
Abstract
Study Design
Systematic Review.
Objectives
Cervicothoracic junction (CTJ) deformities, particularly kyphosis, significantly impact patients’ quality of life, causing pain, dysphagia, and inability to maintain horizontal gaze. Various surgical osteotomy techniques are available to correct CTJ kyphosis, but their relative effectiveness and associated complications remain unclear. This systematic review and meta-analysis aim to provide an evidence-based comparison of different surgical techniques for correcting cervicothoracic sagittal imbalance.
Methods
A comprehensive search of PubMed, Scopus, Embase, and Web of Science was conducted up to August 2024. Studies included in the analysis involved adult patients undergoing cervical or upper thoracic osteotomy for sagittal imbalance correction. Data on radiographic outcomes, complication rates, and surgical factors were extracted and analyzed using random-effects models. Publication bias and heterogeneity were assessed using Begg’s test and I2 statistics, respectively.
Results
Twenty-three studies met the inclusion criteria, with a total of 995 patients. Pedicle subtraction osteotomy (PSO) provided the greatest correction for cervical sagittal vertical alignment (cSVA) and cervical lordosis (CL) compared to anterior cervical osteotomy (ACO) and Smith-Petersen osteotomy (SPO). Upper thoracic osteotomies showed superior correction of T1 slope (TS) and chin-brow vertical angle (CBVA). ACO had the lowest complication rate, while SPO showed the highest neurological complication rate, particularly at the C7-T1 level.
Conclusion
Cervicothoracic osteotomy techniques, while effective, present significant risks. PSO provides the most powerful correction but is associated with greater surgical risks, while ACO offers lower complication rates. These findings highlight the need for careful surgical planning based on patient-specific deformities and risk factors.
Introduction
The Cervicothoracic junction (CTJ) is a distinctive spinal region where the flexible, lordotic cervical spine transitions into the rigid, kyphotic thoracic spine. This area encompasses the joints of the lower cervical spine and the uppermost thoracic vertebrae, typically defined as C7–T1 or C7–T2, although this definition can be extended to include C6–T4.1–4 Kyphotic deformity at the CTJ can cause cervical sagittal imbalance, leading to significant morbidity, including pain, myeloradiculopathy, dysphagia, dysphonia, and difficulty maintaining horizontal gaze. 5 CTJ deformity can result from various causes, including congenital anomalies, intra- and extra-medullary tumors, rheumatological conditions such as ankylosing spondylitis, trauma, degenerative spondylosis, and iatrogenic factors (post-laminectomy).6,7 Severity ranges widely, with the most severe cases, such as chin-on-chest deformities, causing extreme disability and requiring extensive surgeries to restore horizontal gaze. 2
The unique anatomy and functional physiology of the CTJ makes it subject to unique opposing mechanical forces. The sharp transition of cervicothoracic curvature, the ventral neurovascular structures, 8 the flexibility of the cervical segment coupled with the relative rigidity of the thoracic area, and the small nature of the pedicle diameter in the cervical and upper thoracic portions all contribute to the challenges of corrective surgery, particularly in transpedicular screw placement and rod transition between these segments. 9
Despite the complexities of this region, there has been a growing focus on developing surgical osteotomy techniques to correct CTJ kyphosis. This manuscript aims to comprehensively review the existing literature on various surgical techniques for treating CTJ kyphosis and provide an evidence-based approach to this critical spinal region.
Methods
Protocol and Registration
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 10 Our review is registered in PROSPERO under the registration number CRD42024601493.
Literature Search
The search strategy was comprehensive, encompassing PubMed, Scopus, Embase, and Web of Science databases from their inception to August/2024. Medical subject headings (MeSH) terms and keywords were employed in each database search using the Boolean operators OR and AND. The terms used were “Cervic* AND Osteotomy AND (Deformity OR Kypho* OR Imbalance).” The search was limited to publications in English. We searched titles, abstracts, and keywords manually and individually to assess for inclusion in this analysis. The reference lists of key articles were reviewed to collect additional relevant studies.
Study Selection
Studies were included in this systematic review if they met the following eligibility criteria: (1) The procedure involved some form of cervical, cervicothoracic, or upper thoracic (T4 or above) spinal osteotomy, including various cervical osteotomies as classified by the Ames-ISSG classification 11 or upper thoracic osteotomies per the Schwab classification. 12 (2) the primary indication for surgery was cervical and/or cervicothoracic sagittal imbalance. (3) participants were 18 years of age or older.
Studies were excluded if they did not meet the inclusion criteria or if the following conditions were present: (1) They were meta-analyses, reviews, editorials, letters, or books. (2) Incomplete patient demographic and alignment data. (3) The study received a poor-quality rating as assessed by the Joanna Briggs Institute (JBI) critical appraisal tool. 13 (4) Case series with fewer than 4 patients were also excluded.
Quality Assessment
Two investigators (SB and MR) independently assessed the quality of the selected studies using a predefined standardized set of criteria. Cohort studies were evaluated using the 11-question JBI critical appraisal tool, 13 while case series studies were assessed with the 10-question JBI tool. 14 The appropriate checklist was applied based on the study design to ensure a rigorous evaluation of internal validity. In cases of disagreement, a third reviewer (FR) was consulted to reach a consensus. The overall quality of the studies, as determined by the JBI tool, was categorized based on responses to specific appraisal questions as follows: studies with ≤1 “No” or ≤2 “Unclear” responses were classified as high quality, those with 2 “No” or 2-4 “Unclear” responses were considered moderate quality, and those with >2 “No” or >4 “Unclear” responses were deemed low quality. 13
Data Extraction
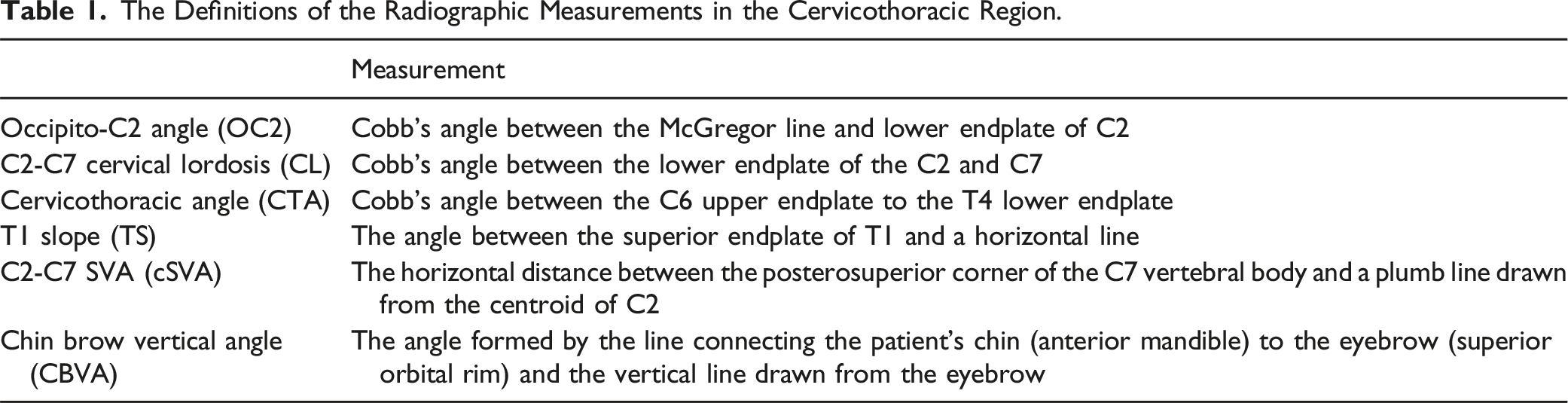
The Definitions of the Radiographic Measurements in the Cervicothoracic Region.
Statistical Analysis
In this study, we utilized the Comprehensive Meta-analysis (CMA) software, version 4.0. The studies analyzed were considered random samples from a larger population. Based on this assumption, we used the random-effects model to generalize our results to all adult patients undergoing cervicothoracic sagittal imbalance surgery. We applied random effects synthesis to estimate the mean and calculated the 95% Confidence Interval (CI). Statistical significance was determined using a P-value threshold of <.05. Sensitivity analysis was performed by removing each study individually and calculating the P values of the remaining studies. As there were fewer than ten studies for each variable, we conducted Begg’s test to assess potential publication bias for variables reported in at least 3 studies (P < .05 indicating publication bias). 15 If publication bias was detected through Begg’s test, we applied the Trim and Fill method to estimate the adjusted mean. 16 We used I2 statistics to assess the heterogeneity between studies. (0-25%: Low, 25-50%: Moderate, 50-75%: Substantial, 75-100%: Considerable). 17
Results
Study Identification
A total of 292 publications were identified based on the search criteria. After removing duplicates, 169 articles remained. Of these, 107 were excluded after screening the title and abstract. From the remaining 62 articles, 39 were excluded for the following reasons: failure to meet inclusion criteria (15), lack of relevant data (6), duplication (16), and unavailable full text (2). Finally, 23 articles were included in the meta-analysis (Figure 1). PRISMA flow diagram outlining the study’s systematic search process. The diagram illustrates the identification, screening, eligibility assessment, and inclusion of studies in the meta-analysis, detailing the number of records at each stage and reasons for exclusion.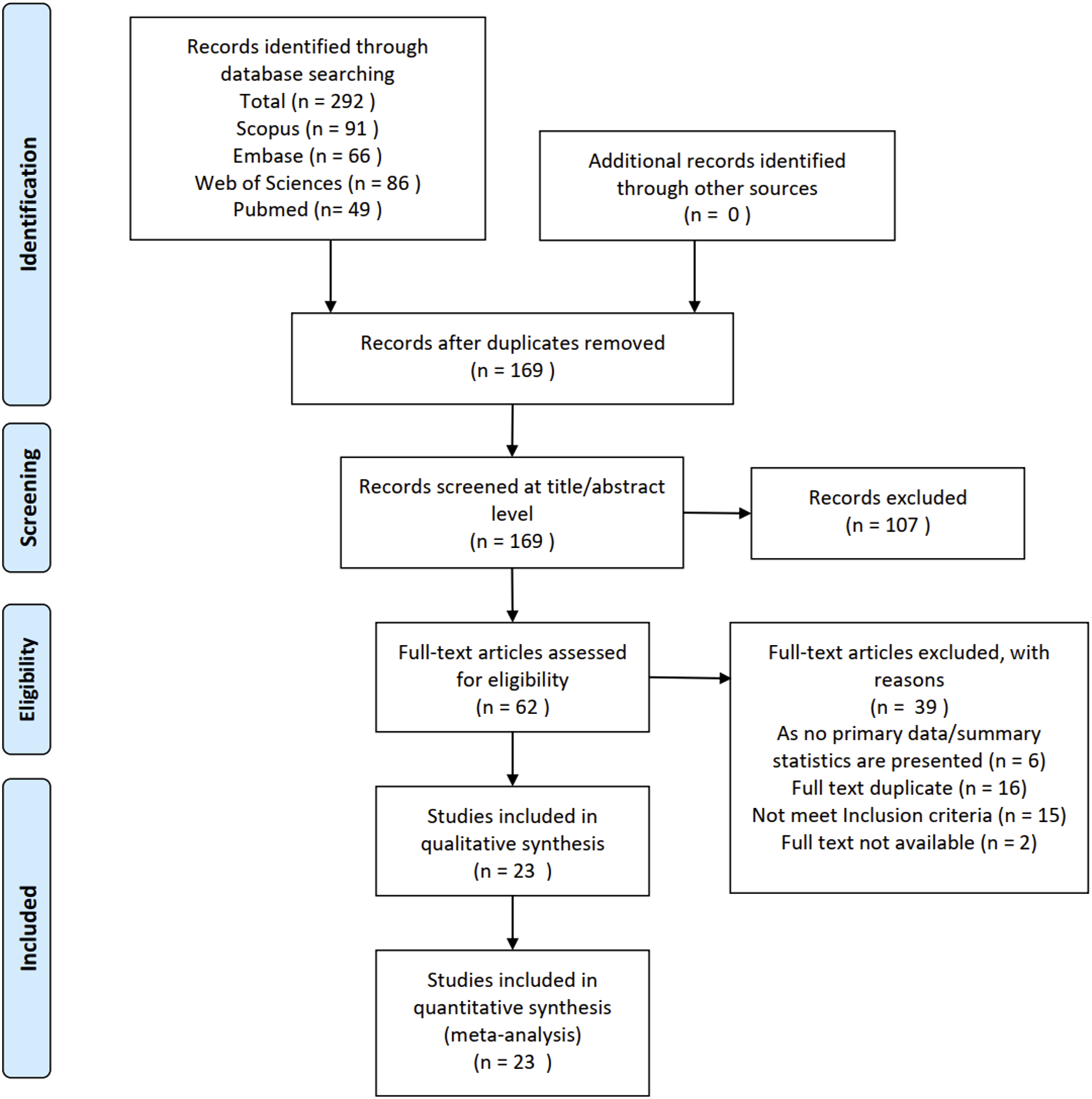
Study Characteristics
Results of Critical Appraisal Using KBI Criteria for Case Series Studies.
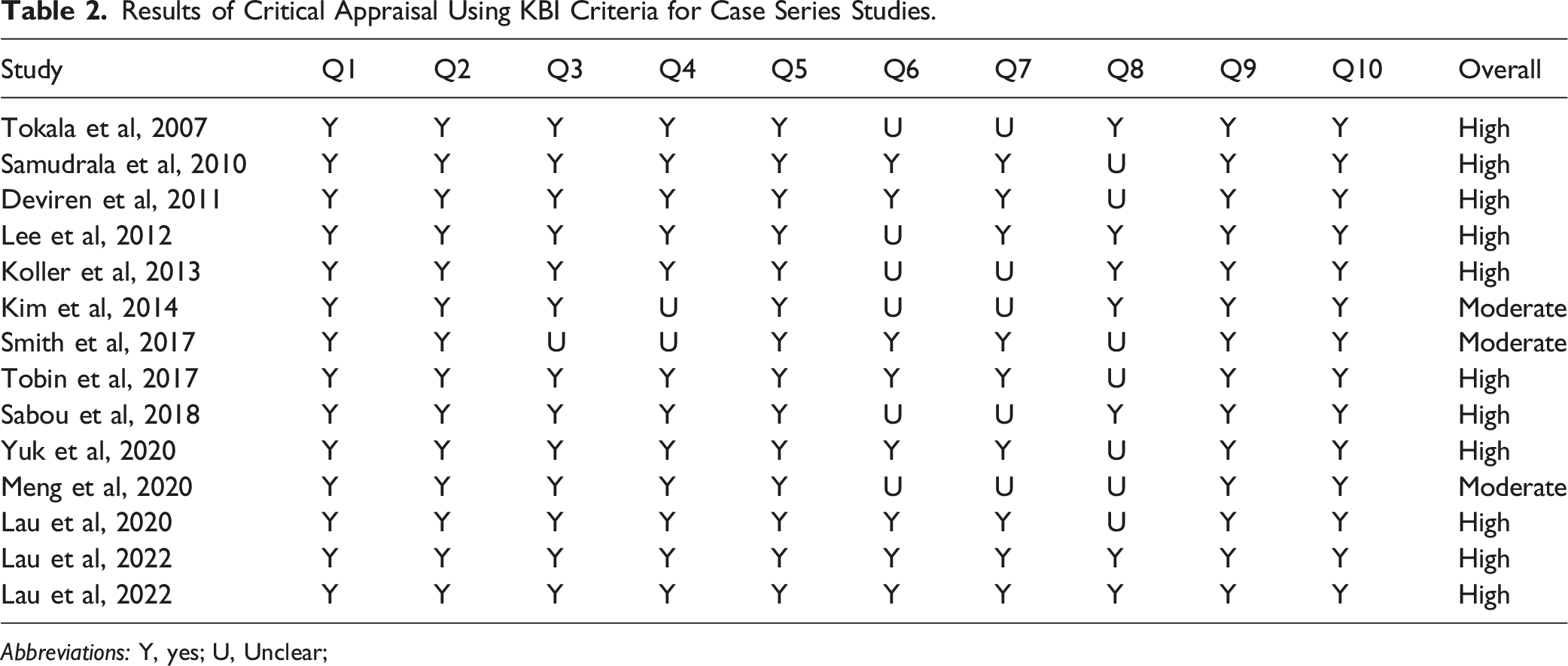
Abbreviations: Y, yes; U, Unclear;
Results of Critical Appraisal Using KBI Criteria for Cohort Studies.
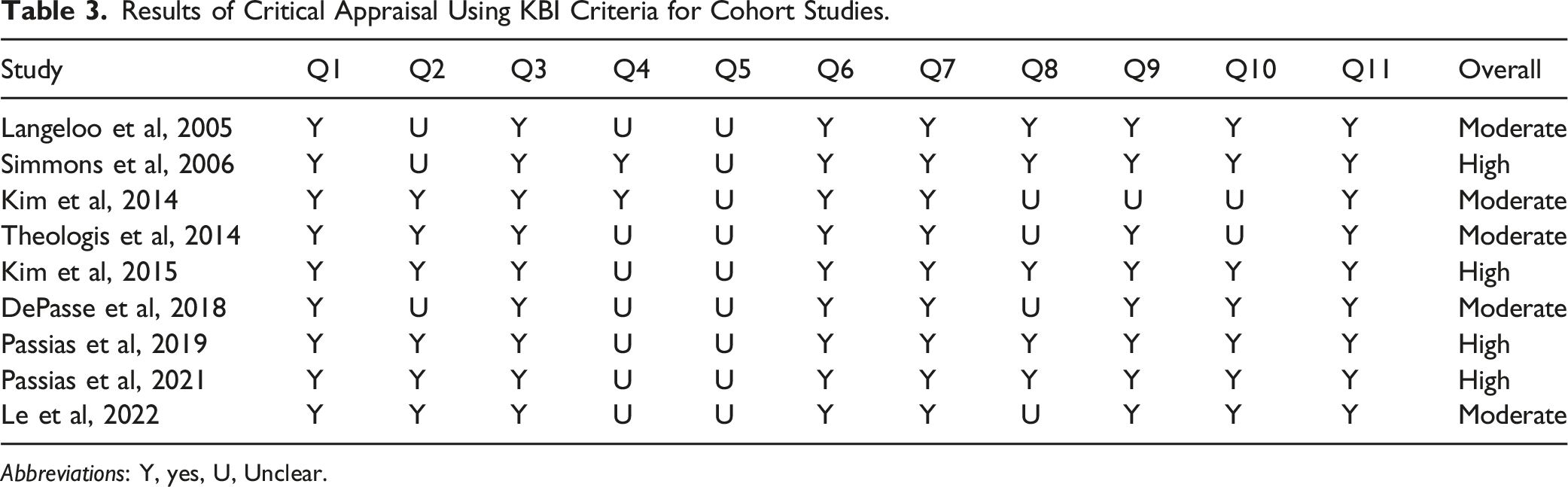
Abbreviations: Y, yes, U, Unclear.
Overall Features of Included Studies.
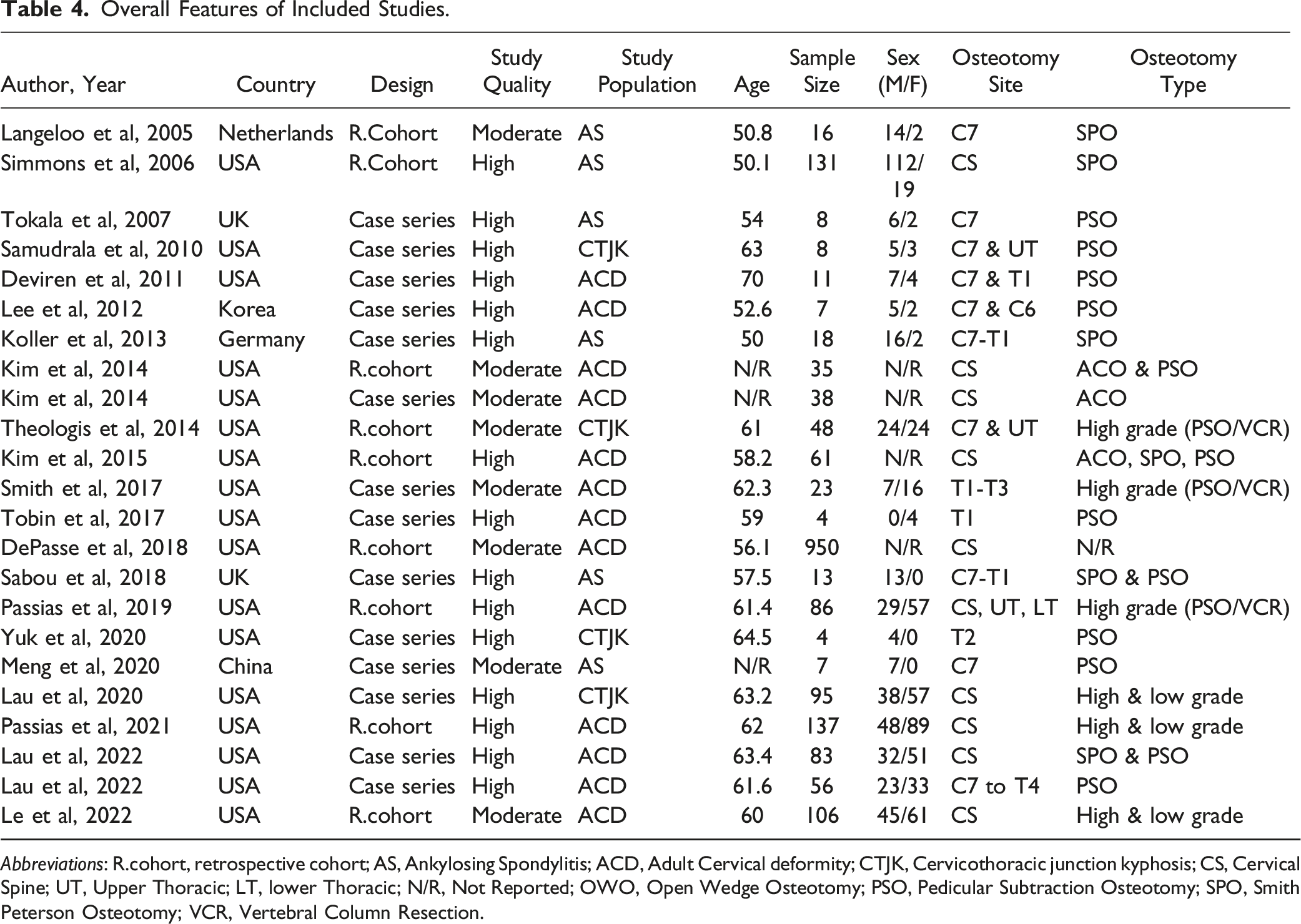
Abbreviations: R.cohort, retrospective cohort; AS, Ankylosing Spondylitis; ACD, Adult Cervical deformity; CTJK, Cervicothoracic junction kyphosis; CS, Cervical Spine; UT, Upper Thoracic; LT, lower Thoracic; N/R, Not Reported; OWO, Open Wedge Osteotomy; PSO, Pedicular Subtraction Osteotomy; SPO, Smith Peterson Osteotomy; VCR, Vertebral Column Resection.
Correction Power of Each Type of Osteotomy
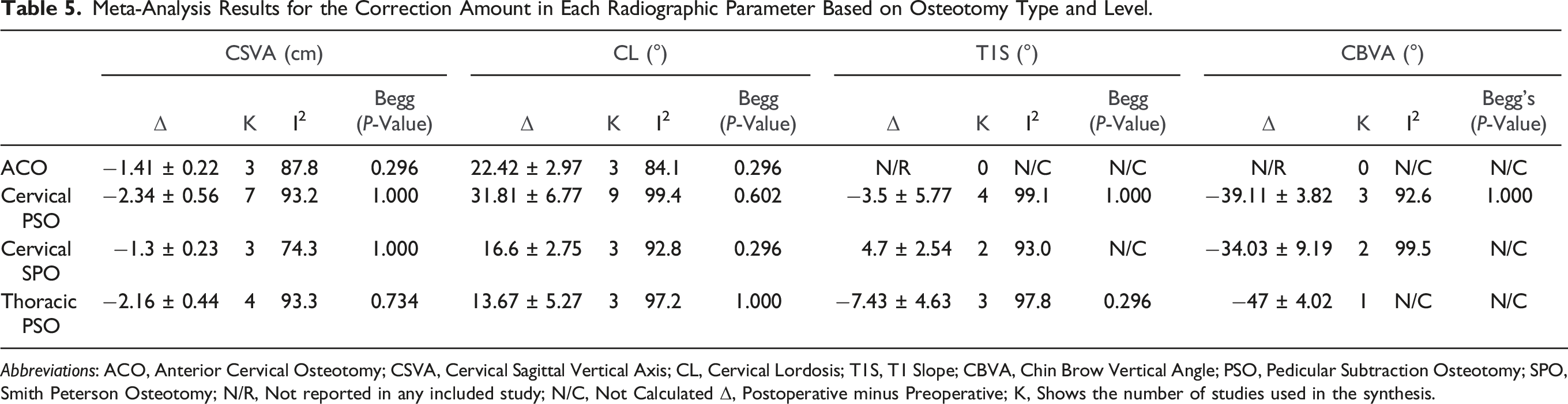
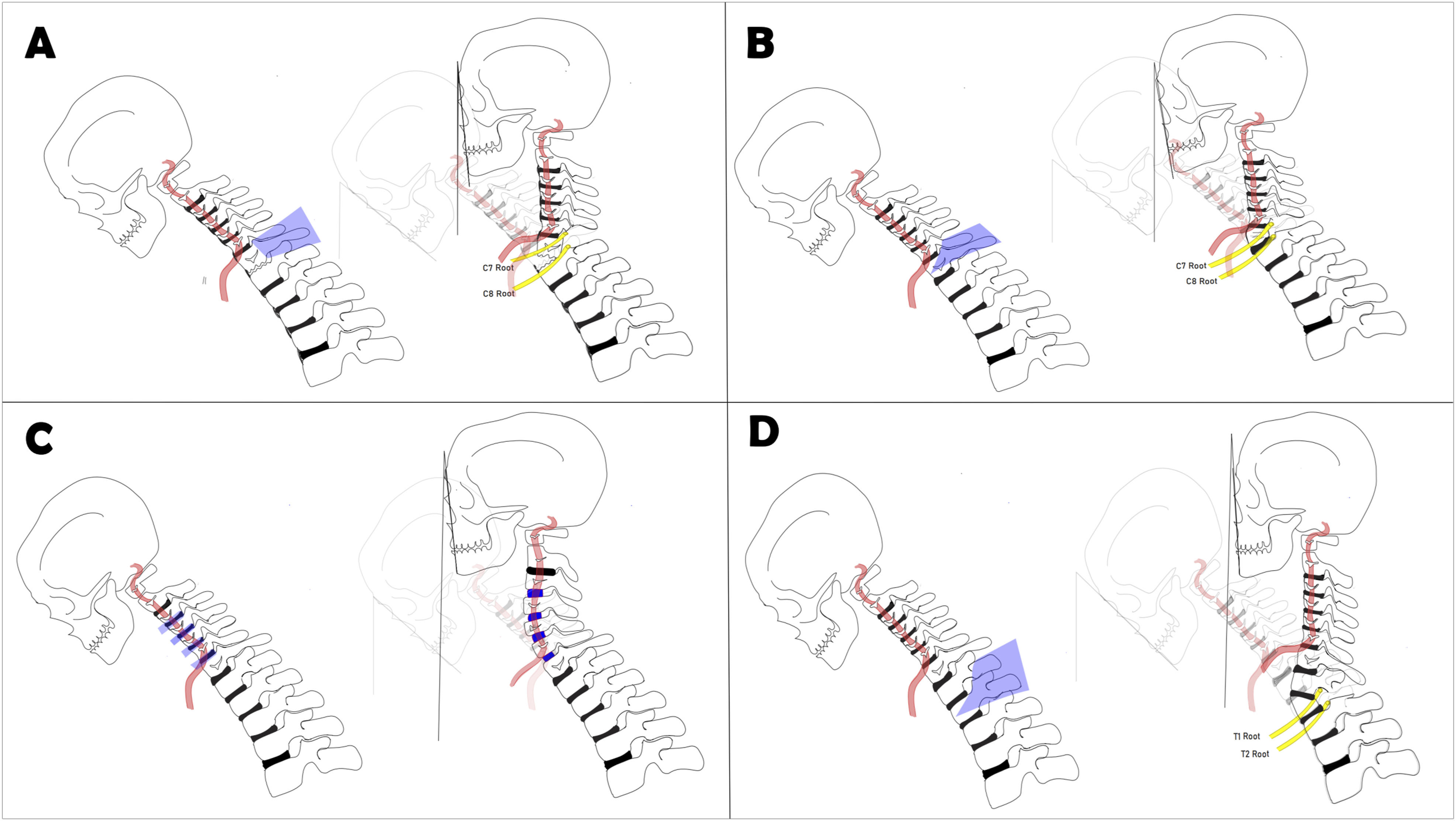
Figure 2 and Table 5 summarize the estimated corrective strength for each reported type of osteotomy. Figure 3 provides a schematic representation of the 4 osteotomy techniques discussed. Direct quantitative comparisons cannot be made since most of the data are derived from cross-sectional studies. However, based on our meta-synthesis, the below-mentioned results are calculated. Meta-analysis results for the magnitude of correction in various radiographic parameters based on osteotomy type. The analysis evaluates changes in Cervical Sagittal Vertical Axis (CSVA), Cervical Lordosis (CL), T1 Slope (T1S), and Chin-Brow Vertical Angle (CBVA) across different osteotomy techniques, including Anterior Cervical Osteotomy (ACO), Pedicle Subtraction Osteotomy (PSO), and Smith-Petersen Osteotomy (SPO). Meta-Analysis Results for the Correction Amount in Each Radiographic Parameter Based on Osteotomy Type and Level. Abbreviations: ACO, Anterior Cervical Osteotomy; CSVA, Cervical Sagittal Vertical Axis; CL, Cervical Lordosis; T1S, T1 Slope; CBVA, Chin Brow Vertical Angle; PSO, Pedicular Subtraction Osteotomy; SPO, Smith Peterson Osteotomy; N/R, Not reported in any included study; N/C, Not Calculated Δ, Postoperative minus Preoperative; K, Shows the number of studies used in the synthesis. Schematic representation of the 4 osteotomy techniques discussed. Each panel illustrates the anatomical site, surgical technique, and resulting correction. The purple sections highlight the anatomical structures and the surgeon’s approach to the procedure. (A) Cervical Smith-Petersen Osteotomy (Cervical SPO), (B) Cervical Pedicle Subtraction Osteotomy (Cervical PSO), (C) Anterior Cervical Osteotomy (ACO), and (D) Thoracic Pedicle Subtraction Osteotomy (Thoracic PSO). The correction of the Chin-Brow Vertical Angle (CBVA) achieved with these techniques is also depicted.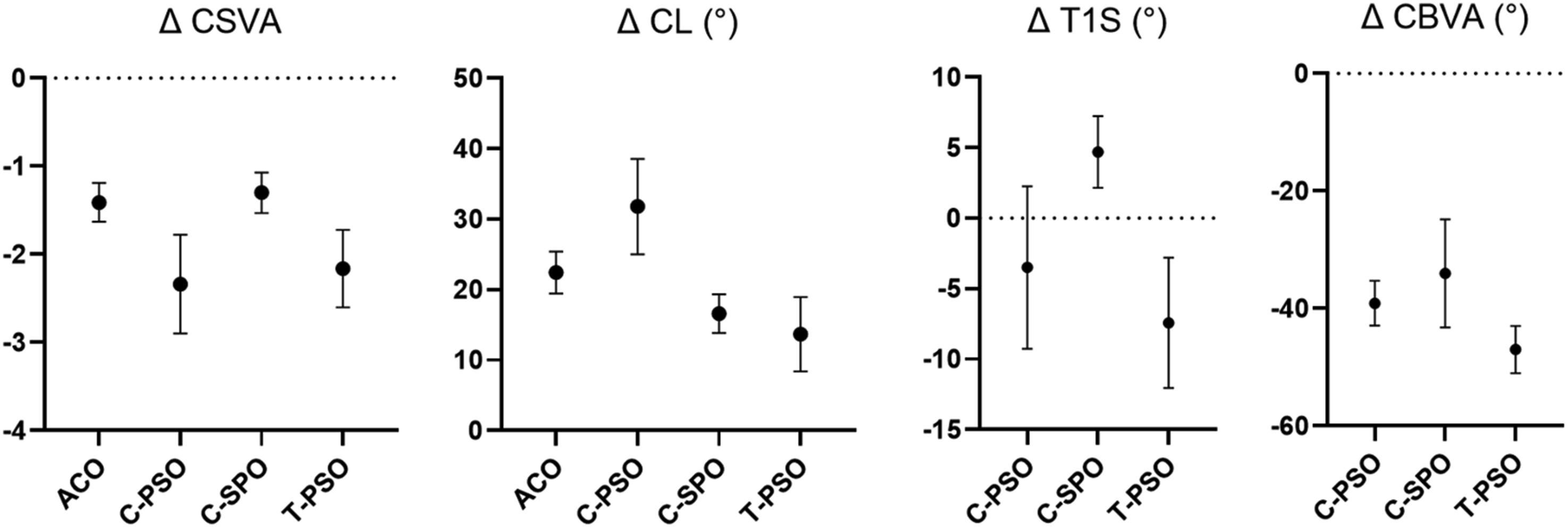
Cervical SVA Correction (Δ CSVA in cm)
The ACO (−1.41 ± 0.22 cm) and Cervical SPO (−1.3 ± 0.23) procedures provide a comparable degree of correction for cSVA. However, both ACO and SPO are less effective in correcting cSVA compared to PSO, which offers superior translational correction, whether performed in the lower cervical (−2.34 ± 0.56 cm) or upper thoracic (−2.16 ± 0.44 cm) regions.
Cervical Lordosis Correction (Δ CL in Degrees)
As shown in Table 3, C-PSO provides the greatest CL correction (31.81 ± 6.77), while T-PSO, as expected, offers the least correction (13.67 ± 5.27). Among cervical osteotomies, the magnitude of correction was highest with PSO, followed by ACO, and then SPO, in decreasing order.
T1 Slope Correction (Δ TS in Degrees)
In T-PSO, performing the osteotomy below the T1 vertebra results in the highest TS correction at −7.43 ± 4.63. In contrast, C-PSO provides roughly half the TS correction compared to T-PSO. Interestingly, C-SPO, typically performed at the C7-T1 level, increases the T1 slope by 4.7 ± 2.54°.
Chin Brow Vertical Angle Correction (ΔCBVA in Degrees)
T-PSO offers the greatest correction in CVBA (−47 ± 4.02). In comparison, C-SPO (−34.03 ± 9.19) and C-PSO (−39.11 ± 3.82) provide similar correction in CBVA.
Surgical Factors and Complication Rate
Figure 4 and Table 6 summarize the data on surgical procedures and complications. However, it is important to note that these are general findings and have not been tested for statistical significance. Meta-analysis results for complication rates based on osteotomy type. The analysis compares the complication rates associated with different osteotomy techniques, including Anterior Cervical Osteotomy (ACO), Pedicle Subtraction Osteotomy (PSO), and Smith-Petersen Osteotomy (SPO). Estimated Blood Loss (EBL) is also evaluated as a potential factor influencing complication rates. Meta-Analysis Results for the Surgical Factors and Complication Rate Based on Osteotomy Type and Level. Abbreviations: ACO, Anterior Cervical Osteotomy; EBL, Estimated Blood Loss; PSO, Pedicular Subtraction Osteotomy; SPO, Smith Peterson Osteotomy; K, Shows the number of studies used in the synthesis; N/C, Not Calculated.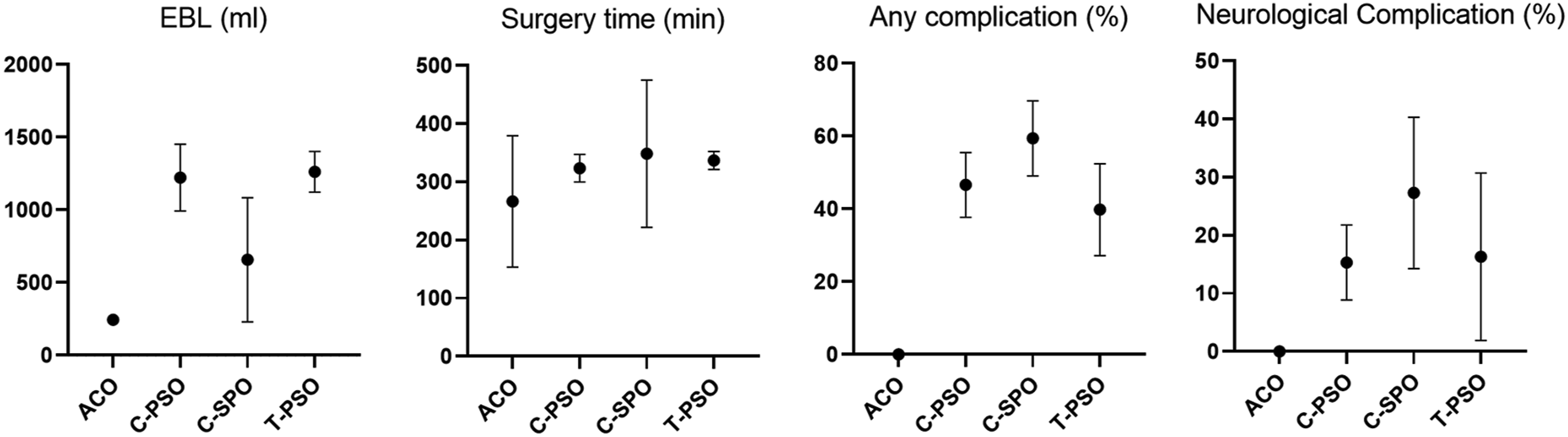
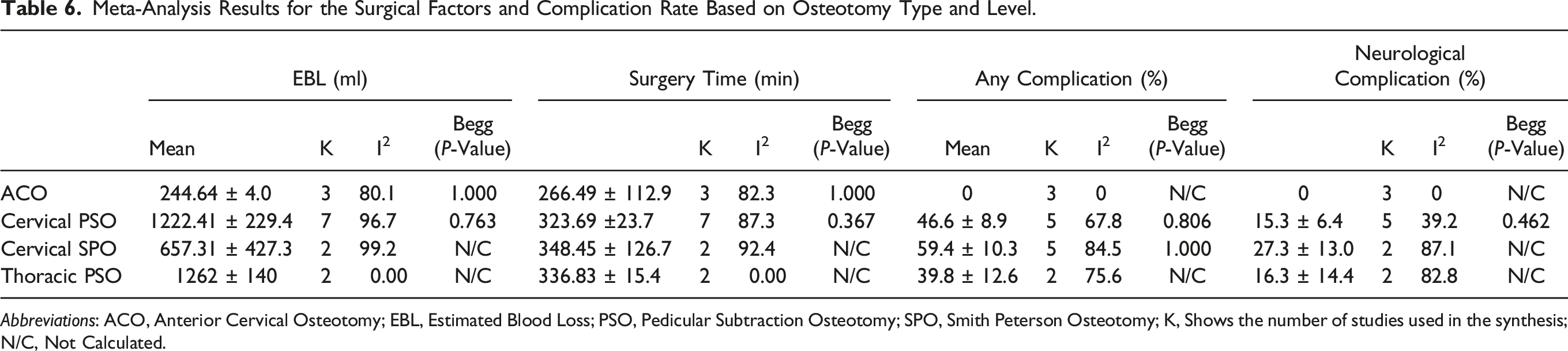
Estimated Blood Loss (EBL in Milliliter)
In the comparative analysis, it was found that T-PSO (1262 ± 140) and C-PSO (1222.41 ± 229.44) exhibited similar levels of blood loss, both exceeding the EBL observed in C-SPO (657.31 ± 427.34). Notably, ACO showed the lowest EBL (244.64 ± 4.06).
Surgery Time (in Minutes)
The surgical durations for T-PSO (336.83 ± 15.47), C-PSO (323.69 ± 23.70), and C-SPO (348.45 ± 126.71) are comparable. However, ACO has a notably shorter surgical duration (266.49 ± 112.97).
Any Complication (in Percent)
As shown, C-SPO has the highest rate of surgical, medical, or neurological complications (59.4 ± 10.3). Notably, no complications were reported in association with ACO.
Neurological Complications (in Percent)
Patients who underwent C-SPO had the highest incidence of neurological complications (27.3 ± 13.01), while those who underwent T-PSO (16.3 ± 14.41) and C-PSO (15.3 ± 6.45) showed similar rates of neurological complications.
Publication Bias and Heterogeneity Assessment
Based on the results of our meta-analysis assessing publication bias using Begg’s test, no significant publication bias was detected for any of the variables. However, the I2 statistics for most of the variables showed considerable heterogeneity between the results of each study. This high heterogeneity can be attributed to the inclusion of many case series studies and may be explained by variability in design, patient populations, and outcome measures. Notably, Thoracic PSO EBL and Surgery time had low heterogeneity, while Cervical PSO Neurological Complication showed moderate heterogeneity, and Cervical PSO any complication and Cervical SPO ΔcSVA exhibited substantial heterogeneity.
Discussion
The findings of this systematic review and meta-analysis provide an overview of the efficacy of various high-grade osteotomy techniques and describe the potential complications associated with each approach. According to our results, although high-grade spine osteotomies at the cervicothoracic junction are associated with a high complication rate, successful execution of these procedures results in significant corrective outcomes. Several deficiencies regarding the quality of the analyzed studies should be noted, ranging from inherently difficult factors to address based on the type of pathology and surgical morbidity (such as a lack of prospective and well-controlled studies) to even relatively simple factors, such as the utilization of inconsistent radiological parameters and outcome measures. Nevertheless, the following observations were able to be derived from the available data.
C2-C7 Cervical Lordosis (CL) Correction
Historically, the cervical C2-C7 Cobb angle was considered abnormal when it was in kyphosis.19,20 However, it has been proven that this angle may be kyphotic in up to 35 % of asymptomatic individuals. 21 Staub et al 22 demonstrated that the ideal TS-CL is around 16.5° ± 2°, suggesting that individuals with a TS <16.5° may physiologically exhibit a kyphotic cervical alignment. Previous studies show a correlation between CL and health-related quality-of-life (HRQOL) measures. Iyer et al conducted a study on 90 preoperative patients referred to a cervical spine clinic for surgery. The study found that an increased C2-C7 Cobbs was associated with higher disability, as measured by the Neck Disability Index (NDI). 23
Our findings indicate that osteotomies performed in the cervical region result in greater CL correction than the upper thoracic osteotomies. This is due to the direct effect of cervical osteotomy on CL, while the upper thoracic osteotomy has an indirect effect. PSO provides the greatest correction among cervical osteotomies, and ACO offers better correction than SPO. This can be explained by simple trigonometry and the fact that cervical discs are usually collapsed in degenerative deformity. This knowledge has been inherent to the spine deformity community for years and is reflected in increasing grade of the Ames-ISSG classification of cervical osteotomies. 11
C2-C7 SVA (cSVA) Correction
cSVA is a measure of the global cervical subaxial alignment compounded by the alignment of the base of the cervical spine (T1 slope), itself influenced by myriad factors such as spinopelvic alignment, neuromuscular ability to retrovert the pelvis among others. From a biomechanical perspective, an increased cSVA leads to a greater forward bending force on the cervical spine. As a result, this increased force requires higher muscle energy expenditure to maintain an upright head posture and horizontal gaze. 24 Over time, this may lead to muscle fatigue, pain, and potential disability. Importantly, several studies have found direct correlations between cSVA measurements and patients’ scores on HRQOL measures. Previous studies have shown that cSVA is correlated with the Neck Disability Index (NDI), SF-36 physical component scores, 25 and modified Japanese Orthopedic Association (mJOA) scores. 26 Tang et al 27 found a threshold of 40 mm for moderate disability, with a cSVA greater than 40 mm being indicative of cervical sagittal imbalance (CSI). 28 Our results show that PSO, whether in the lower cervical or upper thoracic region, achieves superior cSVA correction compared to ACO and SPO. Given that improved cSVA correlates with reduced muscle fatigue, lower pain, and higher HRQOL, better clinical outcomes may be expected with PSO over other osteotomy techniques. This may rationalize the necessity of performing PSO despite its relatively high complication rate. Mirroring this issue in the lumbar spine, cho et al 29 have shown that PSO improves the SVA better than SPO after the same correction angle.
T1 Slope (TS) Correction
The T1 vertebra, similar to the pelvis in the thoracolumbar spine, is a relatively immobile segment of the spine. Its orientation is influenced by thoracic kyphosis (TK) and the thoracic inlet angle. Due to these factors, there is growing evidence to suggest that the orientation of T1 may play a crucial role in regulating cervical alignment. 30 It has been proposed that the balance between TS-CL mirrors the relationship between pelvic incidence minus lumbar lordosis in defining deformities of their respective spinal regions. 31 TS increases as thoracic kyphosis increases; if the TS exceeds 32°, one should consider the presence of the thoracolumbar spine sagittal imbalance. 32
Our findings indicate that UT osteotomy offers superior correction for TS compared to cervical osteotomy. Osteotomy at or below T1 directly decreases TS, whereas osteotomy above T1 has limited power to correct TS indirectly. Furthermore, our results demonstrate that performing an SPO in the lower cervical spine increases TS, primarily because most cervical SPO procedures are conducted at the C7-T1 intervertebral level, leading to a simultaneous increase in CL and TS.
CBVA Correction
CBVA is a critical angle to consider in patients with a spine fused from the occiput to the lower cervical spine. If the cervical deformity is not fixed, CBVA has less significance as compensatory changes will occur in the cervical spine after corrective osteotomy because the upper cervical segments (OC2) can compensate for the changes in subaxial cervical spine alignment caused by fusion. 33 However, when the patient’s cervical spine has been fused surgically or by ankylosing spondylitis (AS) or diffuse idiopathic skeletal hyperostosis (DISH), measuring the preoperative CBVA is critical.
As demonstrated in Table 3, the upper thoracic osteotomies result in better CBVA correction compared to other techniques. Performing an osteotomy at a more caudal level in the spinal column provides an opportunity for even greater CBVA correction. This finding might be attributed to the following factors: As we move caudally, the pedicle size and vertebral body height increase, providing more space for wedge resection and greater correction.34,35 In addition, performing the osteotomy at a more caudal level allows for the use of segments between the osteotomy and UIV to perform low-grade osteotomies (such as Ponte osteotomy), enabling additional correction through compression across these levels.36,37
Iyer et al analyzed 120 asymptomatic adults and reported a mean CBVA of −1.7°. 21 Lafage et al found a CBVA between −4.7 and +17.7° correlated with the lowest Oswestry Disability Index (ODI). 38 A recent study by Song et al 39 concluded that optimal CBVA for Ankylosing spondylitis patients is + 10° to +20°. We should avoid overcorrecting the deformity and aim for a balance where patients can look straight ahead when standing and walking but still be able to work at a desk or drive a car. Simmons et al used to aim for full correction with a 0° CBVA. They have revised this to approximately +10°, providing the ability to see the ground while walking and maintain overall functionality. 40
TS-CL as a Key for CTJK Correction
Literature shows that cSVA and TS-CL (T1 slope minus Cervical Lordosis) are closely associated with patient-reported outcome measures. Studies have also shown that in patients undergoing multilevel posterior cervical fusion, a TS–CL mismatch greater than 22.2° corresponds to severe disability, along with a cSVA greater than 4.35 cm. 41 Staub et al 22 demonstrated that the ideal TS-CL is around 16.5° ± 2°. Protopsaltis et al 31 determined that a TS-CL exceeding 17°, even with an underlying thoracolumbar deformity, indicates CSI.
Changes in TS-CL are strongly correlated with changes in cSVA, meaning correcting the TS-CL will automatically improve cSVA. 42 Additionally, a high T1 slope is associated with increased CVBA and cSVA. These findings suggest that optimal correction of CSI should involve not only an increase in CL but also a reduction in TS.33,43 Therefore, in cases of CSI, either side of the TS-CL equation can be manipulated to reduce the disparity. This forms the foundation for 2 corrective options for cervical sagittal alignment: decreasing the TS with upper thoracic osteotomy or increasing the CL with lower cervical osteotomy. It is also intuitive that performing osteotomy at the apex of the deformity allows for the maximum possible correction. Occasionally, spinal osteotomy outside the deformity may be warranted for the following reasons: (1) to achieve a safer correction at a level where the spinal canal is wider or at a more caudal level to preserve upper spinal cord function; (2) to achieve a greater correction angle with the same amount of bone resection. Upper thoracic osteotomy is a powerful and relatively safer option compared to lower cervical osteotomy for addressing CSI. It is important to note that the upper thoracic osteotomy is not suitable for all cases of CSI, and there are following specific situations where this technique can be used for correction: (1) The main driver of cervical imbalance is located in the upper thoracic region: This can occur, for example, in patients with cervical deformity combined with upper thoracic proximal junctional kyphosis following thoracolumbar fusion. (2) Cervicothoracic junction kyphosis is rigid: this can happen, for example, in patients with Ankylosing Spondylitis, DISH patients, or patients with previous cervical fusion who develop distal junctional kyphosis. However, in the case of flexible or semi-rigid primary cervical kyphosis or focal primary cervical kyphosis with myelopathy or cord compression, the upper thoracic osteotomy cannot be used.
Complications of Different Osteotomy Types
Our findings suggest that the overall complications of PSO are lower than those of SPO (Ames-ISSG grade 5). The main complications of SPO include the risk of translation during the correction,44,45 osteoclasis at the undesired level, 46 lengthening of the mediastinal organs (such as the esophagus and trachea) leading to dysphagia and vascular injury, and the risk of non-union due to the anterior gap between vertebral body endplates. 2 PSO reduces the risk of unwanted translation, eliminates the need for osteoclasis, 47 provides bone-to-bone contact that reduces non-union risk, 48 and shortens the posterior column without lengthening the anterior column. 49 However, SPO is associated with lower blood loss than PSO, likely due to the more extensive bone resection required by PSO, especially in the highly vascular vertebral body. Our findings showed that the duration of the surgery is not significantly different between PSO and SPO.
The anterior cervical osteotomy (ACO) procedure has lower blood loss and shorter surgery duration. The analyzed articles indicated zero overall and neurological complication rates for ACO, possibly due to factors such as the supine position, reduced blood loss, and the approach to the spinal column from the anterior direction, allowing for spinal cord decompression before correction. However, it’s worth noting that the included papers are retrospective, and there may be some selection bias for performing ACO in patients with better overall health conditions. Additionally, this type of osteotomy has limited indications in cervical deformity surgery, particularly in cervicothoracic kyphosis, due to challenges in accessing the spine from the anterior approach. Another disadvantage of ACO is the limited power to correct the cSVA.
Complication Risk Factors and Complication Avoidance Strategies
Medical Complications
DePasse et al 18 found that in patients undergoing cervical osteotomy surgery, the overall non-neurological complication rate was 15.8%. The most frequent complications included transfusion (78%), readmission (45%), and reoperation (32%). Identified risk factors for non-neurological complications, including increased age, American Society of Anesthesiologists classification III and IV, and increased operative duration.
Surgical Complications
In a retrospective cohort study, Lau et al 51 found that the complication rate was 49.0%, and the rate of new neurological deficits was 17.9%. They also observed significantly higher rates of neurological deficits at the C7 and T1 osteotomy levels: C7 (37.5%), T1 (44.4%), T2 (16.7%), T3 (14.3%), and T4 (0.0%; P = .042). Lau et al 52 identified independent risk factors for surgical complications, which encompassed male sex, cSVA >8 cm, and kyphosis >20.
Mechanical Complication
In the study by Lau et al, 50 posterior-based osteotomies carried a high rate of mechanical complications (MC), around 30%. The most common MCs were distal junction kyphosis (DJK), while pseudarthrosis occurred at a rate of 10.8% and implant failures at 16.9%. The study identified preoperative cervical scoliosis >5° and BMI (>30) as MC risk factors.
Neurological Complication
The C8 and T1 roots are particularly susceptible during posterior osteotomy at the lower cervical and T1 levels. The nerve root is at risk during the osteotomy, its closure (due to direct compression of surrounding structures such as the T1 rib head), and following correction (due to potential stretching and nerve damage, known as neuropraxia). Hand dysfunction can be disabling; according to Lau et al, 51 only one-third of patients return to their previous function. Surgeons must minimize injury risk and maximize recovery. Counseling about the risk of hand weakness following surgery is important, with a 20% risk at 1 year and 22% at 2 years.40,50,52,53 Considering the function of the C7, C8, and T1 nerves near the osteotomy site. Performing osteotomy at the C7 and T1 levels may risk these nerves. It may be safer to consider osteotomy at the T2 and T3 vertebral levels. 54
Limitations
The incidence of CTJ kyphosis is relatively low, and there is a diverse range of evidence regarding its treatment and surgical approaches with varied methodologies. Combining these results with our meta-analysis may introduce a risk of bias. Our primary aim was to conduct a literature review to analyze outcomes, identify strategies to maximize correction while minimizing complications and thus establish a basis for surgical decision-making. Due to the non-comparative design of the previous studies, we are unable to directly compare different osteotomy types and levels. Our meta-analysis aimed to estimate the mean of continuous variables across studies rather than performing direct group comparisons. Given this analytical approach, which prioritized data aggregation to determine central tendencies (i.e., means) rather than hypothesis testing or effect size comparisons, statistical significance (P-values) was not calculated or reported. Since P-values are primarily used for hypothesis testing or comparative analyses, which were beyond the scope of our study, their inclusion would not have been appropriate. Instead, our approach provides a more accurate and unbiased representation of overall trends in the data, minimizing the risk of misinterpretation from improper statistical comparisons
Conclusion
Cervicothoracic junction kyphosis significantly affects the quality of life of patients, especially those with ankylosing spondylitis. The distinct anatomical features of the CT junction require special considerations for surgical interventions. To offer evidence for surgical decision-making, we have compared the corrective ability and complications of various surgical approaches based on the level and type of osteotomy and hope it can provide assistance to surgeons planning these difficulty corrections.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.