
Abstract
Study Design
Retrospective study.
Objectives
To investigate the impact of diabetes mellitus on neurological recovery and determine the relationship between moderate-severe diabetes and neurological recovery in patients with cervical spinal cord injury (CSCI) without bone injury.
Methods
A retrospective study was conducted on 389 consecutive patients aged ≥65 years with CSCI without bone injury across 33 medical institutes. The patients were divided into a nondiabetic group (n = 270) and a diabetic group (n = 119). Neurological outcomes were compared between the two groups through propensity score matching. The impact of moderate-severe diabetes (defined as hemoglobin A1c ≥ 7.0% or requiring insulin treatment) on neurological recovery was evaluated through multiple linear regression analysis.
Results
Propensity score matching revealed no significant differences between the diabetic and nondiabetic groups in terms of American Spinal Injury Association (ASIA) impairment scale grade and mean total ASIA motor scores (AMS) at 6 months post-injury. Multiple linear regression analysis indicated that age on admission (B = −0.34; 95% confidence interval [CI], −0.59 to −0.08; P = 0.01), dementia (B = −16.50; 95% CI, −24.99 to −8.01; P < 0.01), and baseline total AMS (B = −0.62; 95% CI, −0.72 to −0.51; P < 0.01) were negative predictors of neurological recovery at 6 months post-injury. The presence of moderate-severe diabetes did not influence neurological recovery at 6 months post-injury.
Conclusions
Diabetic patients with CSCI without bone injury achieved improvements in neurological function comparable to those of nondiabetic patients. Moderate-severe diabetes did not affect neurological recovery in patients with CSCI without bone injury.
Keywords
Introduction
Cervical spinal cord injury (CSCI) is one of the most devastating spinal injuries, and can cause severe permanent neurological deficits. A nationwide survey in Japan demonstrated that the overall rate of CSCI among cases of traumatic spinal cord injury (SCI) was 88.1%. 1 Among the CSCI cases, 70.7% did not suffer a bone injury resulting from minimal trauma, the older population. The incidence of CSCI without bone injury is anticipated to increase with the growing aging population.
Although several prognostic factors for neurological recovery in patients with CSCI without bone injury have been identified, most studies have focused on imaging features or surgical interventions. Preexisting conditions such as cervical spondylosis, ossification of the posterior longitudinal ligament (OPLL), and signal intensity (SI) changes in the spinal cord on magnetic resonance imaging (MRI) are relevant prognostic factors for neurological recovery in patients with CSCI without bone injury.2-4 Surgical intervention is also reported as a prognostic factor for neurological recovery in patients with CSCI without bone injury.5,6 Recently, Nakajima et al revealed that factors such as body mass index (BMI), OPLL, SI changes on MRI, American Spinal Injury Association (ASIA) impairment scale (AIS) on admission, comorbidity of dementia/delirium, and post-injury pneumonia were independent prognostic factors for the recovery of walking ability in patients with CSCI without major bone injury. 7
Diabetes mellitus is one of the most common comorbidities which is well known to negatively affect perioperative complications in spine surgery, including decreased spinal fusion rates and increased surgical site infections.8-10 Additionally, numerous studies have suggested that diabetes is a risk factor for poor surgical outcomes in patients with lumbar disc degenerative disease.11,12 Regarding cervical spondylotic myelopathy (CSM), some studies have reported preferable surgical outcomes in diabetic,13-15 while others diabetes contributes to poor surgical outcomes.16,17 However, the influence of diabetes on CSCI without bone injury also remains unclear because of the few studies. 7 Several animal studies supported that diabetes negatively affected neurological outcomes in patients with CSCI without bone injury.18,19 Furthermore, no previous studies have evaluated the relationship between diabetes severity and neurological recovery in patients with CSCI without bone injury.
This multicenter large-cohort study aimed to investigate the impact of diabetes on post-injury complications and neurological recovery, and the relationship between moderate-severe diabetes and neurological recovery in patients with CSCI without bone injury.
Materials and Methods
Participants
The multicenter study was conducted by the Japan Association of Spine Surgeons with Ambition and included 1512 consecutive patients aged ≥65 years with cervical spine/SCIs from 33 medical institutes between 2010 and 2020. The original dataset used in the study has also been utilized in other studies.7,20,21 Of the 1512 patients, 614 (40.6%) were diagnosed with CSCI without bone injury. This condition was defined as a CSCI with no evidence of spinal fractures or dislocations on radiography or computed tomography (CT).
22
Any patients with missing values in diabetes, baseline AIS grade, baseline ASIA motor score (AMS), AIS grade at 6 months after injury, or AMS at 6 months after injury were excluded from the study. Patients with baseline AIS grade A were also excluded because the probability of the AIS grade converting to grades C–E is very low.
23
A total of 389 patients followed up for at least 6 months were included in the present study (Figure 1). The 6-month time period was chosen based on previous clinical trials that demonstrated that neurological recovery after traumatic SCI mainly occurs within the first 6-9 months.24,25 Patients were divided into two groups: nondiabetic (n = 270) and diabetic group (n = 119). The diabetic group consisted of patients with hemoglobin A1c (HbA1c) ≥6.5%, those undergoing diabetes treatment with oral agents or insulin or both, or those previously diagnosed with diabetes by diabetologists by the clinical practice guidelines for diabetes.
5
National Glycohemoglobin Standardization Program method was used for measuring HbA1c. Patients with an HbA1c level ≥7.0% or those requiring insulin treatment were categorized into the moderate-severe diabetic group (n = 55).26,27 Flowchart of the multicenter cohort. ASIA, American Spinal Injury Association; AIS, American Spinal Injury Association impairment scale.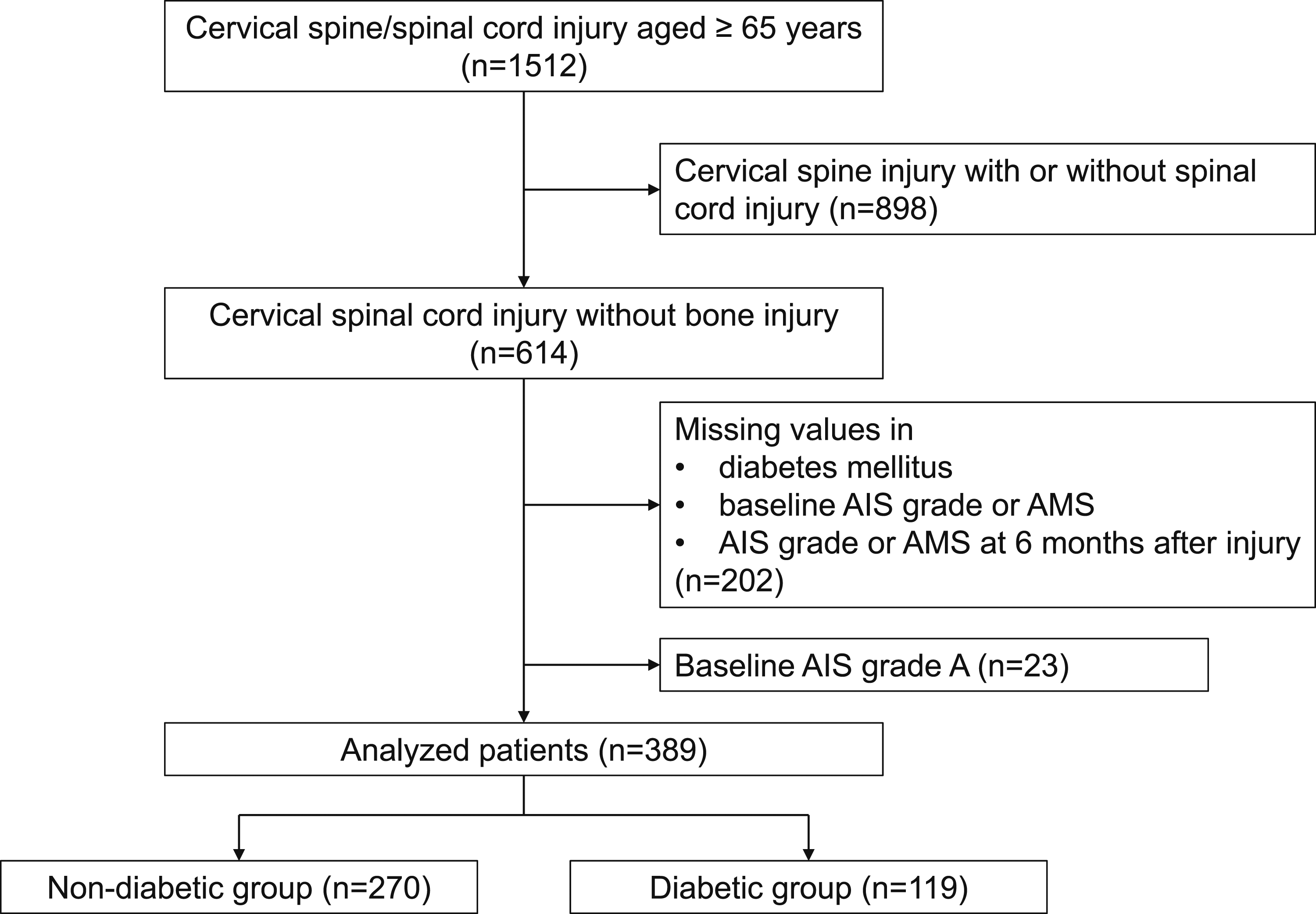
Data Collection
Demographic variables, including age at injury, sex, BMI, and medical comorbidities, were collected. Medical comorbidities included diabetes, hypertension, cardiovascular disease, cerebrovascular disease, rheumatoid arthritis, osteoporosis, respiratory disease, renal disease, Parkinson’s disease, dementia, and a history of surgery for musculoskeletal disorders. For diabetic patients, the HbA1c levels at admission and medication details, including insulin, were also documented. Cervical OPLL and diffuse idiopathic skeletal hyperostosis (DISH) were assessed by spinal radiography and CT. SI changes in the cervical spinal cord were evaluated using T2-weighted sagittal and axial MRI at the time of injury. Senior spinal surgeons and physical therapists at each center evaluated the neurological status on admission, at discharge, and 6 months post-injury using the AIS and AMS. The indications for surgery and steroid therapy were determined by the attending spinal surgeons at each institute. Complications during hospitalization, such as motor or sensory neurological deterioration, cerebral infarction, delirium, dysphagia, respiratory failure, pulmonary embolism, pneumonia, and renal infection, were also documented.
Statistical Analysis
The level of statistical significance was set at P < 0.05. The R Statistical Package version 2.6.0 (R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analyses. Continuous variables were analyzed using the unpaired t-test, Welch’s t-test, or Wilcoxon rank-sum test, as appropriate. Categorical variables were analyzed using the χ2 test or Fisher’s exact test. Propensity score matching was conducted to compare neurological outcomes between the nondiabetic and diabetic groups. A multivariate logistic regression model was used to calculate the propensity scores. The moderator variables were age, sex, BMI, cervical OPLL, cervical DISH, SI changes on MRI, medical comorbidities, baseline AIS grade, baseline AMS score, steroid therapy, and surgical intervention for CSCI. To adjust for baseline characteristics and comorbidities, 1-to-1 matching with fixed caliper widths (0.15) was performed without replacement. Each nondiabetic case was matched with a corresponding case in the diabetic group with the same propensity score. Standardized differences were used to measure covariate balance, with a standardized difference <10% indicating a negligible difference between both groups. Additionally, patients with an HbA1c level ≥7.0% or those requiring insulin treatment were classified as the moderate-severe diabetes group. Clinically relevant variables (age, sex, BMI, cervical DISH, SI changes on MRI, baseline AIS grade, baseline AMS, and surgical intervention), along with variables with significance level <0.05, as determined by univariate analysis (blood glucose level on admission, diabetes, rheumatoid arthritis, dementia, post-injury complication of dysphagia, cervical OPLL, and steroid therapy for CSCI), were included in the multiple linear regression analysis with listwise deletion of missing data. This was performed to assess the influence of moderate-severe diabetes on the degree of improvement in total AMS at 6 months post-injury.
Results
Comparison of Baseline Characteristics and Medical Comorbidities Between the Nondiabetic and Diabetic Groups
Comparison of Baseline Characteristics and Medical Comorbidities.
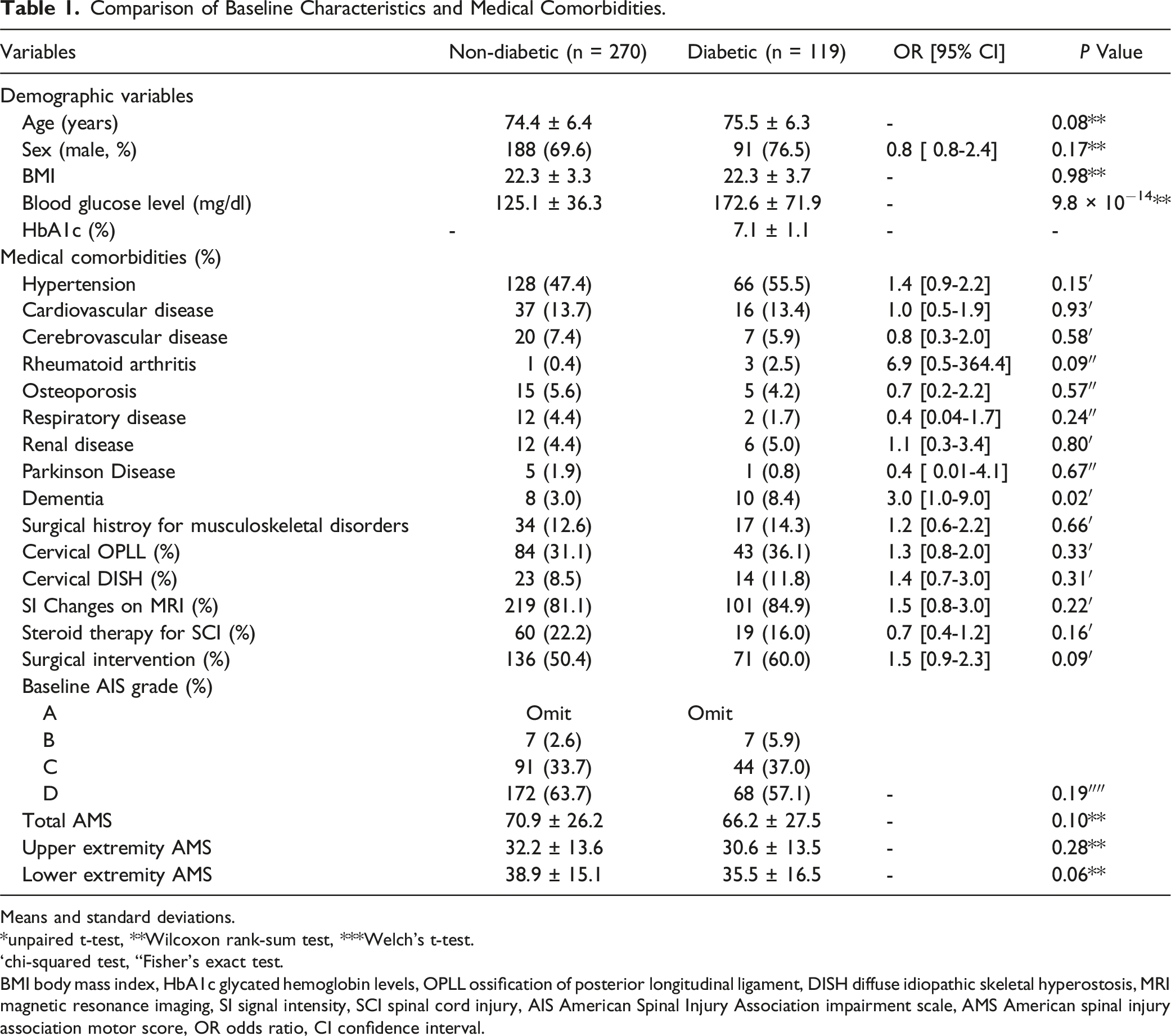
Means and standard deviations.
*unpaired t-test, **Wilcoxon rank-sum test, ***Welch’s t-test.
‘chi-squared test, “Fisher’s exact test.
BMI body mass index, HbA1c glycated hemoglobin levels, OPLL ossification of posterior longitudinal ligament, DISH diffuse idiopathic skeletal hyperostosis, MRI magnetic resonance imaging, SI signal intensity, SCI spinal cord injury, AIS American Spinal Injury Association impairment scale, AMS American spinal injury association motor score, OR odds ratio, CI confidence interval.
Comparison of Post-Injury Complications and Neurological Outcomes Between the Nondiabetic and Diabetic Groups
Comparison of Post-injury Complications and Neurological Outcomes.
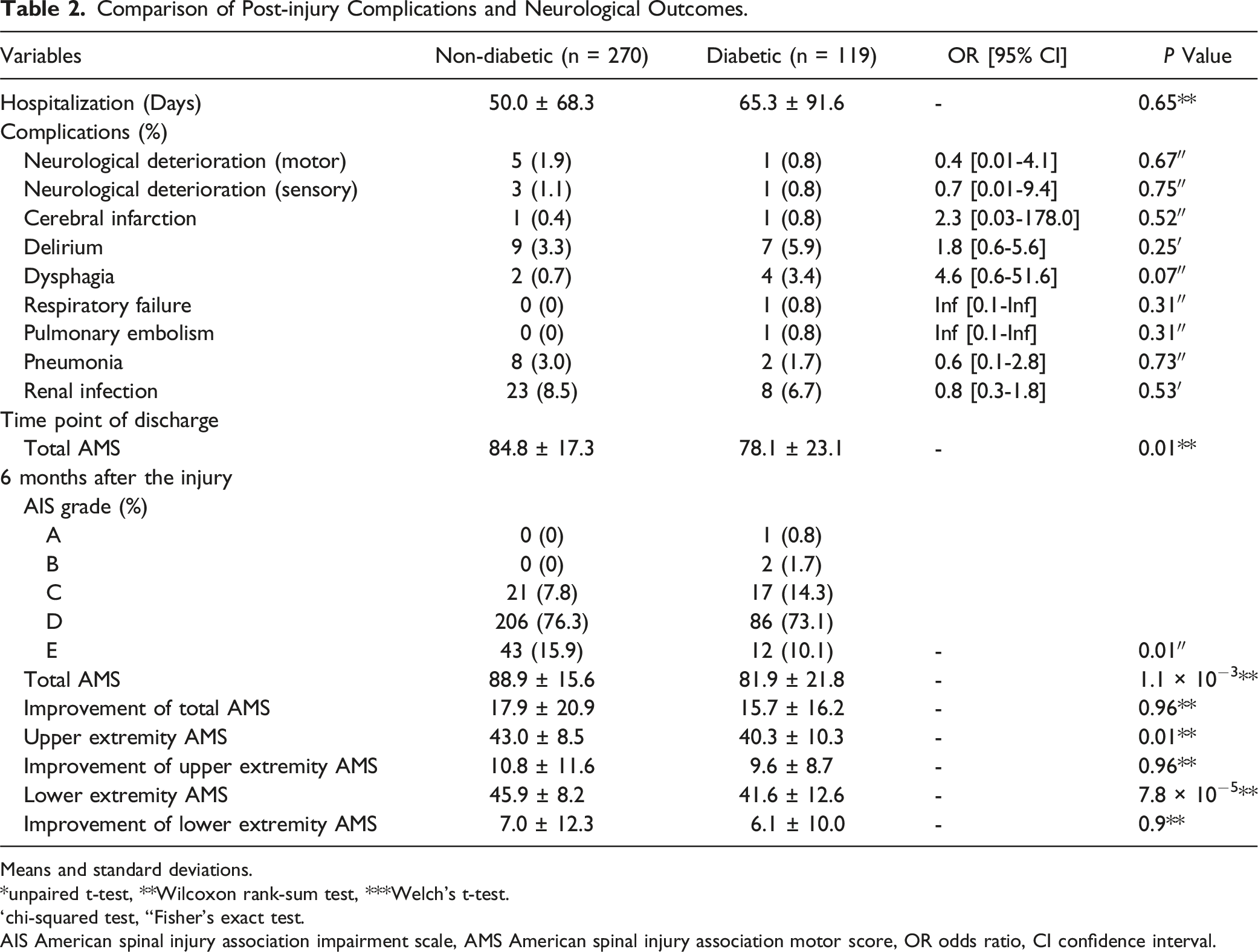
Means and standard deviations.
*unpaired t-test, **Wilcoxon rank-sum test, ***Welch’s t-test.
‘chi-squared test, “Fisher’s exact test.
AIS American spinal injury association impairment scale, AMS American spinal injury association motor score, OR odds ratio, CI confidence interval.
Propensity Score–Matched Comparison of Baseline Characteristics and Comorbidities Between the Nondiabetic and Diabetic Groups
Propensity Score-matched Comparison of Baseline Characteristics and Medical Comorbidities.
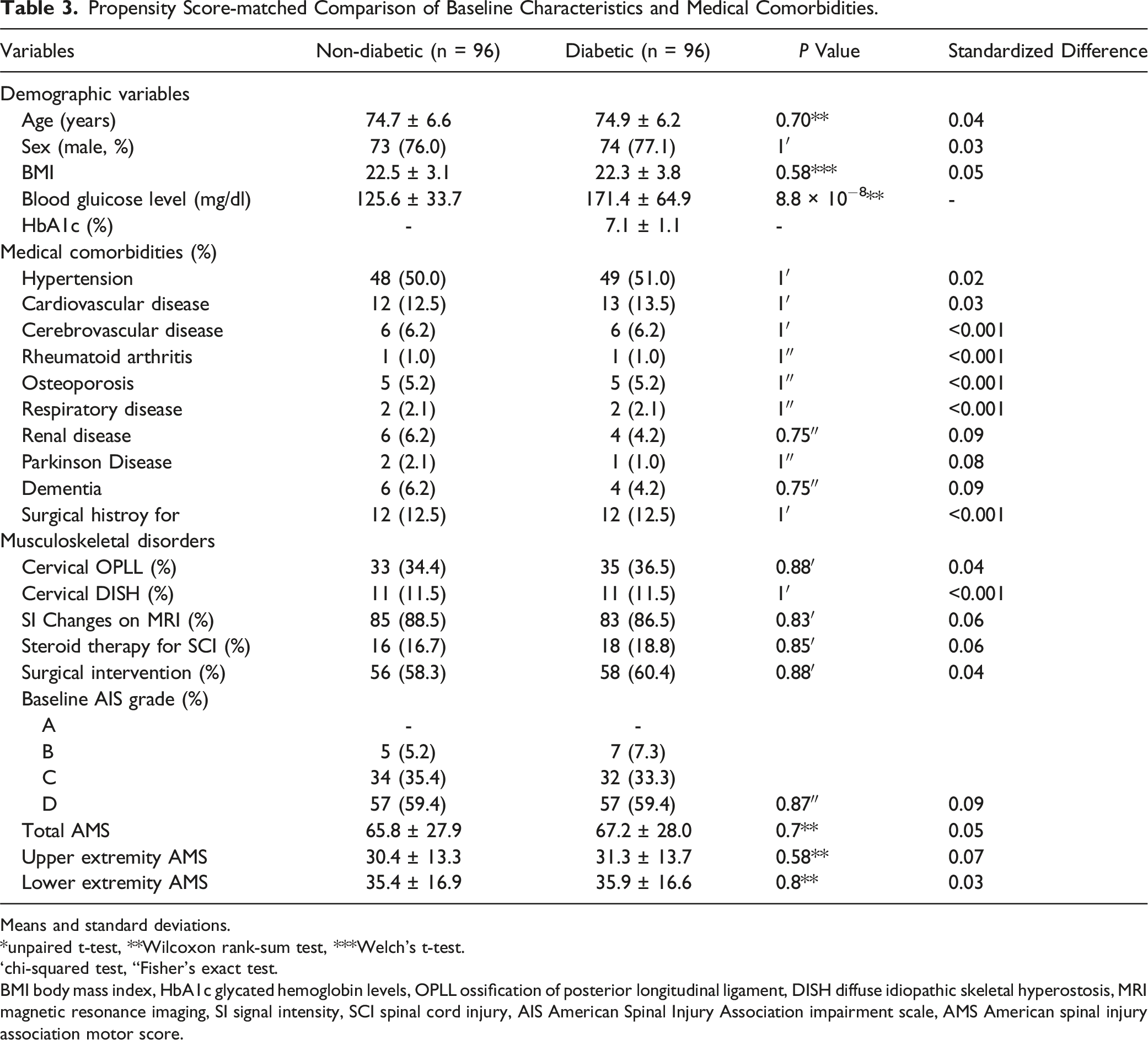
Means and standard deviations.
*unpaired t-test, **Wilcoxon rank-sum test, ***Welch’s t-test.
‘chi-squared test, “Fisher’s exact test.
BMI body mass index, HbA1c glycated hemoglobin levels, OPLL ossification of posterior longitudinal ligament, DISH diffuse idiopathic skeletal hyperostosis, MRI magnetic resonance imaging, SI signal intensity, SCI spinal cord injury, AIS American Spinal Injury Association impairment scale, AMS American spinal injury association motor score.
Propensity Score–Matched Comparison of Post-Injury Complications and Neurological Outcomes Between the Nondiabetic and Diabetic Groups
Propensity Score-matched Comparison of Post-injury Complications and Neurological Outcomes.
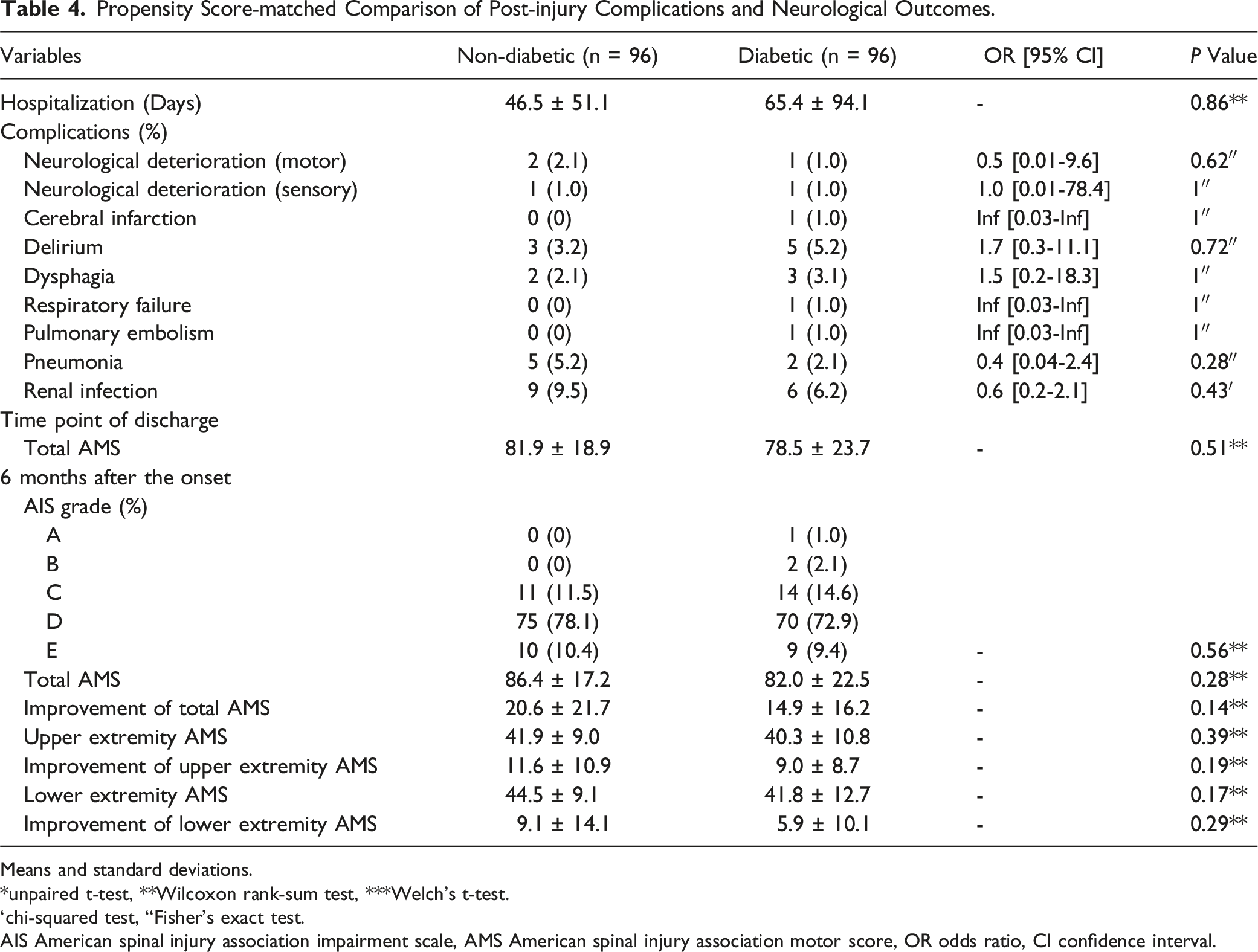
Means and standard deviations.
*unpaired t-test, **Wilcoxon rank-sum test, ***Welch’s t-test.
‘chi-squared test, “Fisher’s exact test.
AIS American spinal injury association impairment scale, AMS American spinal injury association motor score, OR odds ratio, CI confidence interval.
Comparison of Baseline Characteristics, Medical Comorbidities, and Post-Injury Complications Between Nondiabetic And Moderate-Severe Diabetic Groups
Comparison of Baseline Characteristics, Medical Comorbidities and Post-injury Complications Between Non-diabetic and Moderate-Severe Diabetic Groups.
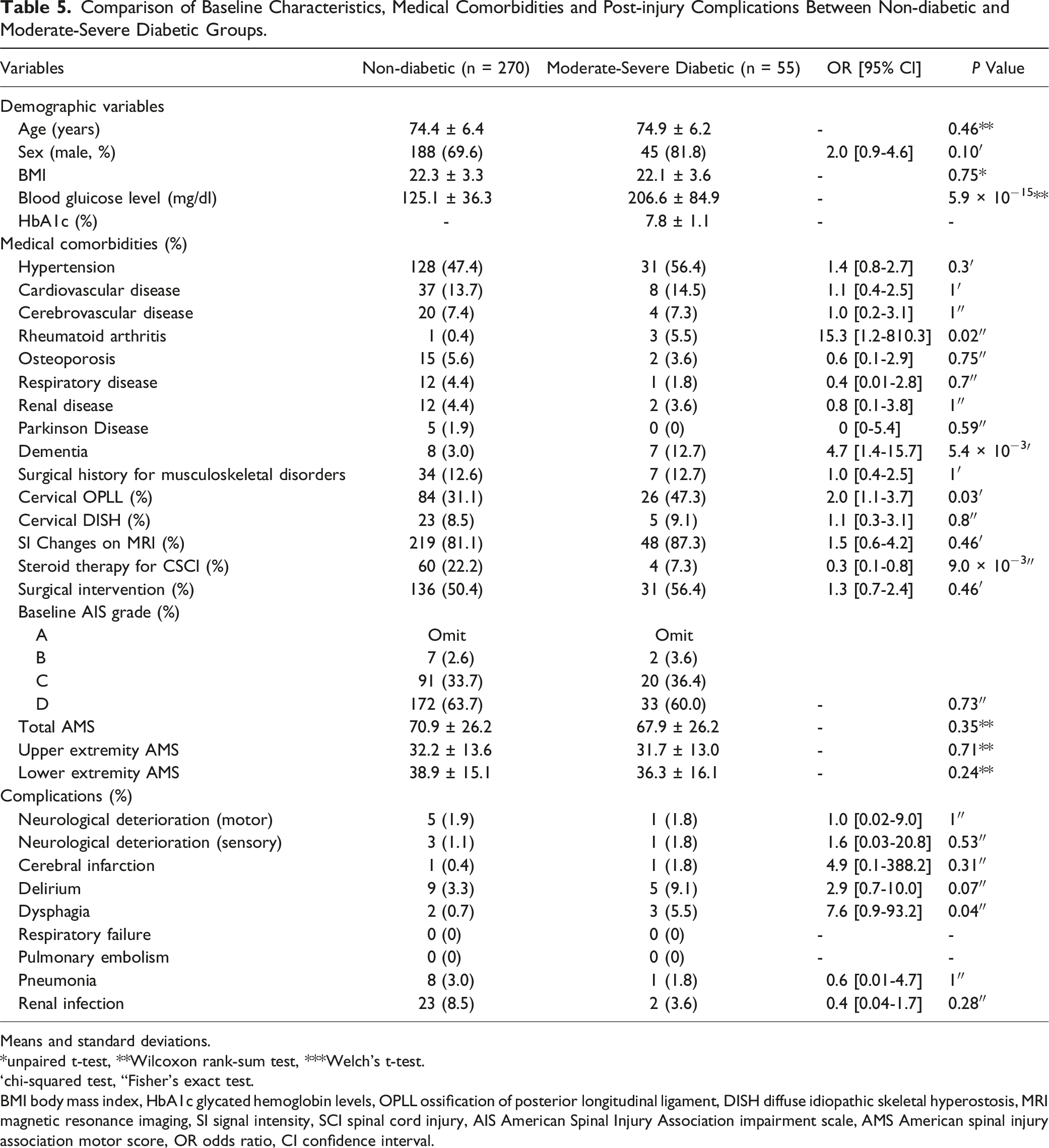
Means and standard deviations.
*unpaired t-test, **Wilcoxon rank-sum test, ***Welch’s t-test.
‘chi-squared test, “Fisher’s exact test.
BMI body mass index, HbA1c glycated hemoglobin levels, OPLL ossification of posterior longitudinal ligament, DISH diffuse idiopathic skeletal hyperostosis, MRI magnetic resonance imaging, SI signal intensity, SCI spinal cord injury, AIS American Spinal Injury Association impairment scale, AMS American spinal injury association motor score, OR odds ratio, CI confidence interval.
Influence of Moderate-Severe Diabetes on Neurological Recovery in CSCI Without Bone Injury
Multiple Linear Regression Analysis of the Degree of Improvement in Total AMS at 6 months After Injury.
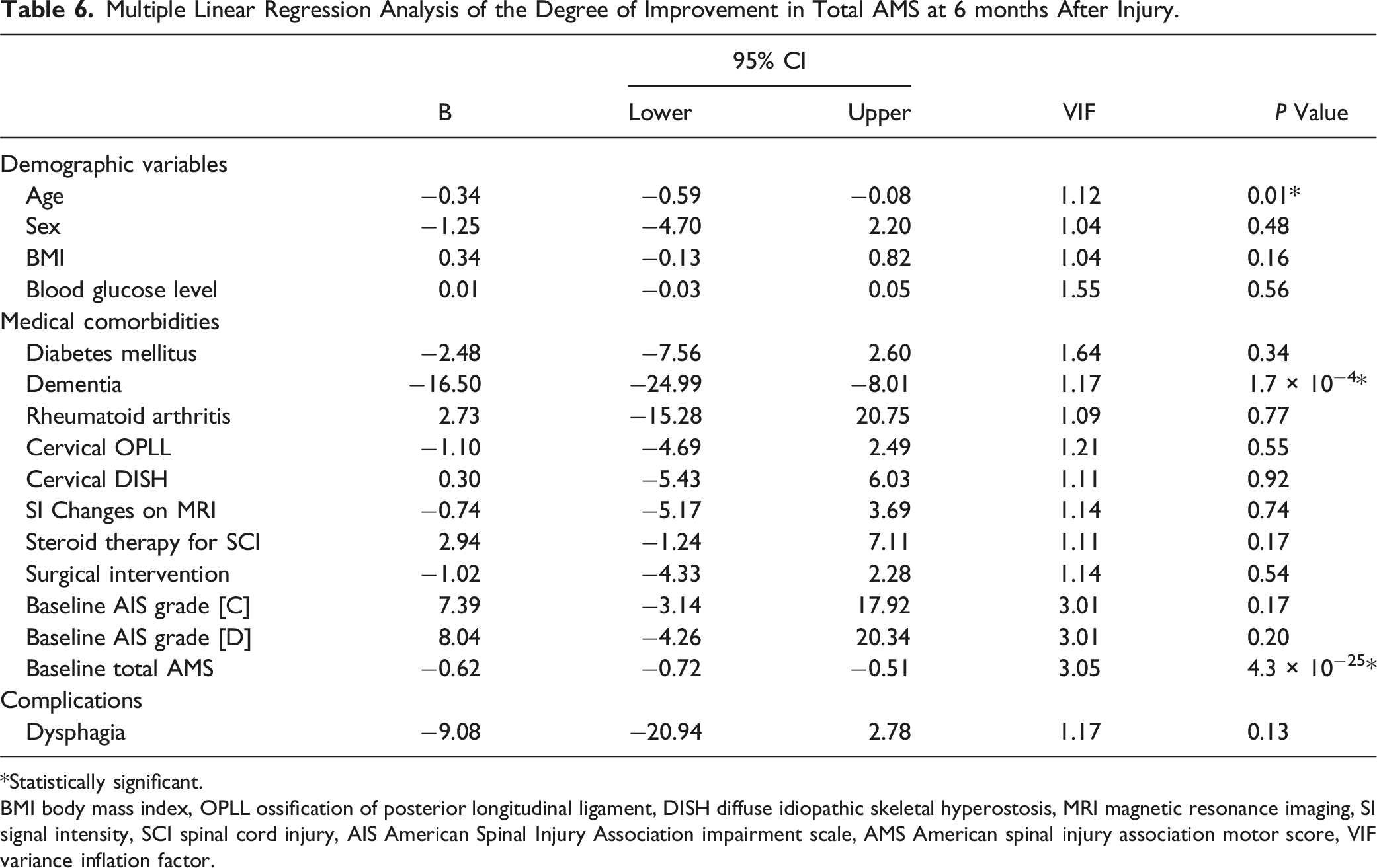
*Statistically significant.
BMI body mass index, OPLL ossification of posterior longitudinal ligament, DISH diffuse idiopathic skeletal hyperostosis, MRI magnetic resonance imaging, SI signal intensity, SCI spinal cord injury, AIS American Spinal Injury Association impairment scale, AMS American spinal injury association motor score, VIF variance inflation factor.
Discussion
To the best of our knowledge, this is the first multicenter large-cohort study using propensity score matching to demonstrate the influence of diabetes on neurological recovery in patients with CSCI without bone injury. Propensity score matching revealed no significant differences in the degree of improvement in AMS at 6 months post-injury between the nondiabetic and diabetic groups. Furthermore, multiple linear regression analysis indicated that moderate-severe diabetes did not affect the degree of improvement in AMS. The aforementioned findings provide valuable insights for decision-making regarding the medical treatment of patients with CSCI without bone injury.
Influence of Diabetes on Neurological Outcomes in CSCI Without Bone Injury
Previous reports have emphasized that diabetes leads to poor neurological outcomes following surgical intervention in patients with lumbar degenerative disc disease.11,12 However, the influence of diabetes on neurological recovery in patients with cervical spine disorders remains controversial. Kim et al reported that although diabetic patients with CSM could benefit from cervical laminoplasty, their rate of recovery was expected to be lower than those without diabetes. 28 Machino et al conducted a prospective cohort study of more than 500 patients with CSM and concluded that both diabetic and nondiabetic patients with CSM experienced similar benefits from cervical laminoplasty. 14 Dokai et al and Nori et al noted that CSM patients with diabetes experienced improvements in neurological function as a result of posterior decompression surgery to the same extent as those without diabetes.13,15 Although numerous studies have evaluated the influence of diabetes on neurological recovery in patients with CSM, few comparative studies have assessed this in patients with CSCI. Kobayakawa et al conducted a human cohort study of 206 patients with SCI, focusing on the relationship between blood glucose concentration on admission and functional outcomes, and supplemented by mouse model experiments. 18 They reported that hyperglycemia on admission exacerbated secondary injury, resulting in poor functional outcomes after SCI, regardless of whether the patient had diabetes. In the present study, a propensity score matching demonstrated that AIS grade, AMS, and degree of improvement in AMS were not significantly different between two groups. Several possible factors influence the effects of diabetes on neurological recovery in the studies. First, the previous study included patients with CSCI as well as those with thoracic and lumbar SCI. Second, the sample size of the previous study was relatively small. Third, the previous study mainly focused on nondiabetic patients with SCI and hyperglycemia on admission. The study was strictly limited to patients with CSCI without bone injury and utilized a multicenter large-cohort analysis. We evaluated the differences in neurological recovery between the nondiabetic and diabetic groups using propensity score matching, which can accurately match baseline characteristics, including neurological status, on admission.
Influence of Moderate-Severe Diabetes on Neurological Recovery
There has been only one study has investigated relationship between severity of diabetes and neurological recovery in patients with SCI. 18 The study reported that the HbA1c was negatively associated with AMS and recovery rate of AMS. 18 However, the severity of diabetes is defined by not only HbA1c but also by the requirement for insulin treatment. In line with previous studies, including the Clinical Practice Guideline for Diabetes, we classified patients with an HbA1c ≥ 7.0%, which is the treatment target for preventing diabetes-related complications, and those requiring insulin treatment as having moderate-severe diabetes.26,27 Multiple linear regression analysis revealed that age on admission, preexisting dementia, and baseline total AMS negatively influenced neurological recovery, whereas blood glucose level and moderate-severe diabetes did not impact neurological recovery. These results indicated that tight glycemic control by diabetologists during the acute phase of CSCI might lead to better neurological outcomes even in moderate-severe diabetic patients who not only had conservative treatment but also underwent the surgery. Several reports have suggested that early surgery for CSCI is beneficial, and we believe that clinicians should not consider the sufficient justification to deny the spine surgery for CSCI with diabetes alone.5,29 The present study did not evaluate the transition in blood glucose concentration during post-injury hospitalization. Further study is mandatory to reveal the impact of tight glycemic control during the acute phase of CSCI on neurological recovery in patients with CSCI. Age is widely recognized as a negative prognostic factor for neurological recovery in patients with SCI. 30 Jakob et al reported that elderly SCI patients have difficulties in translating an improvement of neurological deficit into function even after discharge from the rehabilitation center. 31 Clinicians should consider the personalized rehabilitation approaches which focus on training of daily living activities and ensure that patients are motivated to apply the skills they have acquired. A systematic review of cognitive function after SCI demonstrated a strong correlation between cognitive impairment and SCI and identified cognitive impairment as a predictor of poor social participation, including rehabilitation post-discharge.32,33 In patients with dementia, the quality of rehabilitation might decline, which could contribute to reduced neurological improvement. Systematic literature review based on prospective studies also revealed that diabetes mellitus is likely to increase the risk of cognitive impairment such as Alzheimer’s disease, which has frequently been attributed to cerebrovascular disease. 34 While diabetes can be managed with the tight glycemic control, interventions for dementia are often more challenging. Therefore, a multidisciplinary CSCI care approach should focus on preventing prolonged immobility and complications such as infections (pneumonia, renal infection and surgical site infection) that can exacerbate preexisting cognitive impairment. Nakajima et al reported similar findings, asserting that the AIS grade on admission and the presence of dementia/delirium were independent prognostic factors for walking recovery (for patients whose baseline AIS grades A-C converted to AIS grades D-E) among patients with CSCI without bone injury, using a comparable patient population from the same original dataset, 7 and they concluded that diabetes did not influence neurological recovery in patients with CSCI without bone injury. Conversely, Nori et al, utilizing a similar patient population from the same original dataset, applied multiple linear regression analysis, which revealed that diabetes adversely impacted postoperative changes in total AMS among patients with CSCI without bone injury who had undergone surgery. 20 The discrepancy in results between the studies may be attributable to different patient selection criteria. Specifically, the present study and that of Nakajima et al included patients with CSCI without bone injury who underwent both surgery and conservative treatment, whereas the study of Nori et al focused solely on those who underwent surgery. The findings suggest that patients with CSCI without bone injury who have undergone surgery are more likely to develop moderate-severe diabetes.
Limitations and Strength
The primary limitation of this study is its retrospective nature; thus, the study has some missing values. The present study had the retrospective nature and the analyses were conducted using a heterogeneous cohort without a control group, which was not a comprehensive survey. Since the clinical data were collected from 33 high-volume trauma centers, it was difficult to obtain the completely accurate medical records. The present study excluded patients with missing values in diabetes, baseline AIS grade, baseline AMS, AIS grade at 6 months after injury, or AMS at 6 months after injury, which can cause the selection bias. The present study excluded the patients with baseline AIS grade A as well even though that could cause selection bias. The previous study demonstrated the probability of the AIS grade converting to grades C–E is very low in SCI patients with AIS grade A. 23 We excluded 23 CSCI patients without bone injury who were classified into AIS grade A on admission, and 83% of them were AIS grade A or B at final follow-up. This result was comparable with the previous study and indicated that it was difficult to evaluate the neurological recovery especially motor function. Furthermore, it was difficult to completely compare treatment outcomes due to the biases that the surgical indications and procedures, and rehabilitation approaches differed across the facilities and there was no standardized treatment approach. Additionally, the survey was conducted in Japan, which has the unique background of being the most advanced aging society in the world. However, as the pace of population aging has been accelerating drastically worldwide, the results of the present study might be generalized beyond the specific population. Regarding the missing values, smoking and drinking histories, which could potentially influence the neurological outcomes, were excluded from the analysis due to the high proportion of missing data. Although the proportion of missing values in other demographic variables that evaluated in the present study were all less than 5% and pairwise deletion was used in each statistical analysis, that could potentially cause the bias. Preexisting conditions such as CSM and SI changes in the spinal cord on MRI have not evaluated because of the retrospective nature of the present study. Evaluation of cervical and global spinal alignments, which might have potentially impact on the neurological outcomes, was not performed. Follow-up period was relatively short at 6 months post-injury to evaluate cases that show delayed recovery following CSCI. It is common for CSCI patients to be transferred to the rehabilitation hospitals immediately after acute-phase treatment in Japan, resulting in a high proportion of missing AMS at 12 months post-injury (approximately 30%), which also had to be excluded from the analysis. Neurological outcomes at 6-month post-injury were chosen, since the previous clinical trials demonstrated that neurological recovery after traumatic SCI mainly occurs within the first 6-9 months.24,25 Further studies are mandatory to determine the influence of diabetes on long-term neurological recovery in patients with CSCI without bone injury. The transition in blood glucose concentration during post-injury hospitalization was not observed in the present study. Kobayakawa et al reported that controlling the blood glucose concentration during the acute phase of SCI could prevent exacerbation of the pathophysiology and improve motor function in hyperglycemic mice post-SCI. 18 Tight glycemic control by diabetologists during the acute phase of CSCI might lead to better neurological outcomes in diabetic patients with CSCI without bone injury in the present study. Despite these limitations, this is the first multicenter large-cohort study to demonstrate the influence of diabetes on neurological recovery in patients with CSCI without bone injury.
Conclusion
We investigated the influence of diabetes, particularly moderate-severe diabetes, on neurological recovery in patients with CSCI without bone injury. Diabetic patients with CSCI without bone injury experienced improvements in neurological function comparable to those of nondiabetic patients. Furthermore, moderate-severe diabetes did not affect neurological recovery.
Footnotes
Acknowledgments
The authors acknowledge the contributions of the members of the 33 participating institutions in the assistance with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.