
Abstract
Objectives
Among patients undergoing elective spine surgery, psychological processes such as kinesiophobia and pain catastrophizing are associated with postoperative disability and poor quality of life. These represent risk factors which could be modified to improve surgical outcomes. We reviewed perioperative interventions to modify psychological processes and their effects on psychological and surgery-related outcomes.
Methods
We searched MEDLINE, EMBASE, and Cochrane databases for studies examining any interventions for modifying psychological processes in adult patients undergoing spine surgery. Two reviewers screened studies for eligibility, extracted data in duplicate, and performed risk of bias assessments. Outcomes included pain, disability, quality of life, kinesiophobia, self-efficacy, and pain catastrophizing.
Results
368 titles and abstracts were retrieved, of which 27 studies underwent full-text screening. We included 12 studies which reported on 1263 patients. Eight were randomized controlled trials. Interventions included preoperative and postoperative cognitive behavioural therapy, cognitive-behavioural-based physical therapy, a web-based interactive platform, an information booklet, and music therapy. The psychological and surgery-related outcomes of interventions were variable, with some studies reporting significant benefits and others reporting no differences between groups. The greatest potential benefits were found in studies of post-operative cognitive-behavioural-based physical therapy. Risk of bias among studies was high due primarily to lack of blinding and limited standardization of interventions.
Conclusions
Several interventions to potentially modify psychological processes in patients undergoing spine surgery have been reported. Post-operative cognitive-behavioural-based physical therapy might be associated with improved outcomes, but confidence is limited by inconsistency, risk of bias, and limited long-term follow-up.
Keywords
Background
For many patients living with debilitating spine conditions, surgery can offer substantial improvements in pain, function, and quality of life. However, some patients also have comorbid psychological processes such as anxiety, depression, pain catastrophizing, and kinesiophobia (an excessive, irrational, and debilitating fear of physical movement and activity 1 ), which have been associated with worse outcomes and less satisfaction2-10 even among patients who experience clinical improvement. 11 As such, these psychological processes may represent modifiable risk factors that could potentially be altered to improve patient care.
Interventions to modify psychological processes include cognitive behavioral therapy, specialized physical therapy, music therapy, biofeedback, mindfulness, and meditation, 12 but the potential effects of these interventions for patients undergoing spine surgery are poorly understood. Although there is evidence to support various psychological interventions as adjuncts in the treatment of chronic spinal pain,13,14 studies of their implementation and effectiveness in the context of surgery have shown mixed results. Two recent meta-analyses15,16 suggested no benefit for preoperative “prehabilitation” programs on functional or psychological outcomes in spine surgery, and one meta-analysis of perioperative cognitive behavioural therapy (CBT) 17 suggested a significant effect on postoperative quality of life, psychological outcomes, disability, and pain despite substantial heterogeneity between studies.
In order to inform patient care and guide further research in this field, we performed a systematic review to answer the following questions: 1. Among patients undergoing elective spine surgery, what interventions are used to modify preoperative psychological processes? 2. What are the psychological and spine-related outcomes of these interventions?
Methods
Selection of Studies
We performed a systematic review according to the methodology outlined in the Cochrane Handbook for Systematic Reviews. MEDLINE, EMBASE and Cochrane Databases were searched using MESH and EMTREE headings and subheadings in various combinations, supplemented with free text (Appendix 1). All databases were searched from inception to March 18, 2024. Two reviewers (AA and MG) performed the initial title and abstract screen of retrieved studies, full manuscript review, and data abstraction from the final list of included studies. In cases of disagreement, a third author (NE) screened the studies with discrepancies resolved by consensus.
Eligibility
We included randomized controlled trials, prospective and retrospective cohort studies, and prospective case series that were available in English. We excluded case studies, review articles, and conference abstracts. Patient populations were limited to adults over 18 years of age undergoing spine surgery for an indication at any spinal level. Studies were eligible if psychological processes were measured pre- and postoperatively using a standardized scale or questionnaire and a preoperative or postoperative intervention to modify psychological processes was evaluated. Data abstracted from full-text review included type of surgery; type, duration, and protocol of intervention implemented; administrator of intervention and their training level; time points for outcome evaluation; and outcomes evaluated.
Outcomes
Outcome data abstracted included all psychological and/or surgery-related outcomes, which ultimately included: pain catastrophizing, kinesiophobia, fear avoidance beliefs, self-efficacy, perceived control over pain and ability to decrease pain, anxiety and depression, global rating of mental health; disability, axial and extremity pain, quality of life, physical activity, tests of physical performance and range of motion, and return to work and activities of daily living.
Risk of Bias Assessments
Included studies were evaluated for Risk of Bias using the RTI Item Bank on Risk of Bias and Precision of Observational Studies 18 or the Revised Cochrane Risk-of-Bias Tool for Randomized Trials 19 as applicable.
Synthesis
Data abstracted from each study were compiled and interpreted descriptively. A meta-analysis was not planned or performed due to the anticipated and observed substantial heterogeneity of study design and outcomes among the included studies.
Results
Study Selection
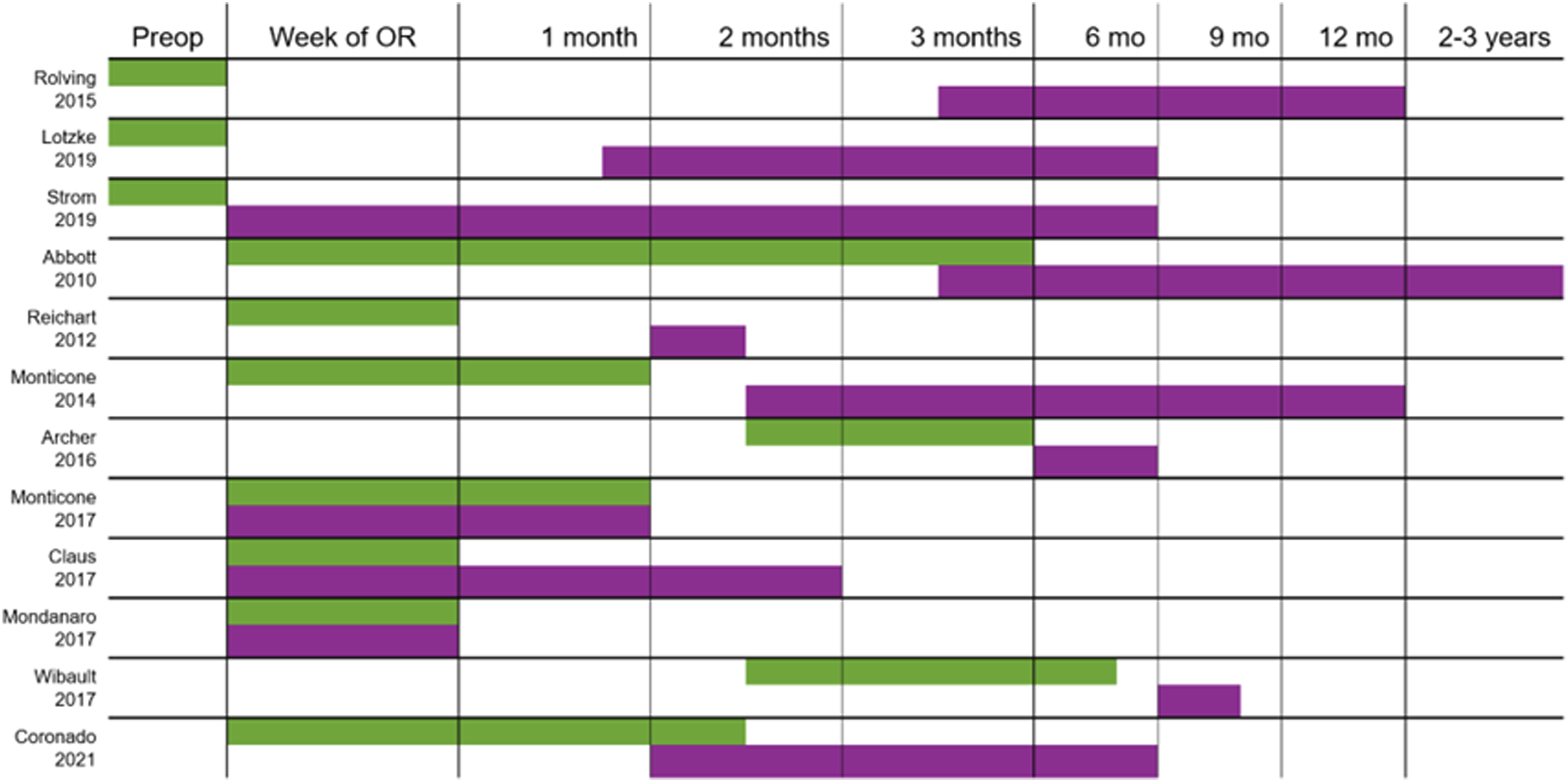
The study selection process is summarized in Figure 1. We identified 368 potentially relevant studies, of which 27 were selected for full-text review after screening of titles and abstracts. Screening of reference lists from these articles as well as prior systematic reviews identified 3 more potentially relevant studies. In total, 12 studies were included. Study designs, timing of interventions, patient populations, and interventions are summarized in Figure 2. Study selection. Duration of interventions (green) and follow-up (violet).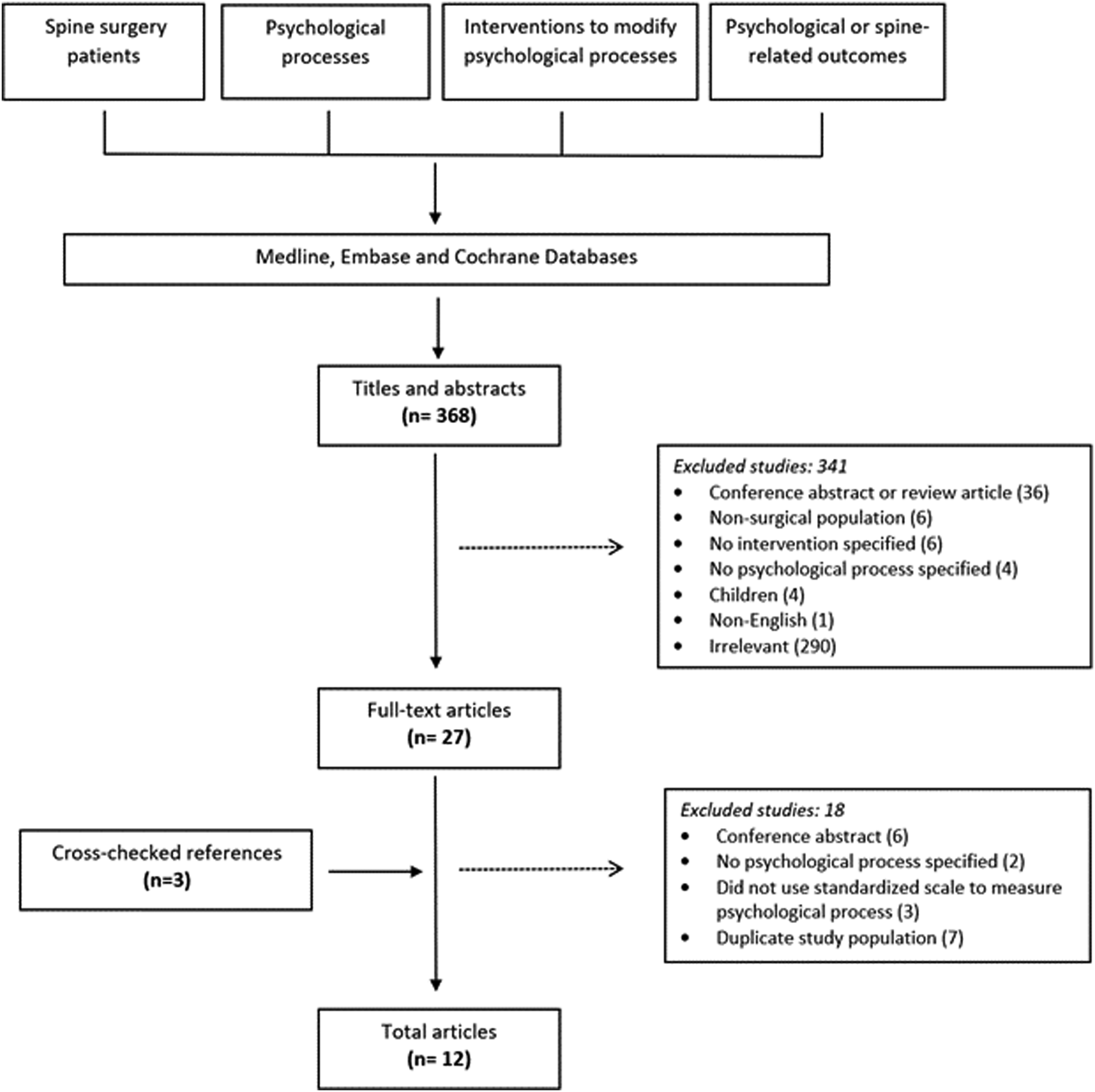
Study Characteristics
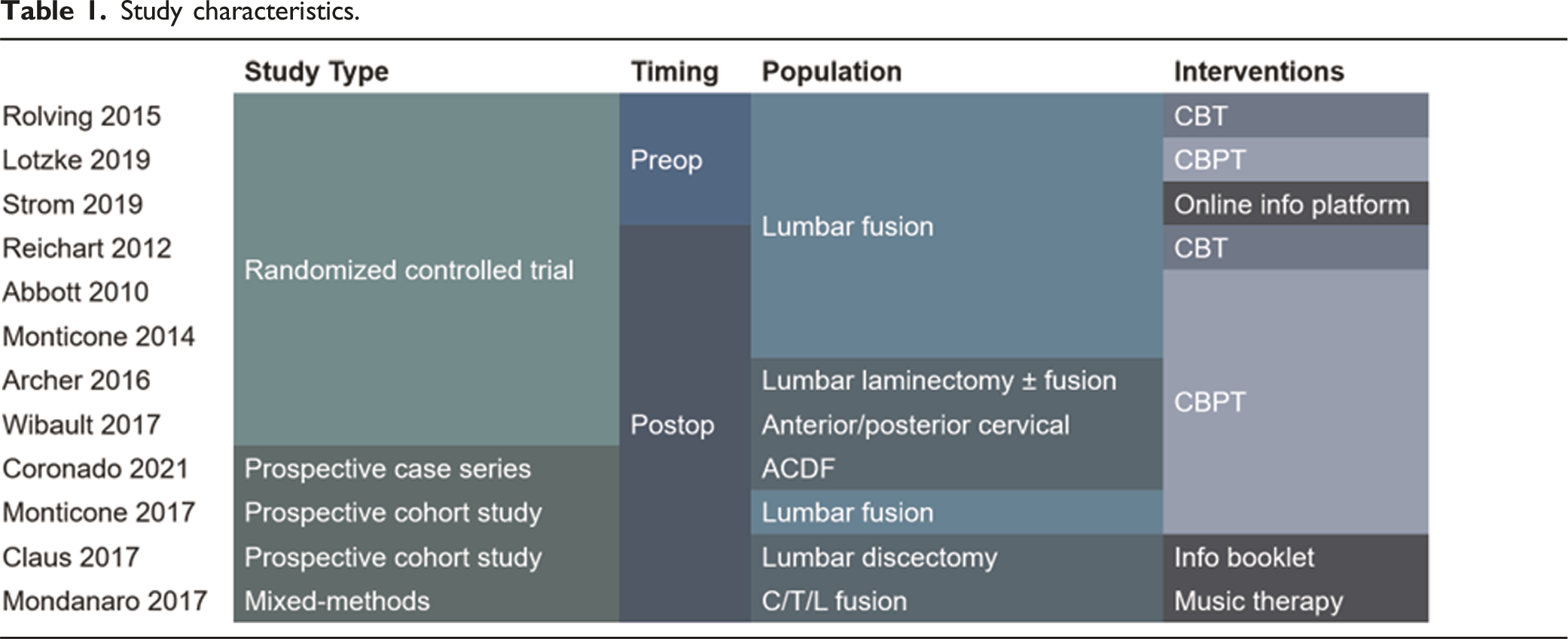
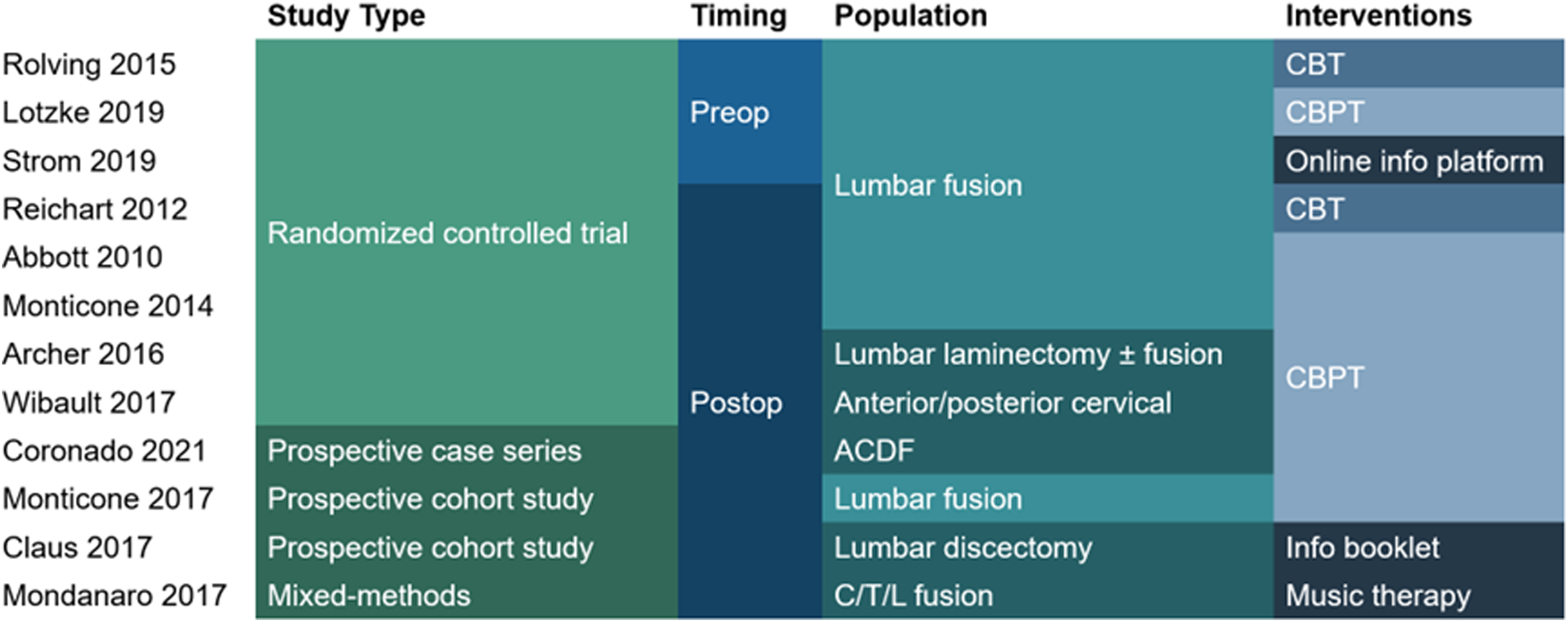
The 12 included studies reported on 1263 patients. Three studies20-22 investigated preoperative interventions and nine23-31 postoperative interventions. All 3 studies of preoperative interventions and five studies of postoperative interventions25,28-31 (67%) were conducted as randomized controlled trials. Other study designs included prospective cohort studies,24,27 a prospective case series, 23 and a mixed methods study. 26 Study populations included patients undergoing lumbar fusion (seven studies, N = 778), lumbar decompression with or without fusion (one study, N = 86), lumbar discectomy (one study, N = 129), anterior cervical decompression and fusion (two studies, N = 171), posterior cervical decompression (one study, N = 39), and anterior, posterior, or combined spinal fusion not otherwise specified (one study, N = 60).
Study characteristics.
Effects of Interventions
Study characteristics, results, and risk of bias assessments for 12 included studies.
AUC = area under curve, DDD = degenerative disc disease, MIC = minimally important change, OT = occupational therapist, PT = physical therapist, QOL = quality of life, ROC = receiver operating characteristic, SF-12 = 12-Item Short Form Survey, SF-36 = 36-Item Short Form Survey, VAS = visual analogue scale.
Of the 9 studies of cognitive-behavioural-based interventions, seven20,23,25,27-29,31 (78%) reported a significant improvement in psychological outcomes and six21,23,28-31 (67%) in surgery-related outcomes. All four studies which reported positive results in both domains used postoperative cognitive-behavioural physical therapy techniques. None of the preoperative interventions reported a significant benefit for postoperative pain or disability. The reported psychological 20 and quality of life 21 effects from preoperative interventions were small and transient, suggesting a potential benefit in the immediate postoperative period with uncertain clinical significance.
Psychological Outcomes
The most commonly reported psychological processes were kinesiophobia, impaired self-efficacy, and pain catastrophizing. The number of studies reporting significant results for these processes are summarized in Figure 3. Seven20,23,24,27-29,31 of nine studies reporting on kinesiophobia used the Tampa Scale for Kinesiophobia or Fear Avoidance Beliefs Questionnaire and reported better postoperative scores in the intervention group, as did three23,28,31 of five studies that used a self-efficacy scale (Pain Self-Efficacy Questionnaire, Self-Efficacy for Exercise Scale, Swedish Self-Efficacy Scale). Four20,23,25,29 of six studies that measured pain catastrophizing (Pain Catastrophizing Scale or catastrophizing subscale of Coping Strategies Questionnaire (CSQ-CAT)) reported better scores with the intervention. Differences in kinesiophobia, self-efficacy, and catastrophizing were observed at early follow-up in six studies,23,24,27-29,31from as early as 4 weeks with effects sustained at long-term follow-up in two of 3 studies.29,31 Other studied psychological processes and outcomes included the Hospital Anxiety and Depression Scale and the SF-36 and SF-12 Mental Health scores. Significant results for psychological outcomes by study.
Surgery-Related Outcomes
Six23,26,28-31 of ten studies reported on pain outcomes (Visual Analogue Scale, Numerical Rating Scale, Brief Pain Inventory, or German Pain Questionnaire) and found a significant difference favouring the intervention group, as did five23,28-31 of eight studies which reported disability outcomes (Oswestry Disability Index, Neck Disability Index, Hannover Back Function Questionnaire). The numbers of studies reporting significant results for these traits are summarized in Figure 4. Pain outcomes were improved in the intervention group at short-term (<3 months) follow-up in six studies23,26,28-31 with sustained effects seen at 6 months in two out of two studies23,31 reporting pain outcomes at this timepoint and 12 months in one study
29
out of two. For disability, an effect was seen at short-term follow-up in six studies,21,23,28-31 up to 6 months in one study,
23
and at long-term (≥12 months) follow-up in two studies.29,31 One of 3 studies which reported on quality of life (EQ-5D/5L indices) found a significant improvement up to 8 weeks.
21
Significant results for surgery-related outcomes by study.
Risk of Bias
Detailed bias assessments are reported in Appendix 2 and are summarized in Table 2. The risk of bias among studies was generally high due to lack of blinding of patients, intervention providers, and assessors, as well as limited adherence to and standardization of interventions.
Discussion
We performed a systematic review to identify interventions to modify psychological processes among patients undergoing spine surgery. We found that several interventions have been reported, but that post-operative cognitive behavioural therapy combined with exercise-based physical therapy might be most associated with improvements in kinesiophobia and pain catastrophizing, as well as postoperative pain and disability. Confidence in these findings is limited by inconsistency, heterogeneity, imprecision, risk of bias, and limited long-term follow-up.
Relation to Prior Literature
This study adds substantially to a small but growing body of literature about perioperative psychological interventions for patients undergoing spine surgery. In contrast to prior reviews on this topic, we report on both psychological and surgery-related outcomes, and we compared multiple pre- and postoperative intervention modalities. A recent systematic review by Scarone et al 32 studied the effect of perioperative psychological interventions on persisting spinal pain and secondary surgical outcomes including disability and quality of life in a more restricted population of patients undergoing fusion procedures. That review did not report psychological outcomes but similarly found that perioperative cognitive behavioural-based interventions may be associated with improved pain, disability, and quality of life postoperatively. A recent meta-analysis by Parrish et al 17 of RCTs on CBT-based interventions in lumbar spine surgery analyzed seven studies of 531 patients with generally more restrictive inclusion criteria excluding observational studies and non-CBT interventions. Using a sensitivity analysis, significant positive effects were identified for psychological outcomes (standard mean difference, SMD = 0.61), quality of life (SMD = 0.55), and to a lesser degree, pain and disability. On subgroup analysis of psychological outcomes, the largest effect size was observed for kinesiophobia (SMD = 0.67). This review quantitatively corroborates our findings in a more limited sample of studies amenable to meta-analysis. Similar heterogeneity was nonetheless observed between studies in this work.
Our findings suggest increased benefits from postoperative interventions rather than preoperative or “prehabilitation” strategies, which is supported by a pair of recent meta-analyses finding no significant effect of preoperative CBT on postoperative outcomes.15,16 Some studies included in similar reviews, such as two RCTs analyzed in Parrish et al,33,34 were excluded here because psychological processes were not measured preoperatively or post-operatively. Despite this finding, psychotherapeutic interventions have a strong body of evidence for treating specified comorbid diagnoses associated with poor surgical outcomes including substance use disorders, eating disorders, anxiety, and depression. It follows that psychological prehabilitation strategies could still have a clinical role in high-risk patients, 16 but further work in future studies including preoperative risk stratification will be necessary to define their potential benefit and optimal target population.
Our assessment of the risk of bias among included studies differed from both Scarone et al and Parrish et al, with seven of eight RCTs graded as having a “high” risk of bias in the present work using the Cochrane RoB 2 tool 19 (Appendix 2). This discrepancy is attributable to the use of different bias assessment tools, and specifically the importance given to lack of blinding of patients, providers, and assessors, but we acknowledge that blinding is not possible for many psychological interventions. 35
Outside of spine surgery, the observed effects of perioperative psychological interventions have been inconsistent. In elective orthopedic surgery, meta-analyses have suggested some improvements in postoperative pain, anxiety, quality of life, and disability, but results have varied between studies and even between similarly conducted reviews.36-39 Both pre- and postoperative interventions have shown variable benefit for modifying psychological processes, but postoperative interventions may have a stronger impact on postoperative pain.36,37 While cognitive behavioural-based methods have been the most widely studied perioperative psychological interventions, there is also evidence across surgical disciplines to support a variety of techniques less commonly cited in the spine literature, including relaxation, guided imagery, hypnosis-based interventions, and digital psychoeducation platforms.40-42 Our review retrieved an insufficient sample of interventions besides cognitive behavioural-based methods to draw clear conclusions on other specific techniques.
Implications
The impact of psychological processes on postoperative outcomes in spine surgery is well-known,2-11 but strategies to screen for and potentially intervene on patients at risk may be underutilized in clinical practice. The results of our review suggest that postoperative cognitive behavioural strategies combined with exercise-based physical therapy (CBPT) might be considered for patients undergoing elective spine surgery, but further research is warranted to confirm these findings and increase confidence when considering application to clinical care. While a survey of US spine surgeons 43 demonstrated strong beliefs regarding the impact of psychological factors on pain relief, adherence to therapy, and return to work following surgery, approximately only one third of these surgeons employed presurgical psychological screening despite its validation as a predictor of postoperative outcomes. 44 The extent of screening, tools used, and effects seen were variable among survey respondents.
The large and growing surgical and non-surgical patient volume at many spine surgery centres suggests that indiscriminate application of perioperative psychological interventions could be clinically and economically unfeasible, but routine psychological screening with validated questionnaires to identify candidates who could benefit from such interventions might be a reasonable approach. 45 While not the primary focus of this review, we found that the Tampa Scale of Kinesiophobia 46 was the most widely used instrument in the included studies. Perioperative kinesiophobia has been shown to be modifiable with CBT-based interventions in spine surgery 17 and has been previously validated as a predictor of postoperative outcomes.7,8,47
Limitations
It is not possible to draw strong conclusions from this review due to the limitations and small volume of the included studies. There was substantial inconsistency of the effects seen in both psychological and clinical outcomes between studies with similar research protocols and patient populations. Risk of bias further limits the interpretation and utility of these results when considering the clinical and economic effectiveness of implementing specific intervention strategies. This study was also limited by the methodological heterogeneity of study design and intervention protocols which precluded a quantitative meta-analysis.
Conclusion
Several interventions to potentially modify psychological processes associated with poor outcomes in patients undergoing elective spine surgery have been reported. Postoperative cognitive behavioural therapy combined with exercise-based physical therapy may be associated with improved psychological and clinical outcomes, but interpretation of the literature is limited by inconsistency, imprecision, and risk of bias. Preoperative CBT has not been conclusively shown to significantly modify postoperative outcomes.
Supplemental Material
Supplemental Material - Interventions to Modify Psychological Processes in Patients Undergoing Spine Surgery: A Systematic Review
Supplemental Material for Interventions to Modify Psychological Processes in Patients Undergoing Spine Surgery: A Systematic Review by Matthew Skarsgard, Alysa Almojuela, Martin Gagliardi, Ganesh Swamy, Fred Nicholls, W Bradley Jacobs, Kenneth C Thomas, Alex Soroceanu, Denise Eckenswiller, Elias Soumbasis, Rob Tanguay, and Nathan Evaniew in Global Spine Journal.
Footnotes
Author contributions
MS: literature retrieval, data abstraction, descriptive analysis, manuscript preparation, editing, and approval. AA: study design, literature retrieval, data abstraction, descriptive analysis, manuscript preparation, editing, and approval. MG: study design, literature retrieval, data abstraction, descriptive analysis, manuscript editing and approval. GS: study design and manuscript editing, review, and approval.FN: study design and manuscript editing, review, and approval. WBJ: study design and manuscript editing, review, and approval. KCT: study design and manuscript editing, review, and approval. AS: study design and manuscript editing, review, and approval. DE: study design and manuscript editing, review, and approval. ES: study design and manuscript editing, review, and approval. RT: study design and manuscript editing, review, and approval. NE: study design, review of data abstracted and bias assessments, descriptive analysis, manuscript editing, review, and approval
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.