
Abstract
Study Design
Retrospective cohort study.
Objectives
Using propensity match score to remove those confounding bias and focuses on age factor to compare clinical outcomes and perioperative complications following spinal surgery in cohort of Korean octogenarians treated at a single tertiary hospital.
Methods
We classified patients of 80s as the octogenarian group (group O), those 65 and older, and under 80 as the elderly group (group E). We strategically employed the Propensity Score Matching (PSM) analysis as a method to counteract potential confounding variables. 1: 1 nearest-neighbor PSM for fusion level, estimated blood loss (EBL), transfusion, body mass index (BMI), American society of anesthesiologists (ASA) score, Charlson Comorbidity Index (CCI) surgical method and operation time was performed. After PSM, 98 patients are categorized each group evenly (group O, n = 49 vs group E, n = 49). Demographics, clinical, radiologic and postoperative complications were analyzed.
Results
The clinical outcomes showed no significant differences in the VAS and ODI preoperatively or postoperatively. And most of hospitalization related factors shows no differences between 2 groups. However, follow-up period was longer in group E (1053.37 ± 684.14 days) than group O (640.29 ± 496.68, P = 0.001) and group O has higher incidences of medical complication (38.77% vs 16.32%, P = 0.013), especially in delirium (34.69% vs 6.12%, P = 0.001) than group E.
Conclusions
With the preparation for the prevention and treatment of postoperative delirium, age itself should not be a reason to hesitate in performing the spinal surgery.
Keywords
Introduction
According to data of KOrean Statistical Information Service (KOSIS), the percentage of people in Korea aged 65 years or more is expected to double from 19.2% in 2024 to 40.1% in 2050. Additionally, those aged 80 years or more are anticipated to increase from 2.3 million in 2024 to 7.6 million in 2050. In the United States, those aged 85 years or more are anticipated to increase to 20 million by 2060, three times the current population. 3 In this super-aged society with modern advances in medical management, larger numbers of octogenarians will require surgical intervention for degenerative spinal diseases.4,5
Spine surgery in the elderly has historically been thought to be associated with an increased incidence of postoperative complications.6,7 Hence, spinal surgery in the elderly was considered taboo. Recently, studies have shown that elderly patients have favorable complication rates and clinical outcomes after spine surgery compared with younger patients.4,8-10 However, because of the complicacy of age factor itself, spine surgeons still regard old age as a burden for surgery. Elderly patients also hesitate to undergo spine surgery.
It is generally accepted that longer operation time, more estimated blood loss, comorbidity, and extent of surgery are negative risk factors for safety of spine surgery.11-13 Herein, the authors of this study used propensity match score to remove those confounding bias with focuses on age factor to compare clinical outcomes and perioperative complications following spinal surgery in a cohort of Korean octogenarians treated at a single tertiary hospital.
Methods
Population
A retrospective review of electronic medical records was conducted to identify patients aged between 65 and 89 years who underwent primary spinal fusion surgery with instrumentation at our institution for the diagnosis of degenerative lumbosacral spinal disease from January 2016 to December 2021. The reason for targeting only surgeries that performed fusion and instrumentation was to ensure uniformity in the extent of surgery between the 2 groups. We classified patients aged 80 to 89 years as the octogenarian group (group O). Those aged 65 years to 79 years were assigned into the elderly group (group E). Institutional Review Board approval was obtained prior to initiation of this study (No. 2024-1671-0001).
Surgical indications were severe neurologic symptoms and/or low back pain despite conservative treatment more than 3 months. Those who underwent surgeries related to trauma, malignancy, infection, and revision lumbosacral spine surgeries were excluded. A total of 400 cases were surgically treated at our institute based on those surgical indication during the aforementioned study period. Recognizing the need to enhance the robustness of our study, we strategically employed Propensity Score Matching (PSM) to counteract potential confounding variables.1,2
Information investigated in this study included demographics, length of stay in hospital (LoS), intensive care unit (ICU) stay, whether transfer after discharge or not, re-admission or mortality rate at 3 months postoperatively, treatment cost, postoperative complications, revision surgery, Charlson Comorbidity Index (CCI), fusion level, estimated blood loss (EBL), transfusion, BMI, American society of anesthesiologists (ASA) score, surgical method (1: post. approach fusion, 2: ant. approach fusion, 3: ant. & post. approach fusion in a single day, 4: ant. & post. approach fusion on separate days), and operation time. To assess frailty or comorbidities associated with age, we measured the CCI and ASA classification, both of which are well-known to be related to postoperative outcomes and complications.14,15 This approach was intended to further isolate the impact of age as an independent factor and refine the risk stratification.
Clinical and Radiological Assessments
Clinical assessments were evaluated using the Korean Oswestry disability (K-ODI), visual analog scale (VAS) of LBP (LBP-VAS), and VAS of buttock and lower limb pain (BLP-VAS). All tests were performed preoperatively and at 1 month and 1 year postoperatively. Radiological assessments were conducted using plain radiograph at 3, 6, and 12 months postoperatively and once every year thereafter. We counted metal failure or pseudoarthrosis as a nonunion and adjacent septal disease (ASD) which needed additional fusion surgery.
Postoperative Complications
For complications, we applied the complication classification system for orthopaedic surgery. 16 Postoperative complications were defined as those requiring changes of treatment compared with routine postoperative treatment during patient’s admission. Confirmed complications included delirium, urinary tract infection (UTI), pneumonia, surgical site infection (SSI), ileus, fever unknown origin (FUO), deep vein thrombosis (DVT) and atrial flutter.
Statistical Analysis
IBM SPSS Statistics version 24 (IBM Corp, Armonk, NY, USA) was used to perform all descriptive and comparative statistical analyses as well as propensity score matching. Significance was defined at P < 0.05. First, we compared unadjusted variables between Groups O and E. Categorical variables were analyzed using Pearson χ2 test or Fisher’s exact test when appropriate. Continuous variables were analyzed using Student'st test or Mann-Whitney U test for nonnormally distributed variables. Between-group balance after PSM was evaluated by calculating the standardized mean difference (SMD). SMD values <0.1 were considered to be indicative of a good balance.
Results
Over approximately 6 years, a total of 2056 patients underwent spinal surgery at this institution. Among them, 49 patients in Group O and 351 patients in Group E who aged between 65 years and 89 years underwent lumbosacral fusion surgery. They were followed up for 1 year after surgery. Using 1:1 nearest-neighbor propensity score matching (PSM) for fusion level, estimated blood loss (EBL), transfusion, BMI, ASA, CCI, surgical method and operation time, 49 patients from Group O and 49 patients from Group E were selected for analysis (Figure 1). Among the 98 patients assessed after PSM, the incidence of osteoporosis and mean BMD were 63% (29/45) and BMD -2.53 ± 1.08 in group E, and 72.3% (34/47) and BMD -2.76 ± 0.97 in group O, respectively, with no statistically significant differences (P = 0.295 and 0.338). Flow diagram for propensity score matching of studies.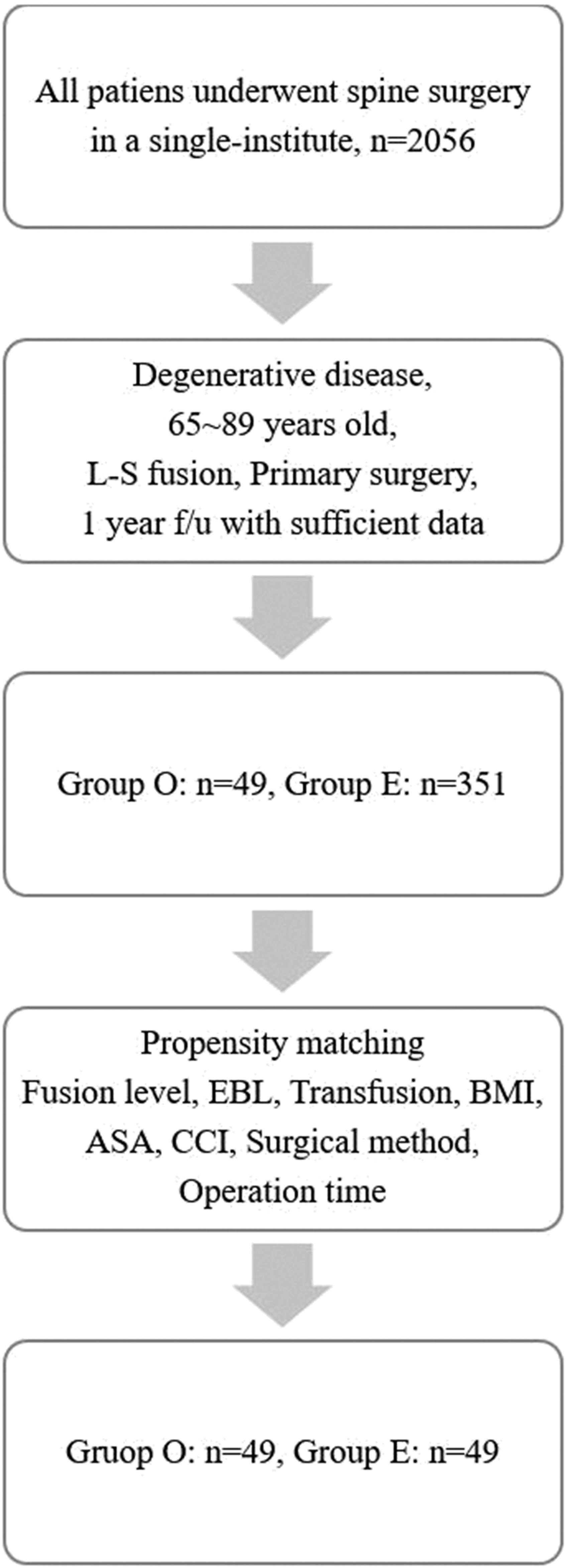
Patients Demographics and Surgical Factors Before and After Propensity Score Matching.
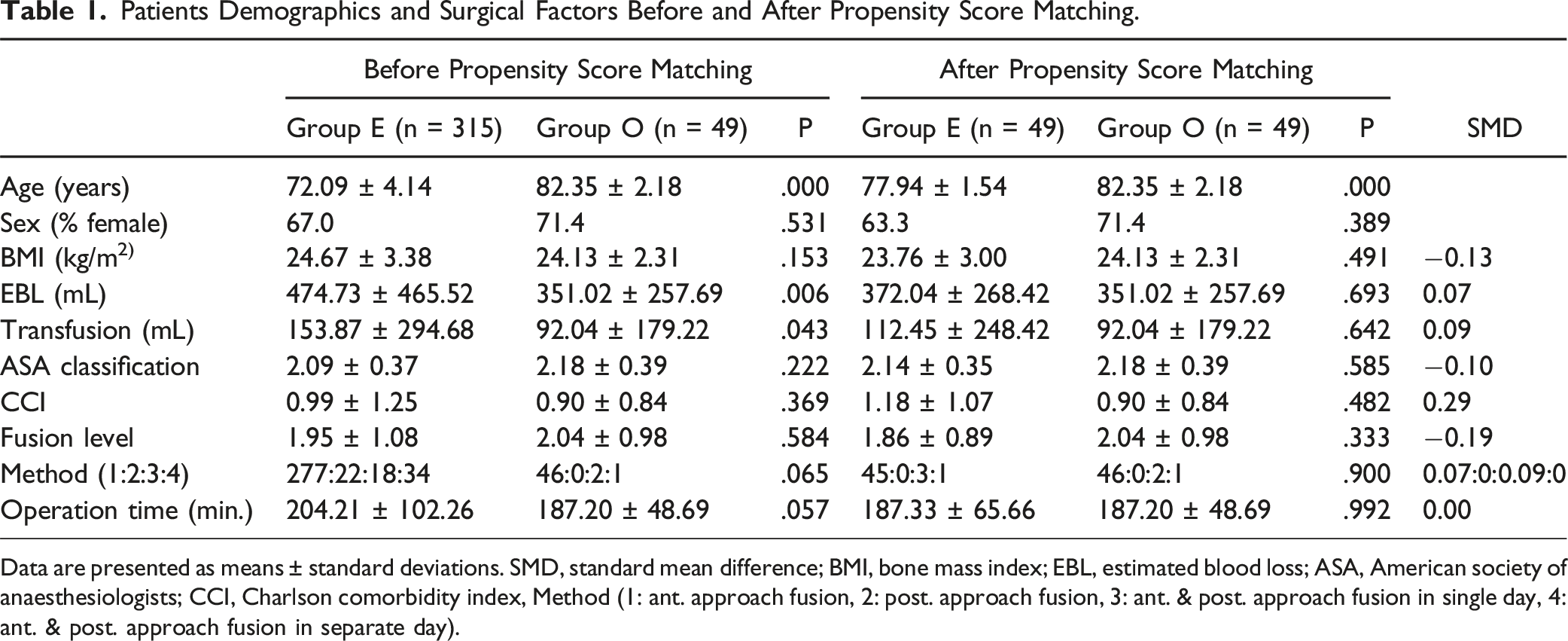
Data are presented as means ± standard deviations. SMD, standard mean difference; BMI, bone mass index; EBL, estimated blood loss; ASA, American society of anaesthesiologists; CCI, Charlson comorbidity index, Method (1: ant. approach fusion, 2: post. approach fusion, 3: ant. & post. approach fusion in single day, 4: ant. & post. approach fusion in separate day).
Clinical and Hospitalization Related Outcomes After PSM.
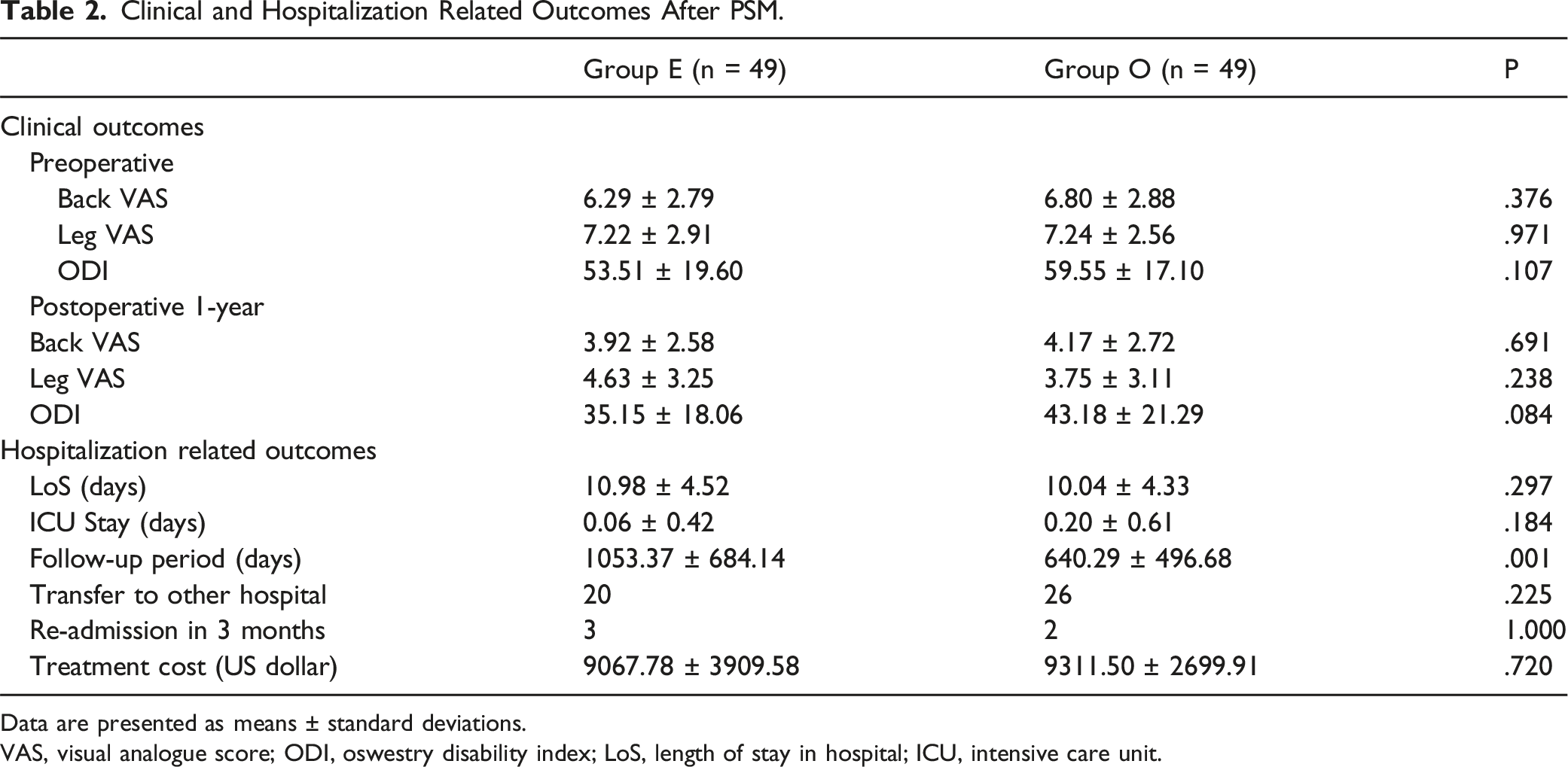
Data are presented as means ± standard deviations.
VAS, visual analogue score; ODI, oswestry disability index; LoS, length of stay in hospital; ICU, intensive care unit.
Postoperative Complications After PSM.
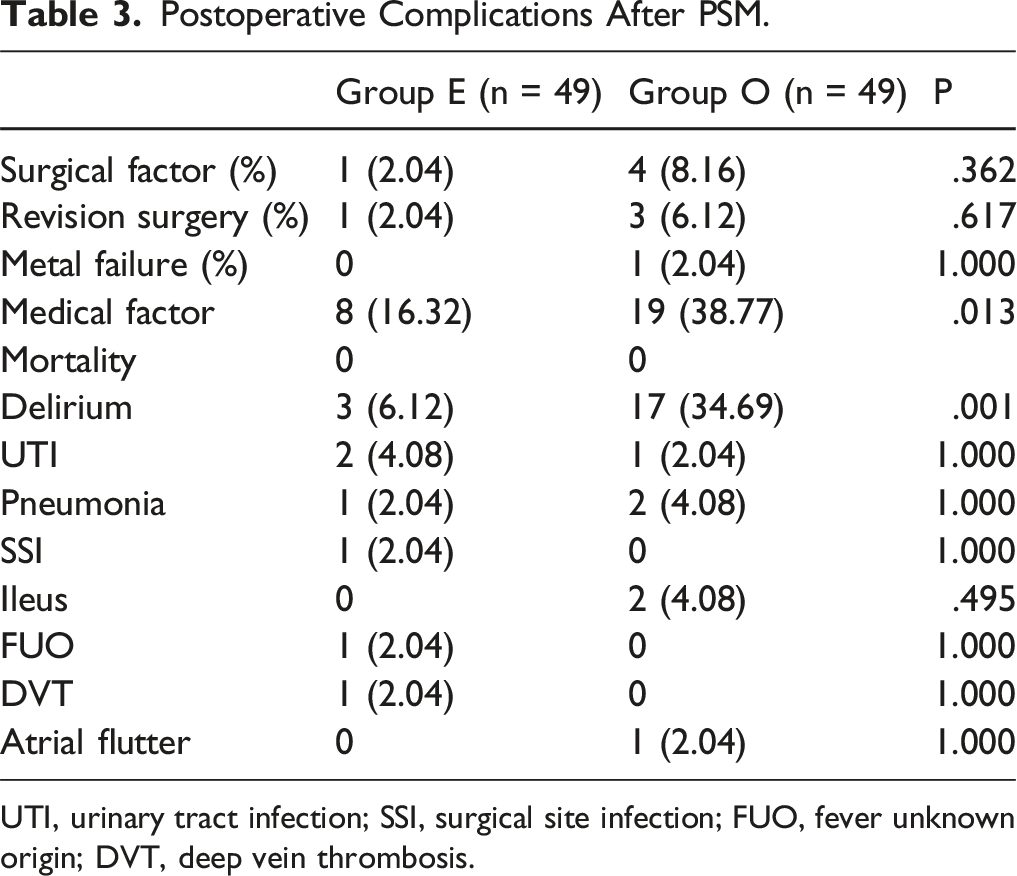
UTI, urinary tract infection; SSI, surgical site infection; FUO, fever unknown origin; DVT, deep vein thrombosis.
Discussion
Currently, the world is experiencing an aging society, 17 leading to an increase of spinal surgery patients. The age of these patients is also increasing.3,5,18 Additionally, elderly patients undergo significant degenerative changes, making the types and methods of spinal surgeries highly varied and often complex. Therefore, even with good management of underlying conditions through collaborative care, spinal surgery in elderly patients remains a constant concern for both patients and surgeons. However, with continuous advancement of medical care and improvement in living conditions, the diagnosis and treatment of comorbid conditions in elderly patients have significantly improved. Previously undiagnosed and untreated conditions are now being diagnosed and treated. Educational level of elderly patients has also improved, allowing them to undergo spinal surgery more safely.
Comparative Literatures of Spine Surgery in Super-elderly Patients.
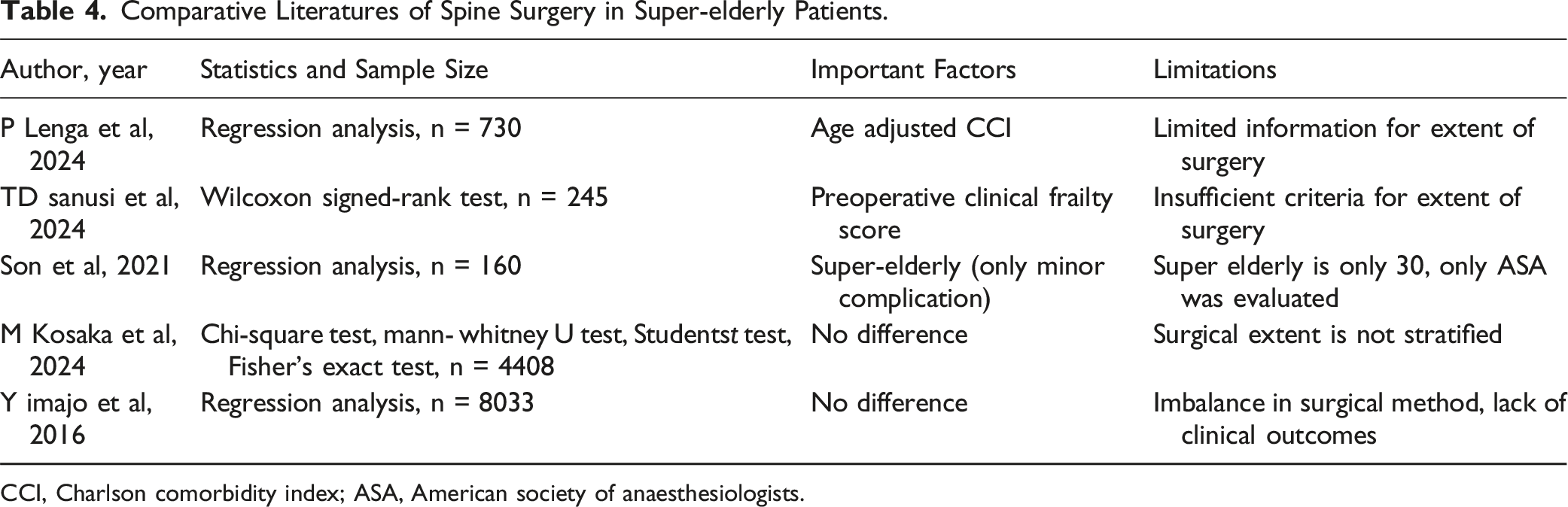
CCI, Charlson comorbidity index; ASA, American society of anaesthesiologists.
A review of existing research suggests that factors other than age can influence surgical outcomes, with most studies performing regression analyses.4,23,24 Considering the variety of surgeries performed on elderly patients and the age itself, concerns about age still persist. Therefore, this study was conducted to analyze the impact of age on spinal surgery using PSM with well-known surgery-related factors. PSM has several advantages compared with regression analysis. First, PSM tends to reduce selection bias. Unlike regression analysis, PSM can minimize bias by balancing covariates between groups.25,26 Second, while regression analysis heavily depends on the accuracy of model specifications, PSM is less sensitive to model fit. This implies that PSM can provide more consistent results across various models. 26 Third, PSM is better at capturing non-linear effects or interaction effects. This is especially important when linear relationships assumed by regression analysis do not adequately reflect reality. 27 Because of the small sample size, SMD was somewhat dissatisfied with some of the results. BMI (SMD = 0.1382) and ASA (SMD = 0.1079) are more than 0.1 but the SMD value is borderline and definite value is similar between group E and O. CCI (SMD = 0.2910) and fusion level (SMD = 0.1922) are slightly more than 0.1, but definite value shows group O rather has higher CCI and more fusion level, which means those variables in group O is not superior than group E.
Results of this study indicated that clinical symptoms before and after surgery were similar in both groups, consistent with previous research studies.8,20 Most hospitalization-related factors were also similar between the two groups except that patients under 80 years old had a longer average follow-up period. This was thought to be because younger patients tended to have a wider range of activities and a higher level of commitment to treatment. Hospitalization days and costs were also similar between the two groups. Thus, the authors could conclude that if the overall health condition and extent of surgery are similar, age itself does not cause a significant difference in the treatment process. The significantly higher incidence of postoperative delirium observed in group O was consistent with results of previous studies.8,28 Since postoperative delirium is still considered to be closely related to age, it is advisable for surgeons to remain vigilant and familiarize themselves with appropriate treatment methods. Furthermore, through detailed research on factors influencing postoperative delirium, it is believed that additional factors directly related to delirium can be identified.
This study has several limitations. First, it had a small sample size and a retrospective study design. However, since this was a single-institution study, it could be considered to have a relatively high-quality despite its small sample size, as it somewhat standardized spinal surgeries of a very diverse elderly patient population. Second, there might be a selection bias because this study only included patients who underwent spinal surgery. For safety, detailed reviews and collaborative care with other departments were conducted. Thus, not all patients over 80 years would be safe for the spinal surgery. Instead, this study indicates that if it is determined that surgery is feasible, then old age itself is not considered a significant problem. Third, we did not have a concept of frailty previously and did not measure frailty, so we were not able to fully incorporate this concept into this study. Frailty is a concept that has been used classically to distinguish between age and aging, 29 but it has been reported in many studies that age is just a number and that aging is a more sensitive indicator of stress on the body, such as spinal surgery. 30 However, in the case of modified frailty index (mFI), which is commonly used as an indicator to measure frailty, there is a lot of overlap with CCI, so I think that there is a certain amount of supplementation for frailty.
Conclusions
To achieve safe and satisfactory symptomatic improvement in spinal surgery for elderly patients, formulating an appropriate surgical treatment plan alongside meticulous medical diagnosis and treatment is crucial for surgeons. With these efforts, coupled with preparation for the prevention and treatment of postoperative delirium, age itself should not be a reason for hesitation when performing the spinal surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.