
Abstract
Study Design
Retrospective cohort study.
Objective
Limited clinical literature addresses potential differences in fusion features between Oblique lumbar interbody fusion (OLIF) and transforaminal lumbar interbody fusion (TLIF). We observed that in OLIF, there are many cases with the appearance of extra-vertebral bone bridges (EVB), a phenomenon distinct from traditional TLIF fusion. This study aims to compare fusion rates, cage subsidence, and fusion features among OLIF stand-alone (OLIF-SA), OLIF with posterior pedicle screw fixation (OLIF-PS), and TLIF.
Methods
We retrospectively analyzed 198 patients (311 levels) undergoing OLIF-SA, OLIF-PS, or TLIF from July 2017 to June 2021. We assessed patient-reported outcomes, cage subsidence, fusion rate, and fusion features on CT scans.
Results
The study included 64 OLIF-SA patients (102 levels), 60 OLIF-PS patients (99 levels), and 74 TLIF patients (110 levels). Cage settling rates were 33.3% (OLIF-SA), 17.2% (OLIF-PS), and 32.8% (TLIF), with significant differences between OLIF-PS and TLIF (P < 0.05). Cage subsidence rates showed no significant difference: 11.8% (OLIF-SA), 9.1% (OLIF-PS), and 12.7% (TLIF) (P > 0.05). Fusion rates were 100% (OLIF-SA), 97.0% (OLIF-PS), and 96.4% (TLIF) (P = 0.167). Lateral fusion rates significantly differed: 49.0% (OLIF-SA), 30.3% (OLIF-PS), and 10.9% (TLIF) (P < 0.001). Preoperative osteophytes strongly promote lateral fusion (P < 0.001). VAS and ODI scores improved significantly post-surgery (P < 0.01).
Conclusions
OLIF-SA, OLIF-PS, and TLIF surgeries show satisfactory results with comparable fusion rates. Notably, distinctive differences exist in fusion features between OLIF and TLIF surgeries, with lateral fusion more prevalent in OLIF, particularly in OLIF-SA surgeries.
Keywords
Introduction
Literature reports suggest that the annual incidence rate of lumbar spine-related diseases ranges between 2.4%–5.7%. 1 It is estimated that by 2050, the prevalence of lumbar spine-related diseases will reach 843 million. 2
Lumbar spinal fusion is currently the main surgical intervention for lumbar spine diseases. Procedures are classified based on their surgical approaches. 3
In patients undergoing transforaminal lumbar interbody fusion (TLIF) surgery, bone bridge primarily is confined in the central region of the intervertebral space. While literature reports note the occurrence of the ‘sentinel sign’ after TLIF surgery, its incidence is relatively low.4-6 During later follow-ups in oblique lumbar interbody fusion (OLIF), we have noted an intriguing phenomenon that early extra-vertebral bone bridges (EVB) formation occurs in a considerable number of patients. We believe this phenomenon may signify a novel fusion mechanism distinct from TLIF approaches.
Currently, there is no literature reporting the differences in fusion features among fusion procedures. We conducted a retrospective analysis of OLIF stand-alone (OLIF-SA), OLIF with posterior screw fixation (OLIF-PS), and TLIF surgeries performed in authors’ hospital from July 2017 to June 2021 to assess: 1. Whether there are differences in fusion and subsidence rates among the three surgical methods; 2. Whether the OLIF procedure exhibits distinctive fusion features compared with traditional TLIF.
Materials and Methods
Patient Population
All procedures complied with relevant laws and institutional guidelines approved by the institutional review board. This study was approved by the ethics committee of the authors’ hospital (Approval number: 2023-0676) with a waiver of informed consent from patients due to its retrospective feature.
Patients who underwent OLIF or TLIF surgery performed by a senior surgeon at the authors’ hospital between July 2017 and June 2021 were retrospectively reviewed. They were categorized into three groups: OLIF-SA, OLIF-PS, and TLIF.
Inclusion Criteria
The inclusion criteria were: 1. Age between 18 and 80 years; 2. Surgeries were performed between the 1st and 5th lumbar level after conservative treatment failed; 3. Complete preoperative X-rays, CT, MRI, X-ray immediately postoperative, at one, three months, and six months, and CT scans postoperative one year; 4. Patients had normal bone mineral density (BMD) (T score > −1.0)
Exclusion Criteria
The exclusion criteria were: 1. Use of drugs that affect bone healing (steroid and bisphosphonate); 2. Revision surgery in the same segment; 3. Intervertebral fusion with non-cage methods, such as bulk autogenous iliac bone; 4. OLIF with additional anterior or lateral screw-rod fixation.
Surgical Technique
OLIF-SA
After general anesthesia, the patient was typically placed in the right lateral decubitus position. An approximately 4 cm longitudinal incision was made at the midpoint of the target level. The external, internal obdominis oblique muscle, and transverse abdominis muscle were bluntly separated. After reaching the retroperitoneal space, the abdominal organs and psoas major muscles were pulled ventrally and dorsally, respectively. With C-arm fluoroscopy confirming the correct level, a sharp knife cut the ipsilateral annulus fibrosus (AF) and removed the nucleus pulposus (NP) with forceps. The endplate cartilage was treated with reamers and scrapers. The trail was inserted parallelly into the intervertebral space. The head of the trail touched the contralateral epiphyseal ring to release the contralateral AF, as confirmed by fluoroscopy. A demineralized bone matrix (DBM)-packed poly-ether-ether-ketone (PEEK) cage of an appropriate size was implanted. Layer-by-layer sutures were completed.
OLIF-PS
The OLIF procedure was performed as described in the OLIF-SA section, using the same DBM-packed PEEK cage. Either one-stage (performed during the same general anesthesia session) or two-stage (performed on a subsequent day) posterior pedicle screw fixation with the monitoring of X-rays was performed through the Wiltse approach with the patient in the prone position.
TLIF
The patient was positioned prone after general anesthesia. The approach was performed via a midline incision one level below and above the target site. The affected facet joint was resected to expose the disc space and the affected root. After placement of the contralateral pedicular screws and rod, allowing distraction, a nearly complete discectomy was performed, and the endplates were scraped. A PEEK cage filled local autograft implanted. The screw-rod construct was completed with an anteroposterior and lateral fluoroscopy to confirm the cage and screw position.
Postoperative Treatment
All patients were encouraged to initiate ward ambulation one-day post-surgery with lumbar brace support for three months.
Demographic and Perioperative Data Collection
Demographic and perioperative data for patients were collected from medical records. Demographic data included age, gender, BMD, body mass index (BMI), and preoperative diagnosis. Perioperative variables comprised surgical level, operative time per segment, and estimated blood loss (EBL) per segment.
Patient-Reported Outcomes
Clinical outcomes were assessed both preoperatively and 12 months postoperatively using multiple questionnaires, including the Oswestry Disability Index (ODI, version 2), 7 and the visual analog scale (VAS) for back pain.
Radiographic Outcomes
A CT scan was conducted 12 months after the operation to assess the fusion status and cage subsidence. The CT scan was evaluated by three independent observers (provided in the supplemental materials).
Definition of Interbody Fusion
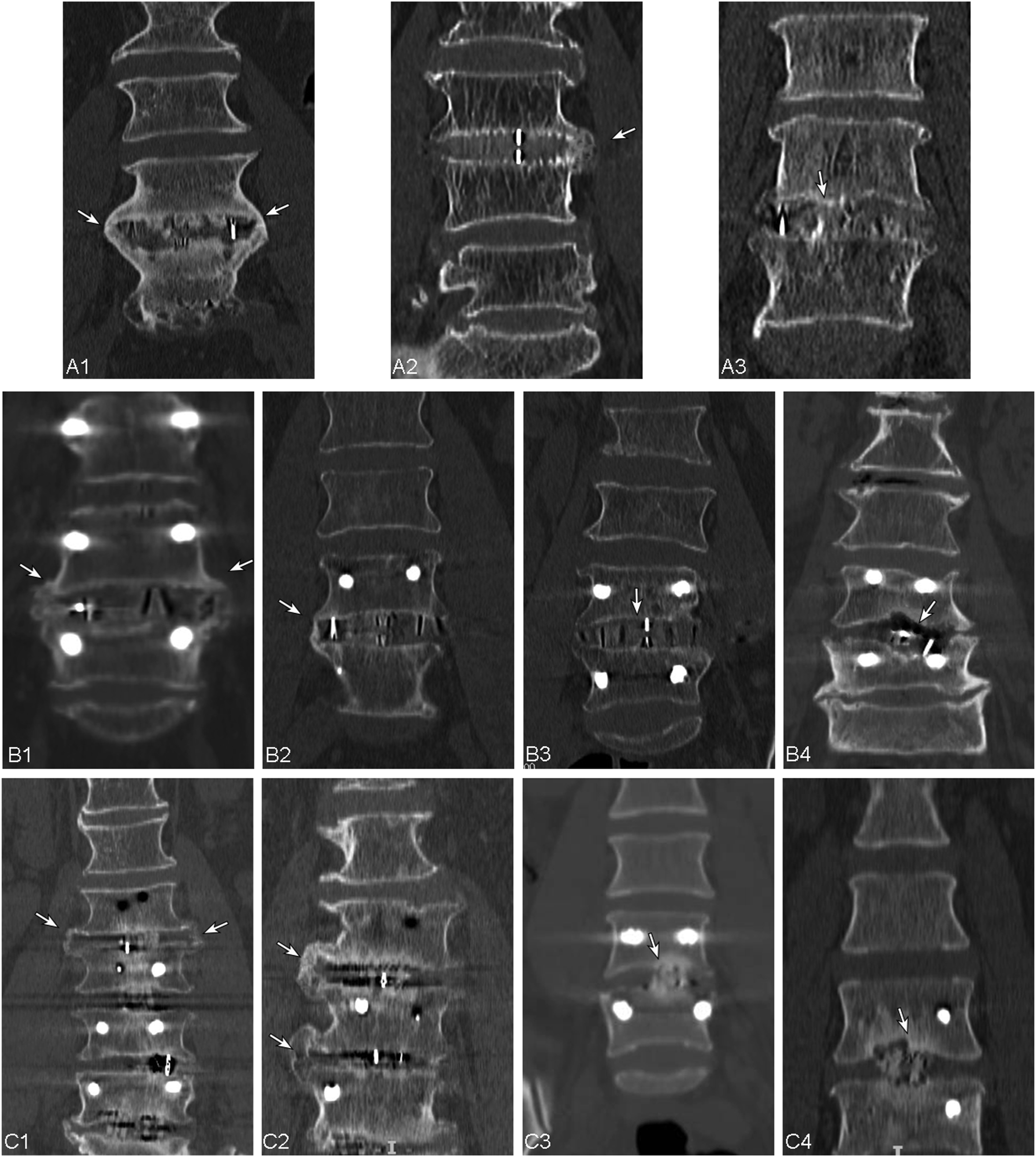
Interbody fusion was defined as follows (Figure 1): 1. Lateral fusion: A continuous bone bridge connection is observed on one or both sides, extending beyond the vertebral body in coronal CT scan at finally follow-up, with or without the formation of bone bridge in the center of the disc space. 2. Central fusion: Defined as Bridwell
8
grade 1 and 2 on CT scan. 3. No fusion: Defined as Bridwell
8
grade 3 and 4 on CT scan. Definition of lateral and central fusion using coronal CT scans of three surgeries. (A) OLIF-SA; (B) OLIF-PS; (C) TLIF. Lateral fusion: continuous EVBs are observed on one or both sides in coronal CT scans (indicated by white arrows in A1-2, B1-2, C1-2); Central fusion: continuous bone bridges connecting the upper and lower endplates in the center of the disc space in coronal CT scans (indicated by white arrows in A3, B3, C3); No fusion: lucency presents at the top or bottom of the graft (indicated by white arrows in B4, C4). OLIF-SA stands for oblique lumbar interbody fusion stand-alone; OLIF-PS, oblique lumbar interbody fusion with additional posterior pedicle screw fixation; TLIF, transforaminal lumbar interbody fusion; EVB, extra-vertebral body bone bridge.
Preoperative Osteophytes
Preoperative osteophytes are defined as those classified with a grade of 2 or higher
9
according to the criteria established by Nathan
10
(Figure 2). The location of these osteophytes within the operative segment is recorded, specifying whether they are present on the left side, right side, or both (left and right). Definition of preoperative osteophytes based on Nathan’s classification. (A) No osteophyte; (B) First-degree osteophytes, characterized by small points of initial hyperostosis; (C) Second-degree osteophytes, protruding horizontally from the vertebral body; (D) Third-degree osteophytes, forming a bird’s beak shape, curving toward the intervertebral disc; (E) Fourth-degree osteophytes, fusing adjacent vertebrae to form a bone bridge, thereby immobilizing the intervertebral joint. Osteophytes are highlighted with a white circle.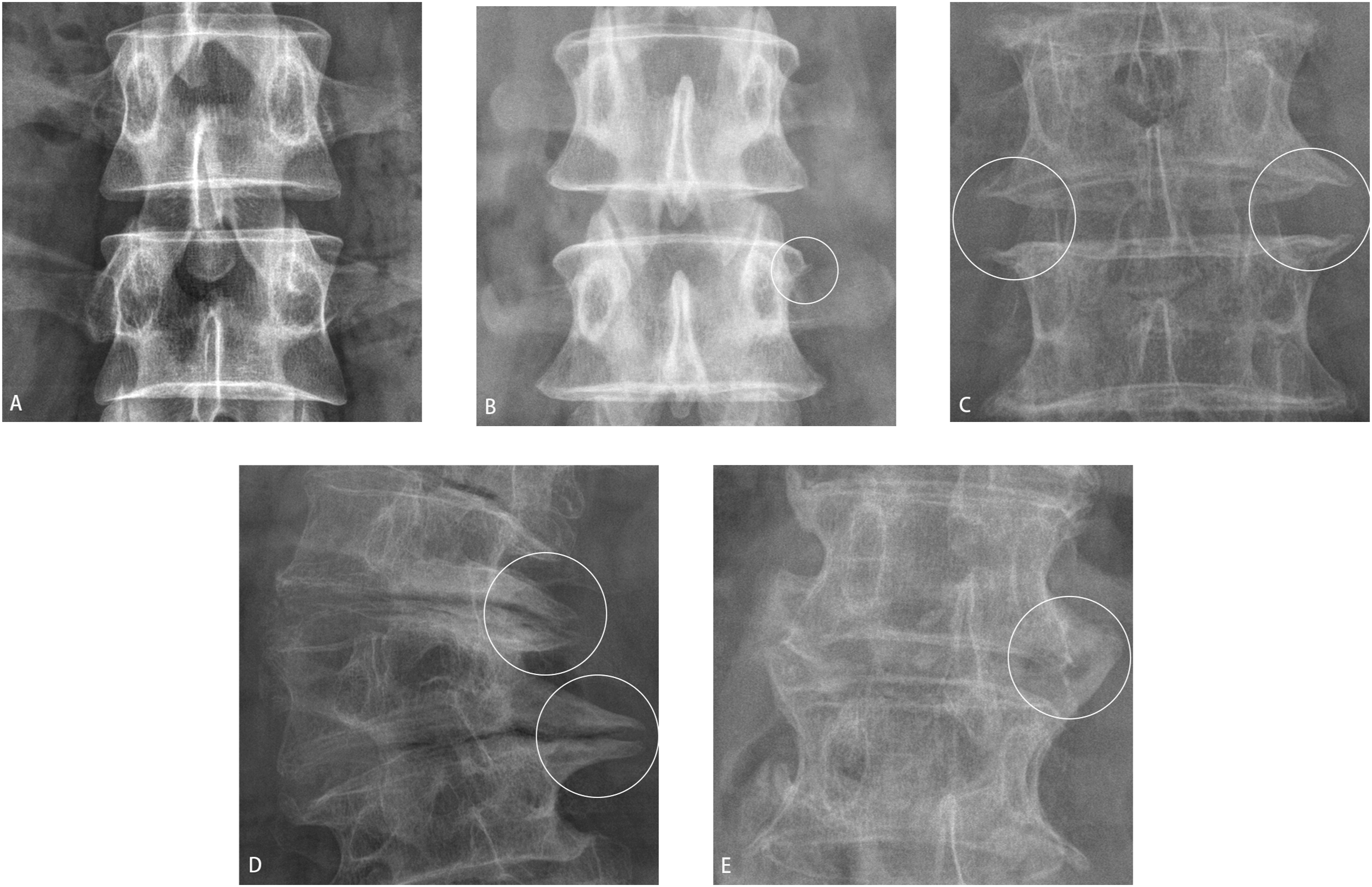
Cage Subsidence or Settling
Various standards for cage subsidence exist, 11 leading to different reported incidences in the literature. 12 A small amount of cage subsidence (eg, ≤2 mm) is considered a normal incorporation process of the cage to achieve better contact with both endplates, This typically presents with little to no clinical symptoms.13,14 Therefore, we define disc height collapse of ≤2 mm as cage settling and disc height collapse >2 mm as cage subsidence. Marchi et al. classified cage subsidence based on the percentage of height decrease. 15 We believe that employing this method for calculating cage subsidence requires a significant number of measurements, leading to considerable bias. We suggest using absolute values to classify the degree of cage subsidence. The degree of cage subsidence is categorized into three grades: grade 1 (>2 mm, ≤4 mm), grade 2 (>4 mm, ≤6 mm), and grade 3 (>6 mm).
Statistical Analysis
The normal distribution of parameters was compared among the groups using a t test and expressed as mean ± standard deviation. If there was a statistically significant difference between the groups, a post hoc comparison was performed using Bonferroni correction. The chi-square or Fisher exact test was used to compare data between the two or more groups. Intra-observer and interobserver reliability were evaluated using Fleiss or Cohen’s kappa test. Statistical analysis was performed using IBM SPSS Statistics ver. 29.0 (IBM Co., Armonk, NY, USA).
Results
In the study, a total of 353 patients met the inclusion criteria. Of these, 148 patients were excluded, leaving 205 patients for the study. During the follow-up of OLIF-SA cases, 7 patients underwent posterior fixation surgery due to cage migration or subsidence resulting in severe pain. All these occurred within 3 months after surgery. Subsequently, these patients excluded from OLIF-SA for further analysis. Consequently, the final number of patients included in each group was as follows: OLIF-SA, 64 cases; OLIF-PS, 60 cases; TLIF, 74 cases (Figure 3). Flow diagram of the patients. OLIF-SA, oblique lumbar interbody fusion stand-alone; OLIF-PS, oblique lumbar interbody fusion with additional posterior pedicle screw fixation; TLIF, transforaminal lumbar interbody fusion.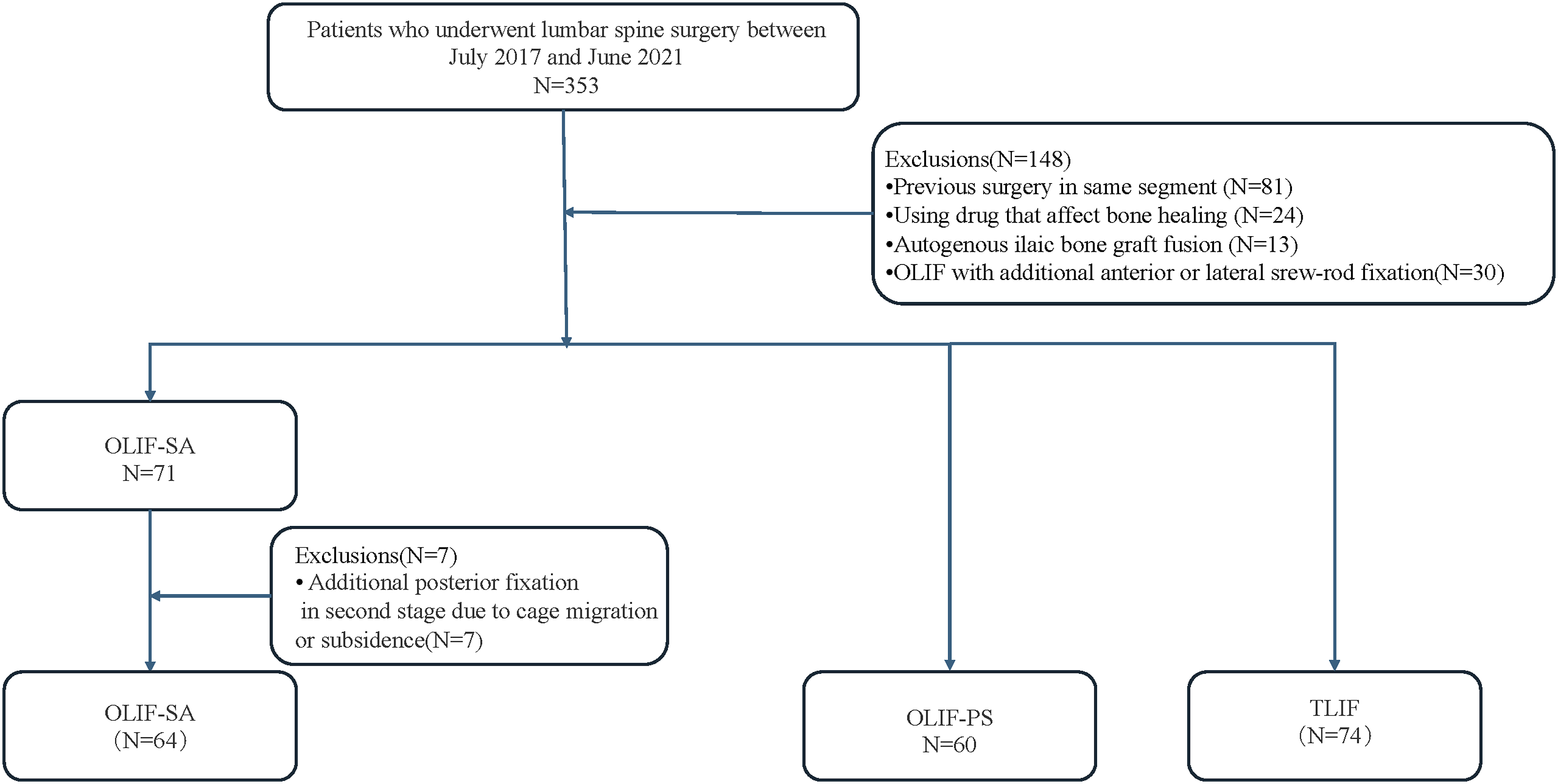
Demographic Data of Included Patients.
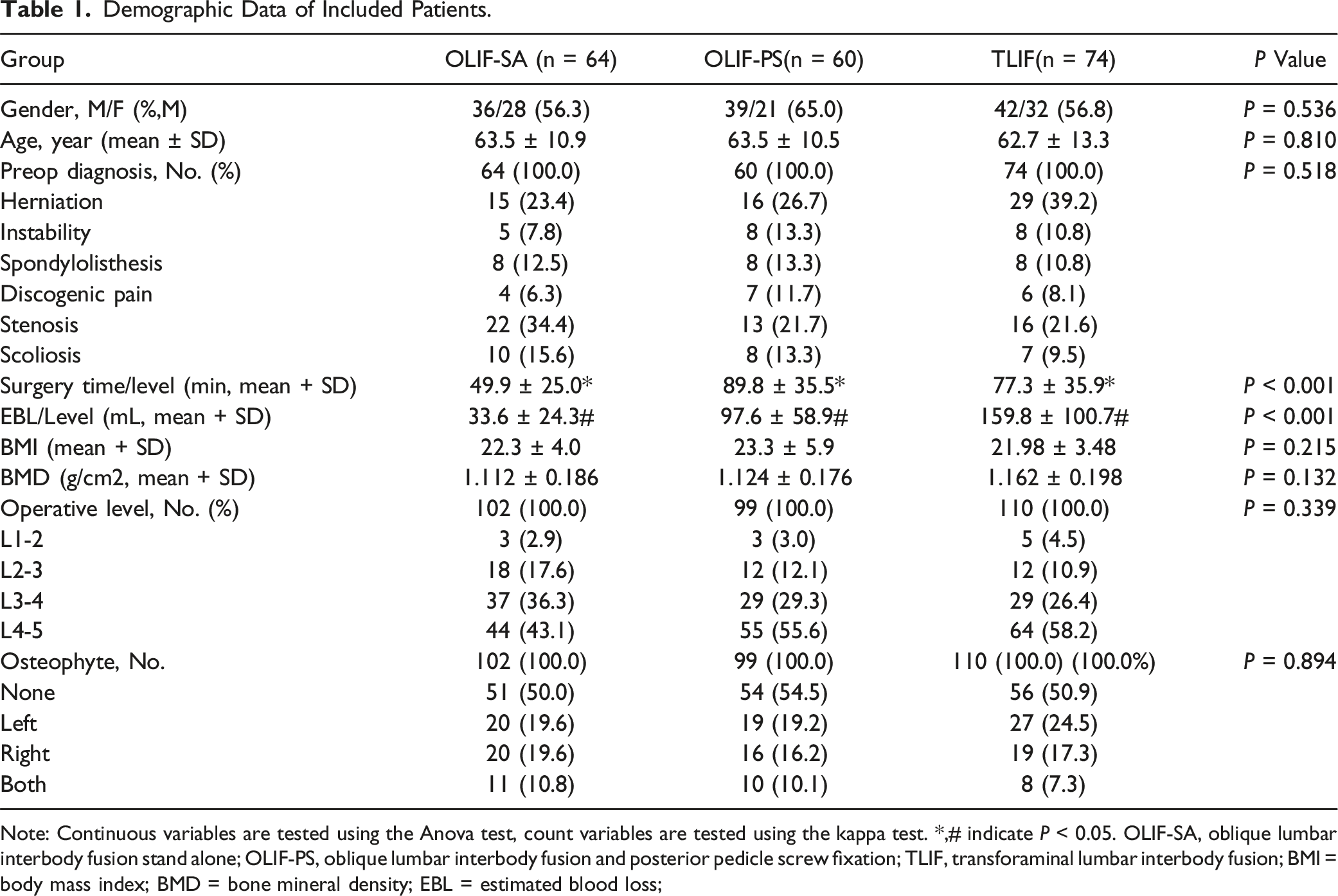
Note: Continuous variables are tested using the Anova test, count variables are tested using the kappa test. *,# indicate P < 0.05. OLIF-SA, oblique lumbar interbody fusion stand alone; OLIF-PS, oblique lumbar interbody fusion and posterior pedicle screw fixation; TLIF, transforaminal lumbar interbody fusion; BMI = body mass index; BMD = bone mineral density; EBL = estimated blood loss;
Overall Fusion Rate Among Groups.

Note: P value for Fisher exact test. OLIF-SA, oblique lumbar interbody fusion stand alone; OLIF-PS, oblique lumbar interbody fusion and posterior pedicle screw fixation; TLIF, transforaminal lumbar interbody fusion.
Differences in Fusion Features Among Groups.
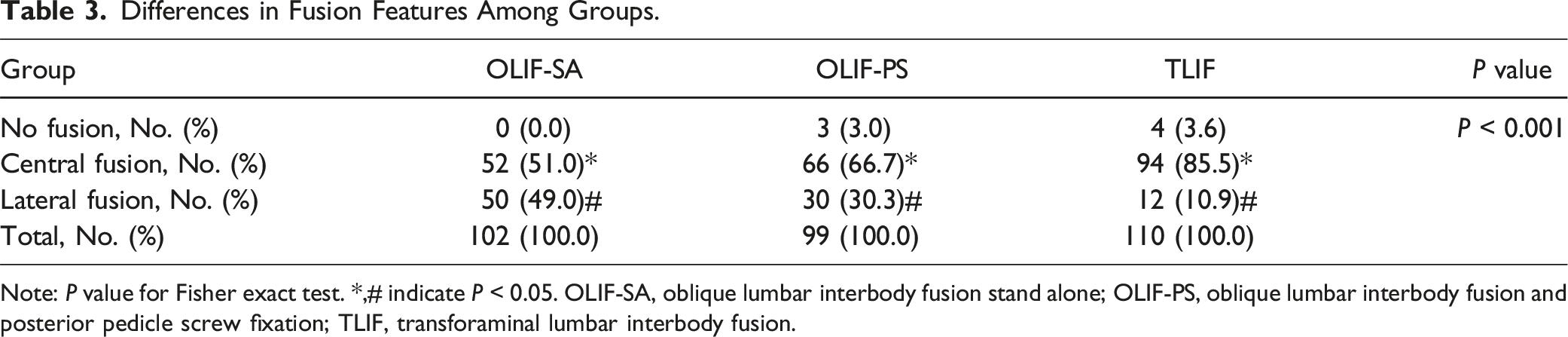
Note: P value for Fisher exact test. *,# indicate P < 0.05. OLIF-SA, oblique lumbar interbody fusion stand alone; OLIF-PS, oblique lumbar interbody fusion and posterior pedicle screw fixation; TLIF, transforaminal lumbar interbody fusion.
Bone Bridge Location Comparison Among Groups.
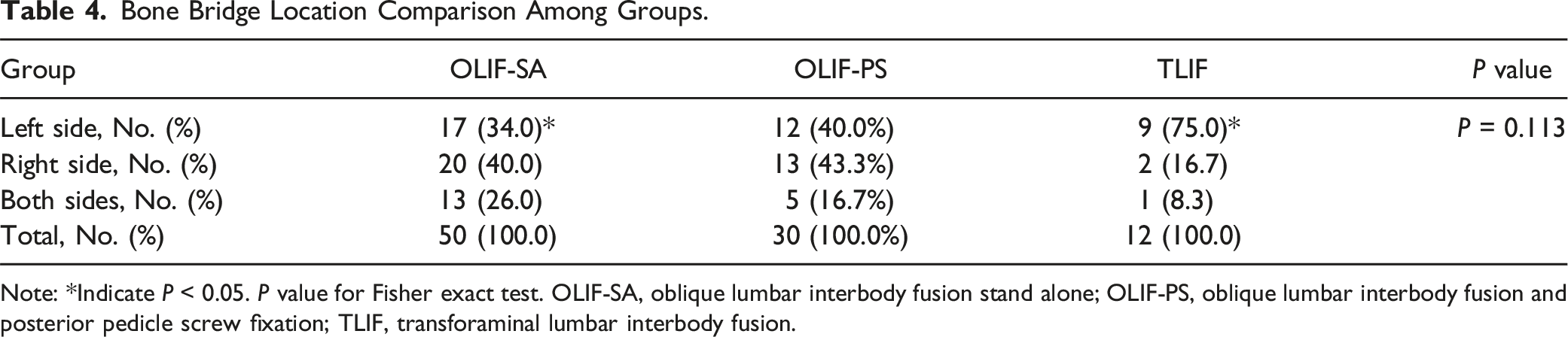
Note: *Indicate P < 0.05. P value for Fisher exact test. OLIF-SA, oblique lumbar interbody fusion stand alone; OLIF-PS, oblique lumbar interbody fusion and posterior pedicle screw fixation; TLIF, transforaminal lumbar interbody fusion.
Association Between Preoperative Osteophytes and Fusion Features Across Groups.
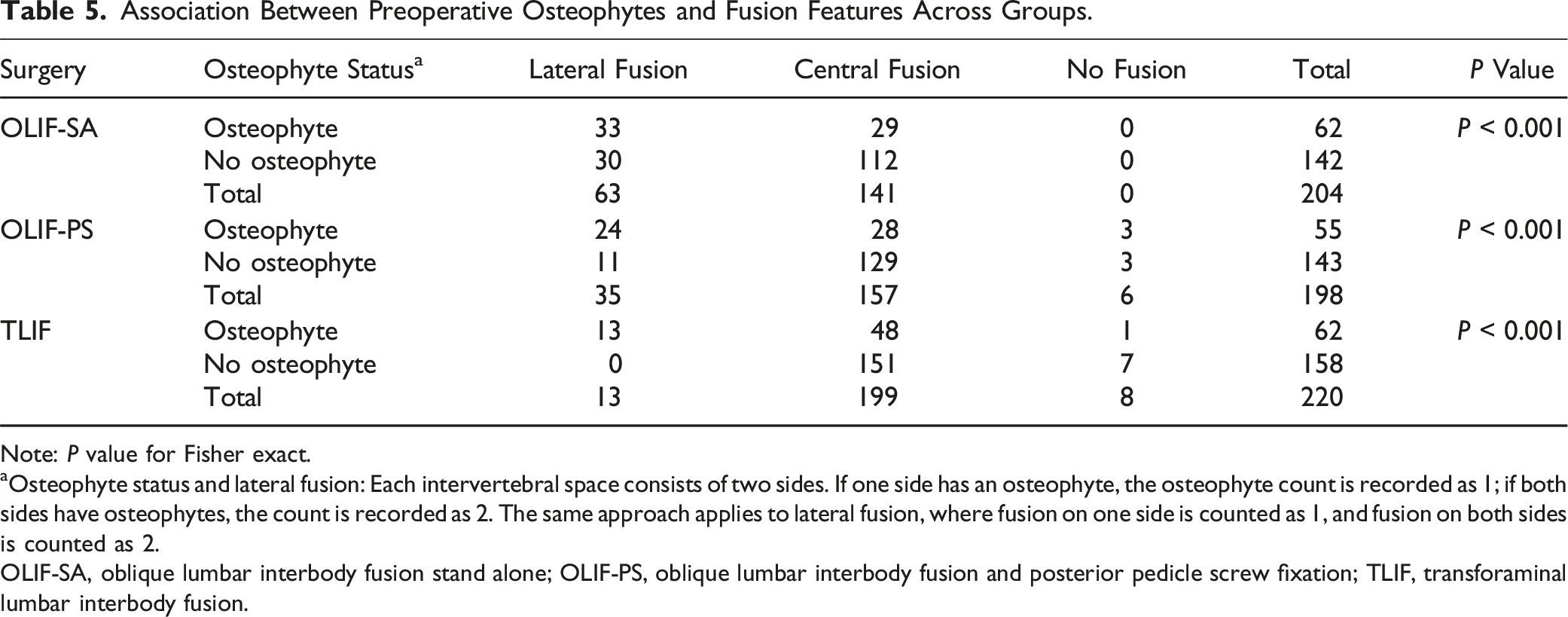
Note: P value for Fisher exact.
aOsteophyte status and lateral fusion: Each intervertebral space consists of two sides. If one side has an osteophyte, the osteophyte count is recorded as 1; if both sides have osteophytes, the count is recorded as 2. The same approach applies to lateral fusion, where fusion on one side is counted as 1, and fusion on both sides is counted as 2.
OLIF-SA, oblique lumbar interbody fusion stand alone; OLIF-PS, oblique lumbar interbody fusion and posterior pedicle screw fixation; TLIF, transforaminal lumbar interbody fusion.
Cage Subsidence and Settling Among Groups.
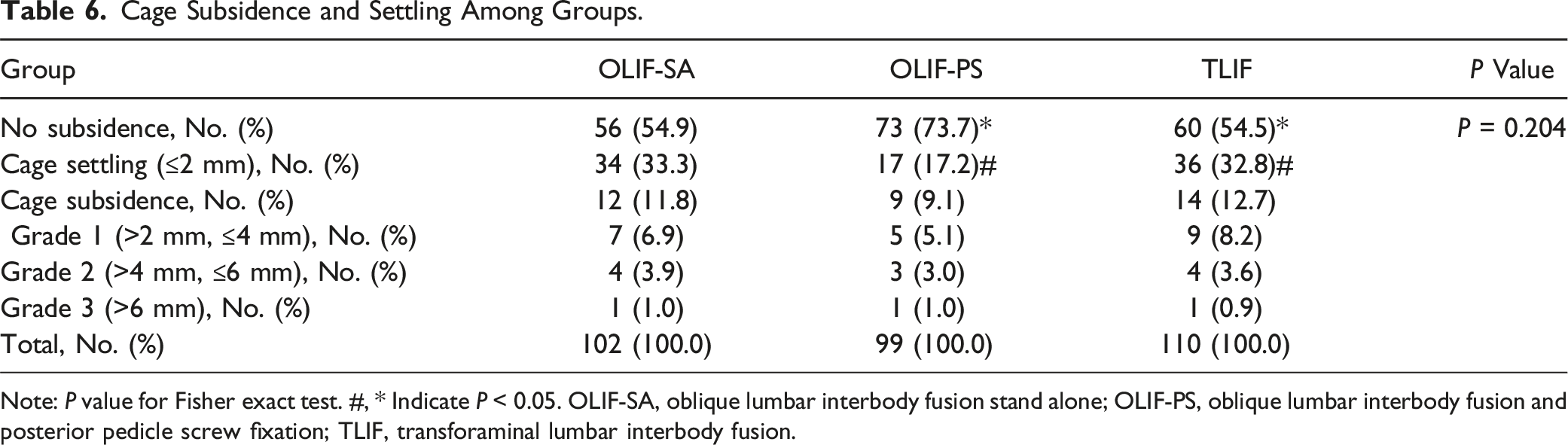
Note: P value for Fisher exact test. #, * Indicate P < 0.05. OLIF-SA, oblique lumbar interbody fusion stand alone; OLIF-PS, oblique lumbar interbody fusion and posterior pedicle screw fixation; TLIF, transforaminal lumbar interbody fusion.
Patient-Reported Outcomes Within Groups.

Note: Data are mean ± SD. t test for VAS and ODI. OLIF-SA, oblique lumbar interbody fusion stand alone; OLIF-PS, oblique lumbar interbody fusion and posterior pedicle screw fixation; TLIF, transforaminal lumbar interbody fusion.
Patient-Reported Outcome Comparison Among Groups.
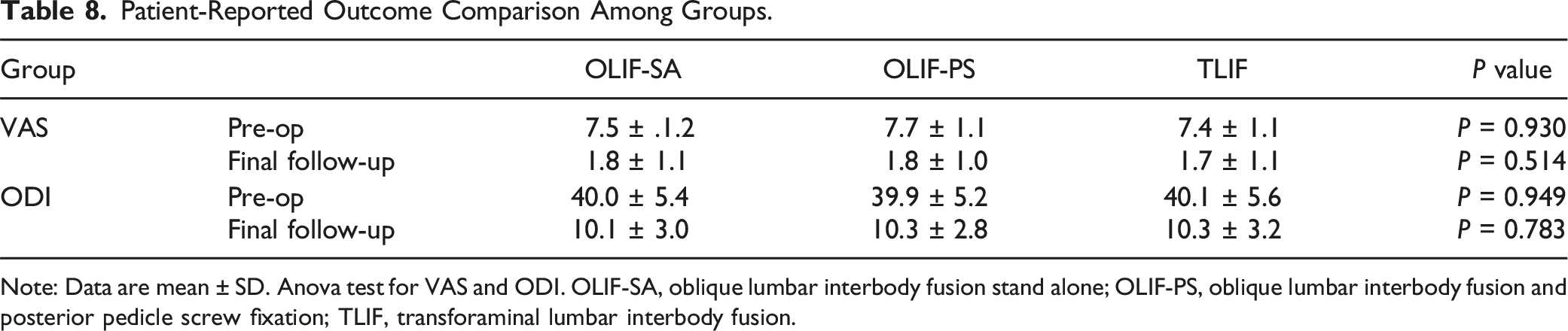
Note: Data are mean ± SD. Anova test for VAS and ODI. OLIF-SA, oblique lumbar interbody fusion stand alone; OLIF-PS, oblique lumbar interbody fusion and posterior pedicle screw fixation; TLIF, transforaminal lumbar interbody fusion.
Discussion
Interbody fusion, exemplified by TLIF 16 and OLIF, 17 represents a milestone in the treatment of lumbar spine disease. The primary feature of spinal fusion is to achieve interbody fusion by removing the intervertebral disc and implanting a cage filled with autograft or allograft into the intervertebral disc space through either the anterior, lateral or posterior approach. 18
TLIF achieves effective interbody fusion by inserting a cage filled with autologous bone or other bone substitutes into the disc space. 19 During TLIF surgery, the cage is typically deployed in the central portion of the intervertebral space. The peripheral AF on both sides and the anterior aspect of the intervertebral space are usually spared and intact. The effective fusion area within the intervertebral space is typically limited to the central region. Therefore, the fused bone bridge typically does not extend beyond the epiphyseal ring. 20 Therefore, the fusion type could be defined as centralized fusion.
However, in our study, we observed an interesting phenomenon. Unilateral or bilateral EVB of the vertebral body was common in OLIF-SA or OLIF-PS. Takami also reported a high rate of EVB following lateral lumbar interbody fusion surgery.
21
On the contrary, the TLIF group had only a few cases with lateral bone bridge formation. What’s more, compared to conventional TLIF, a substantial number of patients showed unilateral or bilateral EVB on X-ray during early follow-up (3-6 months) in OLIF surgeries (Figure 4). The fusion time for the intervertebral space varies, typically ranging from 6 to 12 months in TLIF surgeries.
22
The formation of EVB is earlier than that of intervertebral space fusion in OLIF surgeries. Zhao found that the OLIF-SA group tended to undergo fusion starting from the edge of the vertebral body.
23
The fusion mechanism of OLIF is probably that the formation of EVB, serving as an initial fusion factor, provide the early stability of the intervertebral space and cage.
21
Subsequently, the central endplate is connected by the central bony bridge. Ultimately, both lateral and central fusion are achieved. The patient, a 61-year-old female, was admitted due to recurrent back pain persisting for 8 years, she underwent L3/4 OLIF-SA. Preoperative imaging includes MRI (A1-2), CT (A3-4), lumbar spine AP view (A5), and flexion-extension films (A6-7), indicating grade I degenerative spondylolisthesis at the L3/4 segment. Immediate postoperative AP view (B1) and lateral (B2) X-rays show reduction of the spondylolisthesis and restoration of vertebral height. AP (B3) and lateral (B4) X-rays at 3 months postoperative reveals a tendency for EVB on left side of L3/4 (indicated by white rectangle). AP (B5) and lateral (B6) X-rays at 6 months show EVB on the left side of the L3/4 interspace (indicated by white circle) and a tendency for bridging on the right side (indicated by white rectangle), with cage settling. At 12 months postoperative (C1-2), left-sided EVB further strengthens (indicated by white circle), and there is increased bone spur formation on the right side (indicated by white rectangle). Postoperative CT at 1 year (C3) shows formation of EVB on the left side, achieving osseous fusion within the intervertebral space. OLIF-SA, oblique lumbar interbody fusion stand-alone; EVB, extra-vertebral body bone bridge; AP, anteroposterior. Post 3M, postoperative 3 months; Post 6M, postoperative 6 months; Post 1Y, postoperative 1 year.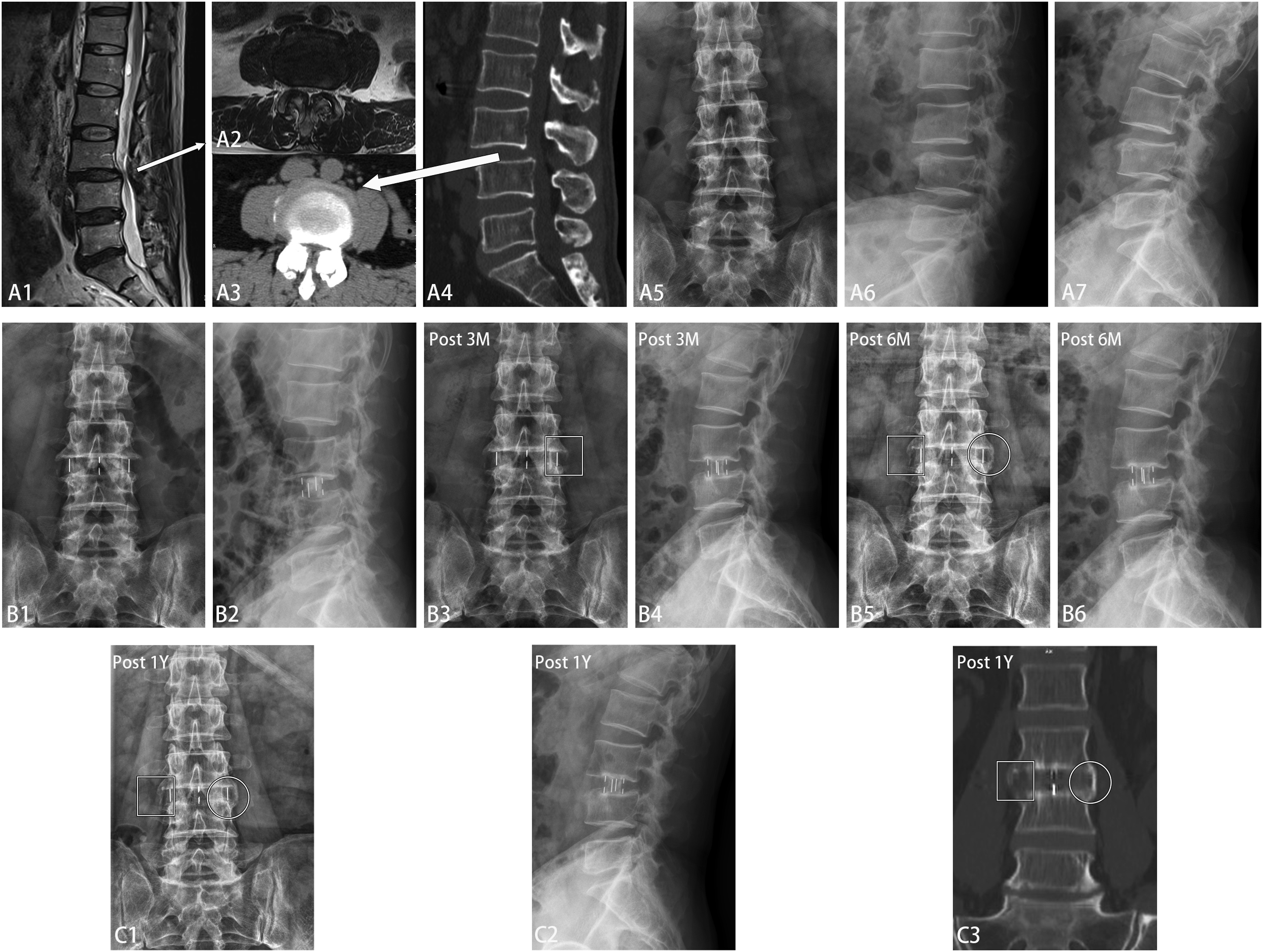
In OLIF surgeries, the fusion bony bridge initially appears outside the epiphyseal rings, marking a characteristic completely different from traditional TLIF. No one has previously defined this unique characteristic. Previous authors had reported the formation of lateral bone bridges, referring to it as the ‘sentinel sign’ in lateral interbody fusion.4-6 However, none of them clearly defined the concept of lateral fusion or reported the incidence of lateral fusion. We are the first to describe the distinctive lateral bone bridge formation as lateral fusion after OLIF and to report the precise incidence of lateral fusion in both OLIF and TLIF.
The potential mechanism for lateral fusion in OLIF may be:
Micro-Motion Within the Intervertebral Space Promotes Lateral Fusion
The vertebral body endplates are concave, resulting in an oval intervertebral space that is wider in the middle and narrower at the vertebral body edge. 24 In TLIF surgery, the cage size is restricted by the limited space between Kambin’s triangle. Due to insufficient space for implanting large cages, surgeons opt for smaller ones. 25
To achieve robust stability 26 and prevent posterior cage migration in TLIF, 27 an additional posterior pedicle screw with posterior compression is necessary. 28 However, the situation is quite different for OLIF surgery. In OLIF surgery, the disc space is accessed through the oblique lateral side of the vertebral body, allowing for ample space.
Mok 29 reported that posterior pedicle screw fixation, when compared to stand-alone in lateral lumbar interbody fusion, significantly reduces the mobility of the vertebral body in all directions. The stand-alone segment shows a significant trend of increased mobility in all directions (including flexion-extension, lateral bending, and axial rotation). This suggests that OLIF stand-alone may preserve micro-motion in the surgical segment. Fan 30 reported similar results when comparing double-level OLIF with different types of fixations. A sizable cage with appropriate dimensions can be implanted into the central part of the disc space in a stand-alone manner, offering robust initial mechanical stability 17 while preserving the micro-mobility of the surgical segment.
The repeated micro-motion of the OLIF-SA segment during daily activities can stimulate the formation of EVB around the intervertebral disc. This phenomenon may resemble the healing process of bone fractures. Two methods of bone fixation exist: absolute stable fixation and relative stable fixation. 31 With absolute methods of fixation (such as compression plates, compression screws, etc.), there is no micro-motion between fracture fragments. The fracture heals directly without the formation of a bone callus. With relatively stable fixation methods (such as bridging plates, etc.), there is micromovement between fracture fragments, and the fracture heals indirectly by forming a bone callus around the fracture site. 32
Similarly, micro-motion occurs in the surgical segment in OLIF-SA, and the periosteal-sharpey fiber-endosteum unit functions as the periosteal membrane. 33 This mechanism results in EVB formation that resembles bone callus. Literature has reported lateral bone bridge formation in cervical disc replacement, further supporting the idea that micro-motion can promote the formation of lateral bone bridges. 34
The stability status of TLIF significantly differs from that of OLIF-SA. TLIF surgery necessitates additional pedicle screw fixation to maintain posterior integrity and spinal stability. Pedicle screw-rod compression is also applied in TLIF to prevent cage migration 35 and restore lumbar lordosis, 36 transforming the screw-rod system into a rigid, absolutely stable fixation. As a result, fusion in TLIF is mainly confined to the central intervertebral space (central fusion) without the formation of EVB.
We observed a higher proportion of lateral fusion in OLIF-PS compared to TLIF, which might attribute to the surgical fixation method. In OLIF-PS, With the intact posterior longitudinal ligament, the anterior centrally positioned cage rarely shifts posteriorly, eliminating the need for compressing the screw-rod system. The screw-rod system functions more like a bridging plate, allowing for micro-movements between fusion segments. This dynamic results in a higher proportion of bone callus-like EVB formation compared to TLIF. Conversely, OLIF-PS exhibited a lower proportion of lateral fusion compared to OLIF-SA, primarily due to diminished micro-motion after pedicle screw fixation.
Bone Debris and Hematoma Contribute to Lateral Fusion
In OLIF surgery, trails penetrate both the ipsilateral and contralateral annulus fibrosus 37 to achieve epiphyseal ring-to-ring support. 38 Bone debris generated during endplate preparation and hematoma from the endplate and the psoas major muscle 39 are compressed toward the lateral side of the annulus fibrosus. These materials, rich in bone growth substances, 40 promote the formation of EVB.
In TLIF surgery, the approach reaches the intervertebral space through the spinal canal. The hematoma and bone debris from the intervertebral space cannot leak into the lateral and anterior site of the vertebral body due to the remaining intact lateral and anterior annulus fibrosus. Therefore, the proportion of lateral fusions in both OLIF-SA and OLIF-PS cases is significantly higher than in TLIF.
Preoperative Osteophytes Promote the Formation of Lateral Fusion
Our study reveals that preoperative osteophytes significantly enhance the likelihood of lateral fusion. Existing literature corroborates this finding, indicating that preoperative osteophytes can contribute to the formation of EVB. 21 This phenomenon may be attributed to two key factors: 1. Shorter Fusion Distances: Lateral osteophytes tend to extend outward from the edges of the vertebral bodies, leading to a more favorable fusion environment. The concave shape of the disc space results in a longer distance at the central endplate, 24 making lateral fusion more efficient. A study by Sheng et al. demonstrated that fusion occurs more rapidly at the uncovertebral joints of the cervical spine compared to the endplates, primarily due to the shorter distance at the uncovertebral joints. 41 This principle is similarly applicable to the lumbar spine. 2. Bone Bed Exposure in OLIF Procedures: During OLIF surgeries, the removal of the annulus fibrosus and surrounding osteophytes exposes the epiphyseal ring, creating a theoretically enhanced fusion bed. This increased exposure of bone significantly boosts the chances of successful lateral fusion.
There were significant differences among the three groups in cage settling rate. The TLIF group exhibited the highest rate, followed by OLIF-SA, while the OLIF-PS group had the lowest rate, as anticipated. During TLIF surgery, the cage is prone to subside when implanted in the central portion of the endplate with a small size. 12 In the OLIF-SA group, cage settling is more likely to occur without rigid pedicle screw fixation, which is attributed to micro-motion. During OLIF-PS surgery, the larger cage is implanted across the epiphyseal ring, 38 providing better support with additional rigid pedicle screw fixation, resulting in a reduced settling rate. 42 Interestingly, there were no significant differences in the cage subsidence rate among the three groups. This may be attributed to: 1. the selected patients all had good bone density, offering robust endplate support, cages tend to be stable without subsidence after the initial early settling; 2. In OLIF-PS and TLIF surgeries, the compression force on the cage was borne by the pedicle screw, which showed the similar subsidence rate. However, in OLIF-SA, patients with severe cage subsidence or migration underwent posterior fixation, ultimately categorized into the OLIF-PS group, resulting in a similar rate of cage subsidence in the final analysis.
Limitations
The study has several limitations. Firstly, it was retrospective, and the sample size was relatively small, the study had a relatively short follow-up time. Conducting a multicenter study with a larger sample size and a longer follow-up period may be necessary. Secondly, the included patients had various diagnoses, and the varying number of lumbar disc herniation cases among the groups could potentially influence the results. Thirdly, due to the retrospective nature of this study, we lack postoperative CT scans at 3 or 6 months. Fourth, OLIF and TLIF utilized different bone graft with in cage, and the variation in fusion materials may impact postoperative fusion feature. Fifth, we did not compare the differences in fusion feature among ALIF, XLIF, and DLIF. Further research is warranted.
Conclusion
OLIF-SA, OLIF-PS, and TLIF all demonstrated satisfactory fusion rates. The TLIF group exhibited a higher cage settling rate, while the cage subsidence rate remained similar among the groups. The high proportion of lateral fusion rate in OLIF surgeries, which is characterized by the formation of a unilateral or bilateral EVB around the intervertebral space, is an innovative fusion feature distinguishes itself from the conventional central fusion observed in TLIF.
Supplemental Material
Supplemental Material - Lateral Fusion is a Unique Feature in Oblique Lumbar Interbody Fusion Surgery: A Retrospective Cohort Study
Supplemental Material for Lateral Fusion is a Unique Feature in Oblique Lumbar Interbody Fusion Surgery: A Retrospective Cohort Study by Tong Yongjun, Fu Chudi, Zhang Qibin, Huang Bao, Ou Changjiang, Zhang Xuyang, Liu Junhui, Fan Shunwu and Zhao Fengdong in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Zhejiang Provincial Natural Science Foundation of China (Grant No.LZ23H060002). This study was supported by the National Natural Science Foundation of China (Grant No.82272521). This study was supported by the Zhejiang Medical Science and Technology Project (Grant No.2023564481).
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.