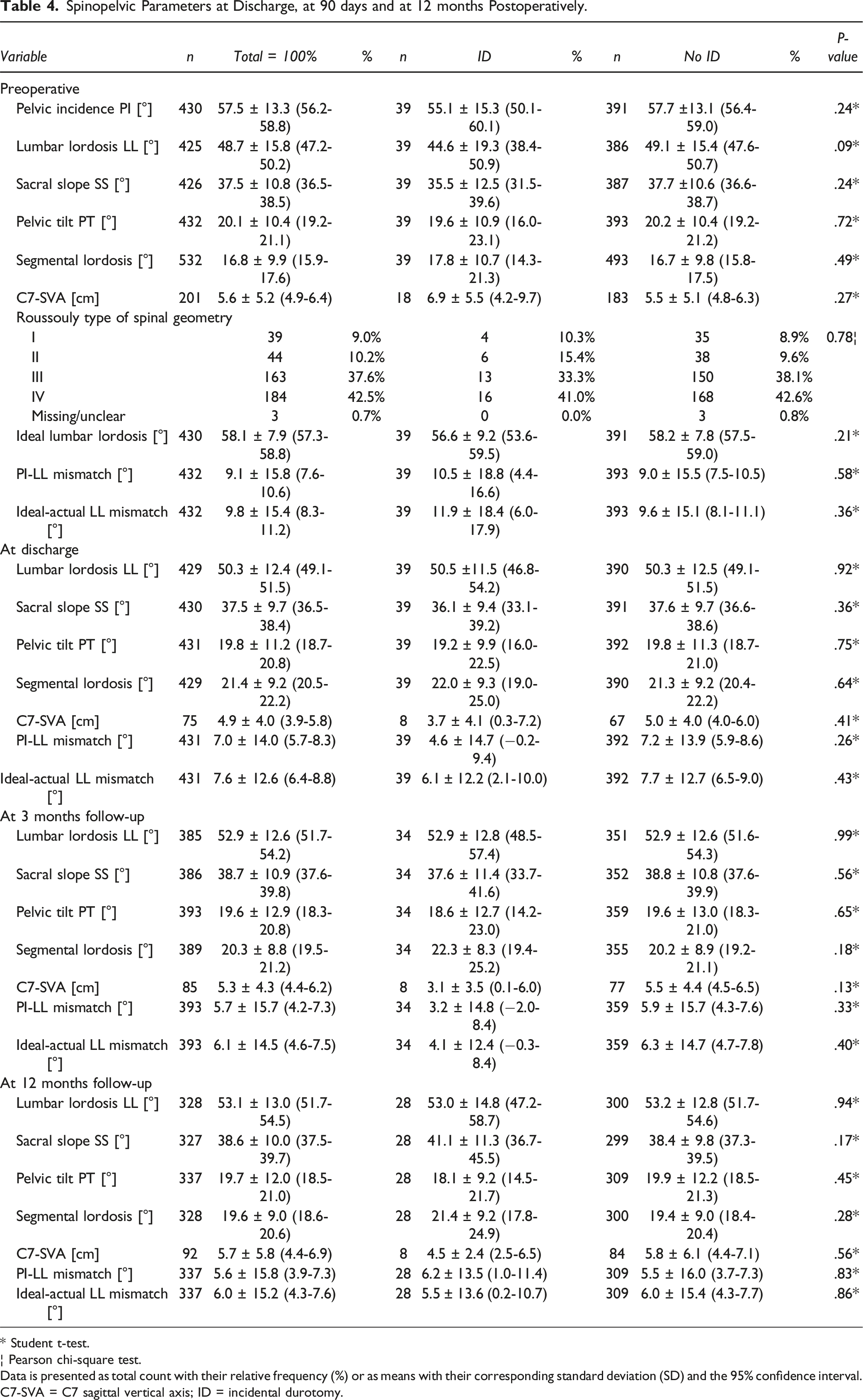
Spinopelvic Parameters at Discharge, at 90 days and at 12 months Postoperatively.
* Student t-test.
¦ Pearson chi-square test.
Data is presented as total count with their relative frequency (%) or as means with their corresponding standard deviation (SD) and the 95% confidence interval. C7-SVA = C7 sagittal vertical axis; ID = incidental durotomy.
Discussion
As life expectancy increases, so does the prevalence of degenerative lumbar spine conditions, leading to a rise in lumbar spine surgeries.4,20 ID ranks among the most common AEs for these surgeries, underscoring the importance of identifying independent risk factors and understanding their impact on downstream AEs and clinical outcomes. In this cohort of patients with a wide variety of underlying pathologies treated with TLIF and use of an expandable interbody spacer, the rate of ID was 9%, making it the most frequent intraoperative complication, which aligns well with current literature reports, ranging from 2.4-12.8%.4,20-24 The most striking findings of this study is that ID was associated with longer surgical time, length of hospitalization and frequency as well as severity of early postoperative AEs, while its negative impact on mid- to long-term outcome seems to be limited.
Risk Factors for ID
Our data did not reveal strong statistical associations between patient demographics and ID, except for a lower mean BMI in patients with ID (Table 1). This finding was not expected, as most prior literature indicates a higher risk for ID in overweight or obese patients.4,20,22,24,25 As such, a U.S. nationwide study by Hanna et al. revealed that ID was more prevalent in obese individuals. 4 Their study encompassed 439 220 patients who underwent lumbar spinal fusion, with 2.6% (n = 11 636) experiencing ID. Similarly, Burks et al. reported a significant increase in ID rates among obese patients undergoing lumbar fusion procedures. 22 The incidence of ID further increased in obese patients undergoing either revision or more complex fusion procedures.20,22,24 A systematic review by Weiss et al. suggested that MIS approaches might reduce overall complications, including the rate of IDs, in obese patients. 25 Obesity is a known risk factor for delayed fusion, increased wound infection risk, and unfavorable outcomes.4,26 The higher rate of ID in patients with elevated BMI may be attributed to the increased depth of the surgical site resulting in surgical challenges as well as inflammatory effects of adipose tissue on connective tissue.4,22 As only about one third of patients in our cohort were obese, the sample may have been underpowered to detect a significant negative impact of obesity on the rate of ID. In fact, most IDs in our cohort occurred in patients considered “healthy”, when BMI was stratified for World Health Organization categories (Supplemental Figure 1).
Our analysis did also not identify age, frailty, sex, smoking status, ASA score, or comorbidity indexes as risk factors. The literature regarding these variables is heterogenous, with a prior study on patients undergoing lumbar decompression without fusion suggesting female sex or higher age may increase the risk for ID. 23 The evidence regarding these variables is conflicting, however, and the effect size of these variables on the risk for ID likely limited. Other variables such as the number of previous surgeries, the presence of zygapophysial joint cysts or other anatomical factors, e.g., presence and degree of spondylolisthesis may play a more important role.3,4,21,23,24 Unfortunately, these variables were not available in our database.
We noticed a slightly lower baseline LL of about 5° in our ID cohort, while LL was identical postoperatively (Table 4). This may indicate that patients in the ID cohort underwent slightly more “aggressive” surgical procedures to restore LL, including the use of other interbody techniques with anterior lengthening, osteotomies and posterior shortening by compression. We did observe a slight trend towards more IDs in patients who had 8 or more segments fused, which aligns with current literature on lumbar decompressions and/or fusion, where is shown that multilevel surgery represents a risk factor.21,22,24 In line, patients experiencing an ID tended to have more PLIFs performed in addition to the TLIF during the same procedure (Table 2). PLIF requires more retraction of the dura than TLIF, which may have contributed to the effect. Altogether, it seems plausible that more extensive procedures increase the risk for ID.2,3,21,24 A retrospective study from Heidelberg examining lumbar interbody fusion identified previous lumbar surgery, the number of operated levels, and the surgeon’s experience as risk factors for ID. 21 In their study, nearly all patients (99.9%) received a complete laminectomy. In contrast, only 26% of our cohort had a complete laminectomy, and we found no correlation between the extent of laminectomy and the rate of ID. Notably, the duration of surgery was significantly longer in patients who experienced ID, which is consistent with previous studies.24,25 Whether the longer surgery predisposed to ID, or whether fixing the ID resulted in longer surgical time is not evident from our data.
It is theoretically conceivable that the use of expandable interbody spacers might reduce the risk of ID, as the device can be inserted requiring less dural retraction, with intradiscal in-situ expansion. The literature regarding the comparative risk for ID in static vs expandable TLIF cages is scarce, however. Chen et al. compared n = 62 patients, 30 of which were treated with an expandable cage. In the static cage group, no ID was detected, whereas in the expandable group one ID (3.33%) occurred. 27 The authors did not discuss in detail why the ID occurred. Weinstein et al. reported a similar ID rate in their study of n = 28 patients treated with an expandable interbody cage in a TLIF procedure, where one patient suffered ID (3.44%). 28 As our database did not comprise a control group of patients with static cages, we currently cannot judge upon the comparative risk profile but our ID rate was within the range of prior TLIF series using static cages. 27
Length of Hospitalization and In-Hospital AEs
Our findings align with those of Enders et al, who reported that ID during lumbar interbody fusion was associated with prolonged hospital stays of 1.5 days, possibly due to extended bed rest after surgery. 21 Similarly, we found that our patients with ID stayed about 3 days longer, compared to those without ID. Toci et al. reported similar results, noting a slightly increase in LOS of 24 hours. 24 In our department, bedrest for 24h is often recommended for patients with ID, even though the necessity for this has recently been challenged.5,6 Moreover, the higher rate of in-hospital AEs (51.3% vs 28.7%, P = .004), some of them requiring additional therapeutic measures, likely prohibited early discharge. Especially the rate of wound healing disorders was three times higher in patients with ID (12.8% vs 4.1%), and this in part resulted in revision surgery during the same hospitalization. We also noticed a 3-fold higher rate of PE in patients with ID (10.3% vs 3.3%), which may be attributed to reduced mobility resulting from the bed rest or symptoms resulting from ID, such as positional headache. Altogether, patients with ID demonstrated worse TDN scores at discharge, indicating that ID’s are associated with a higher likelihood for downstream complications that require health-care resources, (invasive) treatment and may result in significant morbidity.
Mid- & Long-Term AEs & Outcome
Our data suggests that at mid- (3 months) and long-term (12 months) follow-up, AEs and clinical outcomes were not inferior in patients with ID (Table 3). Still, despite lacking statistical significance, the rates of wound-healing disorders at 3 months still appeared somewhat higher with 12.8% in patients with and 3.6% in patients without ID. We found that overall, considering the complete postoperative follow-up interval of 12 months, patients with an ID were four times as likely to experience both, wound healing disorders and PEs, compared to patients without PE. The effect size remained stable, even after statistical adjustment for potential confounders. Yang et al have reported similar outcomes with an increased risk of deep vein thrombosis (DVT) after ID in spine surgery. 29 Enders et al. have stated the same hypothesis while reporting on prolonged bed rest due to postural symptoms in patients with TLIF surgery with expandable cages. 21 Interestingly, Burks et al. reported that obesity was another independent risk factor for both, ID and PE, in spinal surgery, suggesting that obese patients with ID need to be particularly monitored for PE. 22 In a large sample of 156 488 patients undergoing lumbar decompression, Gouzoulis et al. found an incidence of ID of 1.3% and that patients with ID had a significantly higher risk for DVT (OR 1.7), likely due to bed rest. 30 Fortunately, there was no mortality in patients with ID in our series. Other studies have similarly reported no impact of ID on long-term functional outcomes or postoperative complications.20,21,23,31 Toci et al. also found no deterioration in PROMs when patients experienced ID during lumbar decompression with or without fusion. 24
Sagittal Parameters
Analysis of radiographic sagittal parameters revealed a tendency towards less preoperative LL in patients with ID. The reason for this correlation remains unclear; it might be attributed to a more challenging anatomical angle for surgery, a greater need to restore lordosis with additional osteotomies & posterior compression, or a closer proximity of the dura to the posterior wall of the lamina. Similar findings were reported by Toci et al. Their study identified a higher risk for ID in patients with thoracolumbar kyphosis. 24 Even though our database does not comprise more details on the use of osteotomies & further specific intraoperative technical aspects, LL was identical in patients with ID’s and the control group in the postoperative interval (Table 4), which attests a greater degree of sagittal correction in this group.
Comparison to Other Lumbar Fusion Approaches
In the literature, TLIF has been shown to have a lower incidence of ID compared to PLIF. 20 We have observed a trend towards more IDs in patients undergoing additional fusion types (ALIF, LLIF, PLIF), suggesting an increased risk in procedures that use different techniques to approach the disc. While we have found very few studies comparing the rates of ID between expandable and static interbody cages in TLIF procedures, the rate of our study aligns with that reported in the literature.4,20-25 A systematic review by Ghobrial et al, encompassing 15 965 patients who underwent degenerative lumbar spine surgery, found no significant difference in the rate of ID between MIS-TLIF and open TLIF approaches. 20 However, more recent studies have suggested a slightly lower risk of IDs with MIS approaches (0.3-8% compared to 2.4-12.8%). 25 This finding is particularly important as the significance of sagittal parameters, especially segmental lordosis, becomes increasingly relevant, 8 leading to a corresponding increase in the use of expandable interbody implants in MIS approaches. Consequently, the rates of ID should be further evaluated through direct comparison between expandable and static interbody cages in future studies.
Strengths and Weaknesses
Our study presents findings from a large cohort of consecutive patients who underwent TLIF with expandable TLIF spacers. This innovative technology has gained increasing attention in the field of spinal surgery, yet the body of evidence supporting its use remains limited and our study aims to address this gap. 1 Despite its retrospective character, the missing data burden was reasonably low. Additionally, our series comprises a detailed record of intra- and postoperative AEs and grading of their severity using the TDN scale, 32 allowing for the identification of specific risks associated with ID.
Several limitations should be noted in the interpretation of our study results. Foremost, selection bias likely influenced our findings, as we did not control for the factors determining whether patients received an expandable TLIF spacer vs alternative fusion methods. Not having included a control group undergoing either TLIF with static cages or alternative fusion methods limits our ability to draw definitive conclusions about the comparative risks of these interventions to develop ID. Our assessment of functional outcomes was constrained by the recent standardized implementation of PROMs at our center in 2022. Consequently, we relied on the Macnab criteria, a simplified 4-tier scale, to evaluate functional outcome in the complete sample,12,33 while the available PROM data was used to classify outcome correctly. Another limitation relates to the availability of imaging data for the assessment of the degree of fusion. CT or SPECT scans were particularly performed in patients with new or remaining undesired symptoms during follow-up, to detect or rule out pseudarthrosis. This approach, while pragmatic, may have resulted in underestimating the rate of asymptomatic non-union.
Implications for Practice
It is crucial that patients are informed about the potential impact of ID on both their short-term and long-term outcomes. Treating physicians should be aware of the prolonging effects of ID on the length of surgery and hospitalization. The higher risk of PE should be addressed with close clinical (dyspnea) and technical (blood oxygen level) surveillance of patients that develop ID, as well as immediate thoracic CT scan in case of suspicious clinical signs. Early mobilization, symptomatic treatment of postural symptoms and, if needed, earlier use or higher dose chemoprophylaxis should be considered on an individual basis, balancing the risk of thromboembolic events with the risk of rebleeding. Postoperative monitoring of the wound for CSF fistula or signs of infection seems justified, considering the elevated risk. Moreover, the importance of ID prevention must be stressed, as AEs and undesired outcomes can potentially be mitigated or avoided.
Conclusions
Patients who experienced IDs in this series had longer OR time and increased LOS. AEs until discharge occurred more frequently in patients with ID and were more severe. Even though the risks for AE at 3 and 12 months were not significantly higher and clinical outcomes at follow-up were comparable, the odds to develop wound healing disorders or PEs until 12 months postoperatively were four times as high in patients with ID.
Supplemental Material
Supplemental Material - Incidental Durotomy During Transforaminal Lumbar Interbody Fusion (TLIF) Surgery with Expandable Interbody Spacers: A Retrospective, Single-Center Analysis of Complications and Outcomes
Supplemental Material for Incidental Durotomy During Transforaminal Lumbar Interbody Fusion (TLIF) Surgery with Expandable Interbody Spacers: A Retrospective, Single-Center Analysis of Complications and Outcomes by L. Bättig, F. Kissling, S. Motov, F. C. Stengel, Y. Yildiz, L. Feuerstein, G. Fischer, T. Schöfl, D. Gianoli, N. Hejrati, B. Martens, M. N. Stienen, and L. Bertulli in Global Spine Journal
Footnotes
Acknowledgments
The authors would like to thank the entire team at the Spine Center of Eastern Switzerland for their support in data collection and patient care.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.