
Abstract
Study Design:
Cross-sectional study.
Objective:
Recently, there has been a rise in children and adolescents developing low back pain and/or sciatica. Degenerative lumbar spine MRI phenotypes can occur in this population but reports have been sporadic and the true incidence of such spine changes remains debatable. As such, the study aimed to address the epidemiology of MRI phenotypes of the lumbar spine in this young population.
Methods:
597 children and adolescents with lumbar MRIs were included in the study. T1- and T2-weighted lumbar images from L1/2 to L5/S1 were analyzed in axial and sagittal planes. Global phenotype assessment was performed of each level and based on established nomenclature protocols.
Results:
The cohort consisted of 57.3% (342) boys and 42.7% (255) girls, with a mean age of 10.75 ± 5.25 years (range: 0 to 18 years). The prevalence of imaging findings of lumbar disc degeneration (LDD) and lumbar disc herniation (LDH) were 2.2% (95% CI: 0.93–3.43) and 5.8% (95%CI: 2.58-8.99), respectively. There was significant difference between each disc segment from L1/2 to L5/S1 for both LDD and LDH. Schmorl’s nodes were noted in 16 cases (2.7%, youngest case as 15 years), with 11 boys (68.8%) and most frequent segment as L3/4. Modic changes and high-intensity zones were absent in this cohort.
Conclusions:
LDD can emerge as early as the first decade of life with Schmorl’s nodes, without additional specific phenotypes, including Modic changes and high-intensity zones. The study provides valuable information of a unique age group that is often under-represented but equally important as adults.
Introduction
The incidental changes of lumbar discs, such as lumbar disc degeneration (LDD) and lumbar disc herniation (LDH), are involved in several lumbar disc pathologies, negatively affecting adults’ work and lives globally. A sum of 380,305 patients underwent surgical treatment for lumbar disc diseases between 2000 and 2009 in the United States. 1 However, the number of patients is much more than the surgical cases in fact, due to part of patients seeking an alternative treatment, such as epidural injection. 2 To date a majority of the studies concerning these changes are about adults. There is a paucity of evidence regarding lumbar disc changes reflected by diagnostic findings in children and adolescents in the literature.
So far, the prevalence of incidental changes of the lumbar spine in children and adolescents mainly derives from retrospective studies screened with magnetic resonance imaging (MRI). Kumar et al retrospectively analyzed 742 patients with lumbar disc disease for 11 years in India. 3 They identified the incidence of LDH in pediatric and adolescent populations was 3.5% (25/742, aged 20 years or less). Wang et al reported the prevalence of LDH as 2.6% (121/4695, age 13-20 years). 4 The prevalence of LDD in subjects (age range 10-19 years) suffering from low-back pain (LBP) and in age-matched asymptomatic controls was investigated in Paajanen’s study. 5 Disc degeneration was defined as a reduction in signal intensity of the nucleus pulposus on sagittal T2-weighted images in MRI. 6 The incidence of LDD in LBP subjects was 41.25%, while the prevalence in asymptomatic controls was 23.8%. Maurer et al compared the lumbar spine findings in asymptomatic adolescent rowers and age-matched asymptomatic controls. 7 The incidence of LDD was 18.4% in rowers, 9.1% in controls. The rate of disc herniation and disc bulge was 9.1% and 4.5% respectively in rowers, compared to 0% and 4.5% for controls. The prevalence of specific imaging findings in the lumbar spine of 439 children (aged 12-14 years) in Denmark was investigated in a previous study. 8 The prevalence of LDD was 21.4%, which was assessed according to the criteria of Weishaupt. 9 The incidence of HIZ was 5%, while the incidence of Modic changes was 0.5%.
Although several studies focusing on the incidental changes in lumbar discs involving children and adolescents were reported, the actual prevalence of these changes is difficult to reckon across multiple studies due to the differences in criteria for abnormal ratings. For example, not only the signal intensity varation of the nucleus pulposus should be considered when identifying the LDD, the disc height change, and spondylosis deformans should also be considered. LDH consists of disc bulging, disc protrusion, disc extrusion, and sequestration. However, no previous studies explicitly clarify the criterion of LDH in the methods section. Also, the purpose of these studies has varied widely, with some focusing on the comparison of incidence between symptomatic and asymptomatic populations, 5 while others focused on the risk factors of the positive findings, 10 or focused on the impact of competitive sports on the positive finding in the lumbar spine. 9 None of these studies have described in detail the incidence of various changes in lumbar disc MRI. Regardless, to our knowledge, no large-scale epidemiological study has been addressed to report on the prevalence of incidental MRI findings in children and adolescents, ranging from 0 to 18 years of age.
The updated nomenclature of lumbar disc pathology released in 2014 opens a new era for clinicians and researchers in the understanding of MRI phenotypes. 11 Based on a study by Zhang and colleagues, a large scale cross-sectional study, consisting of 5,288 consecutive cases (26 440 lumbar discs), was performed and published in 2016. 12 In the study, the authors reported the MRI imaging findings of lumbar discs of the Chinese population. In lieu of the aforementioned limitations in the literature addressing the MRI phenotypes of the lumbar spine in children and adolescents, we conducted a cross-sectional epidemiological study to address such shortcomings.
Methods
The study was approved by the institutional review board of a tertiary teaching hospital with a considerable patient volume (Number: 200 803 006). The study was conducted based upon the Centricity® Picture Archiving and Communication System (PACS, GE Healthcare Pty Ltd, Piscataway, New Jersey, USA) in the tertiary teaching hospital. All lumbar spine magnetic resonance (MR) images were widely reviewed from January 2008 to December 2010. The exclusion criteria were cases with congenital deformities, infection, and previous surgery in the lumbar spine. Only the cases aged below 19 years with the intact lumbar MRI images were included. Patients’ informed consent was not acquired since the study was a pure imaging observational study without intervention with diagnosis or treatment of patients. The reasons of performing MRIs were various, both symptomatic including specific (such as enuresis, low back pain) or systemic symptoms (such as tuberculosis) or congenital/idiopathic deformities (scoliosis), injury, back/low back pain/leg pain; and asymptomatic (sacrum subfissure).
All cases underwent MRI on a 1.5 T MR scanner (MAGNETOM Aera, Siemens AG, Erlangen, Germany) with the integrated spine coil. The T1-weighted sagittal, T2-weighted sagittal, and axial lumbar MRI images were acquired using a standard TSE sequence. MRI images of the L1/2 to L5/S1 were analyzed.
According to the nomenclature version 2.0 11 and the Pfirr-mann grading scheme, 13 the condition of lumbar discs was classified as follows:
A (Normal), B (Blurred disc as early stage of LDD), C (Black disc), D (Black+bulging disc), E (Decreased height + protrusion disc), F (Pure bulging disc), G (Pure protrusion), H (Extrusion), I (Sequestration), J (Schmorl's node, SN), K (Modic change type I), L (Modic change type II), M (Modic change type III), N (Spondylosis deformans), O (Pure decreased disc height), P (High-intensity zone, HIZ). 12
Two experienced spine surgeons (two of the authors) specializing in spinal diseases assessed the MRI of all cases, respectively. Over 1 month interval, these cases were reassessed by the same surgeons. Referring to the imaging diagnostic reports, a senior spine surgeon (one of the authors) examined the assessment results. All authors discussed cases with divergence, and then the consensus was reached. The phenotypes with corresponding letters were recorded in a spreadsheet.
The lumbar discs were defined as normal when all lumbar discs of a case were classified as A. Once one lumbar disc belongs to any type as B, C, J, K, L, M, N, O, or P, the case was defined as LDD. If one lumbar disc was classified as F, G, H, or I, the case was defined as LDH. The case was defined as LDD and LDH when one disc was D or E, or one disc as degeneration with another as herniation.
Statistical Analysis
All data were analyzed with SPSS 19.0 (SPSS Co., Chicago, Illinois, USA). Intraobserver variability and interobserver variability was measured with the Kappa statistic. Continuous data, such as the average age of the cohort, was expressed as the means and standard deviations, and categorical variables were presented as percentages. The proportion of incidental findings was calculated, with the corresponding 95% confidence interval (CI). A chi-square test was performed to compare the portion of disc degeneration and herniation for each lumbar segment. Prevalence of imaging findings of lumbar disc degeneration and herniation in each segment for the individual with LDD and LDH was noted. The threshold of significance was set as a P value of less than .05.
Results
A good to excellent intra- and inter-observer reliability was reached in the evaluation of included lumbar spine MRI (>0.89).
Subjects Demographics
Overall, 613 (11.6%) cases aged below 19 years (range: 0 to 18 years) among 5,288 cases were screened. Ten cases with congenital lumbar deformities, 1 case with lumbar infections, and 5 cases with previous surgery in the lumbar spine were excluded. Overall, 597 subjects (2,985 lumbar discs) were included in the current study. The cohort of children and adolescents consisted of 57.3% (342) males and 42.7% (255) females (Figure 1). The average age of the cohort was 10.8 ± 5.3 years (range: 0 years to 18 years, Table 1).
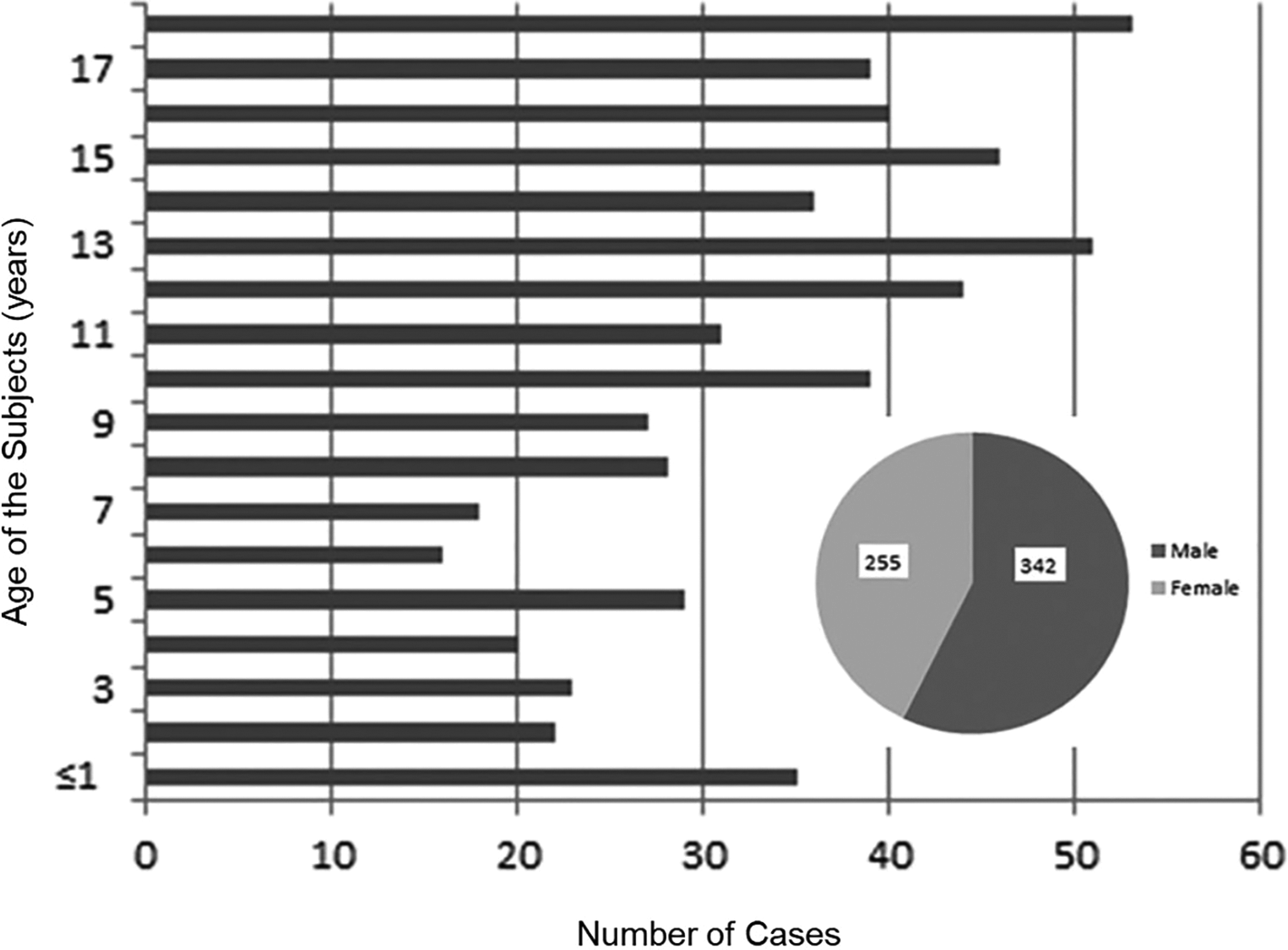
Demographics of study subjects.
Demographic Characteristics of Children and Adolescents.
N* = number.
LDD and LDH Epidemiology
According to the nomenclature, the prevalence of LDD was 2.2% (95% CI: 0.93-3.43). For the individuals with LDD, the incidence of disc degeneration from L1/2 to L5/S1 was 27%, 30%, 30%, 40%, and 40%, respectively. Furthermore, the difference of disc degeneration incidence between each segment and the overall prevalence was found with statistical significance (P < .05). In degenerated segments, L1/2, L2/3, L3/4, L4/5, and L5/S1 accounted for 16%, 18%, 18%, 24%, and 24%, respectively. The difference among each segment was found with statistical significance (P < .05), except for the difference between L2/3 and L3/4, L4/5, and L5/S1.
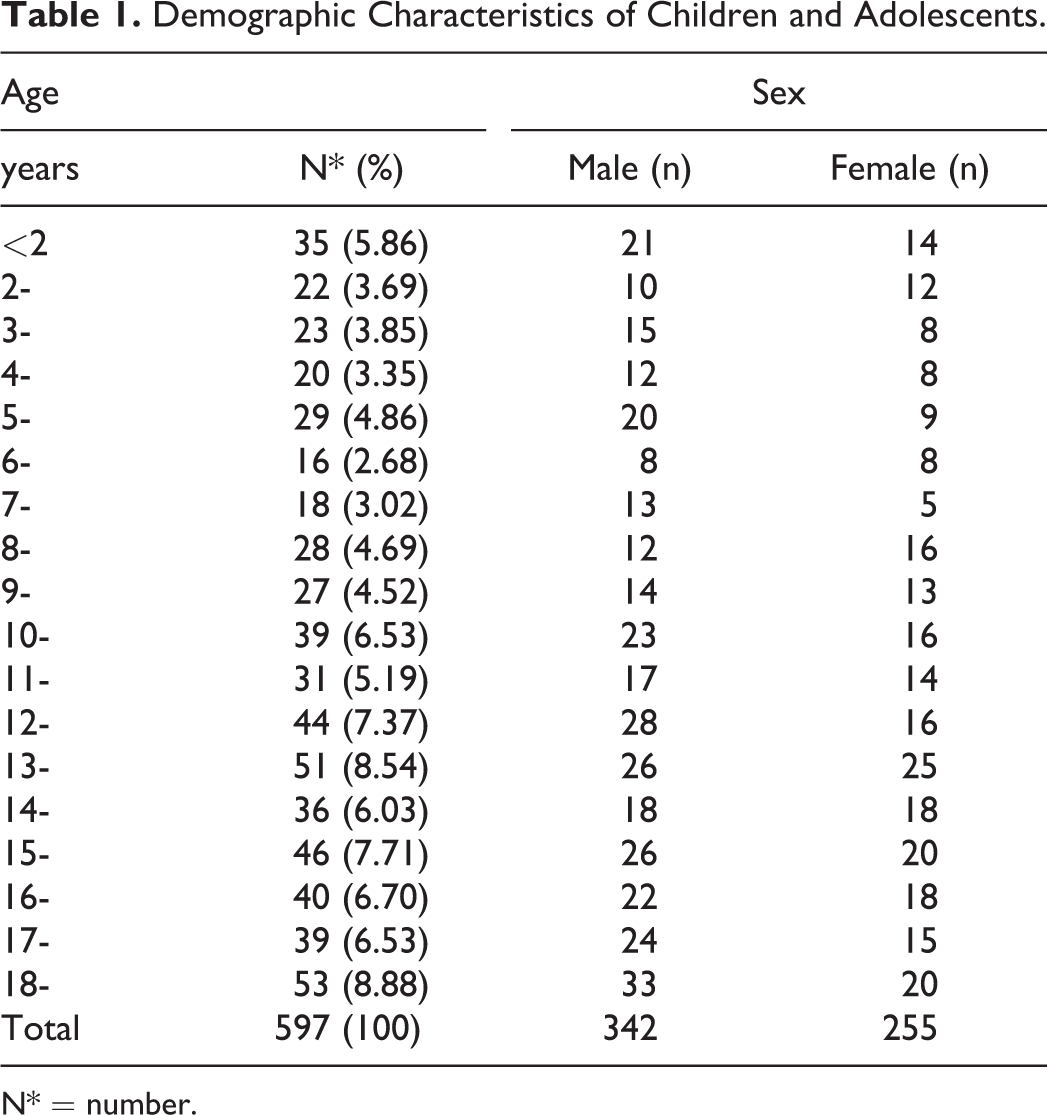
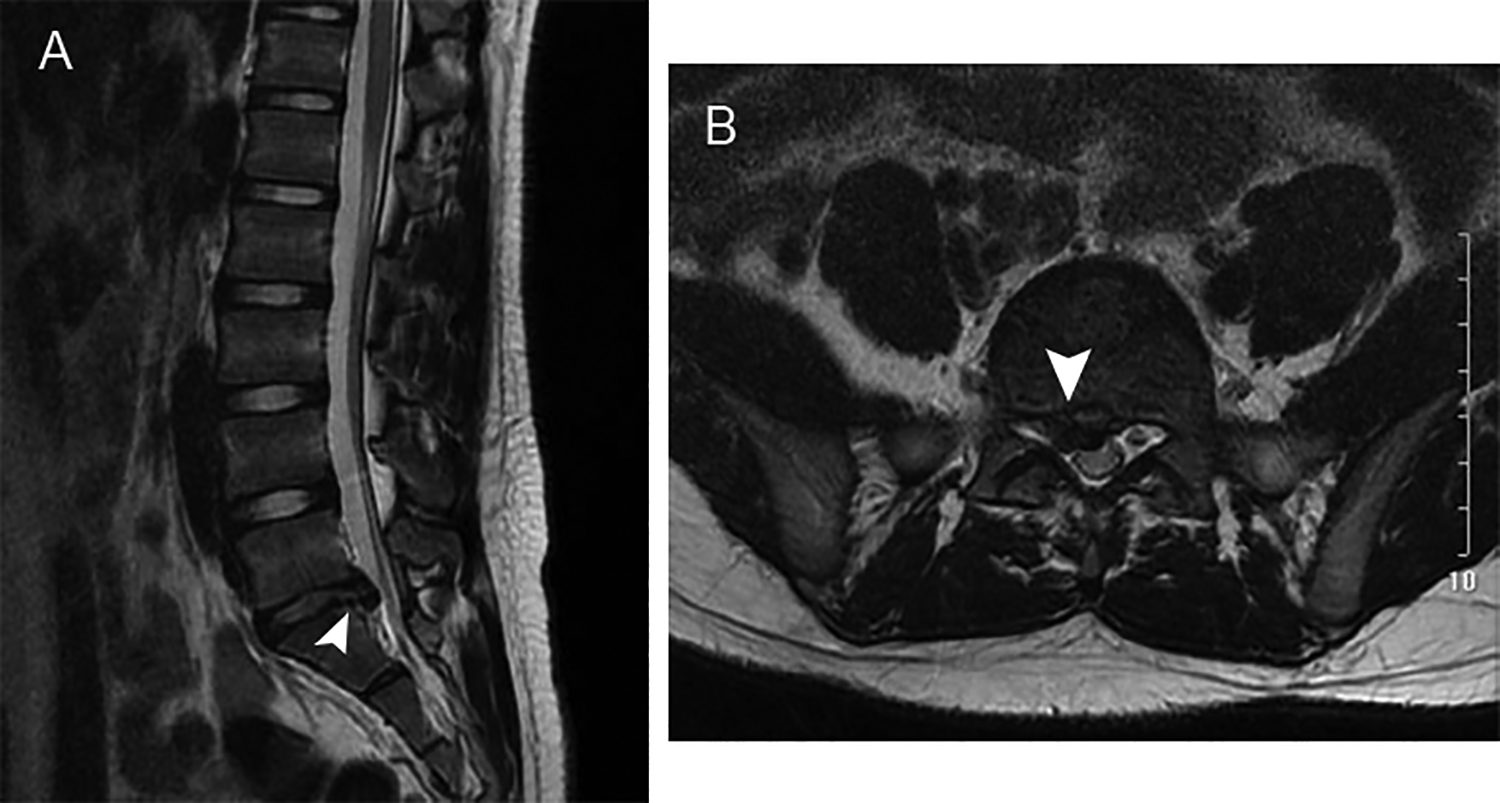
The prevalence of LDH was 5.8% (95% CI: 2.58-8.99). For the individuals with LDH, the incidence of disc herniation from L1/2 to L5/S1 was 2.9%, 2.9%, 17.1%, 57.1%, and 65.7%, respectively. The MR images of a 14-year-old case with herniation in L5/S1 are shown in Figure 2. The MR images of another 14-year-old subject with herniation in L4/5 and L5/S1 are noted in Figure 3. The difference of disc herniation incidence between each segment and the overall prevalence was found with statistical significance (P < .05). The segments of L1/2, L2/3, L3/4, L4/5, and L5/S1 accounted for 2.0%, 2.0%, 11.8%, 39.2%, and 45.1% of all herniated segments, respectively. The difference among each segment was found with statistical significance (P < .05), except for L1/2 and L2/3.
A 14 year-old child with a herniation at L5/S1, demonstrated on sagittal (A) and axial (B) MRI view of the lumbar spine, respectively.
A 14 year-old child with a herniation at L4/5 and L5/S1, as noted on sagittal (A) and axial ( B and C) MRI views of the lumbar spine, respectively.
Specific Phenotypes
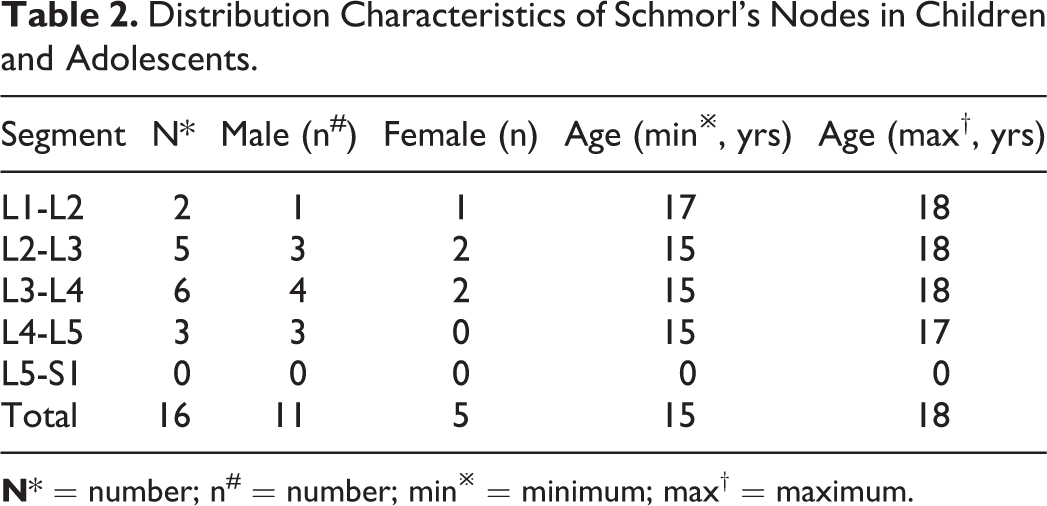
SNs were observed in 16 cases (2.68%, 95% CI: 1.31-4.41) of all subjects. Eleven cases were males (68.75%); the other 5 cases were females (31.25%). The distribution characteristics of SNs are shown in Table 2. SNs occurred mostly in the segments of L3/4, then in L2/3. SNs were observed in children as young as 15 years old. Other specific phenotypes, such as Modic changes and HIZ, were not found in the cohort.
Distribution Characteristics of Schmorl’s Nodes in Children and Adolescents.
Degeneration Grading
According to the Pfirrmann classification scheme, the degeneration grading corresponding to each segment was performed (Figure 4). As shown in Table 3, the highest distribution was grade Ⅰ, the proportion of which was 96.38% (2877 discs). The second was grade Ⅲ, which comprise 1.71% (51 discs) of all discs, observed mostly in the segment of L4/5, then in L5/S1. A thirteen-year-old case with degeneration graded as Ⅲ in L4/5 and herniation in L5/S1 was displayed in Figure 5. The minimum age case of grade Ⅲ was 10-year-old. The percentage of grade Ⅱ was 1.47% (44 discs). The minimum age case of grade Ⅱ was twelve-years-old. Grade Ⅱ mostly appeared in the segment of L5/S1. The proportion of grade Ⅳ was lowest, 0.44% (13 discs)—the minimum age case of grade Ⅳ was 11. Grade Ⅳ appeared mainly in L3/4, L4/5, and L5/S1.
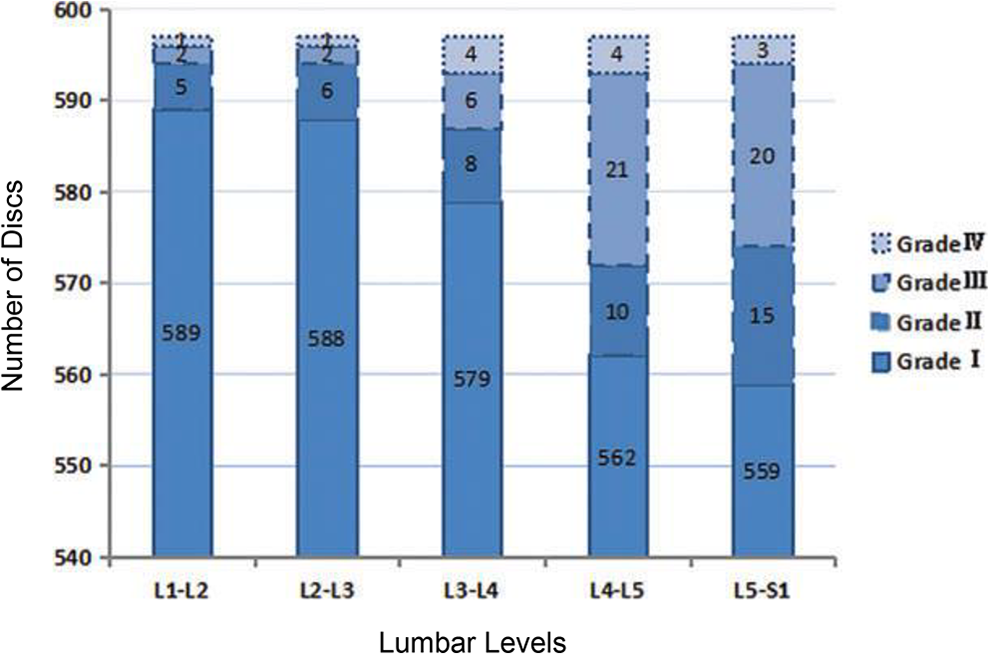
The degeneration grading findings corresponding to each segment. Different borders represent grades of I, II, III, and IV, respectively.
Grade Distribution of Disc Degeneration for Each Lumbar Vertebral Level as Classified with the Pfirrmann Scheme.
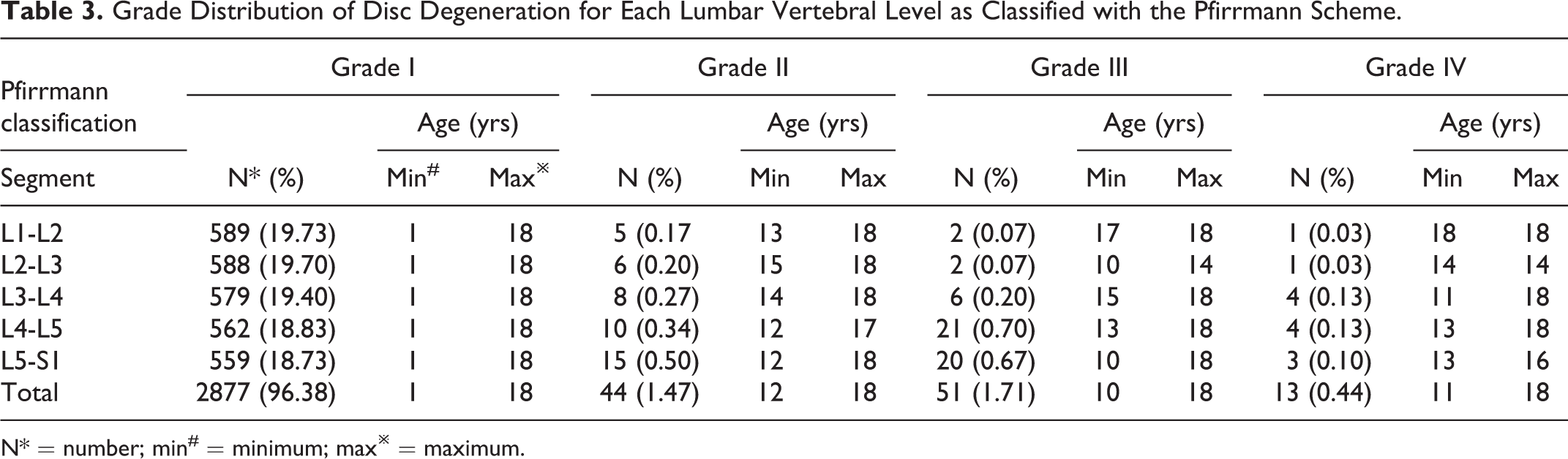
N* = number; min# = minimum; max※ = maximum.

A 13 year-old child with degeneration graded as grade Ⅲ at L4/5 and herniation at L5/S1.
Discussion
To our knowledge, this is one of a few studies concerning the prevalence of incidental MRI changes in children’s and adolescents’ lumbar spine. Based on the latest version of lumbar disc nomenclature for adults, and abundant case data, the prevalence of several incidental findings was ascertained. 11
LDD and LDH
By general consent, LDD and LDH are among the most common form of incidental changes of the lumbar disc. However, due to the sparse literature and vague definition for the young population, the prevalence of these incidental changes in children and adolescents remains unclear. By assessing the MRI images of 597 individuals, we found that the prevalence of imaging findings of LDD and LDH in children and adolescents was 2.17% and 5.84%, respectively. Such a figure was far below the data of adults in our previous study, compared with 44.23% and 14.18% for LDD and LDH in adults, respectively. 12
Employing the Pfirrmann scheme, the distribution of the degeneration was revealed in the present work. The incidence of grade Ⅱ, grade Ⅲ, and grade Ⅳ was 1.47%, 1.71%, and 0.44%, respectively. No grade Ⅴ cases were found. The identified LDD occur as early as 10 years in MRI. A previous study comprising 103 children (1-15 years) with an average age of 6.6 years indicated that 3.49% of the lumbar discs were classified as Pfirrmann grade Ⅱ. 14 However, no discs were classified as grade Ⅲ, grade Ⅳ, and grade Ⅴ. The difference in the patients’ demographics among the 2 studies may account for the discrepancy in degeneration distribution. A much younger population was evaluated in the previous study, which explains all the discs graded as grade I or grade Ⅱ.
As shown in the results, the prevalence of LDH imaging findings in all cases was 5.84% in our work. Similar findings were reported by several studies with the incidence varying from 1% to 5% in age 20 years or less.3,4,15 A previous study reported that L4/5 is the segment most commonly involved in LDH. 3 In contrast to these findings, we found that the occurrence of LDH from L1/2 to L5/S1 is increased gradually, and L5/S1 is the most commonly affected level. For children and adolescents, disc herniation is mostly centrolateral type, then is the central type. LDH of adolescents’ discs in most cases is subligamentous, whereas extruded disc is rare. 3 The most common level suffered from LDH is L4/5 in adults. For adults, central or central-lateral herniation with an intact posterior longitudinal ligament (PLL) predominates in the upper lumbar region. In contrast, in the lower lumbar region, posterior-lateral extrusion with a ruptured PLL is predominant. 16 Ramadorai et al indicated that LDH in children and adolescents is more frequently related to trauma as opposed to the degenerative causes in adults. 17 Several studies demonstrated that trauma and accumulated micro-trauma (injury in intense sports activity) are strong predispositions of LDH.18,19 However, others revealed that the microscopic degenerative changes in disc and endplate might be responsible for LDH in this particular population, and trauma may aggravate these changes subsequently. 3
Disc degeneration was characterized as a multifactorial disease, in which the biomechanical factor is thought to be of high importance. It has been hypothesized that the degeneration in the lower discs is more often and earlier since weight-bearing by the lower lumbar discs is much greater than upper lumbar discs, and the axial rotation cause increased shearing load at the lumbosacral junction. 15 As shown in the results, to each segment, the occurrence of LDD from L1/2 to L5/S1 was increased gradually. We demonstrated that juvenile disc degeneration is strongly associated with overweight and obesity. 10 This finding was consistent with the discovery in adults. 20
Increasing evidence indicated that disc degeneration is age-related and tends to become more severe with growing age, initiating as early as childhood and adolescence, developing and deteriorating in adulthood.21,22 A previous study demonstrated that the percentage of subjects with LDD under 30 was 42%. This percentage increases to 48% in the age group of 30 to 39 years, whereas 70% of subjects in the 40 to 49 years age group were affected by LDD, and this proportion rising to 88% among subjects 50 years of age. 23
Intriguingly, what sorts of factors contributed to LDD in children and adolescents? Several studies concerning the young athletes have shown that this particular population suffered from a higher frequency of intervertebral disc degeneration (IDD) and abnormalities.24,25 A prospective 3-year cohort study of 12 child and adolescent weightlifters revealed abnormal lumbar findings in 11 participants, including 9 LDD cases. Resistance training at the competition level could potentially influence the lumbar spine of children and adolescents, inducing irreversible changes in the lumbar spine without symptoms. 26 The further intensive study revealed that injury to the spine during the growth spurt has etiological importance for the early degenerative process in children and adolescents. 27
Enormous evidence has shown that genetic influences, which predispose individuals vulnerable to disc degeneration, play a significant role in IDD.28,29 Gene variations reported previously are associated with the genes encoding cytokines (ie, inflammatory factors), disc components and metabolic members in IDD.30,31 However, only a few genes have been verified in different ethnic populations. Besides, it seems that a particular gene is associated with IDD at only a specific age. 32 A study taken in a young adult cohort with a mean age of 21 years indicated that single nucleotide polymorphisms (SNP) in IL6, SKT and CILP were associated with moderate IDD. 33 Mutations in the gene that encodes collagen and aggrecan were also suggested as a genetic risk factor for LDH in a study with a mean age of 24 years. 34 While genetic variations of the disc component impair the structural integrity and strength of the disc, the subsequent environmental factors accelerate the degenerative process. This hypothesis was proved in the athletes. A considerably higher incidence of degenerative changes in the athletes was widely reported in the literature.24-26 Long-term intense training regimens, combined with the genetic predisposition, led to an increased risk of disc degeneration in particular teen athletes. 35 In combination of clinical raw data investigation of our included cases, back/low back pain due to heavy schoolbag was a frequent cause for MRI scans. Indeed, the association of back pain and schoolbag use has been confirmed by a large-scale cross-sectional study among 5318 Italian children and adolescent students (aged 6 to 19 years). 36
SNs
SNs were first described in 1927 and have since been commonly found and reported. 37 Lots of evidence confirmed that SNs are not only associated with several pathologies of the lumbar spine, also occurring in the healthy adult population. The prevalence of SNs in the adult population reported previously ranges from 2% to 76%, depending on the diagnostic criteria and modality.38-43 Compared to that, the prevalence of SNs in children and adolescents observed in the current work was 2.68%. We found a higher frequency of SNs in males than in females, consistent with the study conducted in adults. 38 Overwhelming evidence revealed no significant relationships between the presence of SNs and age, weight, and BMI.23,38 The relation between disc degeneration and SNs in the lumbar spine is not clear. A few studies suggested that SN occurrence is positively correlated with lumbar disc degeneration grade. 38
A study in young elite skiers (age ranged from 16-years to 20-years) demonstrated that SNs are significantly more prevalent in skiers than controls, indicating that the cause of SNs may be from direct trauma. 24 In accordance with these findings, in another study, more SNs were found at the fractured vertebrae’s endplates than at the normal levels, which indicated that a vertebral fracture in childhood is a risk factor for SNs. 44 Autopsy research in adolescents and young adults revealed that SNs could occur as a result of acute trauma in a motor vehicle accident, primarily associated with the excess axial loading on the spine. 45 Schmorl's nodes in children and adolescents have been shown to be associated with jumping activities in sports. 46
By convention, the lumbar spine is divided into upper lumbar (L1/2, L2/3, and L3/4) and lower lumbar spine (L4/5 and L5/S1). As shown in the results, SNs occurred more frequently in upper lumbar discs than lower lumbar discs. SNs were mostly observed in the segments of L3/4, whereas SNs were least observed at the L5/S1 vertebral level. This finding was similar to that found in adults. 38 It is believed that compared to the lower lumbar, the upper lumbar are more susceptible to injury. The higher prevalence of SNs in these regions of the spine supports the hypothesis that trauma is a risk factor for the occurrence of SNs. 47 Furthermore, a previous biomechanical study revealed that a fracture of the endplate happened first before the disc injured, when compression stress is applied on the spine of children and adolescent. This suggested that SNs in healthy children and adolescents may happen as the result of trauma, causing herniation of the disc tissue and violating the endplate. 44
HIZ and Modic Changes
The particular degenerative findings in MRI, such as HIZ and Modic changes, were not found in our cohort. Consistently, neither HIZ nor Modic changes were reported as well in a previous study in children with an average age of 6.6 years. 14 In contrast to this, a study that involved young adults (18-20 years) showed a prevalence of 3.2% and 0.7% for HIZ and Modic changes, respectively. 48 Another work with parallel demography displayed a prevalence of 1.5% and 1.4% for HIZ and Modic changes. 49 These findings implied that the HIZ and Modic changes might be age-dependent.
HIZ lesions were defined as a high-intensity signal located in the substance of the posterior annulus fibrosus in T2-weighted images, which is brighter than the nucleus pulposus. 50 It is reported that the incidence of HIZs was 3% to 61% in cases suffered from low back pain (LBP) and 2% to 3% in subjects without LBP. 51 Interestingly, the prevalence of HIZ lesions was highest at the 2 lowest lumbar levels, consistent with the phenomenon observed in LDD.9,49 These findings implied the HIZ may be related to the symptomatic lumbar disc degeneration diseases. Several works confirmed this hypothesis. Series studies revealed that the prevalence of HIZ is not only increasing with aging but also closely relating to disc degeneration and low back pain in adults.52,53
Modic changes are a series of degenerative changes involving the vertebral endplates and adjacent vertebral bodies. 11 Modic changes are frequently located adjacent to the degenerated disc and at the 2 lowest levels, 49 implying the potential link between Modic changes and disc degeneration. 54 However, whether the Modic changes have a relationship with LBP is questionable and deserves further research.
The cases investigated in our study were from a city in northwest of China, which had a population of 8.4 million by the end of 2009, with Han Chinese accounting for 99%. The urban residents accounted for 68.93% of the people, while the rural residents account for 31.07%. The annual per capita disposable income of urban residents and rural residents was 18,963 yuan and 6,275 yuan in 2009, respectively. Both were slightly above the national average of China (17,175 yuan for urban residents and 5,153 yuan for rural residents). Differences in population characteristics, socioeconomic backgrounds, and ethnic composition will affect the rates of seeking care for individuals. Some individuals in the current study consulted doctors with the complaint such as back pain, or limb numbness, or sciatica. It means that the study included not only healthy individuals but also individuals with lumbar spine disease. Therefore, the incidence of the imaging findings in the current work could not ideally represent the prevalence of lumbar disc changes in the general population.
There were limitations in our study. For one, this is a retrospective study of imaging morphologic data in children and adolescents. Although some efforts have been made to reduce the evaluating bias between observers in MR image analysis in our study, considering the difference in professional experience and understanding of the nomenclature version 2.0, we could not eliminate the evaluating bias between observers. The ideal study design should allow for MR scanning and image evaluations for a volunteer population representative of the whole child and adolescent population. Despite the retrospective studying hallmarks, the valuable imaging morphologic findings with relative large-scale observations provide the spinal community an important reference landscape on the lumbar spine of children and adolescents. The hallmarks of degenerative imaging phenotypes, including distribution along segments and presentive ages of SNs, and LDD, greatly expand our knowledge on the lumbar spine of the non-adult sub-population. Furthermore, the overview of the lumbar spine imaging hallmarks in children and adolescents was based on a special sub-population. Prospective large-scale studies are needed to address the issue.
Conclusions
It is rare to observe the incidental changes of the lumbar disc in children and adolescents. LDD can emerge as early as the first decade of life with SNs, without additional specific phenotypes, including Modic changes and high-intensity zones. The study provides valuable information of a unique age group that is often under-represented but equally important as adults. Any patient of this age who presents with low back pain, or limb numbness, or sciatica must be thoroughly investigated to avoid misdiagnosis.
Footnotes
Authors’ Note
Zhong-Yuan Wan, Jun Zhang, and Hua Shan contributed equally to this work. This work was reported during the session “Degenerative-Lumbar 2” as an oral presentation at the Global Spine Congress held in Toronto, May 15-18, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chinese National Natural Science Foundation Grants [grant number 81 270 028 and 81 572 182].