Abstract
Study Design
Cross-sectional survey.
Objective
We explore the demographic factors amongst surgeons responsible for decision-making in the management of Grade I L4-5 degenerative lumbar spondylolisthesis(DLS).
Methods
A survey presenting three clinical scenarios of DLS with varying degrees of neurological compression and instability was distributed to the AOSpine members globally to ascertain surgical management preferences. Management options such as decompression only or decompression and fusion and the techniques that would be employed were presented to the responders.
Results
After dissemination, 479 surgeons responded to the survey. Direct decompression was preferred for all three scenarios with and without neurologic deficits(82.5, 81.2, and 56.8%), with the majority favoring open procedures over minimally invasive or endoscopic procedures. Notably, younger, less experienced, and fellowship-trained surgeons showed a higher inclination toward minimally invasive and indirect decompression methods. A strong preference for surgical fusion over decompression(75.2, 92.5 and 86.6%, respectively) was also significantly observed, reflecting a general consensus on the need to achieve segmental stability.
Conclusion
The results of this study demonstrate a pronounced preference for direct decompression and fusion among a group of global surgeons when treating L4-5 Grade I DLS across all demographics. This indicates a consensus on achieving decompression and stability; however, there are some trends indicating the impact of surgical management based on age, experience, and training of the treating providers. These findings suggest an evolution of surgical interventions toward less invasive techniques, particularly among younger surgeons, highlighting the need for global education to adopt innovative approaches in the management of DLS.
Introduction
Degenerative lumbar spondylolisthesis (DLS) is characterized by subluxation of one vertebral body with respect to the adjacent vertebra due to arthritic changes of the disc and facets, which can lead to mechanical low back pain and/or radicular leg symptoms. 1 DLS is among the most commonly diagnosed spinal disorders and more frequently presents in females over 40-years-old and patients who are obese. 2 DLS is best classified radiographically by the Meyerding Classification, which grades the severity of disease based on the amount of anterior displacement. 3 DLS typically occurs at the L4-5 level, with Grade I slippage being the most common. Due to its high prevalence and respective burden on quality of life, the financial implications of L4-5 Grade I DLS are substantial, including direct costs associated with surgical and non-surgical treatments, as well as indirect costs related to lost productivity and ongoing patient care. 4
While continually evolving, the surgical management of L4-5 Grade I DLS aims to achieve decompression of the neural elements or fusion of the motion segment, or both. 5 Spinal fusion is generally considered in patients with excessive motion or malalignment, while decompression surgery, which does not address the vertebral slip, is considered with evidence of mechanical neural impingement. When fusion is indicated, there are a variety of techniques that may be utilized, such as posterolateral fusion, anterior lumbar interbody fusion (ALIF), lateral lumbar interbody fusion (LLIF), posterior lumbar interbody fusion (PLIF), etc. Additionally, novel surgical methodologies of endoscopic and minimally invasive surgery (MIS) have expanded the available treatment options beyond traditional open procedures for Grade I DLS. 6
While the literature remains controversial about the treatment choice to add fusion to the decompression surgery for DLS,7,8 recent studies have found non-fusion to be non-inferior to the fusion counterparts leaving the choice in the hands of the surgeons. 9 The surgeon’s preferred treatment for L4-5 Grade I DLS stems from several factors such as the clinical and radiographic presentation of the patient, surgeon’s training and experience, and the cost implications of different techniques.10,11 By using a global survey of AOSpine surgeons, this study aims to identify surgeon’s relevant sociodemographic parameters, including training and experience, that impact their practice patterns for the management of L4-5 Grade I DLS. By understanding these practices and the underlying factors, the study aims to highlight trends, knowledge gaps, and potential areas for further research to optimise patient outcomes in the context of this prevalent spinal condition.
Methods
Survey Design
A survey was designed by the AOSpine Knowledge Forum Degenerative and disseminated through to the AO Spine members worldside to understand the preferences of surgeons regarding the surgical management of L4-5 Grade I DLS. Three clinical scenarios with varying degrees of neurological compression and instability were presented with corresponding radiological images to understand their management preference. Complete illustrated details of the cases are given in Annexure 1.
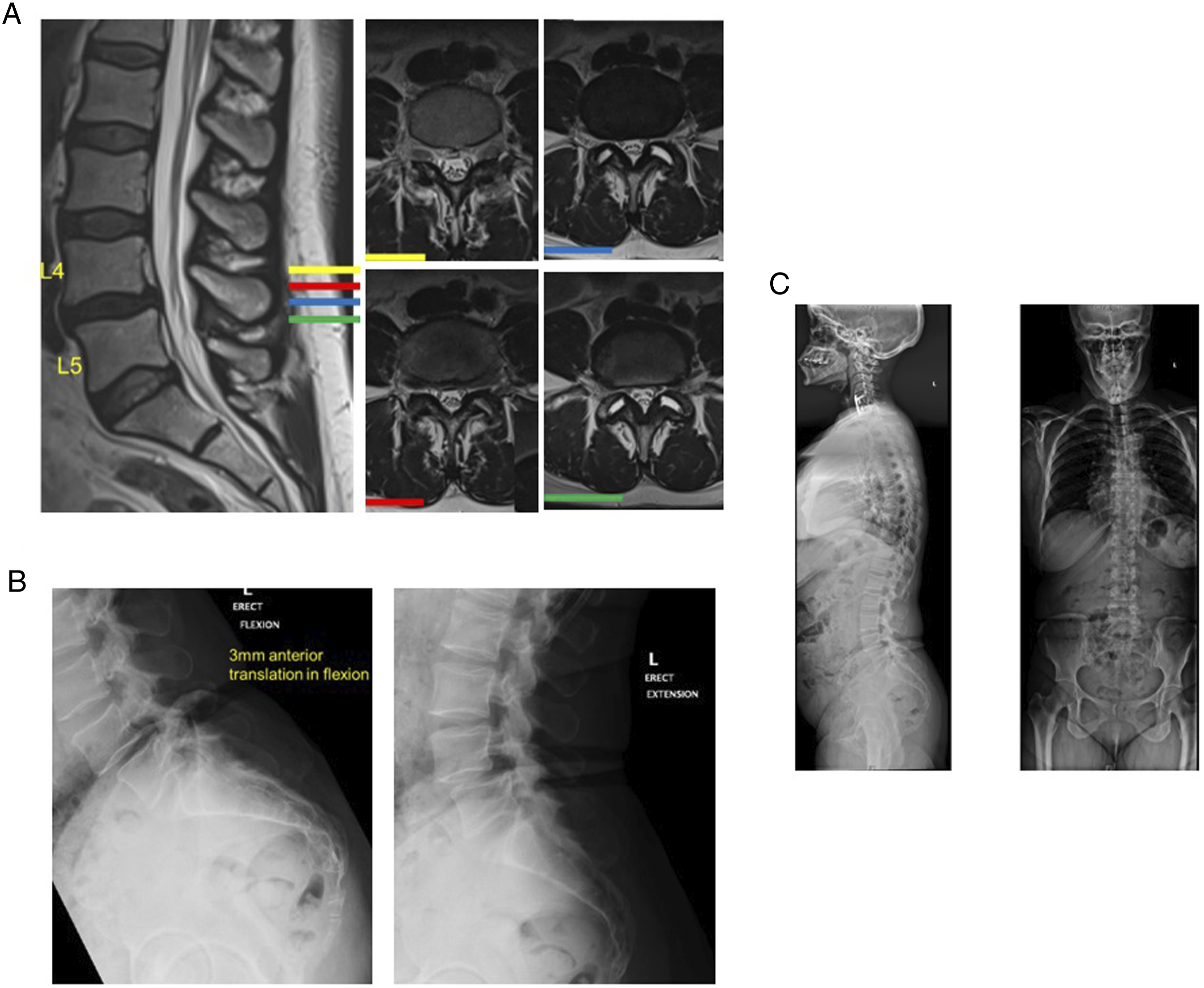
In brief, the first case describes a 73-year-old male with grade I L4-5 DLS with severe central stenosis, minimal translation on dynamic radiographs, and without neurological deficit as shown in Figure 1. The patient had radiculopathy and neurogenic claudication as the presenting symptoms. The second case features a 48-year-old female with grade I L4-5 DLS with severe central stenosis and significant translation on dynamic radiographs as shown in Figure 2. This patient had no neurological deficit with back pain as the presenting symptoms. The third case showcased a 64-year-old female with grade I L4-5 DLS without canal stenosis with demonstrable movement on dynamic radiographs with neurological deficit such as radiculopathy and neurogenic claudication as the presenting symptoms as shown in Figure 3.
Surgeons operating on adult patients with lumbar degenerative pathologies were eligible to participate in the survey. Informed consent was not required since no specific patient data was involved in the survey and ethical committee approval was not obtained given the study was a surgeon-based survey.
The survey was distributed to the AOSpine members internationally and was conducted electronically in March 2022. Surgeon demographic information was collected including geographic region (Asia Pacific, North America, Latin America, Europe and Southern Africa, and Middle East and Northern Africa), gender, age, years of practice, speciality, case volume, and practice setting. Surgeons were asked about their management preference between the choice of decompression - either direct or indirect - and the particular technique utilized for each case scenario presented. They were also asked regarding their preference for stabilization with or without fusion
We used percentages to represent the categorical data and used the chi-squared test or fisher-exact test to analyse the difference in the management among cases presented and among the surgeons for a given case scenario for the demographic variables analysed. A P-value less than 0.05 was considered significant. Statistical analysis was performed using SPSS version 25 (IBM Corp., Armonk, USA). We included for analysis only those respondents who gave a clear and complete management of choice of their decompression either direct/indirect and their choice of stabilization and fusion for particular case.
Results
Survey Demographics
A total of 479 surgeons responded to the survey on the management of presented scenarios of L4-5 DLS. The respondents formed an international cohort, with the largest group from Europe and Southern Africa (33.4%), followed by Asia Pacific (30.9%), Latin America (16.3%), Middle East and Northern Africa (10.9%), and North America (8.6%). The majority of the respondents were orthopedic surgeons (62%) affiliated with an academic/university hospital (39.9%). On the other hand, 25.3% of surgeons were affiliated with public/military hospitals, and 32.4% were in private practice. Finally, surgeon experiences among the respondents varied widely, and they were equally distributed across five groups ranging from <5 years of experience to >20 years of experience. More than 55.3% of the respondents completed a spine surgery fellowship after residency. Neurosurgeons represented 38% of the survey participants.
Case 1: DLS with Severe Central Stenosis
Approximately 87.1% of the surgeons opted for direct decompression while 12.9% of the surgeons opted for indirect decompression. Among direct decompression methods, open procedures were adopted by 67.6% of the respondents, while MIS and endoscopic decompression were preferred by 27.4% and 5.08% of the surgeons, respectively. Although we observed neurosurgeons significantly preferred MIS decompression over orthopaedic surgeons in this scenario (P = 0.02), there was no significant difference in the choice of direct decompression method in the management based on the region, age, experience, practice setting, training, or caseload of the surgeons.
Regarding the choice of indirect decompression choice of the respondents, early career surgeons with <10 years of experience and age <45 years with a caseload less than 25/year chose indirect decompression significantly more than senior surgeons with >10 years of experience with age >45 operating >25 cases/year (P = 0.001). However, there was no difference between the respondents based on the region, training, speciality, or practice setting.
Summary of Demographic Profile of surgeons With Their Decompression and fusion Preferences for Case 1.
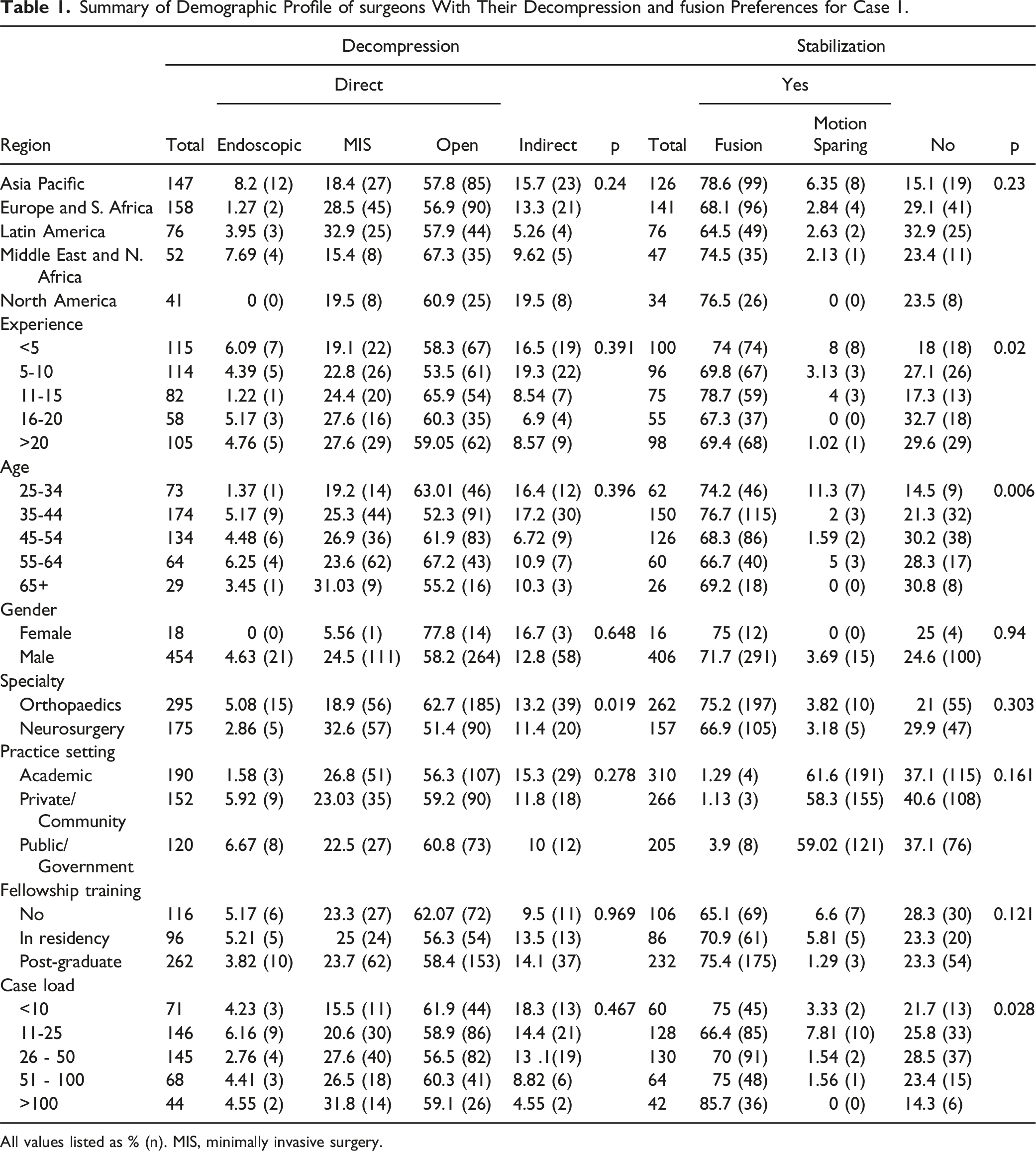
All values listed as % (n). MIS, minimally invasive surgery.
Case 2: DLS with Central Stenosis and Significant Translation
For this case, 82.7% of the surgeons opted for direct decompression while 17.3% of the surgeons opted for indirect decompression. Among direct decompression methods, open procedures were adopted by 58.6% of the respondents while MIS and endoscopic decompression were preferred by 19.9% and 4.23% of surgeons, respectively. Although neurosurgeons significantly preferred MIS decompression over orthopaedic surgeons in this scenario (P = 0.03), there were no significant difference in the choice of direct decompression method in the management based on the region, age, experience, practice setting, training, or caseload of the surgeons.
Concerning the indirect decompression choice of the respondents, surgeons with fellowship training and neurosurgery speciality chose indirect decompression significantly more than the surgeons without spine fellowship and orthopaedic speciality (P = 0.02). However, there was no difference between the respondents based on the region, age, experience, practice setting, or caseload of surgeons.
Summary of Demographic Profile of surgeons With Their Decompression and fusion Preferences for Case 2.
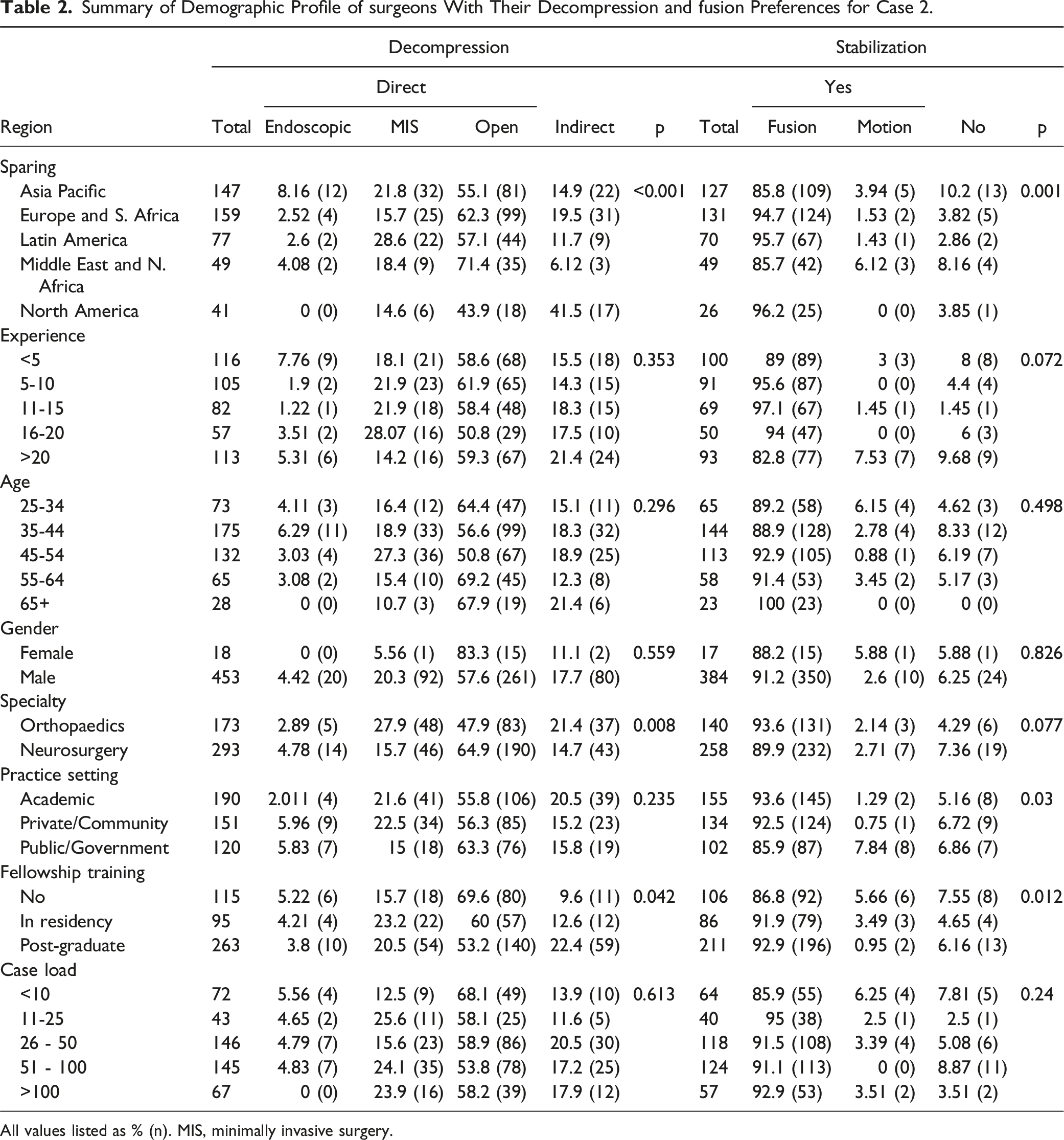
All values listed as % (n). MIS, minimally invasive surgery.
Case 3: DLS without Canal Stenosis
About 55.1% of surgeons opted for direct decompression while 44.9% of surgeons opted for indirect decompression. Among the direct decompression methods, open procedures were adopted by 59.3% of the respondents while MIS and endoscopic decompression were preferred by 33.3% and 7.36% of the surgeons, respectively. Regarding the endoscopic approach, early career surgeons with <10 years of experience, <45 years of age who operate <25 cases DLS cases per year significantly utilized this method compared to senior surgeons >45 years of age with >10 years of experience operating >25 cases a year (P = 0.04).
Concerning indirect decompression technique, early career surgeons with age <35 years with less than <5 years of experience showed significantly reduced utilization of indirect decompression than the senior surgeons with age >35 years and >5 years of experience (P = 0.002). However, there was not any difference between respondents based on their region, training, speciality, or practice setting.
Summary of Demographic Profile of surgeons With Their Decompression and fusion Preferences for Case 3.
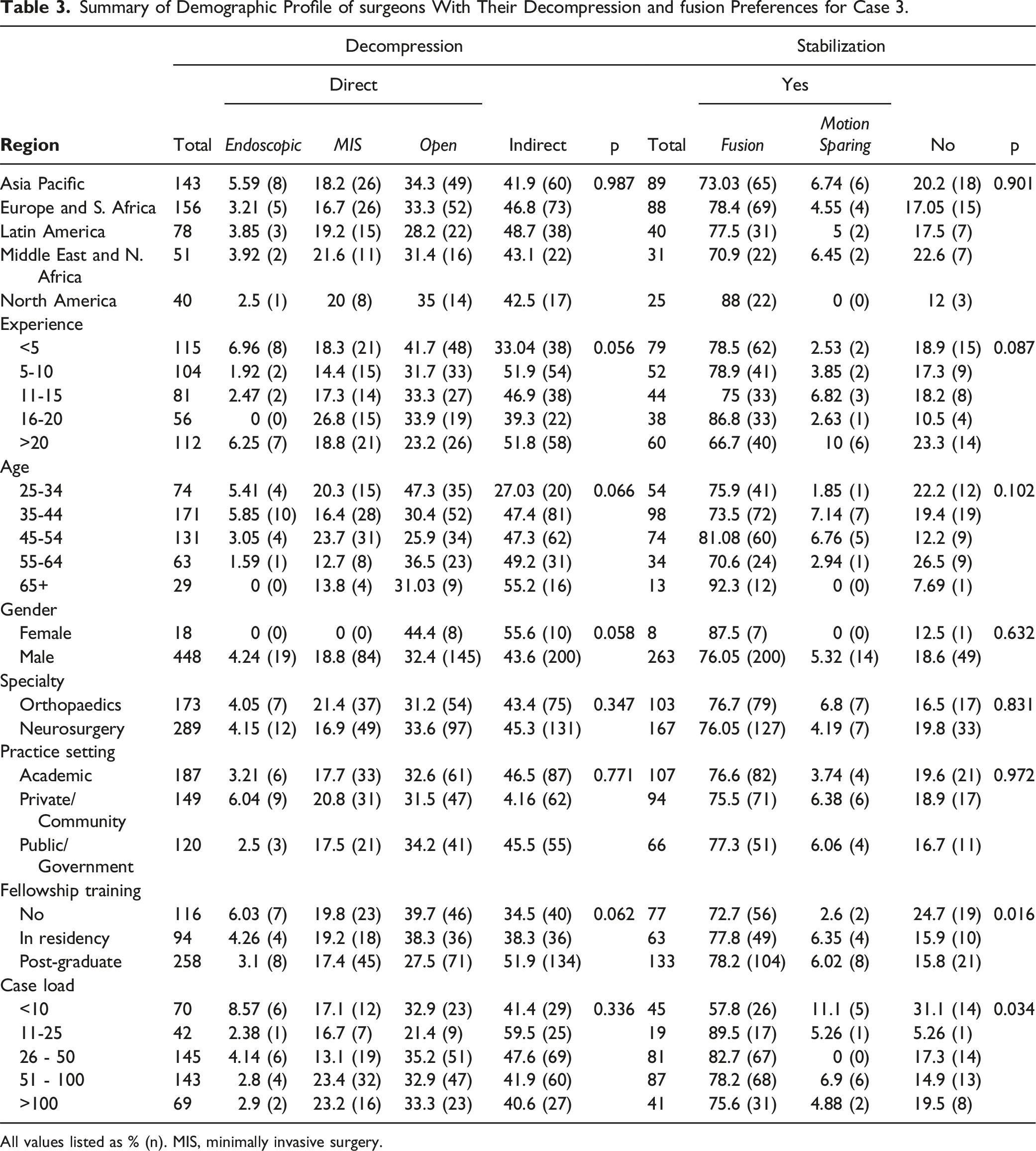
All values listed as % (n). MIS, minimally invasive surgery.
Discussion
Discrepancy exists in the literature on the ideal treatment recommendation in the management of DLS especially on the choice to add fusion to the decompression surgery.7,8 However, recent evidence point towards the non-inferiority of decompression-only surgeries compared to their fusion counterparts leaving the choice in the hands of the surgeons. 9 This study highlights the variability in the surgical management of L4-5 Grade I DLS, underscoring the influence of surgeon-specific factors from responses of AOSpine members. While previous studies have explored variations specific to certain geographic regions,12-15 this is the first international study to report on patterns of surgeon preference for the treatment of DLS via utilization of a global survey from a diverse international cohort, made up primarily of spine surgeons including both orthopaedic (62.9%) and neurosurgery (37%) background, with varying experience (<5 - >20 years), who work mostly in academic settings (40.9%), and coming from Europe (33.3%) and Asia Pacific (31.01%).
Review of respondent demographics most notably showed variation between regions when faced with the choice between decompression alone or decompression and fusion. Surgeons in the Asia Pacific region were more likely to opt for fusion for the given scenarios. This preference reflects a regional emphasis on surgical techniques and the need for universal standardized treatment approaches. 16 Asian spine surgeons have widely adopted MIS and endoscopic surgery (ES) techniques with higher proficiency than their counterparts elsewhere. 17 Additionally, the integration of MIS and ES training into the core curriculum of established programs in Asia, coupled with fewer concerns about equipment costs, institutional obstacles, and insurance hurdles, facilitates the preference for fusion surgeries, that is considered more definitive and beneficial for patients. 17 However, most of the Asian respondents still opted for open fusion rather than MIS or endoscopic fusions for the given scenarios. Additionally, the low adoption of MIS among North American surgeons could also be attributed to variations in the built environment and profile of patients that influence their surgical choice.
Experience and age also influenced these decisions, with less experienced and younger surgeons favoring less invasive strategies like indirect decompression and motion-sparing techniques. On the contrary, those with more than 10 years of experience or older than 45, showed preference for more traditional approaches, such as direct decompression and fusion. Firstly, these results are supported by prior literature, which has established a significantly higher association with improved health outcomes and surgeon operative volumes.18-20 Secondly, another reason for the preference for fusion surgeries is their association with academic practices (majority of respondents of this study were academic surgeons), as these surgeons frequently work at hospitals that are tertiary referral centers. Patients at these centers may have a higher likelihood of completing a full course of conservative care or being diagnosed with more complex spine disorders (e.g., tumor, infection, trauma, scoliosis, and complex deformity), for which fusion may be more appropriate. 21 On the other hand, the noted preference could be due to the training of the senior surgeons in open fusion procedures resulting in a preferential practice choice compared to other non-fusion techniques or the lack of exposure of complications from non-fusion procedures in younger surgeons making them to opt the same for the given cases.
Beyond background, results demonstrated that specialized training in spine surgery through fellowships also influences the adoption of advanced techniques, such as MIS and endoscopic approaches. Additionally, training differences between neurosurgery and orthopaedics were observed, with neurosurgeons showing a higher preference for MIS. A recent study by Shetty et al., which evaluated 90 surgeons at two centers, found large variations in the management of DLS, noting that these variations led to short-term outcomes, including lower readmission rates among fellowship-trained surgeons. 22 Furthermore, neurosurgeons, who generally log more decompressive surgeries during residency, show a higher preference for less invasive procedures compared to orthopedic surgeons, who often handle more spine deformity cases and favor fusion surgeries. 23 This may also account for the observation of a strong preference for fusion in treating all three cases, which also reflects a majority of orthopedic respondents in the present survey. Thus, differences in training, especially when considering the regional impacts of surgical education and resources, are important considerations for the need of evidence-based guidelines to help standardize care and reduce disparities, where possible.
This study has several limitations. First, it is descriptive in nature and cannot definitely provide any insight into causality. Second, since the survey was voluntary, a degree of response bias may also be expected. Importantly, the response rate was low among AOSpine surgeons, which may introduce sampling bias and limit the generalizability of our findings. Furthermore, the survey was only distributed to members of AOSpine, which may not be entirely representative of all spine surgeons including neurosurgeons. We also analysed the respondent variables whose data are complete for their choice of decompression and stabilization or fusion for a given case. The strengths of this study lie in the AOSpine membership group, which represents a truly global spine surgeon community, large sample size, and detailed case presentations for surgical decision-making. This study is also novel in recruiting a large number of both orthopedic and neurosurgeons, aiming to explore practice patterns related to spine surgery. Finally, we did not analyze the financial factors such as incentives and reimbursements that might affect the surgical decisions made by the surgeons.
Conclusion
The findings of this study present a pronounced preference for direct decompression and fusion when treating L4-5 Grade I DLS, reflecting a consensus on achieving decompression and stability. However, significant trends based on age, experience, and specialized training influence the adoption of MIS and endoscopic approaches. Younger and fellowship-trained surgeons, particularly neurosurgeons, show a higher inclination toward less invasive methods, while more experienced surgeons tend to favor traditional approaches. The regional differences, particularly the higher propensity for fusion surgeries among Asia Pacific surgeons, highlight the impact of local training, research contributions, and systemic factors on surgical decisions. There is a need for global education to adapt innovative approaches and evidence-based guidelines to standardize care and reduce disparities in spine surgery practices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine degeneration experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department.
Appendix
Case 1 showing MRI (A), CT (B), dynamic X-ray (C), and standing films (D) evidence of L4-L5 grade I DLS with central stenosis, left-sided cyst, no segmental instability and normal spinopelvic balance.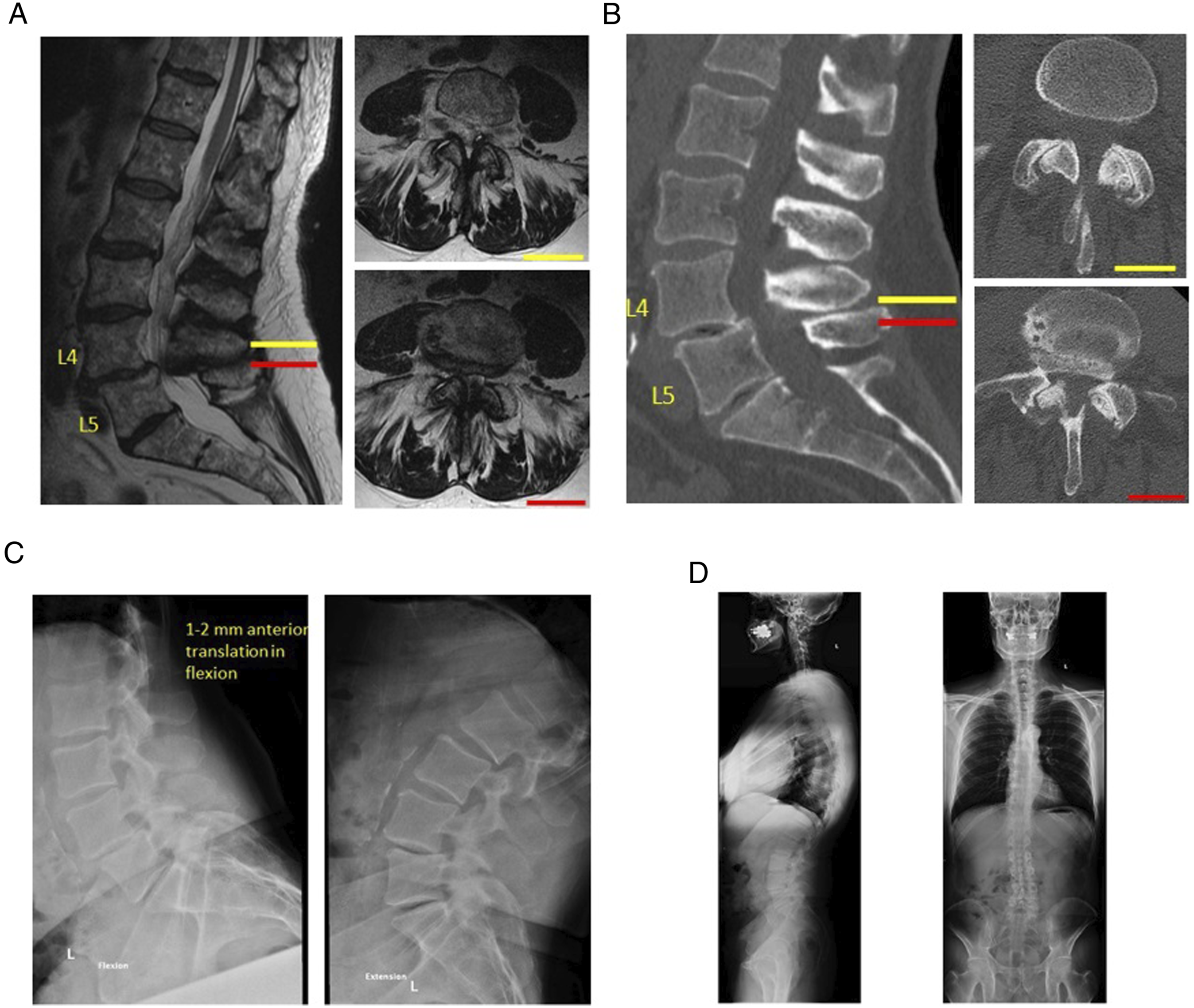
Case 2 showing MRI (A), CT (B), dynamic X-ray (C), and standing films (D) evidence of L4-L5 grade I DLS with bilateral foraminal stenosis, significant segmental instability and normal spinopelvic balance.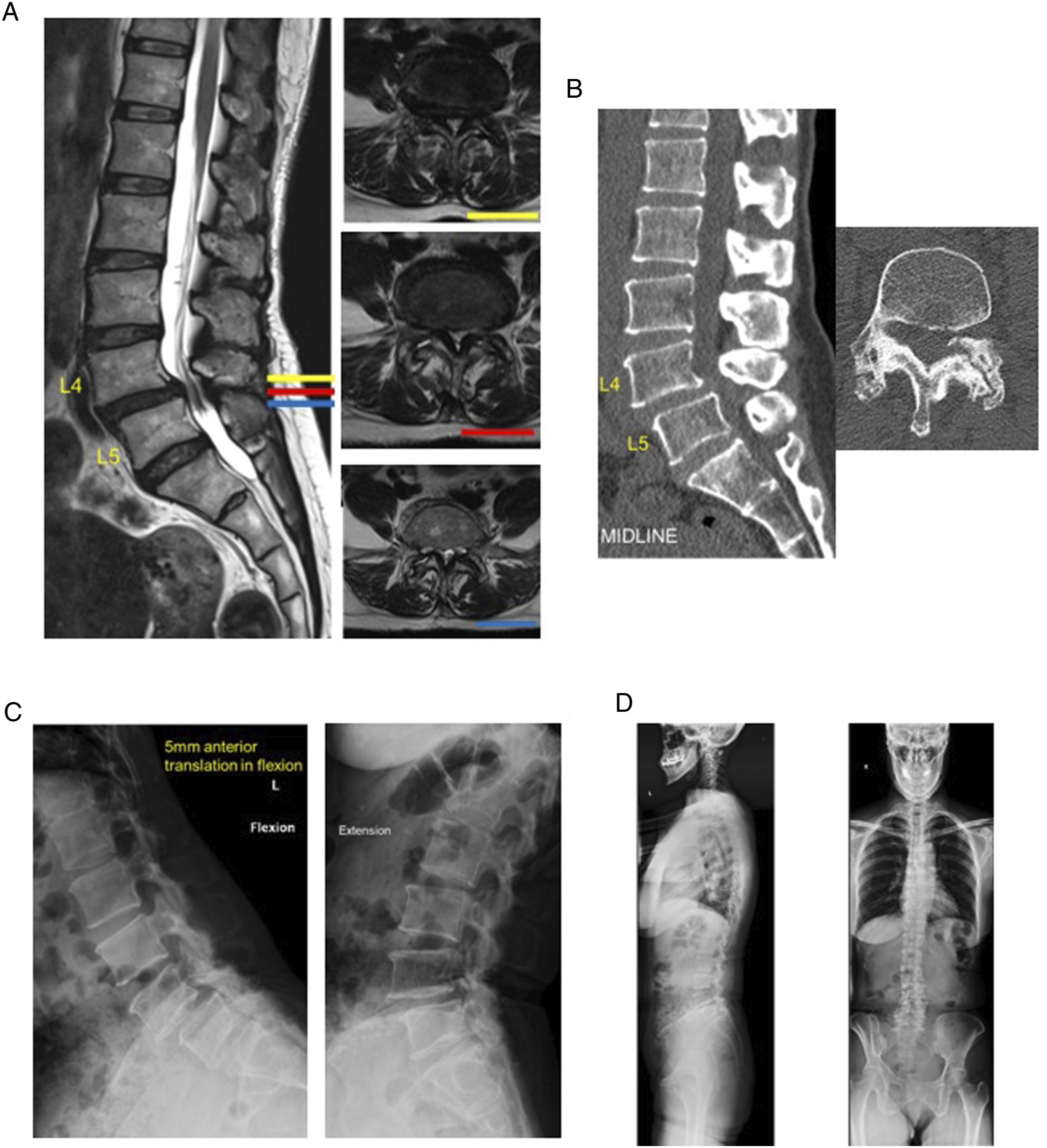
Case 3 showing MRI (A), dynamic X-ray (B), and standing films (C) evidence of L4-L5 grade I DLS with right foraminal stenosis and facet joint effusion, moderate segmental instability and normal spinopelvic balance.