
Abstract
Study Design
Retrospective study.
Objective
To elucidate the factors influencing the identification of causative microorganisms in vertebral osteomyelitis (VO) and the effectiveness of different culture methods in increasing the identification rate.
Methods
A total of 252 patients diagnosed with and treated for VO at a single hospital were enrolled. The results of various culture methods were reviewed along with the clinical data of the patients retrospectively.
Results
Microbiological diagnosis was achieved in 210 out of 252 patients (83.3%). Diagnostic percentages of blood cultures, CT-guided drainage, fluoroscopic disc biopsy, and intraoperative specimens were 73.6%, 73.9%, 27.6%, and 50.8%, respectively. Staphylococcus aureus was the most common pathogen (85 cases, 40.5%). Higher White Blood Cell (WBC) count, lower serum albumin (ALB) level, epidural abscess, and absence of prior antibiotic exposure were significant predictors of positive culture results across all culture methods. Prior antibiotic exposure was the most significant predictor of negative outcomes (OR 0.24). Blood culture results correlated with body temperature, C-reactive protein (CRP), ALB, and prior antibiotic exposure. A shorter duration of antibiotic administration before culture was associated with an increased likelihood of positive blood culture results.
Conclusions
This study demonstrated that laboratory findings indicating a high inflammatory response (elevated WBC count, CRP level, and body temperature), lower ALB level, presence of epidural abscess, absence of prior antibiotic exposure, and shorter duration of antibiotics were significant predictors of positive culture results. Blood cultures should be conducted in the presence of high inflammation levels to improve microorganism identification rates.
Keywords
Introduction
Vertebral osteomyelitis (VO) is a common spinal infection that is diagnosed through clinical presentation, blood tests, and imaging. While conservative treatment with antibiotics is the first choice, surgery may be needed when VO causes spinal instability and neurological symptoms or in cases where the disease is refractory to antibiotic therapy. 1 The first-line treatment for VO is intravenous antibiotic therapy, boasting a reported cure rate of approximately 90% in the literature.2,3
Ensuring antibiotic efficacy relies on identifying the organism responsible for spondylitis and administering an appropriate drug. Recent studies indicate an increasing number of patients with culture-negative VO annually, complicating treatment duration recommendations.4,5 Despite recommendations ranging from 4 weeks to 6 weeks 3 to 3 months, 6 the optimal duration of antibiotic use in patients with culture-negative VO remains controversial. A retrospective comparative study reported that the group without identified microorganisms tended to have a longer duration of antibiotic use. 7 Therefore, the identification of causative microorganisms is pivotal for effective and appropriate treatment.
Microbiological diagnosis of VO can be performed through various methods, including blood culture, computed tomography (CT)-guided biopsy, fluoroscopy-guided intervertebral disc biopsy, and intraoperative specimen culture. The average microbiological diagnosis rate was reported to be 76.7%, ranging from 56% to 92%. 8 Blood culture predominantly identified causative microorganisms, with a positive rate of 58% (range across studies, 30%-78%) reported in a systematic review. 9 Though some reports suggest antibiotic administration prior to culture may hinder the identification of the causative organisms,10,11 few detailed studies have explored the factors involved.
This study aimed to investigate the factors influencing the identification of causative microorganisms in VO and the effectiveness of different culture methods in increasing identification rates.
Methods
Patients and Data Collection
This retrospective analysis was conducted at a single tertiary-care hospital and approved by the institutional review board (approval number: zn231213) using anonymized data and a general opt-out procedure. Procedures adhered to ethical standards per our institutional ethics committee and the 1964 Helsinki Declaration and subsequent amendments or comparable ethical standards. The need for informed consent was waived due to the study’s retrospective design. A total of 252 patients diagnosed with and treated for VO between January 2010 and April 2023 were enrolled in the study. The diagnosis of VO was based on imaging studies, including magnetic resonance imaging (MRI) and computed tomography (CT); blood tests such as C-reactive protein (CRP) and white blood cell (WBC) counts; and clinical findings such as fever and back pain. MRI findings associated with VO include destruction of endplates, increased signals in the vertebral bodies and discs on T2-weighted imaging, and epidural or iliopsoas abscesses. These findings were confirmed by a senior spinal surgeon (E.O.) and expert radiologist. For cases with no identified negative causative organism, imaging results were reviewed by radiologists to confirm the absence of sacroiliitis, ruling out non-infectious spondylitis, such as ankylosing spondylitis or axial spondyloarthritis. All cases were treated by a joint team comprising an orthopedic surgeon and a general medicine physician, from the initial diagnosis to the implementation of the treatment plan and the differentiation of other potential diseases. To validate the accuracy of the VO diagnosis, a retrospective review of the clinical course documented in the medical record was conducted.
For patients with VO, at least two sets of blood cultures were obtained at the initial presentation. CT-guided drainage was performed for abscesses revealed by imaging, with specimens cultured. Intraoperative specimens were obtained for culture in cases requiring surgery. To reduce the potential for contamination in the culture results, we consulted with an infectious disease specialist regarding the interpretation of the culture results and did not adopt those results when there was a high likelihood of contamination. Patients with tuberculous spondylitis, postoperative infections after spinal or other surgeries, or those requiring outpatient treatment were excluded from the study.
Clinical data of the patients, including age, body mass index (BMI), and medical history, were collected from their medical records. The Charlson Comorbidity Index (CCI) was used to assess general health status. 12 Among these, diabetes mellitus (DM) was considered a particularly significant comorbidity associated with infections and was treated as an independent factor. Since some cases of DM were well-controlled, glycated hemoglobin (HbA1c) levels were determined and analyzed as a single variable. Additionally, a history of alcoholism was documented under the diagnoses of alcohol-related conditions, including alcoholic liver cirrhosis, alcoholic liver disease, alcohol dependence, and alcohol withdrawal delirium. Laboratory data collected from the patients included maximum temperature, WBC count, CRP, and minimum serum albumin (ALB) within 1 week of presentation. Imaging studies were used to evaluate the presence of epidural abscesses and abscesses around the iliopsoas muscle, the site of vertebral infection, and the number of infected intervertebral discs. If infection was found in only one vertebral body and not in any disc, the number of discs was recorded as one. The presence of infective endocarditis (IE) and antibiotic treatment prior to culture submission were also assessed. For cases in which antimicrobials were administered before blood culture, the type of antimicrobial agent, mode of administration (oral or intravenous), and duration of antibiotics before blood culture tests were reviewed. Patients who underwent disc biopsy (CT-guided or surgical) were investigated for the association between culture results and whether antibiotics were administered before biopsy, the duration of administration, and the duration of antibiotic interruption before culture. Typically, at our hospital, antibiotics are discontinued for several days, if feasible, before biopsy.
All patients were categorized into culture-positive and culture-negative groups based on whether the causative microorganism was identified. Additionally, patients with blood culture tests were categorized into blood culture (BC)-positive and BC-negative groups. This study analyzed factors affecting causative microorganism identification by comparing these groups. The impact of iliopsoas abscesses and epidural abscesses on inflammatory findings and culture results was investigated. A comparison was made between cases with both abscesses and those without these abscesses or with only one type in terms of inflammatory markers, including CRP, WBC count, and temperature, as well as the rate of pathogen identification.
Data Analysis
SPSS for Windows, Version 25 (SPSS Inc, Chicago, IL, USA) was used for data description and analysis. Student’s t test was performed for continuous normally distributed data, while the Mann–Whitney U test was performed for non-normally distributed data. For categorical variables, either the chi-square test or the Fisher-Freeman-Halton Exact test was used. Multivariate logistic regression analyses were used to investigate the clinical variables related to the identification of causative microorganisms. All clinical variables found to be statistically significant in the univariate analysis were included in the multivariate analysis. Multicollinearity was assessed by examining the variance inflation factor (VIF) for standard error of regression coefficients, where a VIF greater than five indicated high multicollinearity between the predictors. Statistical significance was set at P < 0.05.
Results
Patients Demographics
Patient Demographics.
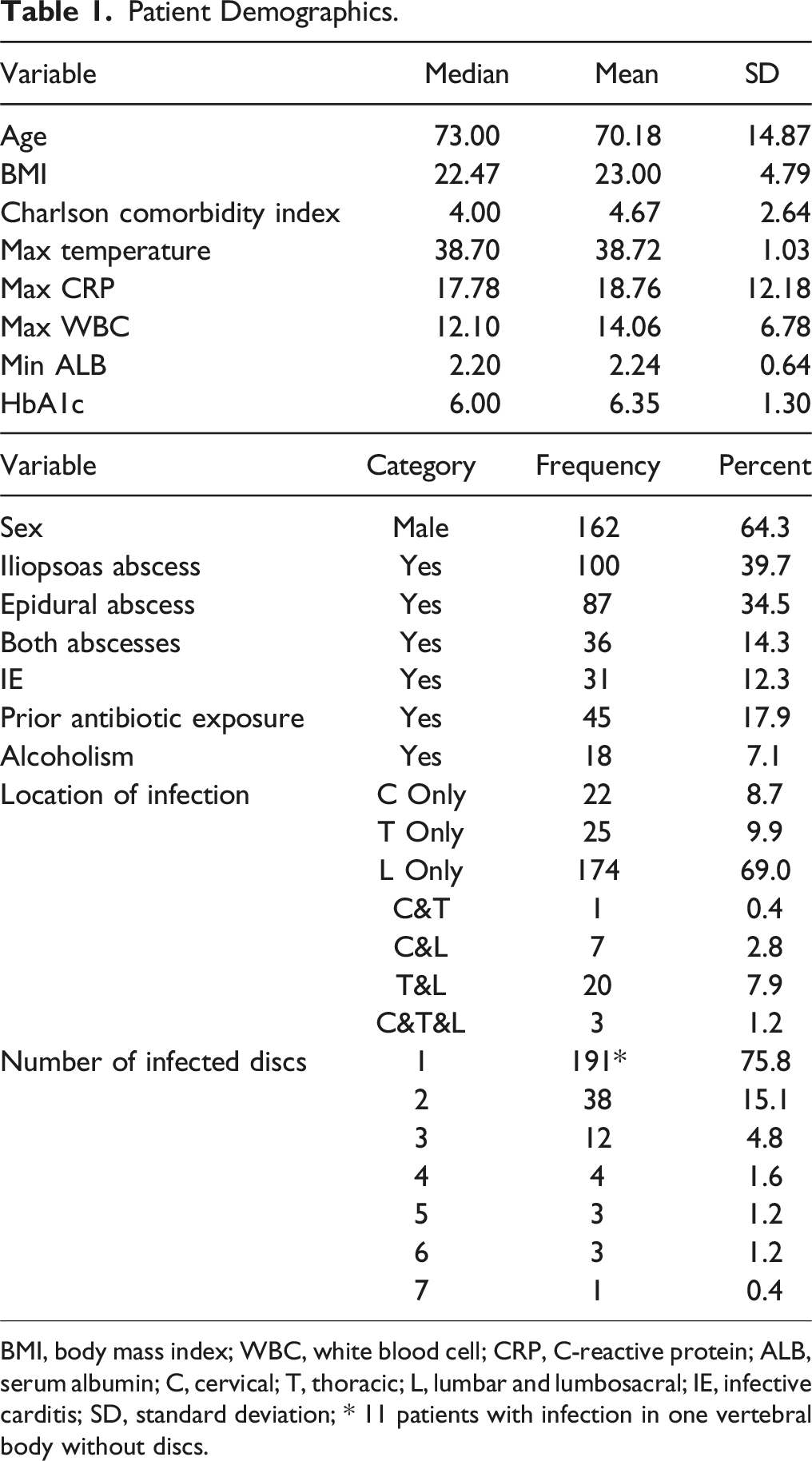
BMI, body mass index; WBC, white blood cell; CRP, C-reactive protein; ALB, serum albumin; C, cervical; T, thoracic; L, lumbar and lumbosacral; IE, infective carditis; SD, standard deviation; * 11 patients with infection in one vertebral body without discs.
Details of the Charlson Comorbidity Index.
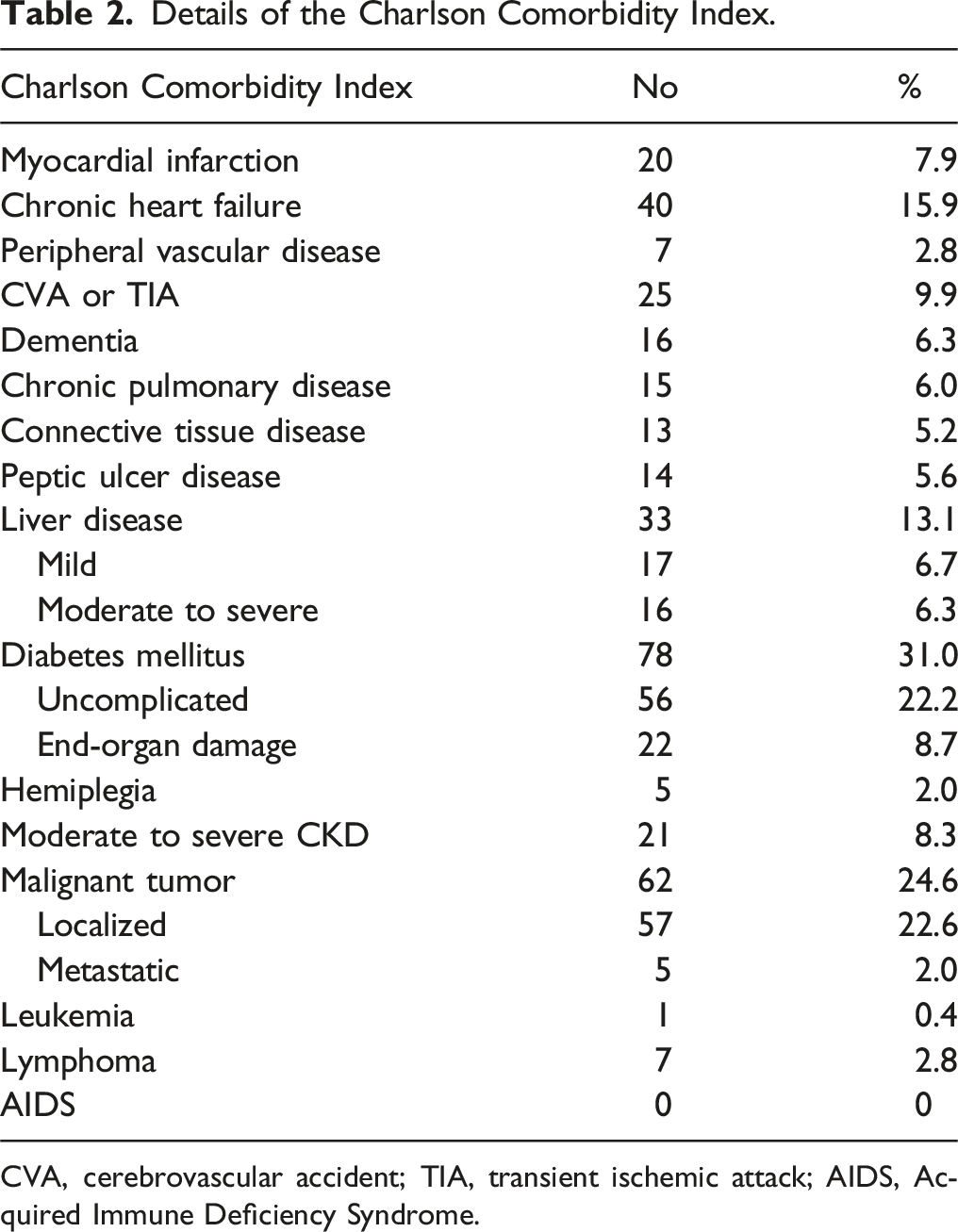
CVA, cerebrovascular accident; TIA, transient ischemic attack; AIDS, Acquired Immune Deficiency Syndrome.
Microbiological Findings
Among the 252 patients with VO, two patients did not have blood cultures but had positive intraoperative specimens. Blood cultures were performed for 250 patients, with 184 (73.6%) yielding positive results. Among the remaining 66 patients, seven of 14 were positive on CT-guided drainage, five of 21 on disc biopsy, and nine of 16 on intraoperative specimens, one of whom was positive on both CT-guided drainage and intraoperative specimens. Additionally, two patients were biologically identified through urine culture, and the other two through cerebrospinal fluid culture. Causative microorganisms remained unidentified in 42 patients (16.7 %) (Figure 1). Culture test flowchart for all patients. VO indicates vertebral osteomyelitis; * 1 positive with both CT-guided drainage and intraoperative specimen; ** 1 negative with disc biopsy.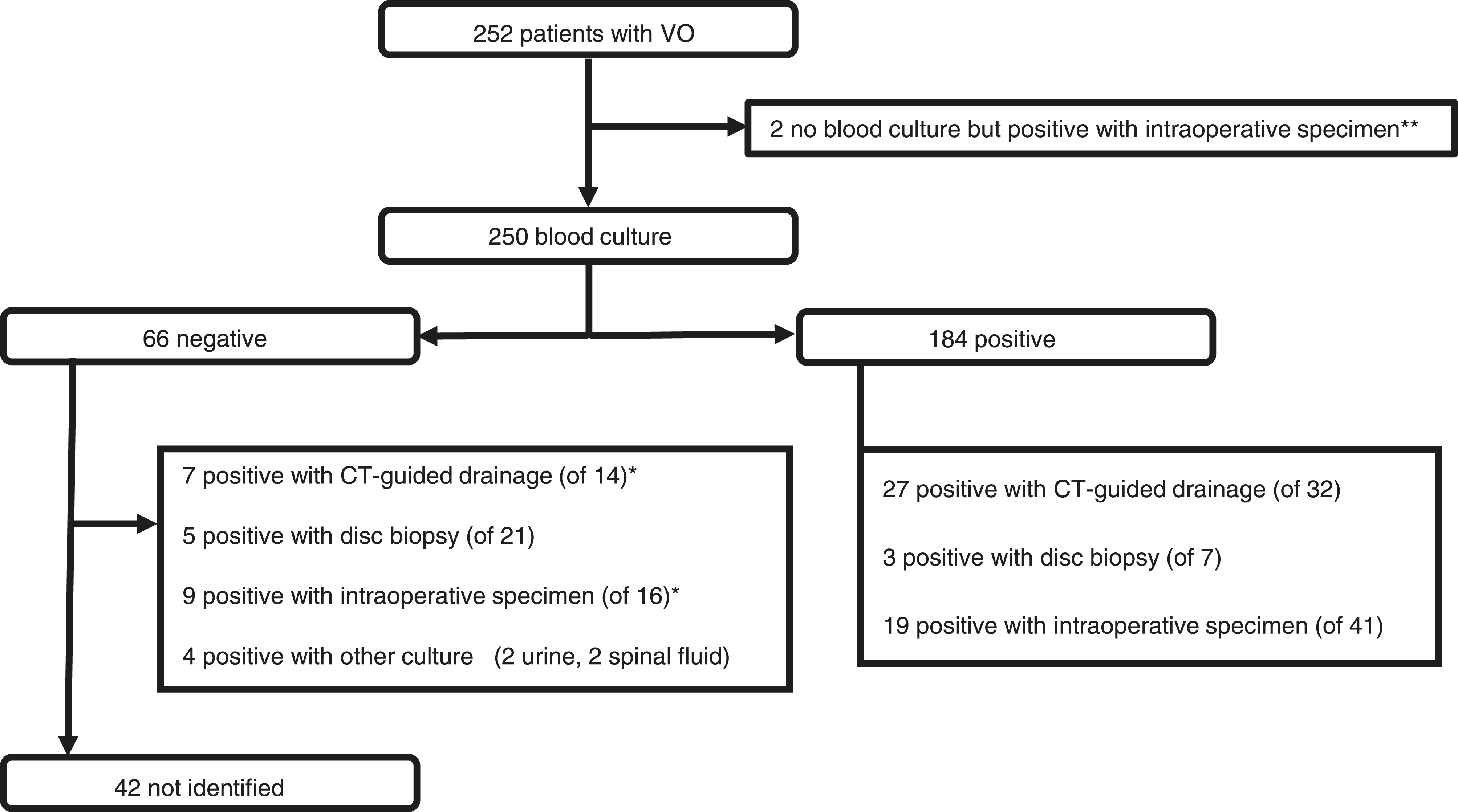
Details of Culture Methods and Identified Pathogens.
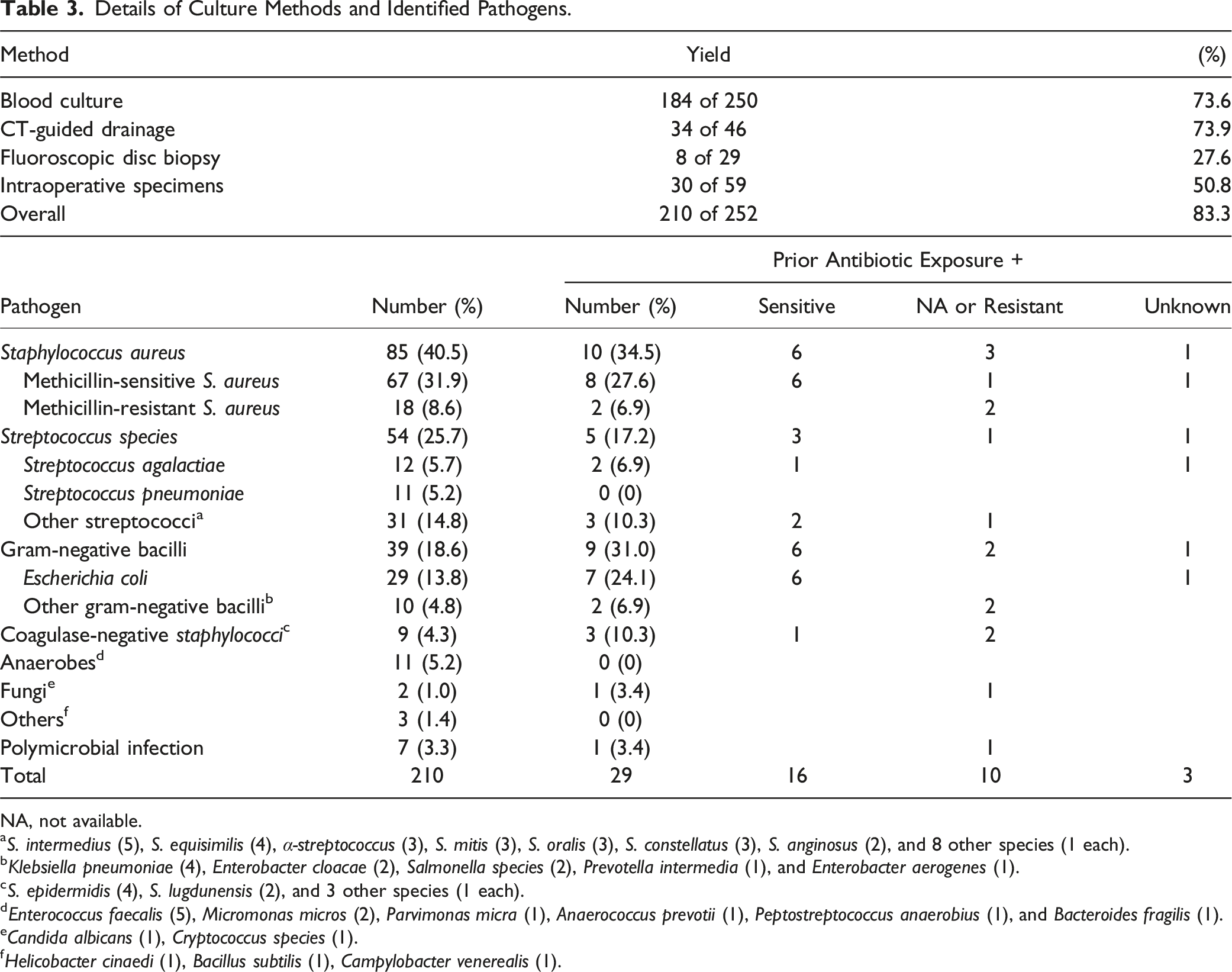
NA, not available.
aS. intermedius (5), S. equisimilis (4), α-streptococcus (3), S. mitis (3), S. oralis (3), S. constellatus (3), S. anginosus (2), and 8 other species (1 each).
bKlebsiella pneumoniae (4), Enterobacter cloacae (2), Salmonella species (2), Prevotella intermedia (1), and Enterobacter aerogenes (1).
cS. epidermidis (4), S. lugdunensis (2), and 3 other species (1 each).
dEnterococcus faecalis (5), Micromonas micros (2), Parvimonas micra (1), Anaerococcus prevotii (1), Peptostreptococcus anaerobius (1), and Bacteroides fragilis (1).
eCandida albicans (1), Cryptococcus species (1).
fHelicobacter cinaedi (1), Bacillus subtilis (1), Campylobacter venerealis (1).
Factors Affecting the Identification of Causative Microorganisms in all Methods
Summary of Univariate and Multivariate Analyses for all Culture Methods.
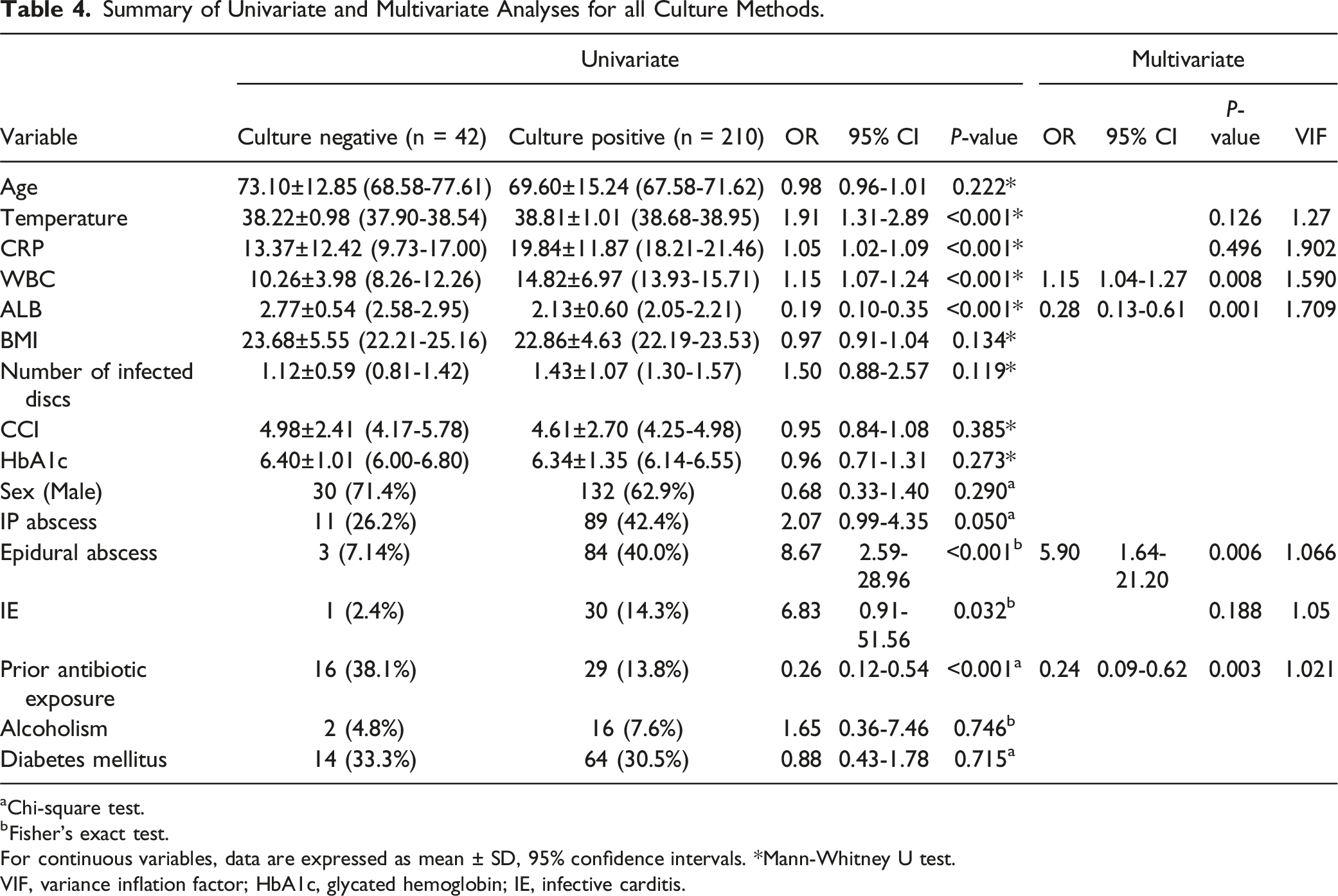
aChi-square test.
bFisher’s exact test.
For continuous variables, data are expressed as mean ± SD, 95% confidence intervals. *Mann-Whitney U test.
VIF, variance inflation factor; HbA1c, glycated hemoglobin; IE, infective carditis.
Factors Affecting the Identification of Causative Microorganisms in Blood Culture
Summary of Univariate and Multivariate Analyses of Blood Culture Test Results.
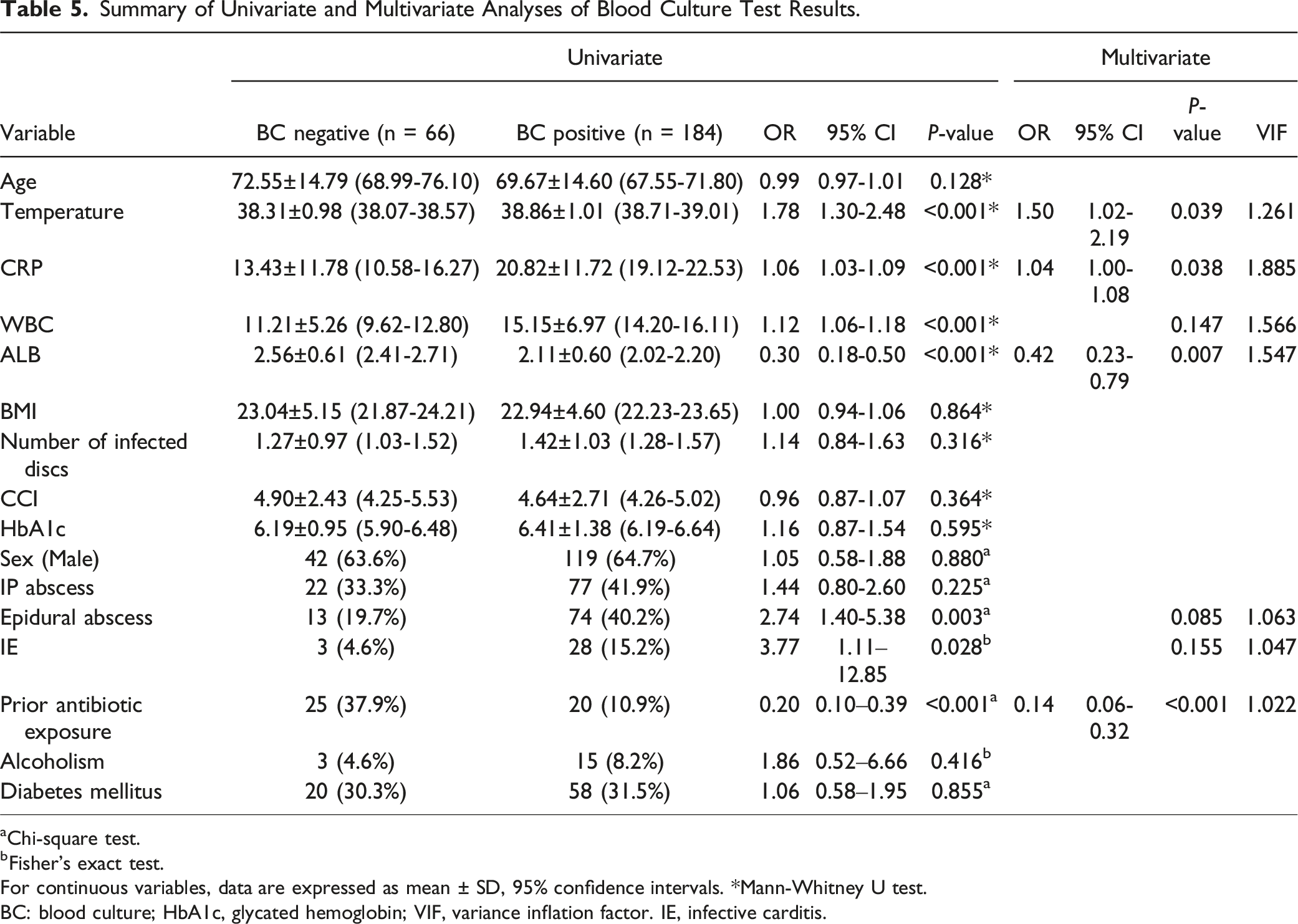
aChi-square test.
bFisher’s exact test.
For continuous variables, data are expressed as mean ± SD, 95% confidence intervals. *Mann-Whitney U test.
BC: blood culture; HbA1c, glycated hemoglobin; VIF, variance inflation factor. IE, infective carditis.
Details of Antibiotic Treatment before Culture
Impact of Prior Antibiotic Exposure on Culture Yield of Blood Culture and Biopsy, Including Fluoroscopic Disc Biopsy, CT-Guided Drainage, and Intraoperative Specimen.
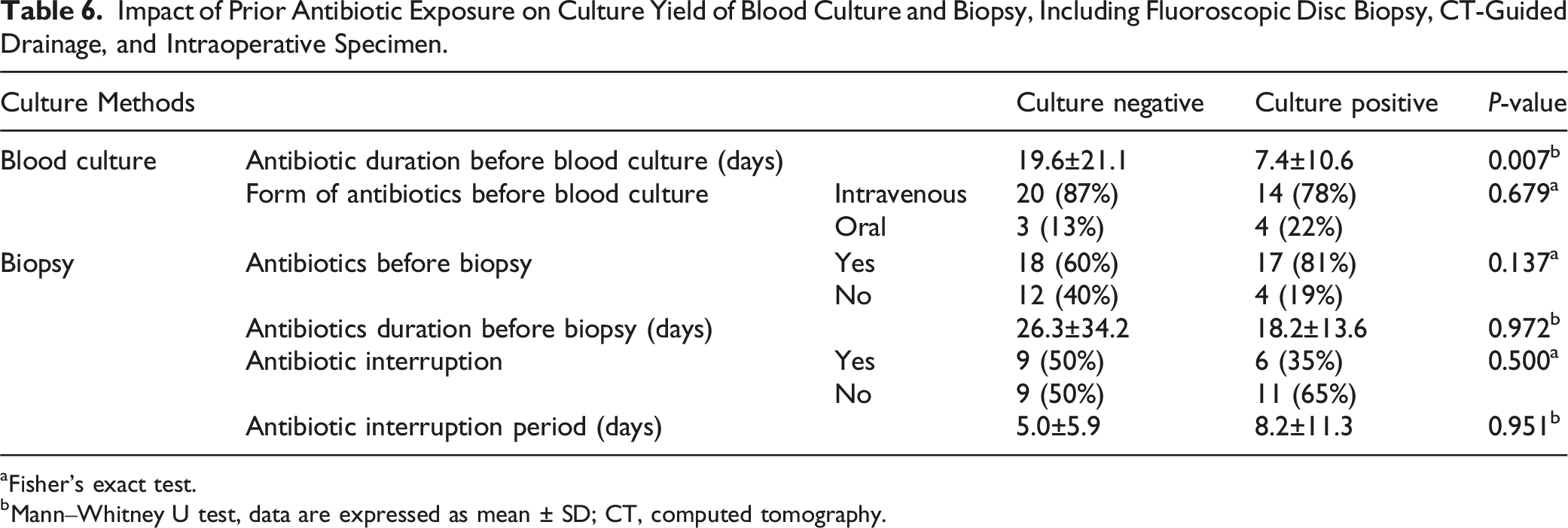
aFisher’s exact test.
bMann‒Whitney U test, data are expressed as mean ± SD; CT, computed tomography.
The administration of antibiotics before performing blood culture was conducted via intravenous infusion in 34 patients and orally in seven patients, yielding a positive outcome in 14 and four patients, respectively, with no statistically significant difference (P = 0.679). In cases where blood cultures were negative or not performed, a total of 51 biopsies were conducted (disc biopsy: 21, CT-guided drainage: 14, surgical biopsy: 16) (Figure 1). Antibiotic administration before the biopsy was performed in 35 cases. The mean duration of antibiotic administration before biopsy was 18.2 days in the culture-positive group and 26.3 days in the culture-negative group. Neither the presence of antibiotics before biopsy nor their duration significantly impacts pathogen identification (P = 0.137, 0.972). In 15 of the 35 cases, antibiotic interruption preceded biopsy, with a duration of 8.2 days in the culture-positive group and 5.0 days in the culture-negative group. Neither the occurrence nor the duration of antibiotic interruption significantly impacts pathogen identification (P = 0.500, 0.951).
Association of Epidural and Iliopsoas Muscle Abscesses with Inflammatory Findings and Culture Results
Association of Epidural and Iliopsoas Muscle Abscesses With Inflammatory Findings and Culture Results.
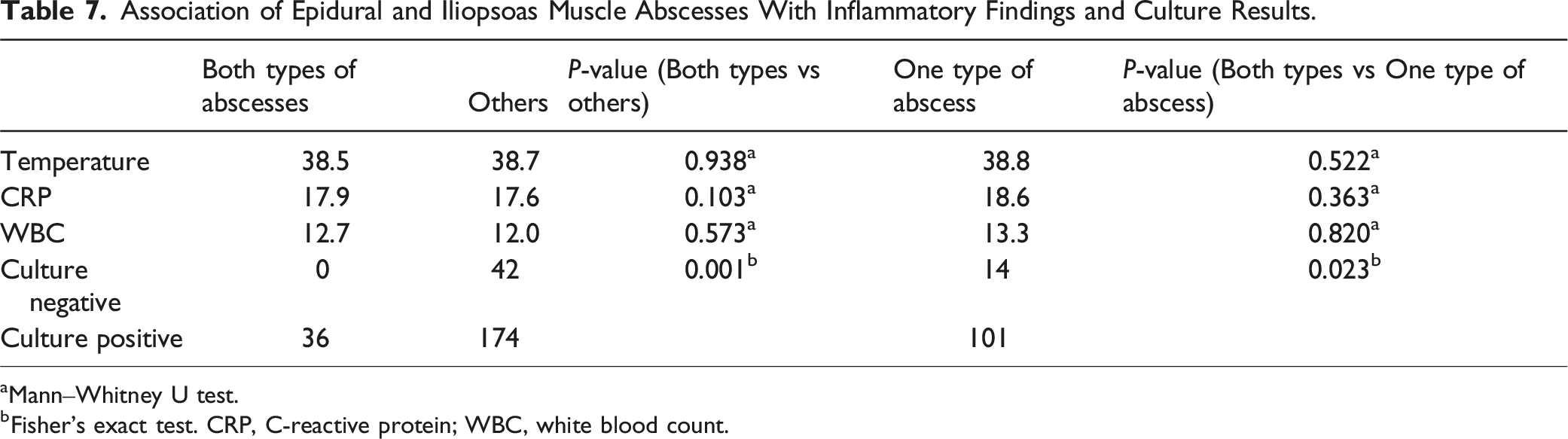
aMann‒Whitney U test.
bFisher’s exact test. CRP, C-reactive protein; WBC, white blood count.
Discussion
This study revealed an 83% identification rate for VO-causing organisms, with blood cultures being the most commonly used method. Additionally, CT-guided drainage, fluoroscopic disc biopsy, and intraoperative specimens collectively increased the identification rate by 10%. The identification of causative microorganisms was influenced by the WBC count, serum albumin level, presence of epidural abscess, and prior antibiotic exposure, with the latter being the most significant risk factor for negative results.
Moreover, our study indicated that blood cultures were performed in 250 of 252 patients (99.2%), yielding a diagnostic rate of 73.2%. This rate aligns with or exceeds findings reported in a previous systematic review, where blood cultures were performed in 91% (range, 43%–100%) of cases with a yield of 58% (range, 30%–78%). 9 Since the yield of blood culture accounts for most of the overall detection rate, blood culture should be performed whenever VO is suspected.
The yield of percutaneous disc biopsy varies widely, as systematic reviews indicate yields ranging from 19% to 92%.13,14 In this study, the yield of percutaneous disc biopsy under fluoroscopy was 27.6%, which is relatively low compared to systematic review results. This lower yield may be attributed to the selective use of disc biopsies in patients with negative blood cultures at our hospital, contrasting with hospitals where disc biopsies are routinely performed. Conversely, the yield of CT-guided drainage in our study was 73.9%, which is comparable to or higher than previous reports (range, 35%-69%).8,13,15,16 However, the yield of intraoperative specimens in this study was 50.8%, which is lower than that of open biopsy in previous studies (range, 70%-81%).8,13,17 Our hospital’s practice of performing CT-guided drainage immediately after diagnosis of VO, while surgery is often delayed until after several weeks of antibiotic treatment for spinal instability and neurological symptoms, may contribute to the lower culture positivity rate of surgical specimens.
A previous systematic review identified S. aureus as the most commonly isolated organism, accounting for 32%-67% of cases, followed by Streptococcus species (0%-24%). 9 Our study aligns with these findings, with S. aureus accounting for 40.5% and Streptococcus species for 25.7%. E. coli emerged as the most predominant etiological agent among the Gram-negative bacilli in this study, as described in a previous review. 9 Interestingly, our findings suggest that prior antibiotic use may slightly decrease the identification of S. aureus and Streptococcus species while increasing the identification of E. coli, possibly influenced by pre-admission antibiotic prescriptions. However, antibiotics used varied widely and were often broad-spectrum. Most of them were effective against Methicillin-sensitive Staphylococcus aureus, non-resistant Streptococcus species, and non-resistant Gram-negative bacilli. Among the 29 patients that received antibiotic treatment, 16 were treated with antibiotics to which the identified organisms were sensitive, indicating that pathogen identification may be possible even when antibiotics susceptible to the causative organisms are administered.
Inflammatory signs and markers, including temperature, CRP, and WBC count, were lower in the negative culture groups, consistent with several reports suggesting that lower pathogenic microorganism inoculation in the culture-negative group may lead to reduced inflammatory signs and markers compared to the culture-positive group.10,18-21 These findings imply that conducting blood culture tests during periods of severe inflammation may increase the number of positive cultures. Epidural abscess emerged as a significant predictor of positive outcomes, likely because patients with epidural abscesses often present with more severe infections, leading to a higher likelihood of being culture-positive. Additionally, these patients are more prone to neurological deficits due to spinal cord compression, 7 necessitating surgery for which intraoperative specimens can be easily obtained.
Both iliopsoas and epidural abscesses were present in 36 patients (14.3%), and although the inflammatory response was not higher in patients with two abscesses, the pathogen identification rate was nevertheless significantly higher in these patients, at 100%. This may be due to the higher bacterial levels in patients with both abscesses and the greater availability of CT-guided drainage and intraoperative specimen collection.
Prior antibiotic exposure emerged as the strongest risk factor for negative outcomes (OR = 0.24 for all cultures, 0.14 for blood cultures). Towns et al stated that prior antibiotic administration before the first sampling and inadequate sampling volume 22 are critical factors hindering microorganism identification in patients with bloodstream infections. While some studies reported no substantial differences in antibiotic treatment before culture to identify the causative organism, the total number of patients was 73 and 129, respectively, which was much smaller than that in our study.7,17 Our study encompassing 252 patients from a single hospital, stands out for its robust sample size, contributing significantly to the observed differences. Previous meta-analyses have indicated that prior antibiotic treatment has a limited impact on the yield of fluoroscopy- and CT-guided biopsies.13,23 Therefore, image-guided biopsy should not be delayed even in patients with VO who have received antibiotics. Maamari et al 11 recommended a minimum antibiotic-free period of 4 days to enhance the yield of image-guided biopsy after antibiotic treatment and suggested repeat biopsies at least 3 days apart.
To our knowledge, this is the first study to investigate in detail antibiotic treatment before culture submission in pyogenic spondylitis. A longer duration of antibiotic administration before blood culture was significantly associated with negative blood culture results. However, causative organisms could be identified in some cases even when sensitive antibiotics were administered. In cases where a biopsy was performed, the presence or absence of antibiotics before the biopsy, the duration of antibiotic administration, whether antibiotic use was interrupted, or the duration of interruption showed no association with the culture results. These findings may be influenced by the small sample size in cases where a biopsy was performed, and further analysis with a larger sample is warranted.
In the present study, lower serum albumin levels were significantly associated with culture positivity. To the best of our knowledge, there are no previous reports on the relationship between VO and serum albumin levels. Patients with low serum albumin levels were considered malnourished. According to Yamamoto et al, hypoalbuminemia is associated with a prolonged hospital stay due to surgical site infections, 24 suggesting that it complicates the suppression of infection. These findings indicate that hypoalbuminemia may impede the suppression of infection and increase microorganism count in the body, making it easier for cultures to be positive.
This study has some limitations. Firstly, being a single-center study, local microbial patterns and clinical practices may differ in other regions. Secondly, although we analyzed predictors in a relatively large sample of 252 patients with VO, the number might still be insufficient to identify minor predictors influencing culture results. Lastly, due to the retrospective nature of the study, some concerns have been raised regarding the lack of a standardized protocol for culture methods; therefore, not all culture tests were performed. Consequently, comparing the effectiveness of different culture tests becomes challenging.
Conclusion
The overall identification rate for causative organisms in VO was 83.3%., with blood culture at 73.6%. Our analysis revealed that laboratory findings indicating a high inflammatory response (elevated WBC and CRP levels), lower serum albumin levels, epidural abscess presence, and no prior antibiotic exposure were significant predictors of positive culture results. A shorter duration of antibiotic administration was associated with a higher likelihood of positive blood culture results. Conducting blood cultures in the presence of high inflammation levels can improve microorganism identification rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Device Status/Drug Statement
The device in this manuscript is FDA-approved or approved by a corresponding national agency for this indication.