
Abstract
Study Design
Retrospective Cohort Study.
Objective
Lateral lumbar interbody fusion (LLIF) is a treatment option for correcting lumbar degenerative pathologies that uses a retroperitoneal, transpsoas corridor to the disc space. Conventional teaching of the LLIF technique has been to perform the procedure ‘as efficiently as possible', with a goal of keeping the total retractor time to less than 20 minutes to prevent injuries. This study aims to examine the sensitivity of the “20-minute” rule for predicting postoperative femoral nerve palsy.
Methods
A multicenter, retrospective cohort of patients who underwent an LLIF was established. Retractor time was recorded and compared to postoperative motor exams for its relationship to motor injury.
Results
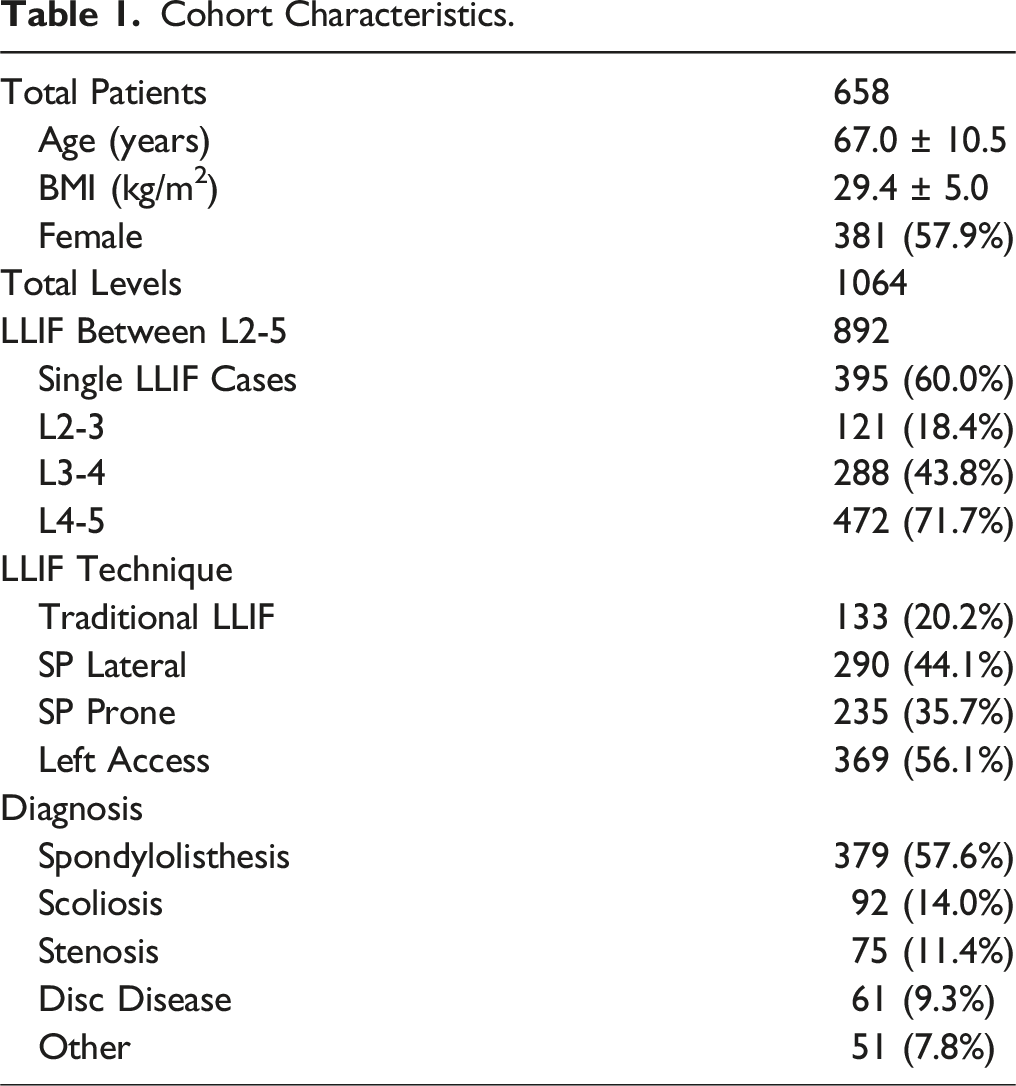
658 total patients were included in the study. The most frequently operated level was L4-5 (71.7%). The average retractor time was 17.5 ± 8.0 minutes. The injury rate of the cohort was 1.8% (12/658). There was no difference in average retractor time for non-injured vs injured patients (17.5 ± 8.0 min vs 19.6 ± 11.2 min, P = 0.367). Analysis of the “20-minute” rule for LLIF revealed a sensitivity of 50%, a specificity of 73.8%, and a positive predictive value of 3.4%. There were 174 patients with retractor times >20 minutes and six injuries, yielding a false positive rate of 96.6%.
Conclusion
Post-operative quadriceps motor palsy after lateral lumbar interbody fusion does not appear to be caused by prolonged retractor time greater than 20 minutes. The authors recommend surgical efficiency without the need to rush through the procedure because the “20-Minute” threshold is approaching. Limiting retractor time to under 20 minutes was a poor predictor of post-operative quadriceps injury.
Introduction
Lateral lumbar interbody fusion (LLIF) is a technique for correcting lumbar degenerative pathologies through a retroperitoneal, transpsoas corridor to the lumbar spine.1-5 This approach gains access to the disc space by splitting the psoas muscle, which can result in transient hip flexor weakness in up to 54.9% of cases.3-6 The lumbar plexus directly traverses through the psoas muscle, and the proximity of the lumbar plexus to the LLIF working corridor has led to apprehension to adoption among surgeons. This concern is greater when operating at the caudal segments of the lumbar spine, as the femoral nerve traverses most anterior at the L4-5 disc space. Prior studies have demonstrated a higher injury rate in constructs including L4-5.7-10 A recent meta-analysis of the transpsoas approach revealed permanent motor neurologic weakness in 2.8% of patients, with individual studies reporting rates as high as 15%.3,11
Since the introduction of the LLIF technique, many studies have examined these injuries and worked to develop methods and techniques to reduce them. Cadaveric studies have assessed the distal lumbar segments and outlined safe anatomical zones for docking, while other studies have evaluated the impact of patient positioning on the location of the nerves and lumbar plexus.12,13 More recent studies have examined the outcomes of different neuromonitoring modalities for identifying injuries intraoperatively. Directional dynamic triggered EMGs (t-EMG) have demonstrated success in identifying nerve location intraoperatively but have shown poor sensitivity alone for predicting postoperative nerve injury. 14 The studies surrounding saphenous nerve somatosensory evoked potentials (SSEP) have demonstrated promising results for identifying if an injury occurred, however neuromonitoring technicians can have some difficulty obtaining reliable signals in every patient.15-17 While helpful in identifying if an injury occurred, these modalities do not currently aid in understanding what causes the injury in each case. Several potential reasons exist, including patient selection, variability in psoas and plexus anatomy, anteriorly located psoas, poor docking technique, excessive retractor opening, traction injury from interbody placement, direct trauma from maleting the implant, and psoas retraction time – to name a few.
Several studies have noted a correlation between post-operative nerve injuries and the duration of lateral surgery. Specifically, they observed that their patients with injuries had a longer time with the retractor expanded within the psoas muscle.14-19 These studies have also found that while t-EMG alone had poor sensitivity, this sensitivity increases in patients with longer retractor times. 14 The interpretation of these results are inconsistent among surgeons but have changed the conventional teaching of the LLIF technique to emphasize performing the procedure ‘as efficiently as possible' and avoiding prolonged retraction of the nerve roots. This has led spine surgeons to focus on retractor times and has created a “dogma” centered around preventing injuries by keeping the retractor time to less than 20 minutes.19-22 In fact, experienced surgeons often quote a low retractor time as a significant factor in reducing the likelihood of an injury.
The 20-minute rule is widely followed, but its effectiveness as a predictor for neural injury remains under debate. This rule emphasizes surgical speed, and the pressure to move quickly may limit adoption of the LLIF technique, especially at L4-5. This study aims to study the rate of post-operative motor neurologic complications associated with LLIF surgery. We further seek to identify the impact of retractor times on LLIF outcomes and assess the reliability of the “20-minute rule” as a parameter related to postoperative quadriceps motor palsy.
Methods
A multi-center cohort of patients who underwent a transpsoas lateral lumbar interbody fusion of L2-3, L3-4, and/or L4-5 was retrospectively established from seven surgeons in three different countries. Due to the retrospective nature of this study, participation was deemed no more than minimal risk to the patients, and informed consent and the need for an IRB were deemed not necessary. All patients with a documented pre-, and serial post-operative physical exam and a recorded retractor time were eligible for inclusion. Patients with abnormal pre-operative quadriceps examinations were excluded. Demographic characteristics, operative details, and clinical follow-up were collected to examine the prevalence of post-operative quadriceps palsy. Since the lateral approach directly penetrates the psoas muscle, it is difficult to delineate between approach-related symptoms and true hip flexor nerve injury. For this reason, our study focused on nerve injury leading to weakness in the quadriceps muscle. Even further, to control for intra-observer differences, a true injury was described as a post-operative quadriceps strength of 3/5 or less on the Medical Research Council (MRC) Scale. 23 Typically, 4/5 strength could also qualify as motor weakness. However, 4/5 could also be due to post-operative pain, poor effort, weak examination in the bed, and/or approach-mediated weakness. A 4/5 examination could be ambiguous and not a true neuropraxia from a nerve root or plexus injury during the procedure. An exam of 3/5 or less was chosen to avoid this ambiguity, as it more closely resembles a poor outcome during a lateral procedure and correlates with a prolonged post-operative functional recovery.
Every injury was followed to assess for resolution of the palsy. Individual LLIF techniques were at the discretion of the operating surgeon, and each surgeon followed their own neuromonitoring standard protocol. If intraoperative neuromonitoring changes occurred and the case was aborted, the case was still included if the retractor was in place for some time and the post-operative examination was recorded. The use of neuromonitoring and individual neuromonitoring protocol was at the discretion of the operating surgeon. For this study, a neuromonitoring alert was categorized as a 50% reduction or 10% latency increase in somatosensory evoked potentials (SSEP), a persistent amplitude decrease or latency increase in transcranial motor evoked potentials (MEP), and a persistent amplitude increase in trans-abdominal motor action potentials (TMAP). If a neuromonitoring alert occurs, the stage of the procedure is recorded for further analysis. Retractor time was recorded from the initial insertion until the final removal.
The “20-minute rule” was analyzed as a mechanism for preventing injuries through sensitivity and specificity analysis. Alternative thresholds were also analyzed to examine if 20 minutes is the optimal threshold for this rule. For patients with multi-level LLIF procedures, the L4-5 retractor time was used to analyze injury unless neuromonitoring indicated a change during a different level. Average retractor time and total retractor time were also examined to assess if the combined retraction of the nerve root correlated with injuries. Subgroup analysis was conducted to examine the difference between injured and non-injured patients, single and multi-level cases, and operative level. Patient characteristics and operative details were recorded to examine their relationship to the injuries.
Statistical Analysis
All of the statistics were performed using IBM SPSS Statistics software (version 29.0.2.0 (20)). Categorical variables underwent univariate analysis using Fischer’s exact test and Chi-squared test. Comparisons of continuous variables were performed using an independent samples student t-test. Univariate logistic regression was used to calculate the adjusted odds ratio and 95% confidence intervals for all variables to examine the risk factors for injury. Receiver operating characteristic (ROC) curve analysis was performed to identify if there was a significant cutoff threshold for retractor time in psoas that was associated with post-operative neurologic injury. Statistical significance was defined as 0.05 for all tests.
Results
Cohort Characteristics.
Post-operative Quadriceps Motor Palsy
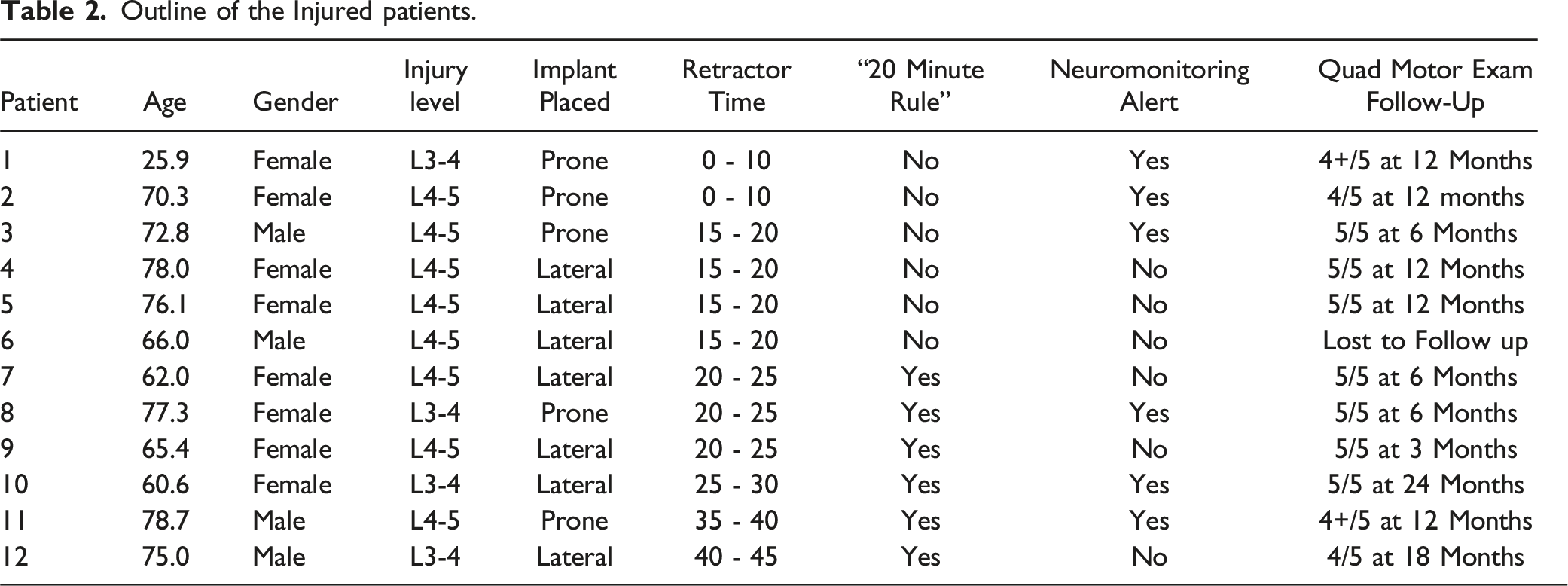
Outline of the Injured patients.
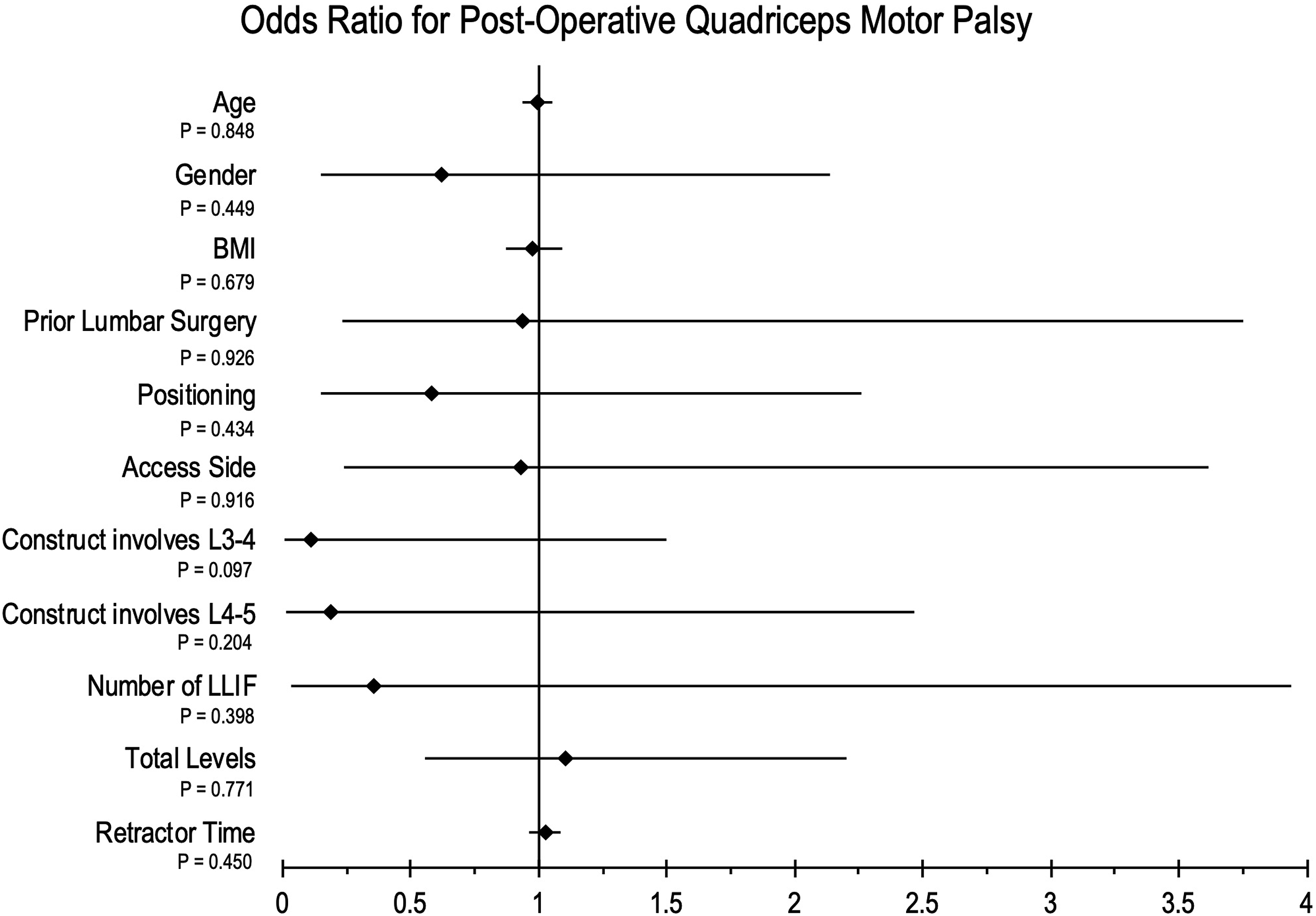
Univariate analysis of the risk factors for post-operative quadriceps motor palsy. ♦ signifies the odds ratio, and the black line signifies 95% confidence interval.
Retractor Time
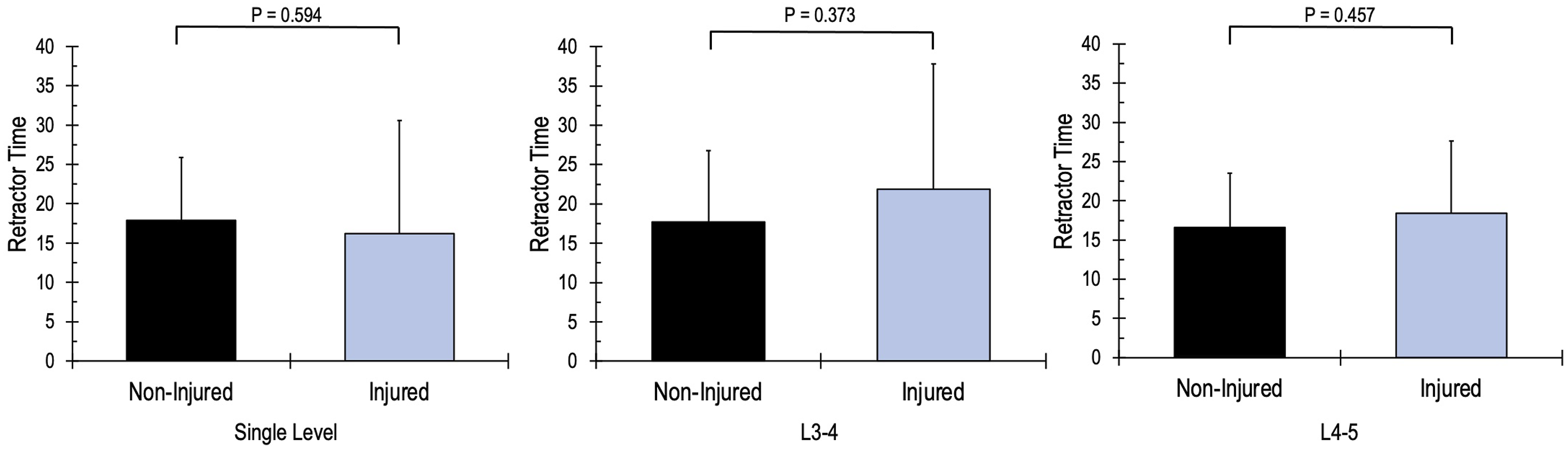
The average retractor time for the entire cohort was 17.5 ± 8.0 minutes. There was no difference between the average retractor time for the cohort and the average retractor time for L2-3 (18.0 ± 8.1 minutes), L3-4 (17.4 ± 10.3 minutes), L4-5 (17.1 ± 8.0 minutes) individually. The average retractor time was significantly shorter for implants placed in the lateral position (16.3 ± 7.2) compared to implants placed in the prone position (19.6 ± 9.0, P < 0.001). The average retractor time for injured patients was 19.6 ± 11.2 minutes, which was not significantly different from the non-injured patients (17.5 ± 8.0 minutes) (Figure 2). There was no difference in retractor time between genders or construct length. Multi-linear regression analysis demonstrated no relationship between retractor time and age, BMI, gender, construct length or number of lateral interbody levels fused. Implants placed in the prone position and prior lumbar surgery both demonstrated a significant relationship with retractor time (P < 0.001 and P = 0.002, respectively). Comparison of the retractor time for injured vs non-injured patients.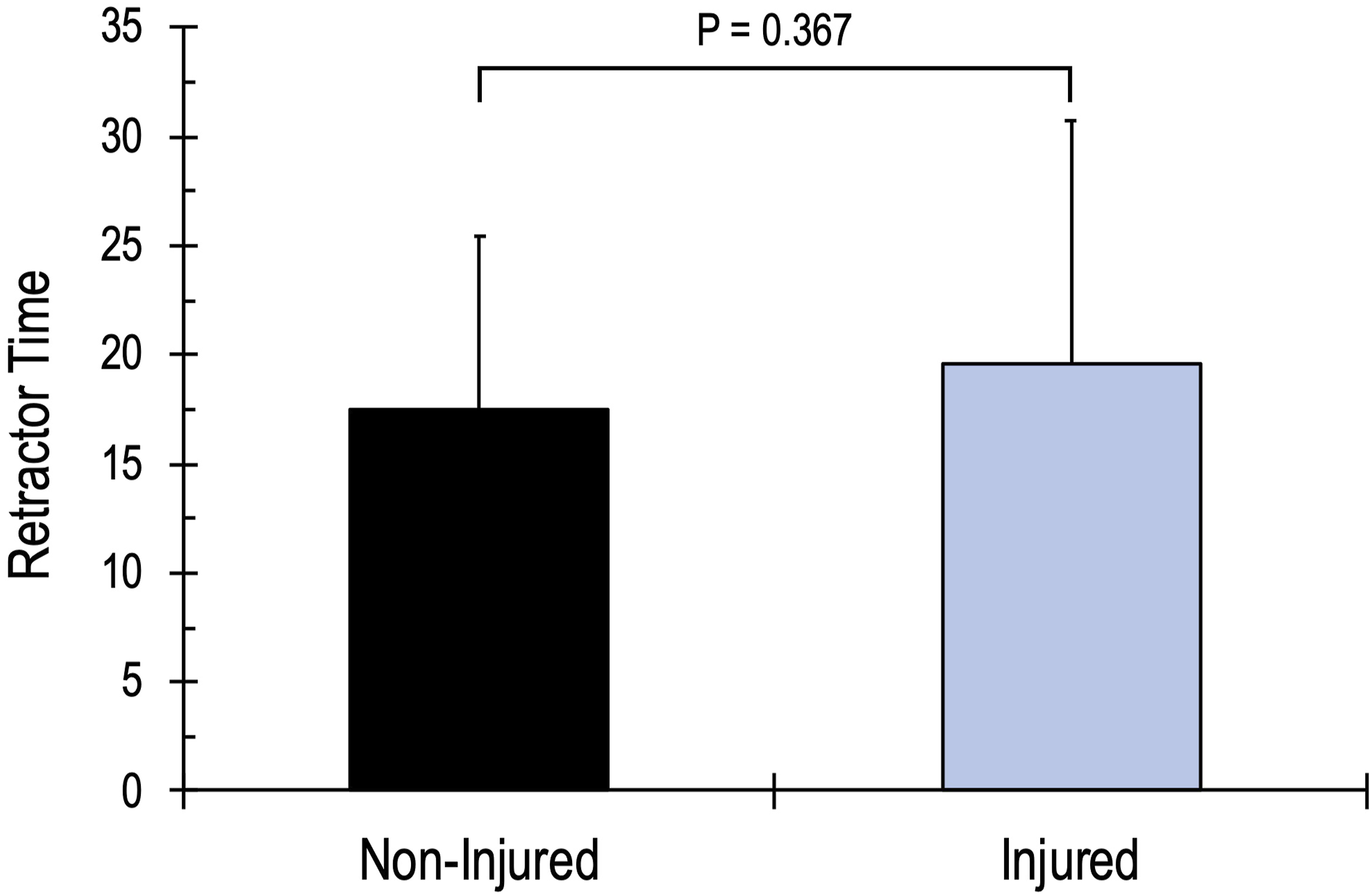
The “20-Minute Rule”
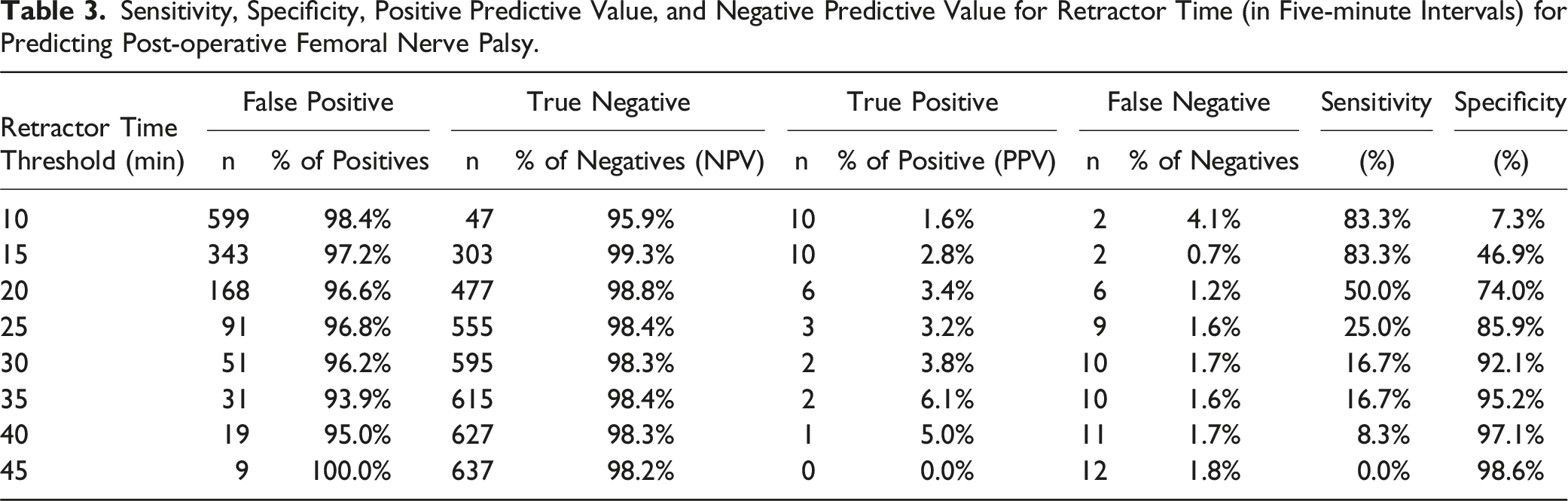
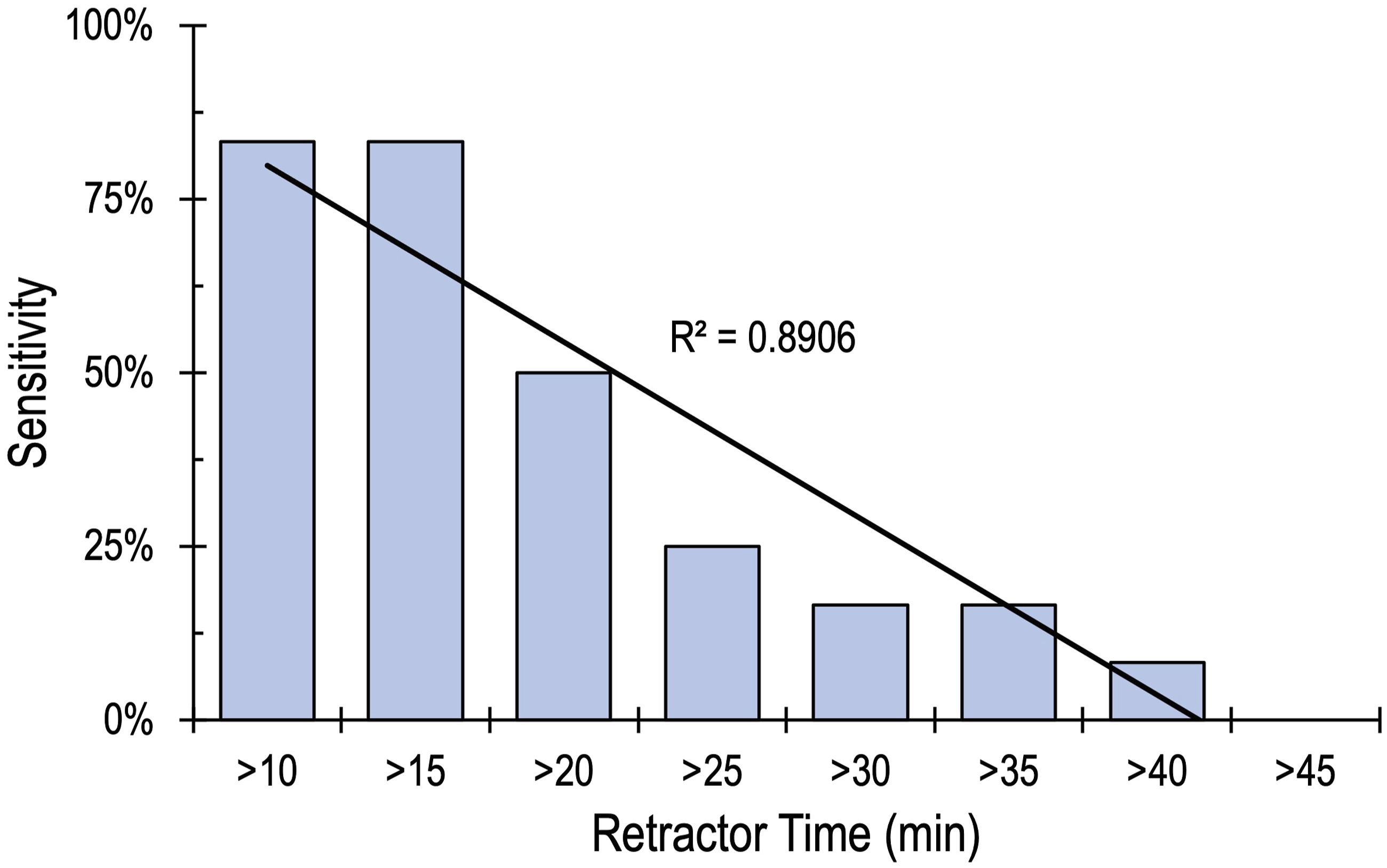
Of the 658 patients reviewed in this study, 26.4% (174 patients) had a retractor time greater than 20 minutes. Six of these patients had a post-operative quadriceps motor palsy, yielding an injury rate of 3.4%, which was not statistically different from those with a retractor time of less than 20 minutes (1.3%). Figure 3 shows the injury rate based on retractor time. To assess the 20-minute rule’s ability as a guide for preventing injury, sensitivity and specificity analyses were conducted to examine the predictive value of the test. In this study, the “20-minute rule” demonstrated a sensitivity of 50% and a specificity of 73.8%; statistical analysis did not find a significant relationship between retractor time greater than 20 minutes and post-operative quadriceps motor palsy. Analysis was then conducted to examine alternative thresholds for the rule. There were 53 patients with retractor times longer than 30 minutes, and 20 had retractor times longer than 40 minutes, yielding a sensitivity of 16.7% and 8.3%, respectively. There were 9 patients with retractor times greater than 45 minutes with 0 injuries (sensitivity of 0%). All of the alternative thresholds are displayed in Table 3. Analysis of the alternative thresholds demonstrated a strong negative correlation between retractor time and sensitivity (R2 = 0.891), as Figure 4 demonstrates a linear decrease in sensitivity as retractor time thresholds increase. The positive predictive value (injury rate) increased for some of the alternative thresholds; however, none of these alternative thresholds yielded a significant relationship. ROC curve analysis indicated that retractor time was a poor predictor and did not identify a retractor time threshold with significant sensitivity or specificity for predicting post-operative quadriceps motor palsy. Injury rate based on retractor time. Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value for Retractor Time (in Five-minute Intervals) for Predicting Post-operative Femoral Nerve Palsy. Sensitivity for predicting post-operative femoral nerve palsy at increasing thresholds for retractor time.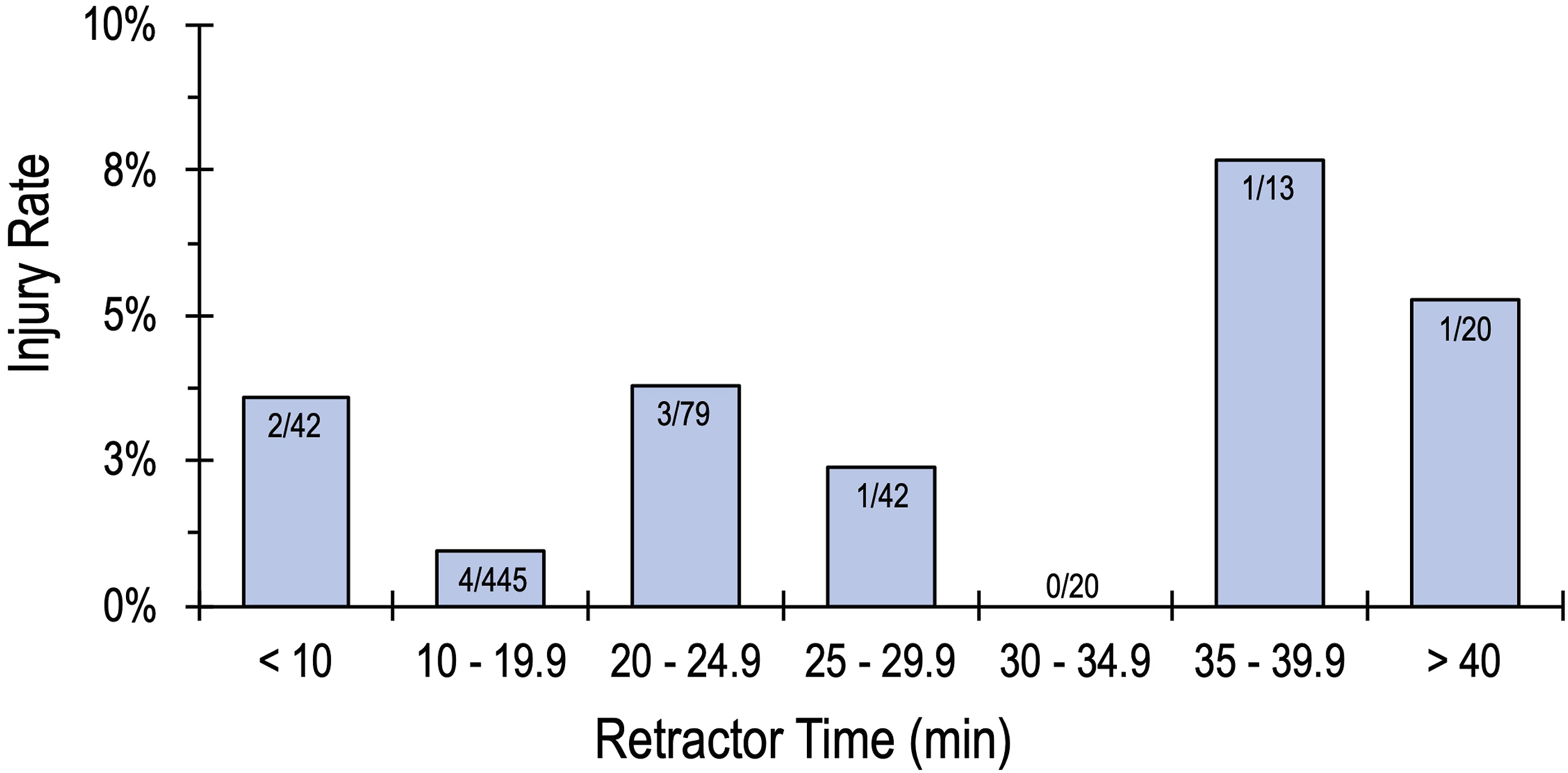
Subgroup Analysis
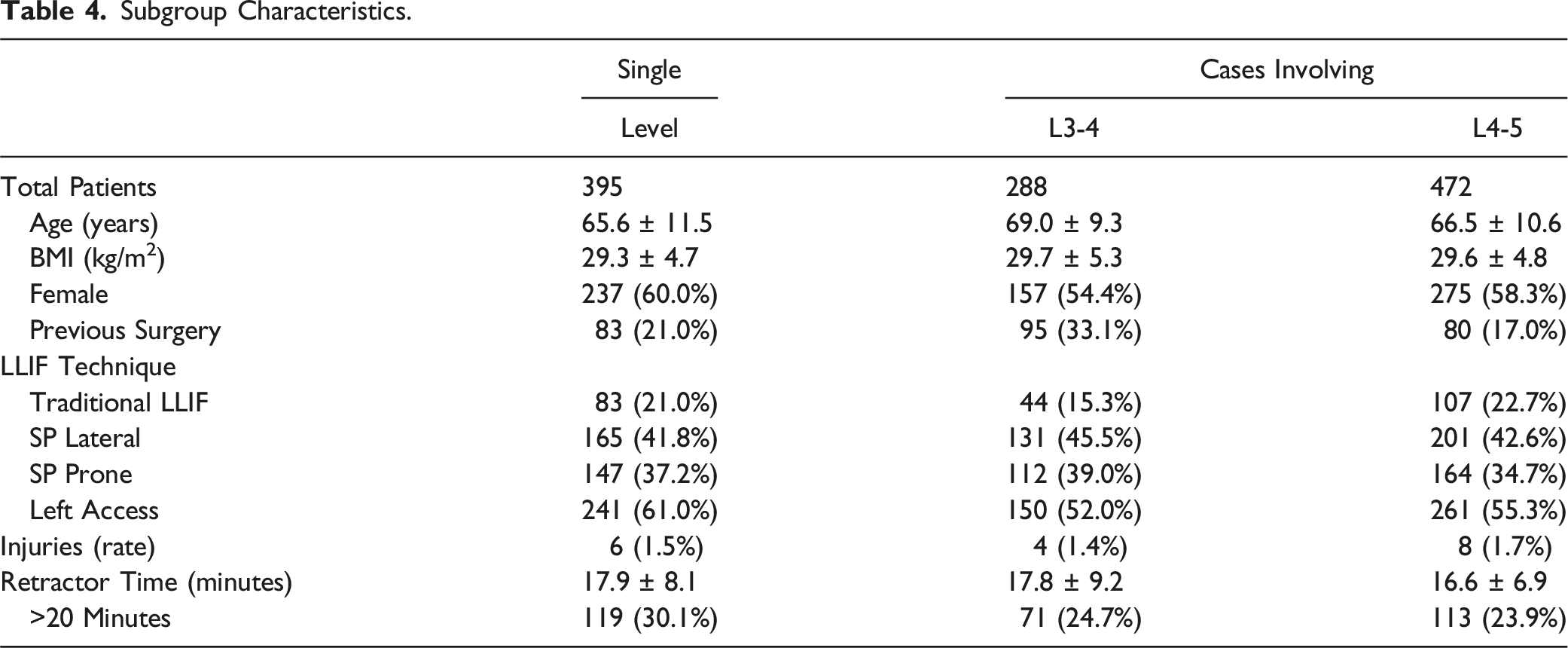
Subgroup Characteristics.
Subgroup comparison of injured vs non-injured retractor times.
Discussion
Improving surgical efficiency to minimize retractor times during lateral lumbar interbody fusion (LLIF) has been at the forefront of conventional teaching since Bendersky et al. and Uribe et al.’s papers in 2015.14,19
Bendersky et al. conducted a prospective single center study of 107 patients undergoing LLIF with a standardized neuromonitoring protocol. There were no patients with new postoperative motor deficits, and 19 patients had minor sensory complaints postoperatively. Following a review of these sensory deficits, the authors began actively measuring retraction time and recommended limiting it to 20 minutes to prevent injuries. 19 Uribe et al. conducted a prospective, multicenter study of 323 L4-5 LLIF sought to examine if t-EMG can predict postoperative symptomatic neuropraxia, it concluded that increasing retractor times was a predictor of declining nerve integrity. In that study, the average retractor time was 23 minutes (range: 6 to 100 minutes); the 13 injured patients averaged 32.2 minutes, significantly higher than the non-injured patients’ average of 22.6 minutes. 14 A similar conclusion occurred after a 2022 study, from the same authors (Morgan el al.), examining femoral nerve neurapraxia following 29 L4-5 prone LLIFs. 18 Morgan reported an average retractor time of 14.6 ± 6.1 minutes and found that 10 of the 29 patients reported postoperative neuropraxia, with only one patient reporting motor symptoms. They reported that the average retraction time for all patients who reported neuropraxia was significantly higher than that of those who did not report symptoms, reporting that the one patient with a motor deficit had a retractor time of 27 minutes. While these studies identified a relationship between prolonged retraction time and postoperative deficits, none delved deeply into the mechanisms underlying these injuries. It remains plausible that other factors, such as patient-specific anatomical challenges, contributed to both the injuries and the longer retraction times. For instance, Bendersky et al. explicitly stated that patients with postoperative sensory deficits often presented with more troublesome surgical approaches, which led to prolonged retraction times. 19 This observation suggests that the injury may have been caused by the difficult approach itself, with longer retraction times serving as a confounding variable.
The concept that prolonged retraction time is not the sole causative factor for injuries is further supported by studies reporting longer average retraction times without an associated increase in injury rates, as well as investigations finding no significant correlation between retraction duration and postoperative nerve deficits.
Pimenta et al. reported an average retractor time double that of Morgan et al. (29 minutes) with a similar rate of motor injury, 1 out of 27 L4-5 prone LLIFs. 24 Silverstein et al. published 172 LLIF cases with an average retractor time of 29 minutes, with only 2 patients having postoperative deficits. 25 Tohmeh et al. published a prospective study examining a neuromonitoring modality where they reported no difference in retractor times between injured vs non-injured patients, with injured patients averaging 14.2 minutes compared to 15.4 minutes for non-injured. 17 Tohmeh reported neuromonitoring alerted on average 9 minutes after the retractor was open and found that the likelihood of encountering an alert was not influenced by retractor time. 17 Recently, Mundis et al. published a retrospective review of 169 patients examining their intraoperative neuromonitoring protocol. In this study, they reported an average retractor time of 19.8 minutes for patients without post-operative deficits and 19.7 minutes for patients with post-operative deficits, finding no association between retractor time and post-operative deficits. 26 Mueller et al. examined the use of retractor time as a predictor of motor dysfunction in 26 patients undergoing L4-5 LLIF. They reported an average retractor time of 26.8 minutes (range 14-51) and found no correlation between retractor time and postoperative motor dysfunction. 27 Despite discrepancies in reported outcomes and no study directly examining the principle of retractor time thresholds for preventing injury, the “20-minute rule” is still discussed by experienced lateral surgeons and taught to surgeons learning the lateral technique today. Reinforcing surgical speed, rather than meticulous technique, may discourage a surgeon from adopting the technique for fear of injuring the patient. There is a need to clarify the relationship between retractor time and motor injuries in LLIF.
This study examined the relationship of retractor time to injuries, analyzed the “20-minute rule”, and examined its ability to predict post-operative quadriceps motor palsy. In this cohort of 658 patients, implant placement in the prone position was the only factor that influenced retractor time. This is an expected finding, as single position prone introduces gravity as a factor that increases retractor instability, which could increase retractor time in the early adoption phase. Retractor instability is typically managed by placing an extra disc or bone shim and/or anterior 4th blade, 4 which would add several steps to the procedure and increase the average retractor time by a minute or two. Despite the increased times, there was no significant difference in the injury rate between prone and lateral positioning. There was also no difference in average retraction time for those with or without postoperative quadriceps motor palsy. In this cohort, one hundred and seventy-four (174) patients had a retractor time >20 minutes, 168 patients did not have an injury, and only six of these patients had a post-operative quadriceps motor injury. Using the “20-minute rule” as a guide for preventing these injuries yielded a positive predictive value of 3.4%, a false positive rate of 96.6%, a sensitivity of 50.0%, and a specificity of 74.0%. The results of this analysis show that the “20-minute rule” is not a good predictor of post-operative quadriceps motor palsy.
Since previous studies had linked longer retractor times to increasing injury rates,14,18,19 a secondary analysis was conducted to see if there was a better threshold for injuries based on retraction times. There was a slight but nonsignificant increase in injury rate at higher thresholds, as only 1/20 (5.0%) of patients with retractor times >40 minutes had postoperative quadriceps palsy. Interestingly, this same trend was not seen with the sensitivity analysis. As the retraction threshold increased, there was a significant, linear decrease in sensitivity, demonstrating a sensitivity of 8.3% at a retractor time threshold of 40 minutes. With only 1 of 20 patients with retractor times over 40 minutes (double the “20-minute rule”) having an injury. The authors of this paper adamantly believe in surgical efficiency. Nevertheless, the results of this study indicate that quadriceps motor injuries during lateral surgery are not primarily caused by increased retraction time.
The surgeons in this study are experienced lateral surgeons, which explains why 73.6% of cases had retractor times less than 20 minutes, with most cases occurring at the L4-5. A majority of these cases were straightforward and completed quickly without intraoperative or post-operative complications. Some patients have large osteophytes, degenerative scoliosis with axial rotation, significant anteriorly translated psoas, high crest, larger BMI, poor bone quality, and other factors making surgery difficult, and could increase the retractor time. Longer retractor times likely add to the local inflammatory reaction and are likely a cause of post-operative thigh and hip symptoms – which was not studied in this paper. This is not the case for nerve injuries, as the results of this study indicate no relationship between retractor time and post-operative quadriceps motor injury.
The injury rate of this retrospective study was 1.8%, which is in line with previously reported rates.3,14,18,20 One injured patient was lost to follow-up, and six patients saw a complete recovery of their injury by their twelve-month follow-up. The remaining did not see the full resolution of their symptoms, but all improved to 4/5 or better. In the review of the individual injuries, neuromonitoring alerts were present in 50% of cases, and the alerts correlated with individual steps of the procedure rather than accumulation over time. This was similar to the results of Tohmeh et al, who reported that the neuromonitoring alerts for their injuries had all occurred prior to 12 minutes of retraction time. 17 Considering those results with the findings from this study, the data indicates that injuries are likely related to the individual steps of the procedure rather than the accumulation of retractor time. These results support the recently published multi-national L4-5 LLIF article that emphasized a careful and standardized LLIF technique that yielded a very low injury rate (0.8% and 0.4% persistent femoral neuropraxia). 28 This study does not have the power to prove that injuries are related to the individual steps of a procedure, as neuromonitoring only identified half of the injuries. There is a need for a reliable neuromonitoring modality that can provide real-time feedback on nerve integrity and run it sequentially after each step of an LLIF.
Careful technique is crucial to a successful LLIF procedure, but the results of this study show that if the retractor is docked in a safe position, longer retractor times do not compromise the integrity of the nerve. Surgical efficiency is still very important, yet if retractor time is becoming long, the authors recommend continuing to work at a normal pace and using neuromonitoring as a guide. The authors believe that injuries are multifactorial, related to patient-specific factors and the individual steps of the procedure. These steps may be complicated by abnormal patient anatomy and/or scar tissue from previous surgeries, possibly increasing the risk of injury. Intuitively, the more difficult cases may be more likely to have an injury, and more difficult cases may take longer. In these cases, retractor time may be an extraneous variable, causing a confounding bias.
Limitations
This study is limited by its retrospective nature and limited data collection, which can give rise to a potential selection bias. The inclusion of consecutive patients for each surgeon hopefully mitigates this risk. This study did not collect variables that may make the lateral access more difficult, including individual patient anatomy measurements, degree of retractor expansion, previous operative history, or medical comorbidities. All studies based on physical exam findings are subject to intra-observer bias; while this study took measures to control for this variable, there is still the possibility for that bias to be present. This study only examines post-operative quadriceps motor deficits and does not examine any sensory or motor deficits in other muscle groups. This is in part due to the difficulty controlling physical exams for each muscle group. Post-operative hip flexor motor deficits were not examined in this study; since the approach is directly through the psoas muscle, post-operative hip flexor deficits are an expected finding in this approach. Only patients with persistent motor symptoms would be considered true hip flexor motor deficits, and this data was not collected consistently on every patient.
Conclusions
Post-operative quadriceps motor palsy after lateral lumbar interbody fusion does not appear to be caused by prolonged retractor times; rather, these injuries are likely a multifactorial issue. Limiting retractor time to under 20 minutes was a poor predictor of post-operative quadriceps injury; as the “20-minute rule” demonstrated a low sensitivity and low positive predictive value for predicting postoperative femoral nerve palsy. Analysis of alternative thresholds for this rule found that the sensitivity decreased as the retractor time cut-off increased. The authors agree that attention to careful docking and careful technique should take precedence over limiting retractor time.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.