
Abstract
Study Design
Prospective multicenter study.
Objectives
Palliative surgery is crucial for maintaining the quality of life (QOL) in patients with spinal metastases. This study aimed to compare the short-term outcomes of QOL after palliative surgery between patients with metastatic spinal tumors at different segments.
Methods
We prospectively compared the data of 203 patients with spinal metastases at 2-3 consecutive segments who were divided into the following three groups: cervical, patients with cervical spine lesions; thoracic, patients with upper–middle thoracic spine lesions; and TL/L/S, patients with lesions at the thoracolumbar junction and lumbar and sacral regions. Preoperative and postoperative EuroQol 5-dimension (EQ5D) 5-level were compared.
Results
All groups exhibited improvement in the Frankel grade, performance status, pain, Barthel index, EQ5D health state utility value (HSUV), and EQ5D visual analog scale (VAS) postoperatively. Although preoperative EQ5D HSUVs did not significantly differ between the groups (cervical, 0.461 ± 0.291; thoracic, 0.321 ± 0.292; and TL/L/S, 0.376 ± 0.272), the thoracic group exhibited significantly lower postoperative EQ5D HSUVs than the other two groups (cervical, 0.653 ± 0.233; thoracic, 0.513 ± 0.252; and TL/L/S, 0.624 ± 0.232). However, postoperative EQ5D VAS was not significantly different between the groups (cervical, 63.4 ± 25.8; thoracic, 54.7 ± 24.5; and TL/L/S, 61.7 ± 21.9).
Conclusions
Palliative surgery for metastatic spinal tumors provided comparable QOL improvement, irrespective of the spinal segment involved. Patients with upper and middle thoracic spinal metastases had poorer QOL outcomes than those with metastases in other segments; however, sufficient QOL improvement was achieved.
Keywords
Introduction
Managing quality of life (QOL) in patients with cancer is essential during the late stage of the disease. 1 The spine is a common site of metastasis, affecting approximately 20% of patients with cancer. 2 Spinal metastases commonly cause severe pain and neurological deficits, severely affecting patients’ activities of daily living (ADL) and QOL.1,3,4 Although recent advancements in oncologic therapies, such as chemotherapy, molecularly targeted biologics, and immunotherapy, have prolonged the survival of patients with spinal metastases, 1 these innovations have limited efficacy against bone metastases.3,5 Thus, managing spinal metastases in a way that maintains patients’ QOL remains an important challenge.6,7
No consensus has been reached on the most effective treatment for spinal metastases. 1 Except for a few cases of isolated vertebral metastases for which radical resection is indicated,8,9 palliative surgery is the mainstay treatment to maintain QOL of patients with spinal metastases.2,3 However, data on the effect of palliative surgery on QOL among patients with metastatic spinal lesions and malignant spinal cord compression are limited. 10 In a retrospective study by Yamashita et al 11 involving 86 patients with spinal metastatic tumors at various segments who underwent surgery, 51.1% experienced improvement in the Eastern Cooperative Oncology Group-performance status (ECOG-PS). Moreover, in a prospective study by Niu et al, 12 39 patients with thoracic or lumbar metastatic tumors demonstrated improved postoperative QOL as assessed by the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire for Patients with Bone Metastases (EORTC QLQ-BM22). These findings suggest that palliative surgery partially improves QOL in patients with spinal metastases. However, because evidence is limited to retrospective or prospective studies with relatively small sample sizes, the data do not reflect the diversity of the actual patient population. Furthermore, metastatic spinal tumors can involve any segment of the spine.
The most common spinal metastasis site is the thoracic spine (60%–80%), followed by the lumbar (15%–30%) and cervical (<10%) spine. 13 Symptom severity and effect on QOL may vary based on the site of the spinal lesion. In an analysis of patients referred to radiation therapy clinics for spinal metastases treatment, Hindle et al 14 found that patients with lesions in the mobile spinal segments (cervical and lumbar lesions) were more likely to experience severe pain than those with lesions in the non-mobile segments. However, previous studies identifying preoperative predictors of QOL outcomes have either not distinguished between lesion segments15-17 or have been limited to targeted analyses.18,19 Thus, QOL impairments experienced by patients with spinal metastases at different segments and the extent of recovery following surgical treatment remain unknown. To address these research gaps, we conducted a prospective multicenter study to evaluate differences in short-term QOL outcomes following palliative surgery in patients with metastatic spinal tumors at different segments.
Materials and methods
Patient Population
This prospective multicenter study was conducted by the Japan Association of Spine Surgeons with Ambition (JASA) group between October 2018 and March 2021. All study participants provided informed consent, and the study protocol was approved by the Institutional Review Board of the coordinating institute and each institute. Patients aged ≥20 years who were scheduled for surgical treatment of metastatic spinal tumors and had consented to participate in the study were included in the study. Patients with dementia or other conditions that made it difficult to complete the questionnaire were excluded from the study.
A total of 413 patients from 38 institutions were enrolled. Of the 413 patients, 257 in whom 1-3 consecutive vertebrae were affected were included, and those with multiple spinal metastases were excluded. Of the 257 patients, 27 who underwent total en bloc spondylectomy and 27 with a postoperative follow-up period <1 month were excluded. Finally, 203 patients were included in this analysis. The average postoperative follow-up period was 10 months (range: 1-31 months).
The surgical procedure was determined by the physician in charge at each institution based on the overall assessment of the patient’s condition and spinal instability neoplastic score (SINS). Generally, decompression was chosen for patients with stable lesions, whereas stabilization with or without decompression was chosen for patients with potentially unstable or unstable lesions. However, stabilization was added for stable lesions when there was concern about iatrogenic spinal instability due to the need to sacrifice facet joints or other components to achieve adequate decompression. If the surgeon deemed that the lesion warranted anterior decompression, anterior decompression and fusion were performed. Balloon kyphoplasty was also an option for potentially unstable lesions in the TL/L/S group.
Variables and Grouping
The following data were collected from all patients: age, sex, primary malignant lesion, Tokuhashi score, 20 surgical procedure, surgical duration, blood loss, and mortality. Furthermore, patients’ ADL and QOL were assessed by Frankel grade classification, ECOG-PS, visual analog scale (VAS) for pain, Barthel index, 21 EuroQol 5-dimension 5-level (EQ-5D-5L), and EQ5D VAS. The difference between postoperative and preoperative values for continuous variables was calculated as the 1-month postoperative value minus the preoperative value and denoted by the delta sign. Surgical site infection, wound problems, and neurological deterioration were investigated as perioperative adverse events.
Based on the segment of the lesion (Figure 1) and the differences in the expected neurological deficits, the patients were divided into the following three groups: cervical, which included cervical spine lesions; thoracic, which included lesions from the thoracic spine up to thoracolumbar junction (upper–middle thoracic); and TL/L/S, which included lesions at the thoracolumbar junction and lumbar and sacral regions. Distribution of the metastatic lesions based on segment (with overlap).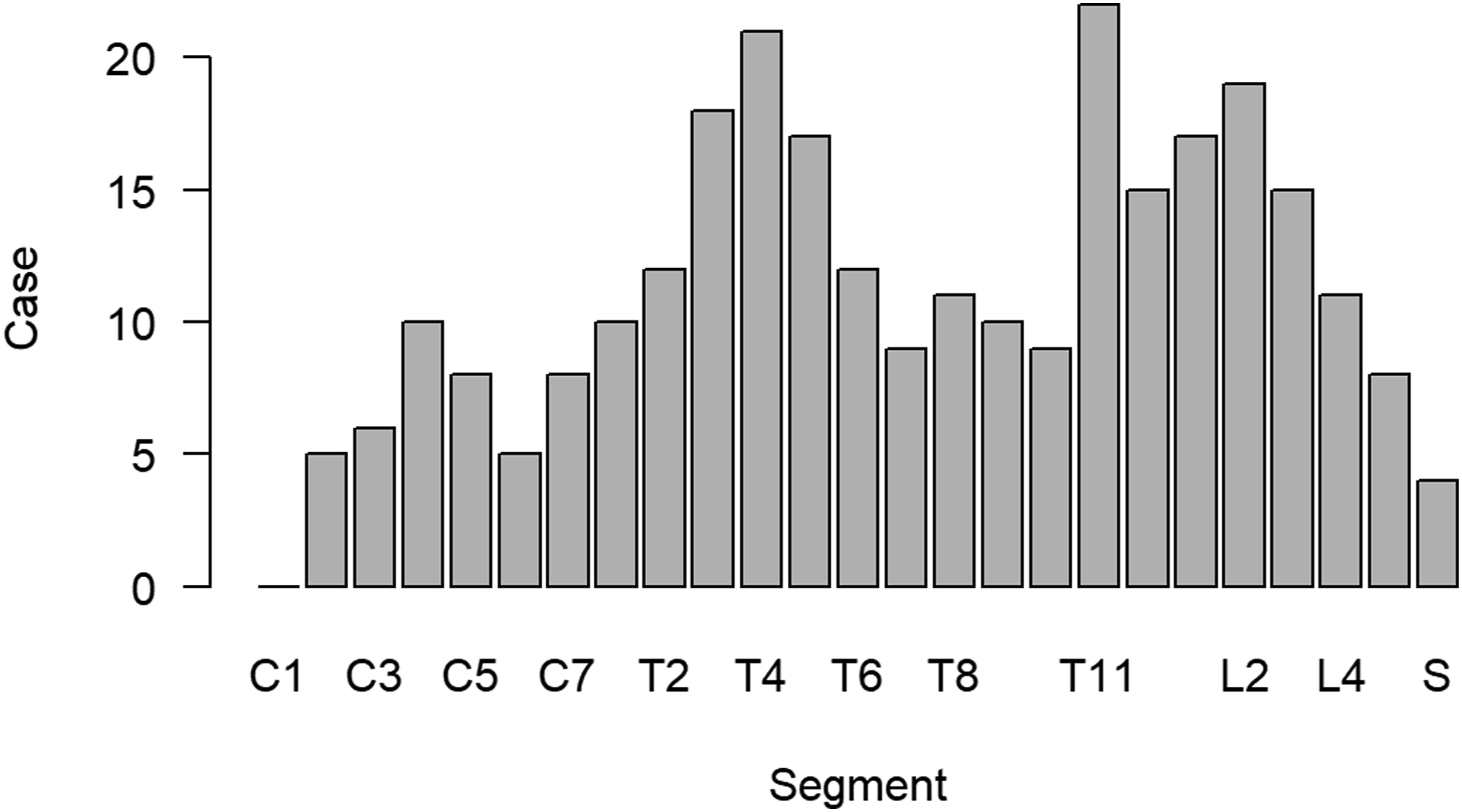
Statistical analysis
Data are presented as means ± standard deviations for continuous variables and as numbers and percentages for categorical data. Statistical analyses were performed using R (version 4.3.1; https://www.R-project.org). Analysis of variance, Tukey’s honestly significant difference test, Wilcoxon signed-rank test with continuity correction, Fisher’s exact test, and Benjamini–Hochberg multiple testing correction were performed. A P-value <0.05 was considered statistically significant.
Results
Metastatic Lesion Segments.
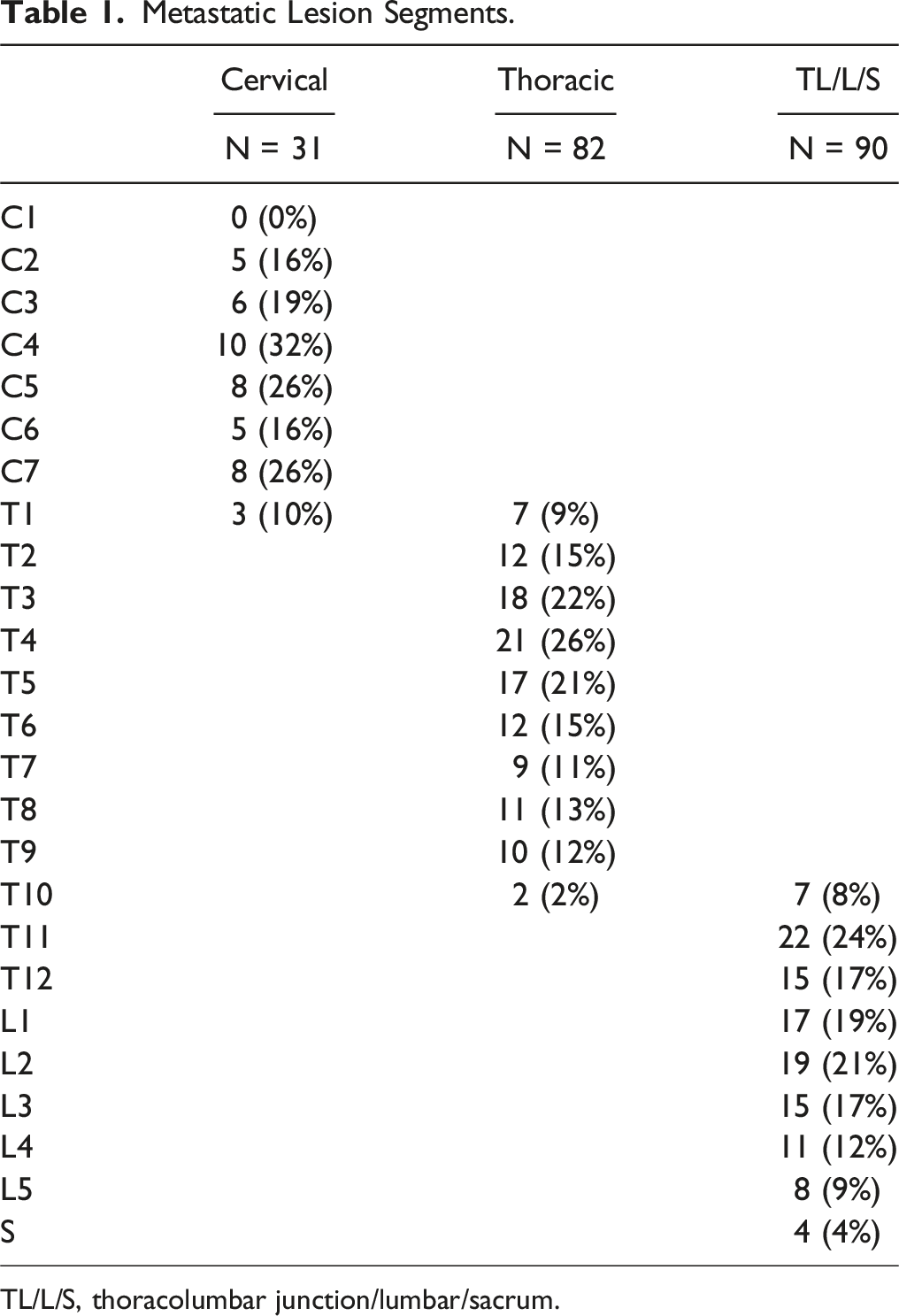
TL/L/S, thoracolumbar junction/lumbar/sacrum.
Patient Characteristics.
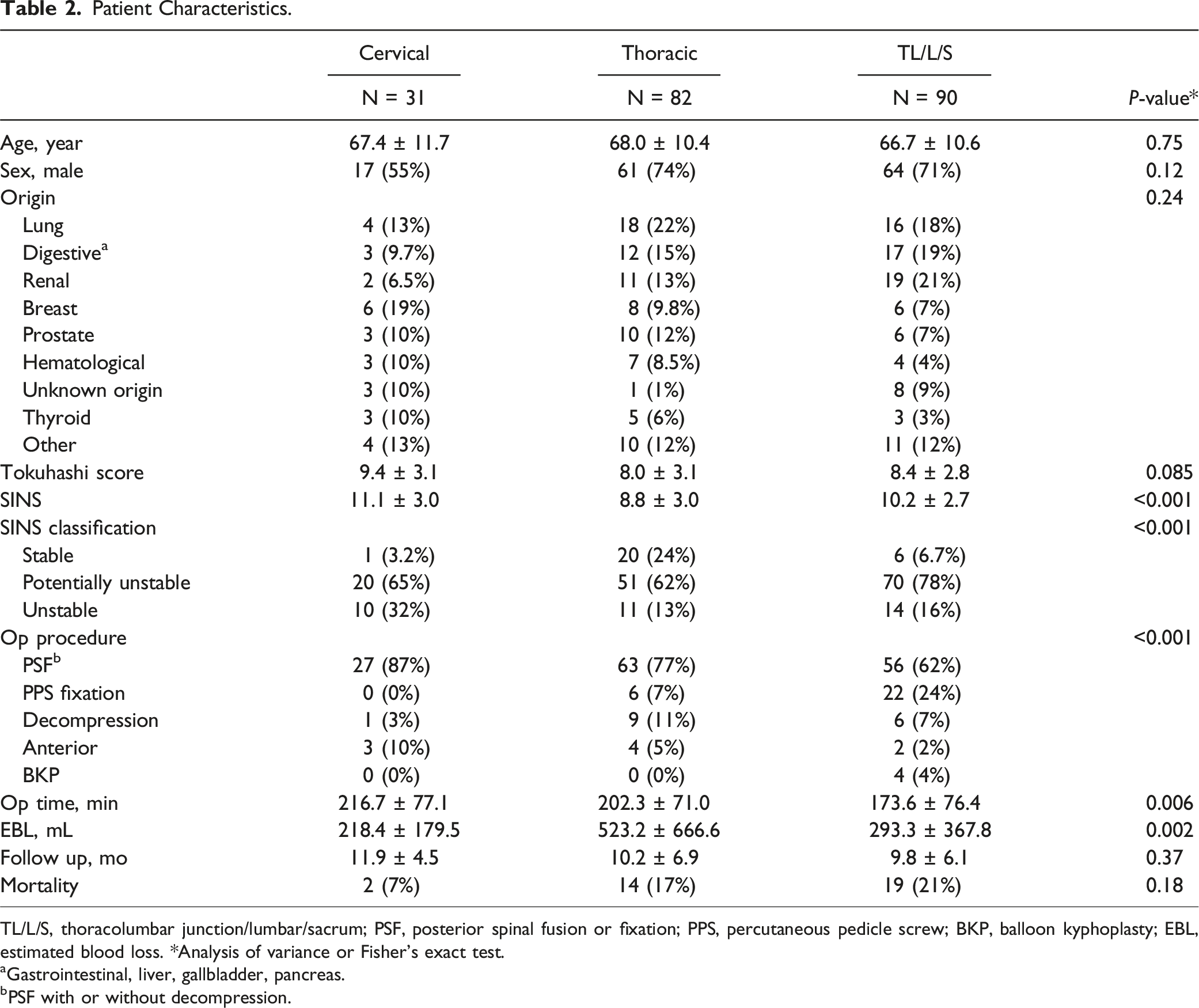
TL/L/S, thoracolumbar junction/lumbar/sacrum; PSF, posterior spinal fusion or fixation; PPS, percutaneous pedicle screw; BKP, balloon kyphoplasty; EBL, estimated blood loss. *Analysis of variance or Fisher’s exact test.
aGastrointestinal, liver, gallbladder, pancreas.
bPSF with or without decompression.
SINS and Surgical Procedures.
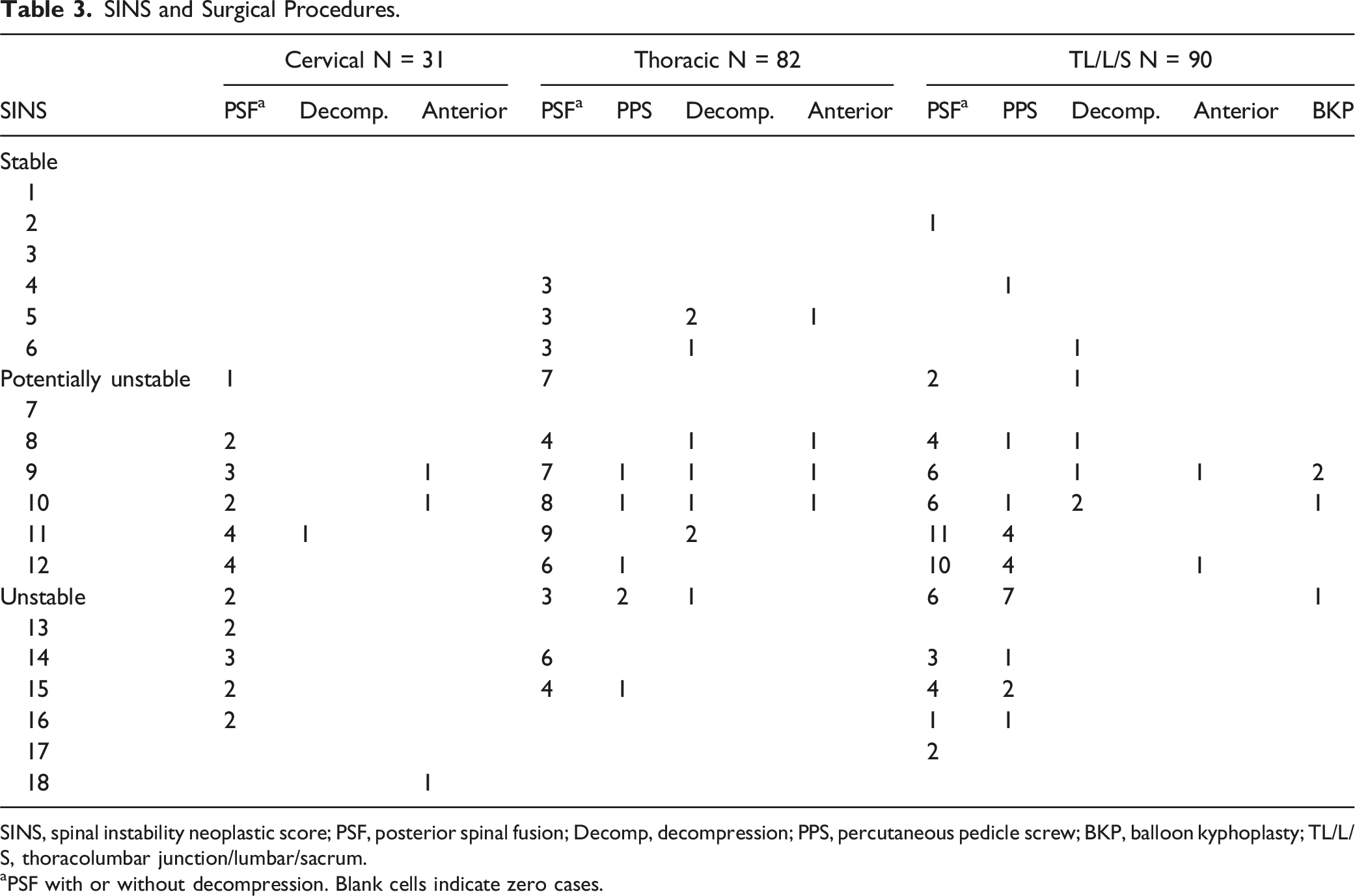
SINS, spinal instability neoplastic score; PSF, posterior spinal fusion; Decomp, decompression; PPS, percutaneous pedicle screw; BKP, balloon kyphoplasty; TL/L/S, thoracolumbar junction/lumbar/sacrum.
aPSF with or without decompression. Blank cells indicate zero cases.
ADL and QOL Recovery Following Surgical Treatment.
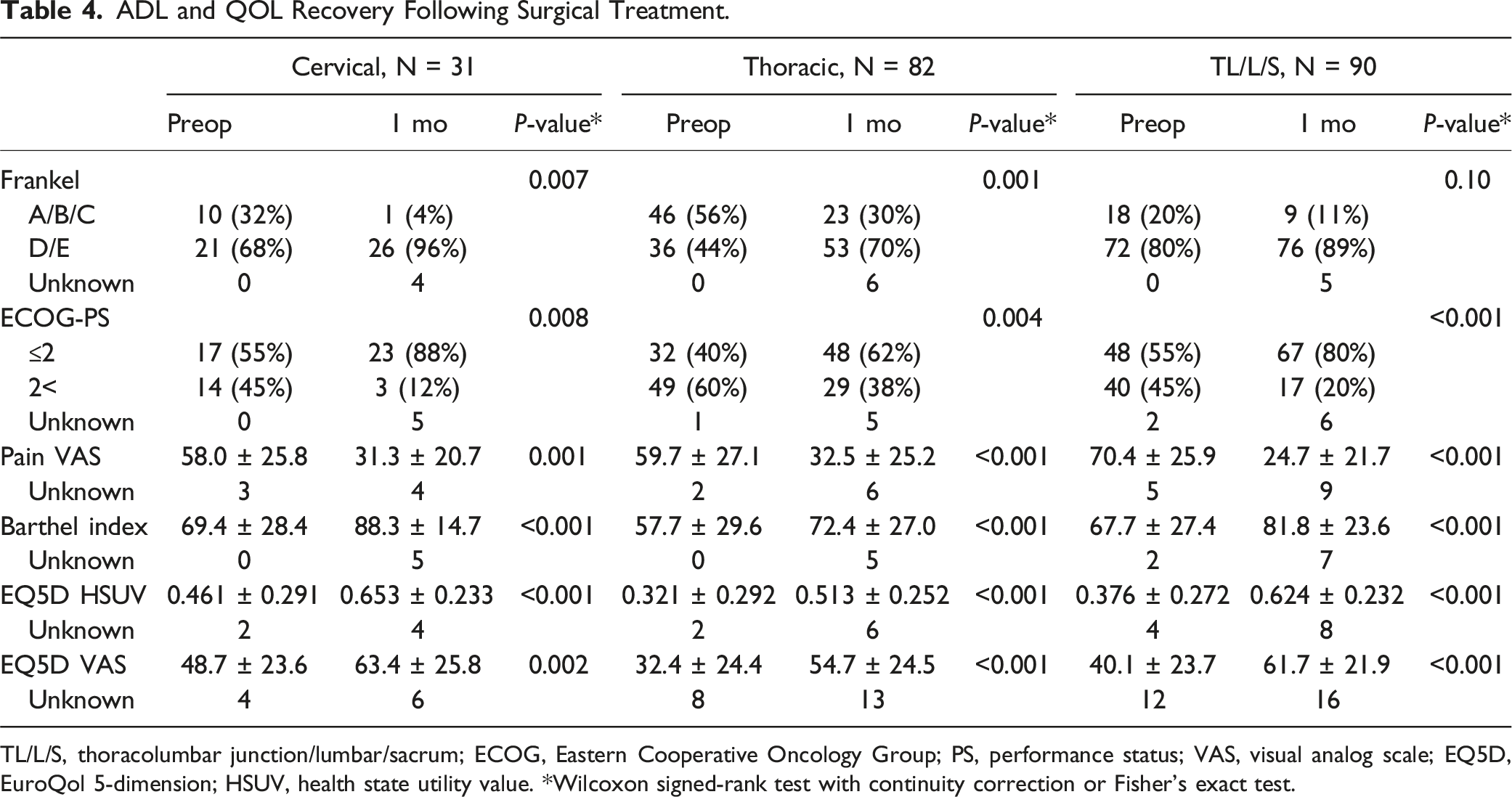
TL/L/S, thoracolumbar junction/lumbar/sacrum; ECOG, Eastern Cooperative Oncology Group; PS, performance status; VAS, visual analog scale; EQ5D, EuroQol 5-dimension; HSUV, health state utility value. *Wilcoxon signed-rank test with continuity correction or Fisher’s exact test.
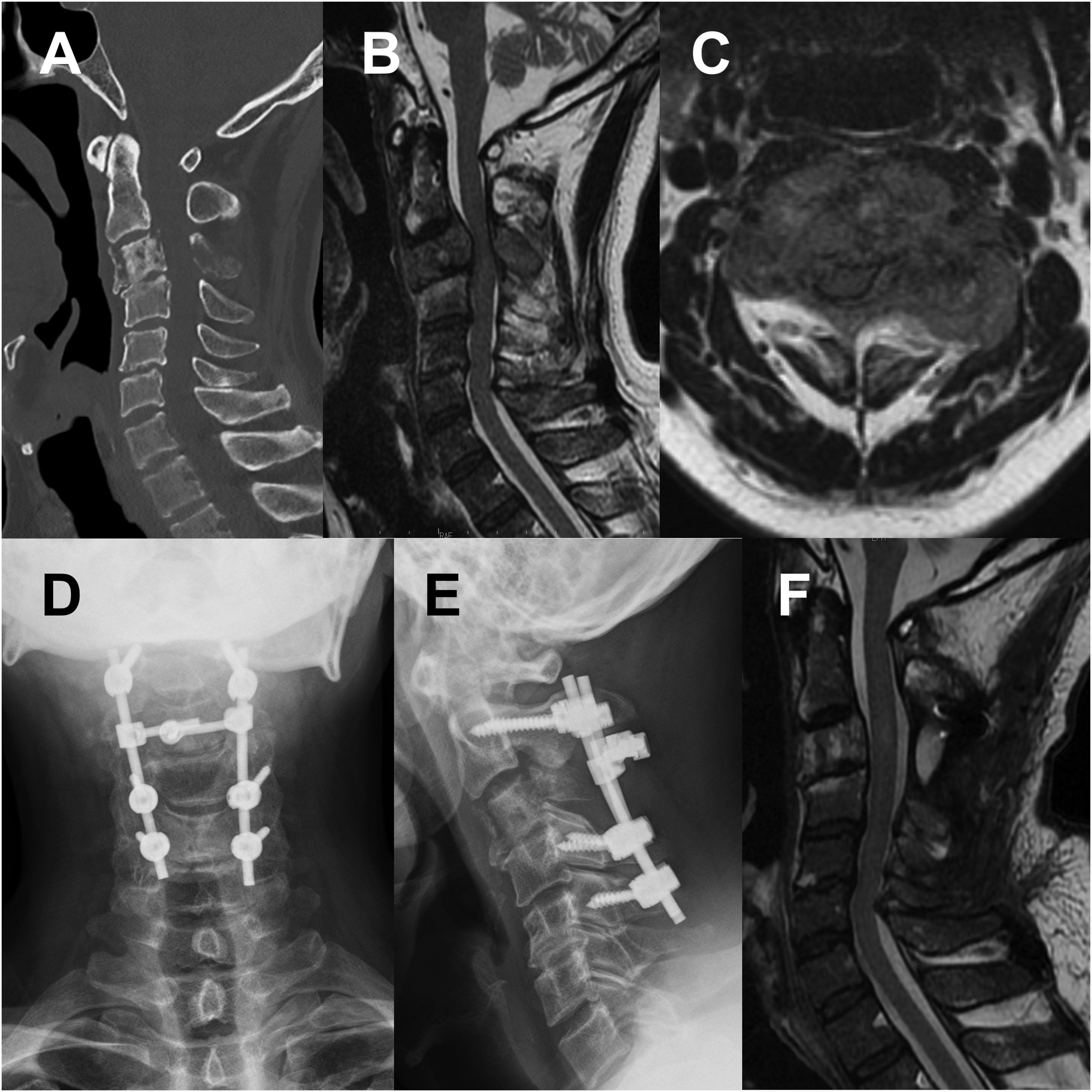
A case of a man in his 60s in the cervical group with a primary lung lesion. The patient had muscle weakness (Frankel grade C) due to C3 spinal metastasis, with preoperative PS of 2, Barthel index of 30, pain VAS of 40 mm, EQ5D HSUV of 0.210, and EQ5D VAS of 50 mm. One month after posterior decompression and fusion, muscle weakness partially improved (Frankel grade D), with a PS of 1, Barthel index of 90, pain VAS of 10 mm, EQ5D HSUV of 0.575, and EQ5D VAS of 80 mm. (A) Preoperative CT sagittal image showing a C3 pathological fracture. (B, C) Preoperative MR sagittal and transverse T2WIs showing compression of the spinal cord. (D, E) Postoperative X-ray images. (F) Postoperative MR sagittal T2WI. PS, performance status; VAS, visual analog scale; EQ5D, EuroQol 5-dimension; HUSV, health state utility value; CT, computed tomography; MR, magnetic resonance; T2WI, T2-weighted image.
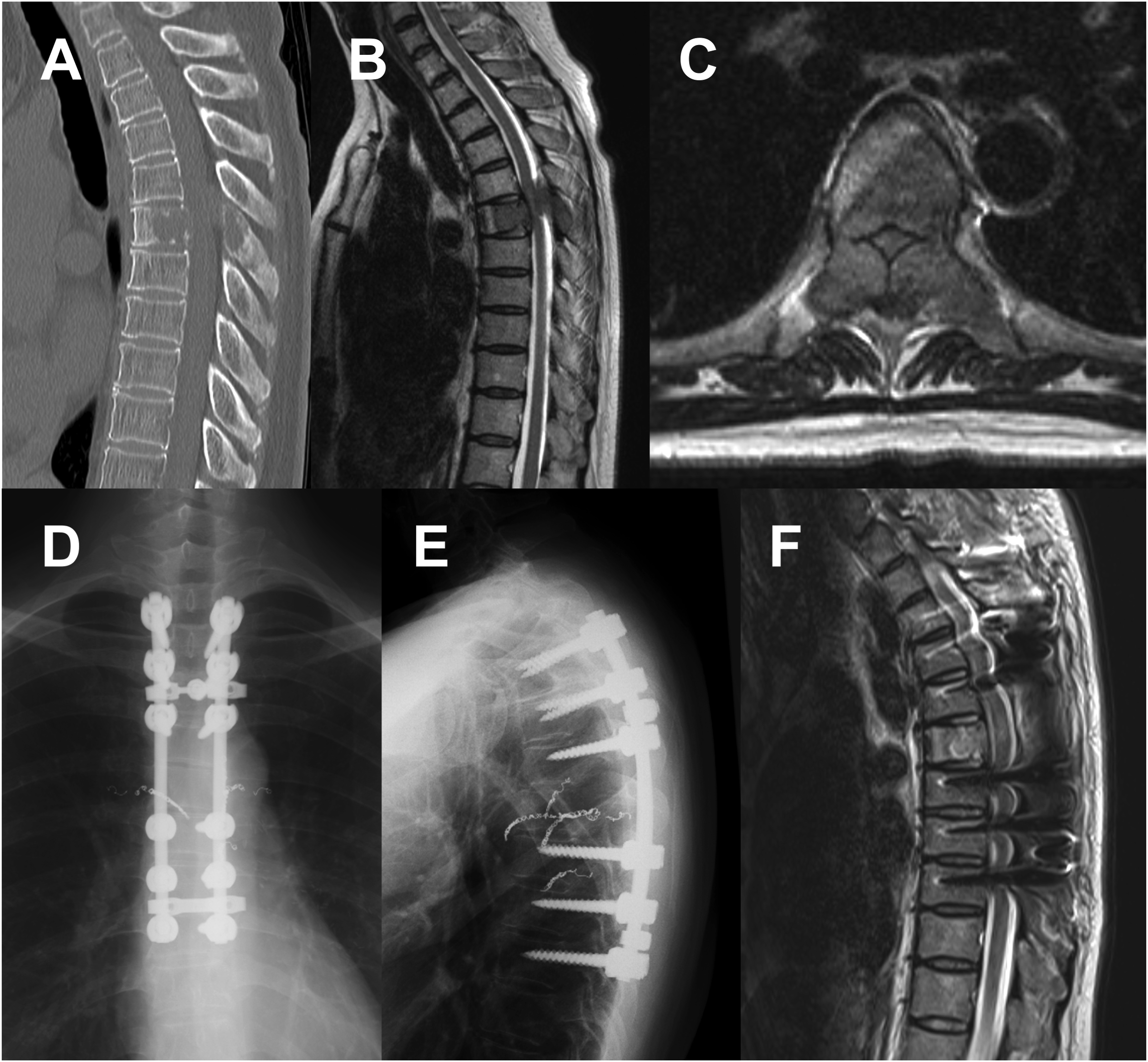
A case of a man in his 70s in the thoracic group with a primary lung lesion. The patient had muscle weakness (Frankel grade C) due to T6 spinal metastasis, with a preoperative PS of 4, Barthel index of 40, pain VAS of 81 mm, EQ5D HSUV of 0.188, and EQ5D VAS of 65 mm. One month after posterior decompression and fusion, muscle weakness remained at Frankel grade C. However, PS recovered to 3, Barthel index to 65, pain VAS to 54 mm, EQ5D HSUV to 0.480, and EQ5D VAS to 60 mm. (A) Preoperative CT sagittal image showing T6 vertebral osteolysis. (B, C) Preoperative MR sagittal and transverse T2WIs showing compression of the spinal cord. (D, E) Postoperative X-ray images. (F) Postoperative MR sagittal T2WI. PS, performance status; VAS, visual analog scale; EQ5D, EuroQol 5-dimension; HUSV, health state utility value; CT, computed tomography; MR, magnetic resonance; T2WI, T2-weighted image.
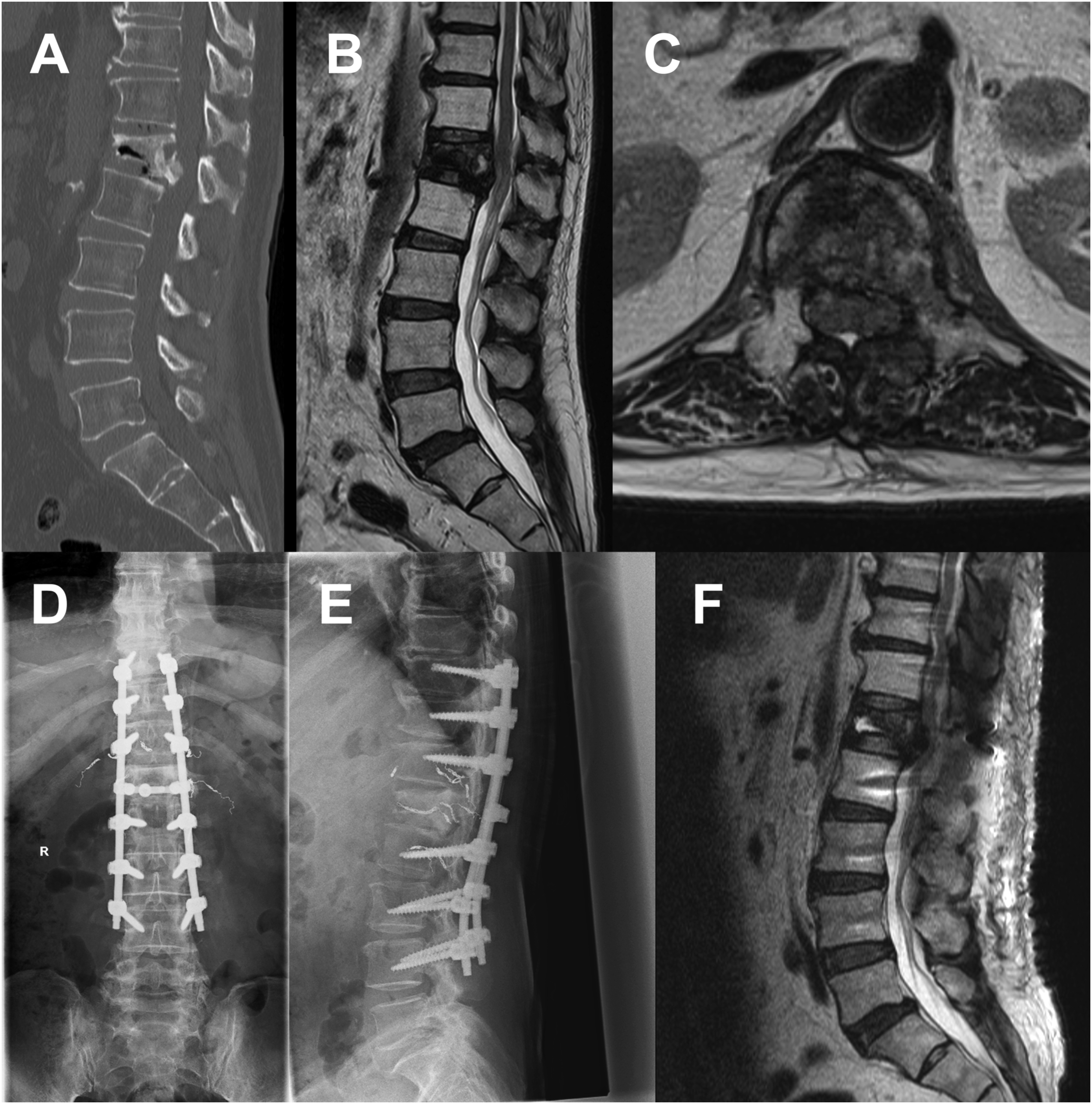
A case of a man in his 70s in the TL/L/S group with a primary lung lesion. The patient had muscle weakness (Frankel grade D) due to L1 spinal metastasis, with a preoperative PS of 3, Barthel index of 60, pain VAS of 50 mm, EQ5D HSUV of 0.414, and EQ5D VAS of 30 mm. One month after posterior decompression and fusion, muscle weakness remained at grade D. However, PS recovered to 2, Barthel index to 95, pain VAS to 14 mm, EQ5D HSUV to 0.665, and EQ5D VAS to 70 mm. (A) Preoperative CT sagittal image showing L1 pathological fracture. (B, C) Preoperative MR sagittal and transverse T2WIs showing compression of the spinal cord. (D, E) Postoperative X-ray images. (F) Postoperative MR sagittal T2WI. PS, performance status; VAS, visual analog scale; EQ5D, EuroQol 5-dimension; HUSV, health state utility value; CT, computed tomography; MR, magnetic resonance; T2WI, T2-weighted image.
Adverse Events.
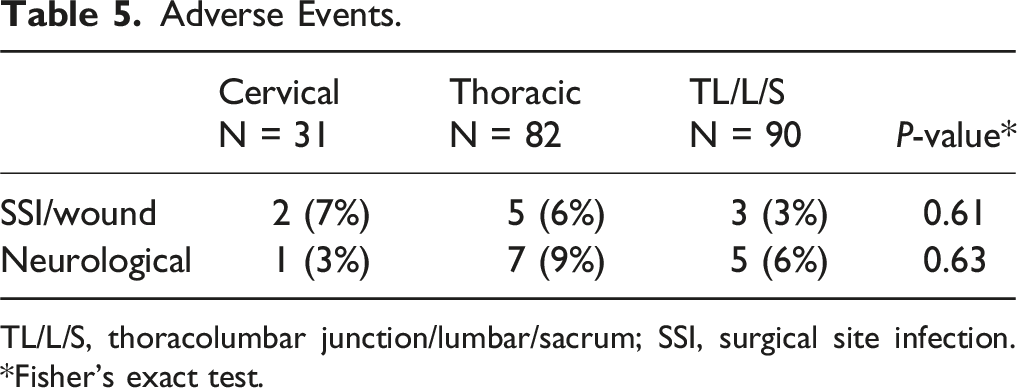
TL/L/S, thoracolumbar junction/lumbar/sacrum; SSI, surgical site infection. *Fisher’s exact test.
Comparison of Pre- and Postoperative ADL and QOL Between Groups Classified Based on Spinal Metastasis Segment.
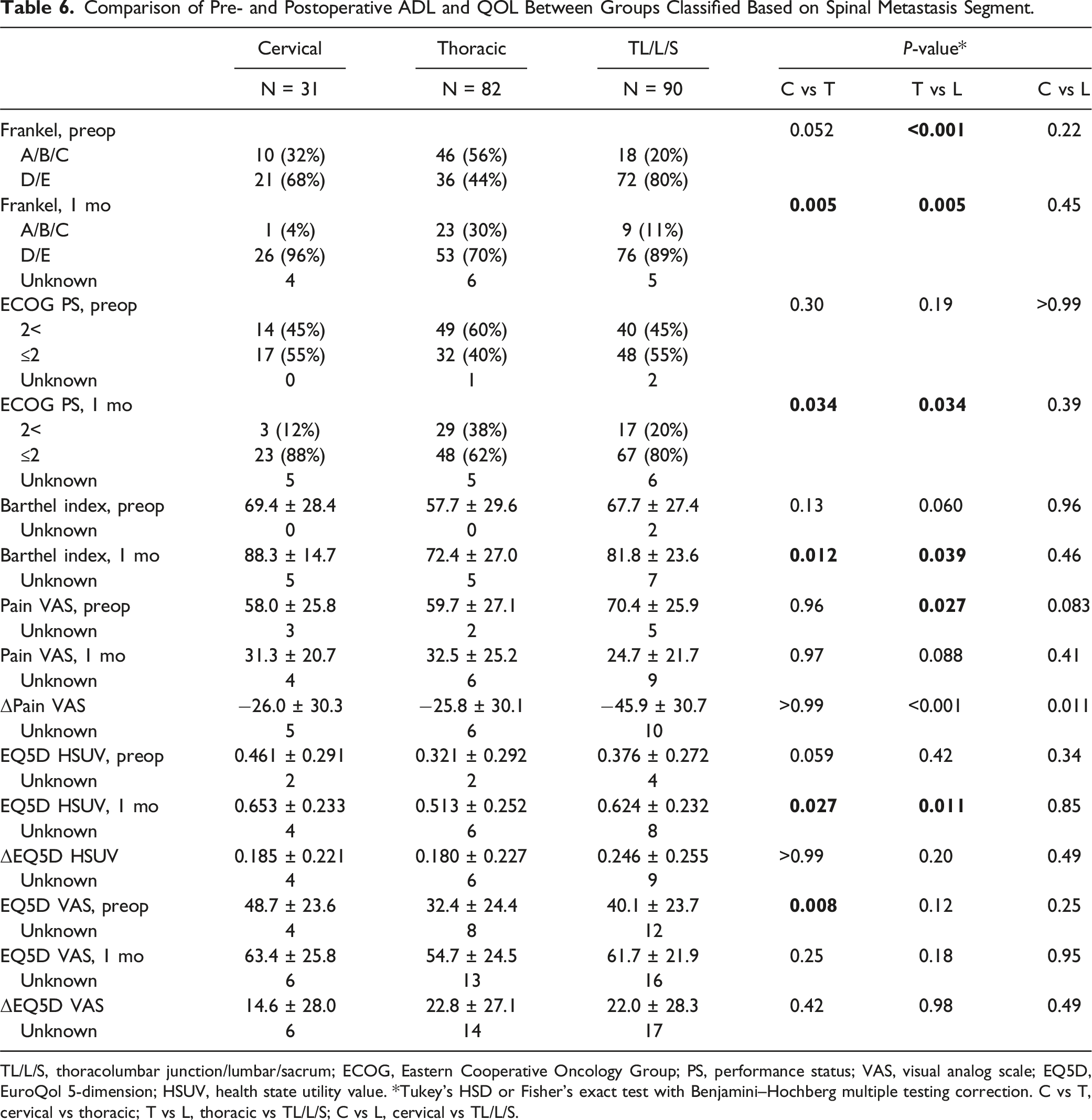
TL/L/S, thoracolumbar junction/lumbar/sacrum; ECOG, Eastern Cooperative Oncology Group; PS, performance status; VAS, visual analog scale; EQ5D, EuroQol 5-dimension; HSUV, health state utility value. *Tukey’s HSD or Fisher’s exact test with Benjamini–Hochberg multiple testing correction. C vs T, cervical vs thoracic; T vs L, thoracic vs TL/L/S; C vs L, cervical vs TL/L/S.
The preoperative EQ5D HSUVs were not significantly different between the three groups. However, the postoperative EQ5D HSUVs were significantly worse in the thoracic group than in the cervical (P = 0.027) and TL/L/S (P = 0.011) groups. The postoperative EQ5D VAS was not significantly different between the groups. No difference in the amount of change in these EQ5D values was observed between the groups (Table 6). Preoperatively, significantly more patients scored higher (worse) in the mobility domain in the thoracic group than in the cervical and TL/L/S groups. Furthermore, significantly more patients scored higher in the self-care domain in the thoracic group than in the cervical group. However, there were no differences in the pain/discomfort and anxiety/depression domains between the groups. One month postoperatively, relatively more patients in the thoracic group than in the cervical and TL/L/S groups demonstrated persistently poor scores in the mobility, self-care, and usual activities domains. However, the differences were not significant. Both pain/discomfort and anxiety/depression domains improved in the majority of patients in all the groups (score, 1-2) (Figure 5). Comparison of the pre- and postoperative EQ-5D-5L between the groups classified on the basis of spinal metastasis segment. EQ-5D-5L, EuroQol 5-dimension 5-level; TL/L/S, thoracolumbar junction/lumbar/sacrum. *Significant in Fisher’s exact test with Benjamini–Hochberg multiple testing correction.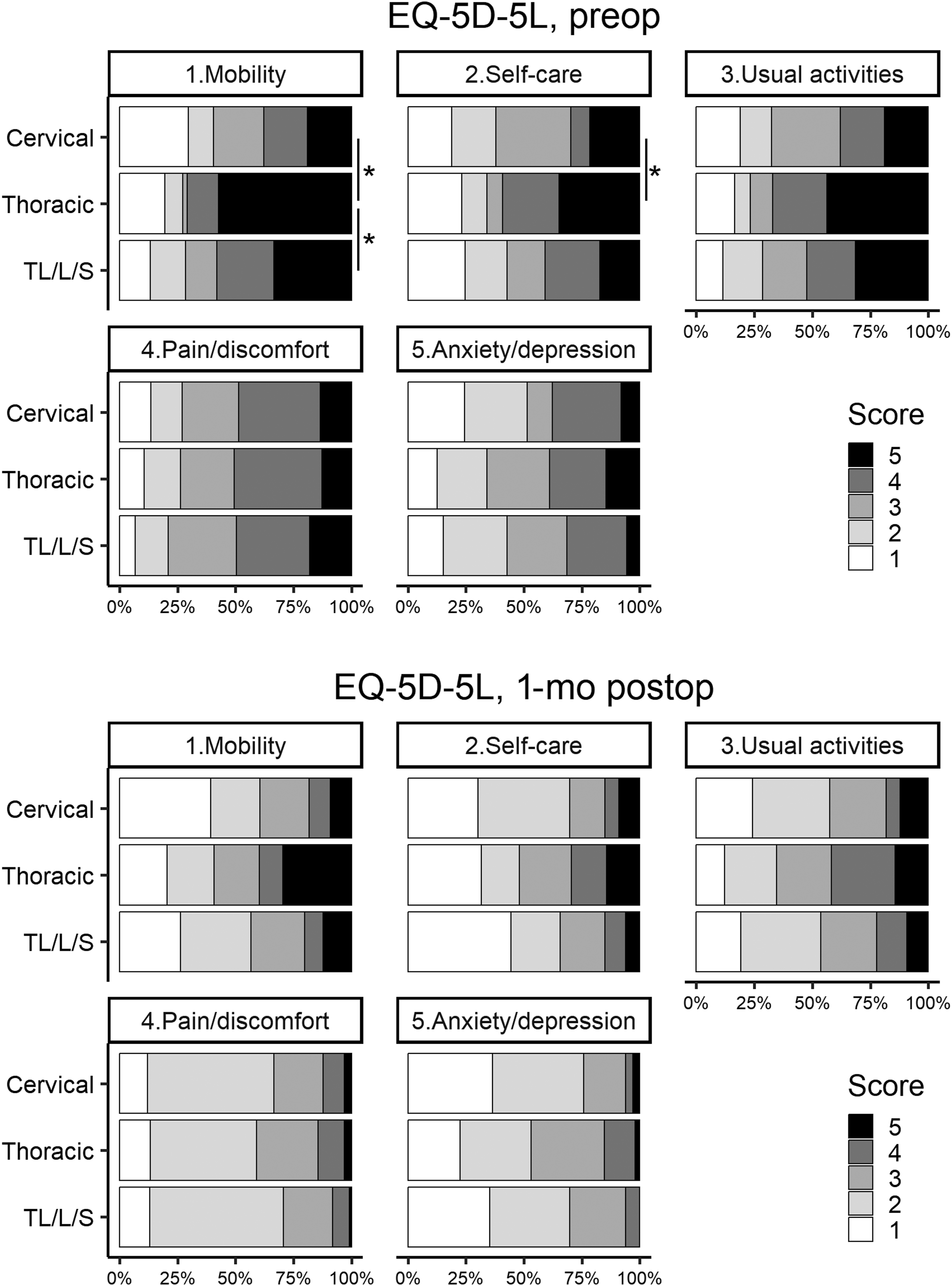
Discussion
This study compared patients with metastatic spinal tumors at different segments who underwent surgical treatment. The patients were divided into three groups according to the metastasis segment. All groups showed significant postoperative improvement in the Frankel grade, ECOG-PS, pain VAS, Barthel index, and EQ5D HSUV/VAS. Although the preoperative EQ5D HSUVs did not significantly differ between the groups, the postoperative EQ5D HSUV was significantly lower in the thoracic group than in the cervical and TL/L/S groups. However, the postoperative EQ5D VAS and postoperative EQ-5D-5 L scores in all the domains were not significantly different between the groups. Thus, although patients with metastases in the upper and middle thoracic spine had poorer QOL outcomes than those with metastases in other segments, palliative surgery provided comparable QOL improvements in all the groups.
Symptomatic spinal metastases develop in approximately 10% of all patients with cancer, and 5%–10% of these patients require surgical intervention. 22 Advancements in cancer treatment have led to increased life expectancy; consequently, the number of patients with spinal metastases and the need for their management are also increasing. 1 Spinal metastasis is considered a terminal stage of cancer, and the predicted prognosis determines the need for surgery. 23 This view is partially validated by the fact that performing spinal surgery on patients with a reduced life expectancy may lead to negative outcomes and burden the patient. However, spinal metastases can lead to progressive paralysis, impaired voiding, severe pain, and even anxiety.1,3,4 Thus, the effects of these symptoms on patients’ QOL during their remaining life are enormous. Dea et al 23 demonstrated that baseline PS is more important than life expectancy for maintaining and improving QOL in patients with spinal metastases, indicating that QOL at 6 weeks postoperatively is independent of survival chance. Therefore, basing the need for surgery on predicted life expectancy is not appropriate.
Despite the drastic increase in the number of patients with spinal metastases, the details regarding QOL are poorly understood. According to Choi et al, 16 the independent predictors of a high postoperative EQ5D score (good QOL) are a high preoperative EQ5D score, good preoperative Frankel grade (grades D and E), and high preoperative Karnofsky Performance Scale (KPS) score. Considering that KPS is primarily an assessment of the patient’s mobility, their study results indicate that the degree of preoperative paralysis is the primary determinant of postoperative QOL. Our study results were similar; patients in the thoracic group demonstrated significantly more severe preoperative paralysis and significantly worse postoperative EQ5D HSUV than patients in the cervical and TL/L/S groups. However, the postoperative EQ5D VAS was not significantly different among the three groups, and there were no significant differences in each EQ-5D-5 L domain. Although patients in the thoracic group did not experience greater improvements in paralysis following surgery, they did not demonstrate significantly poorer improvements in QOL, including in the pain and anxiety domains.
The minimum clinically important difference (MCID) in QOL for patients with cancer based on the EQ-5D-5L is not yet well understood. Hu et al 24 determined that the mean MCID for EQ5D HSUV was 0.039 in patients with cervical intraepithelial neoplasia. Furthermore, Zheng et al 25 found that the mean MCID for EQ5D HSUV was 0.071 in patients with coronary heart disease. In our study, all groups demonstrated a greater recovery of EQ5D HSUV than in those studies. In our study, palliative surgery for metastatic spinal tumors was associated with a sufficient improvement in EQ5D HSUV, even in the thoracic spine, where EQ5D HSUV was significantly lower. Thus, palliative surgical treatment for spinal metastases plays an important role in restoring patients’ QOL, regardless of the segment of the metastatic lesion.
In our study, the higher preoperative pain VAS score in the TL/L/S group than in the other two groups indicates that lesions at the TL/L/S segment cause significantly more pain than lesions at other spinal segments. This result is unexpected as the cervical group had the highest SINS (indicating unstable). Although an unstable cervical spine causes severe paralysis, this finding may mean that an unstable lumbar spine, which supports the trunk, causes more pain for patients. Decompression surgery without stabilization is rarely indicated for spinal metastases due to the high risk of subsequent spinal instability. 26 Stabilization is beneficial not only for unstable lesions but also for potentially unstable thoracic and lumbar lesions. 27 Thus, in our study cohort, which included many potentially unstable or unstable cases, performing stabilization in most cases may have contributed to symptom improvement. The TL/L/S group did not score significantly worse than the other groups in the pain/discomfort domain in the EQ-5D-5L.
Furthermore, these results showed that although neurological pain is more likely to be experienced by patients with lesions at the TL/L/S region, patients experience a similar degree of pain or discomfort in metastases at any spinal segment. Pain and discomfort not only negatively impact the QOL but also affect the mental status and neurological recovery. Worsening pain, impaired physical functioning, and difficulty in treatment are associated with depressive symptoms. 28 Furthermore, depression and anxiety are associated with poor efficacy of surgical treatment for cervical myelopathy. 29 Thus, improvement of pain and discomfort is one of the most important goals for treating patients with spinal metastases. The fact that the EQ-5D-5L pain/discomfort domain improved in all groups following surgical treatment indicates that surgical treatment improves patients’ QOL.
The fact that relatively more percutaneous and minimally invasive procedures were performed in the TL/L/S group than in the other groups may have influenced the results. Minimally invasive procedures are associated with a lower incidence of postoperative complications in patients with spinal metastases, improved pain and outcomes, and better QOL.30,31 Nevertheless, the cervical group was treated with open conventional surgeries because of the inherent challenges associated with performing percutaneous procedures on the cervical spine. In contrast, some patients in the thoracic and TL/L/S groups underwent minimally invasive procedures. However, the percentage was considerably higher in the TL/L/S group. These circumstances may have contributed to the fact that the TL/L/S group exhibited the largest pain VAS change. However, no difference in the extent of change in EQ5D values was observed between the groups. In other words, minimally invasive surgery may be effective in pain management. However, the optimal method selected for each patient resulted in an overall improvement in QOL.
This study has several limitations. First, the outcome was assessed after a short period, 1 month postoperatively. However, previous reports have demonstrated that EQ5D HSUV recovery almost reaches a plateau at 1 month postoperatively. 19 Therefore, it is possible to compare the impact of spinal surgery at different segments, even at 1 month postoperatively, to observe the short-term effects of surgery. Second, the study’s sample size was relatively small. Third, because the study collected limited imaging findings, it was not possible to assess the severity of epidural compression (e.g., Bilsky classification) that might affect neurologic recovery. Fourth, the groups divided by segment of the spinal lesion were essentially heterogeneous populations. Significantly more patients in the thoracic group than in the cervical and TL/L/S group had preoperative paralysis. However, because the thoracic spine includes the spinal segments most vulnerable to compression, 32 these background differences among the groups were inevitable. Additionally, the variables collected did not include the degree of comorbidities or the American Society of Anesthesiologists score, which may affect the outcomes. Despite these limitations, the strength of this study lies in that it was a multicenter prospective study, which ensured that the QOL was assessed and analyzed.
Conclusion
This study prospectively compared the outcomes of palliative surgical treatment in patients with spinal metastatic patients located in the cervical, thoracic, and TL/L/S regions. All three groups demonstrated an improvement in the Frankel grade, ECOG-PS, pain VAS, Barthel index, and EQ5D HSUV/VAS postoperatively. Although the preoperative EQ5D HSUVs were not significantly different between the groups, the thoracic group (T1–10 lesion) demonstrated significantly lower postoperative EQ5D HSUVs than the other two groups. Conversely, the postoperative EQ5D VAS and EQ-5D-5 L domain scores were not significantly different between the groups. Thus, although patients with metastases in the upper and middle thoracic spine had poorer QOL outcomes than those with metastases in the other segments, palliative surgery was associated with QOL improvement in all the groups.
Footnotes
Acknowledgments
We would like to appreciate Dr. Kazuhide Inage, Department of Orthopaedic Surgery, Chiba University, for the secretariat. We would like to appreciate Dr. Katsumi Harimaya, Department of Orthopaedic Surgery, Kyushu University; Dr. Hideki Murakami, Department of Orthopaedic Surgery, Nagoya City University Medical School; Dr. Yasuchika Aoki, Department of Orthopaedic Surgery, School of Medicine, Chiba University; Dr. Seiji Okada, Department of Orthopaedic Surgery, Osaka University Graduate School of Medicine; Dr. Kei Ando, Department of Orthopaedic Surgery, Japan Red Cross Aichi Medical Center Nagoya Daini Hospital for their efforts in managing the Japan Association of Spine Surgeons with Ambition (JASA) organization. Moreover, we thank all members of JASA for collecting the data. We would like to thank Enago (![]() ) for the English review.
) for the English review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.