
Abstract
Study Design
Literature review.
Objectives
To provide an overview of the complications associated with and management strategies for adult patients with osteoporosis requiring spinal reconstructive surgery. Emphasis will be placed on screening, diagnosis, and perioperative medical and surgical management of these patients.
Methods
A review of the literature was performed for studies examining osteoporosis in adult patients undergoing spine surgery, associated complications, treatment and prevention methodologies.
Results
The reported incidence of osteoporosis in adult patients undergoing spinal reconstructive surgery was found to be 10% - 50%, whereas the incidence of osteopenia was 41.4% – 58.6%. DEXA scan is the most widely used modality for assessing bone mineral density (BMD) despite its limitations. Quantitative CT has been found to be the most optimal method for measuring BMD in the spine, yet, its availability is limited. Opportunistic CT scan-based Hounsfield Units (CTHU) have been found to correlate with osteoporosis and osteopenia, instrumentation loosening, proximal and distal junctional kyphosis, and pseudarthrosis. Patients treated with Teriparatide preoperatively and postoperatively were found to have a decreased rate of pseudarthrosis, screw loosening, and reoperation. Modifying surgical techniques can also improve outcomes. Such strategies could involve vertebral cement augmentation, iliac fixation in long constructs to the sacrum, and utilizing longer constructs when addressing spinal deformity or spinal instability.
Conclusions
The incidence of osteoporosis in patients undergoing spinal reconstruction is high. Appropriate preoperative and postoperative medical treatment can result in lower rates of adverse events related to osteoporosis. Surgical treatment and fixation can also be modified to account for suboptimal bone health.
Introduction
Multilevel spinal reconstructive surgery including instrumentation and fusion is often performed for surgical treatment of various spinal conditions including traumatic injuries, neoplasms, degenerative spinal conditions, and spinal deformity in an adult patient.1,2 The incidence of osteoporosis is high in the adult patients undergoing spinal reconstructive surgery (APUSRS).3,4 The incidence of unrecognized osteoporosis in this patient population is also high; up to 64% of patients being unaware of their osteoporosis diagnosis prior to spine surgery. 4 However, poor bone health can lead to severe complications for adult patients undergoing spinal reconstructive surgery.5-14
With recent evidence suggesting the benefits of osteoporosis treatment prior to surgery, it is essential for spine surgeons to understand how to screen for, diagnose, and treat osteoporosis prior to surgery.15,16
A review of the literature was performed for studies examining the incidence of osteoporosis in adult patients undergoing spine surgery, associated complications, treatment and prevention methodologies, as well as the awareness of this condition amongst spine surgeons. We discuss screening guidelines, diagnostic modalities, perioperative medical treatment, and surgical treatment strategies to decrease the risk of complications associated with osteoporosis in adult patients undergoing spinal reconstructive surgery.
Prevalence of Osteopenia/Osteoporosis in Adult Patients Undergoing Spinal Reconstructive Surgery
The prevalence of osteoporosis and osteopenia in a cohort of adult patients older than 50 undergoing spinal surgery was reported to be up to 60.6% in males and 92.7% in females. 17 Out of this cohort of 759 patients, 68% had a Dual-energy X-ray absorptiometry (DEXA) scan. Male patients had a 46.1% prevalence of osteopenia and 14.5% osteoporosis, whereas, females patients had a 41.4% prevalence of osteopenia and 51.3% osteoporosis based on the World Health Organization (WHO) criteria for osteoporosis. 17 Therefore, 60.6% of males and 92.7% of females over 50 undergoing spinal surgery had an abnormal bone mineral density (BMD) thus suggesting that patients over the age of 50 should have evaluation for osteopenia/osteoporosis prior to spine surgery.
In another cohort of 140 adult patients undergoing spinal fusion who had a DEXA scan within a year of their surgery, a 58.6% prevalence of osteopenia and 10% prevalence of osteoporosis was reported. 5
A recent systematic review of literature including 10 studies of patients over the age of 50 undergoing spinal surgery found the prevalence of osteoporosis to be 34.2%, whereas, the prevalence of osteopenia was 43.5%. 18 Therefore, up to 78.7% of patients undergoing spinal surgery had either osteopenia or osteoporosis. 18 The prevalence of osteoporosis increased significantly over the age of 60 in females. 18 A retrospective review of 124 candidates for spine surgery over the age of 50 found that the prevalence of osteoporosis was 45% in females and 20% in men and there was no significant difference in their T-scores. 19 These studies support screening for both male and female patients as opposed to disproportionately directing towards female patients only. 20
Attitudes towards Screening for Osteoporosis and Guidelines for Osteoporosis Screening in Adult Patients Undergoing Spinal Reconstructive Surgery
Complications related to poor bone health could potentially be decreased by preoperatively identifying osteoporosis or osteopenia and subsequently optimizing a patient’s bone health prior to surgery. Unfortunately, up to 64% of patients with osteoporosis have been found to be undiagnosed prior to spine surgery. 4 Several surveys of spine surgeons have been conducted in the past to understand their attitudes towards screening, diagnosing, and treating osteoporosis prior to spine surgery.21-23 The AO Spine Latin America conducted a survey of 349 spine surgeons and found that preoperative screening for osteoporosis was only performed by 19% of surgeons, however, this increased to 75% if the patient was thought to have a risk factor for osteoporosis. 21 The Spanish Neurosurgery Society’s (SENEC) survey of 77 memebrs showed that 32.5% of members do not consider formal evaluation of bone health even in patients with suspected Osteoporosis prior to spinal fusion and 37.7% do not consider medical treatment prior to surgery even in patients they suspect of having osteoporosis. 22 Another survey of 93 surgeons who attended a spine conference in Canada in 2007 reported that only 44% of participants obtained DEXA scans prior to instrumented spinal fusion and only 22% felt the need to obtain DEXA scan prior to un-instrumented spinal fusion. 23 They did not note a difference amongst practices between Neurosurgeons and Orthopedic surgeons and those in academic practice vs those in private practice. Additionally, only 19% reported routinely obtaining a DEXA scan as part of pseudarthrosis workup. 23 Even in patients being treated for a vertebral compression fracture, only 60% routinely obtained a DEXA scan. 23
In a study focused on assessing risk factors for acute fractures at the top of a long segmental fusion, only 39% of all patients were found to have BMD data available and only 54% of those with a fracture had BMD data. 13 These studies indicate that poor bone health is frequently underdiagnosed and emphasizes the need for better preoperative screening.
The 2019 International Society for Clinical Densitometry (ISCD) Official Positions on Use of Bone Health Evaluation in Orthopedic Surgery concluded that all adult patients undergoing elective orthopedic or spine surgery should undergo a bone health evaluation. 24
The ISCD and the National Osteoporosis Foundation (NOF) suggest that BMD testing should be performed in men over the age of 70 and women over the age of 65. 24 For those younger than the suggested age, BMD testing is required if they have certain risk factors for development of osteoporosis. The ISCD 2019 position agreed on the following risk factors: diabetes mellitus, inflammatory arthritis, chronic corticosteroids (5 mg per day for 3 or more months of treatment), a low-trauma fracture after 50 years of age, limited mobility, smoking, and chronic kidney disease stage 3, 4, and 5. 24
The Fracture Risk Assessment Tool (FRAX) can be used to estimate a patient’s 10-year probability of a hip or major osteoporotic fracture including the spine. 25 FRAX includes the following risk factors for elevated fracture probability: age, fracture after the age of 50, parental history of hip fracture, current smoking, chronic corticosteroids, rheumatoid arthritis, and alcohol use >3 units per day.25,26 Finally, the NOF criteria too includes adults with a history of fracture after age 50. 27
Recently, through a Delphi method involving spine surgeons and bone health specialists, a set of guidelines was published for the assessment and treatment of patients with osteoporosis undergoing spine surgery. 28 They recommended BMD testing for all patients over the age of 65 prior to spinal reconstructive surgery and for those above age 50 with one of the aforementioned risk factors.
Diagnostic Modalities for Assessment of Bone Health
Patients in need of formal assessment of bone health are usually referred for a DEXA scan which is considered the current gold standard for bone health evaluation (Figure 1).29,30 DEXA scans are widely used to diagnose and guide medical treatment of osteoporosis.
30
The ISCD 2019 official position recommends that hip and spine DEXA scan should be obtained in these cases.
24
Example of a DEXA of the hip and lumbar spine.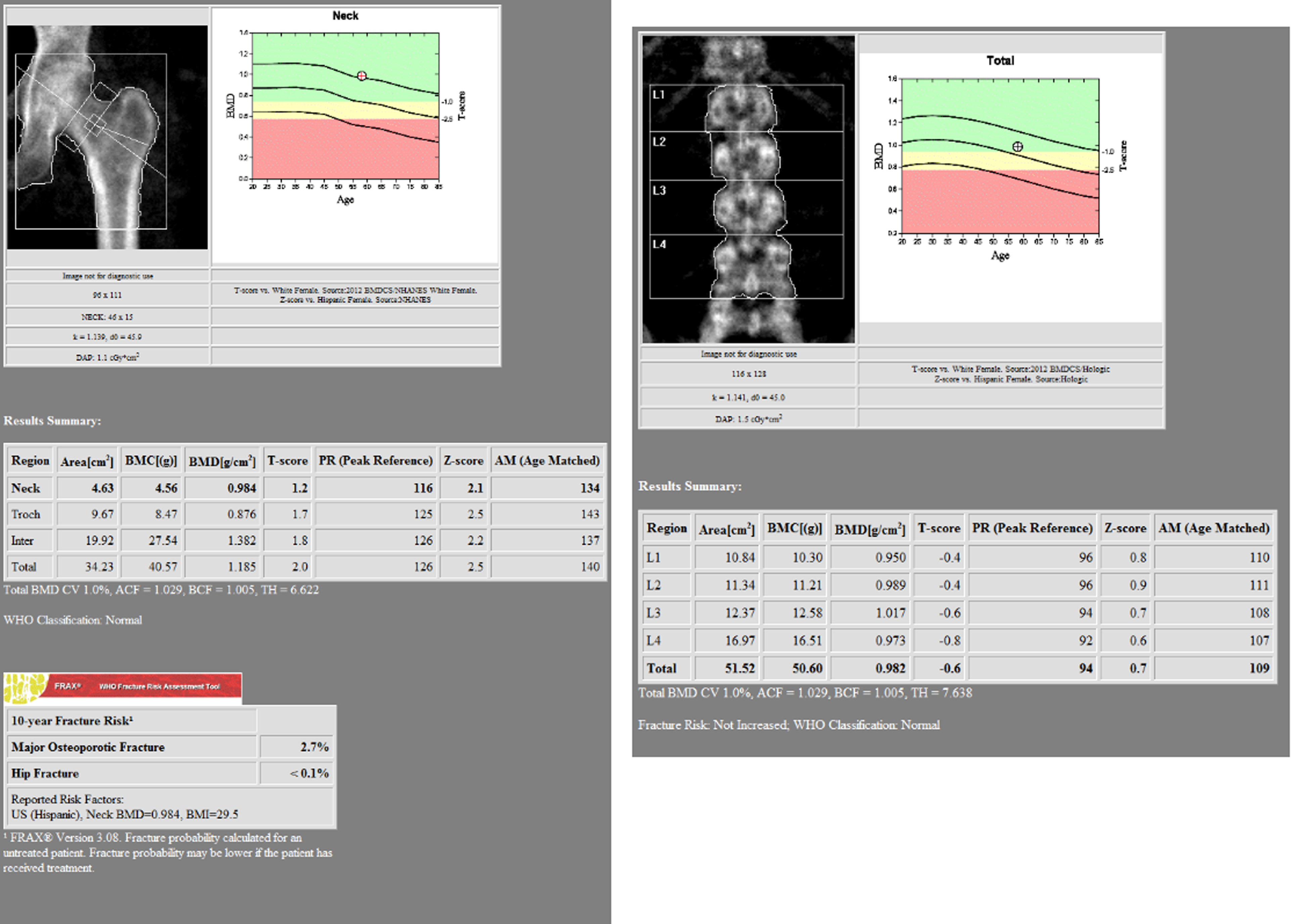
The DEXA scan of the spine can have several limitations.30,31 BMD of the spine measured by DEXA can be inaccurate in patients with scoliosis due to overlap of vertebral segments.30,31 The presence of significant osteophytes can spuriously elevate the measured BMD in the spine.30,31 BMD of the spine is difficult to measure in the presence of spinal fusion or spinal instrumentation. Therefore, a hip DEXA is usually recommended in addition to a spine DEXA. However, in the presence of hip implants and unreliable spine BMD from DEXA, opportunistic assessment by CT or QCT can be a better alternative. 30
Measurement of CT based Hounsfield units (CTHU) was described in 2011 as an opportunistic method of assessing bone health.
32
CT scans are often routinely performed prior to spinal instrumentation procedure, therefore, the use of this opportunistic method of bone health assessment has gained popularity. This involves measuring CTHUs on 3 different axial slices through a vertebral body (superior, middle, inferior) and using their mean (Figure 2). CTHU measurement is typically performed at lumbar segments L1-4 and has been found to correlate with DEXA scan-based BMD in multiple studies.4,7,14,32-38 CTHU has also been shown to have high sensitivity (0.73) and positive predictive value (0.85) in diagnosing osteoporosis when compared to DEXA scans.
32
Therefore, opportunistic CT-based attenuation using HUs can be used to estimate the likelihood of osteoporosis with the parameter of L1 CTHU <100 as abnormal and L1 CTHU >150 as normal to support decisions regarding bone health assessment.
24
Demonstration of measuring Hounsfield Units on CT scan. A: Mid sagittal cut of a Lumbar CT with the green lines in L3 showing the Axial cuts; B: Axial cut just below the superior end plate. C: Axial cut in the middle of the body. D: Axial cut just above the superior end plate.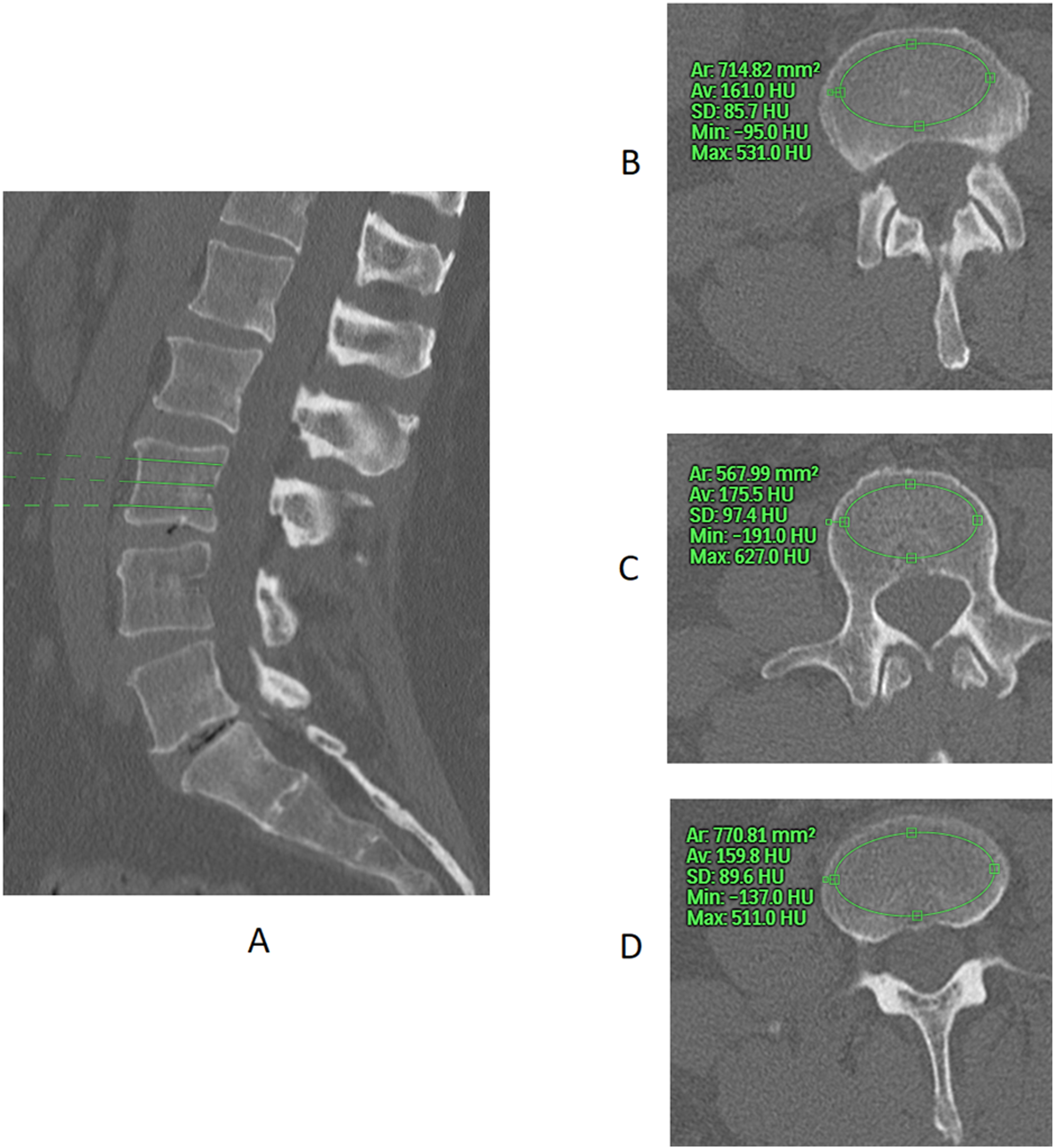
Wagner et al. 4 demonstrated the efficacy of opportunistic CTHU by finding that 49.2% of all patients older than age 50 undergoing TLIF had evidence of decreased BMD on CTHU, with 19.5% consistent with osteoporosis and 29.7% consistent with osteopenia. Only 36% of the patients with osteopenia and osteoporosis on CTHU had DEXA scans and only 23.7% of the osteopenic group had been prescribed medications to improve BMD. 4 Several studies also identified that lower CTHU values in the lumbar spine were associated with vertebral fracture and adjacent segment fractures.7,34 Schreiber et al found that patients with a successful fusion had significantly higher CTHU values of 203.3 vs 139.8 for those with pseudarthrosis. 14 Other studies have found an association between cage subsidence and low CTHUs.39,40 Meredith reported that patients who developed adjacent segment fracture after undergoing spinal fusion had a lower CTHU value compared to those without a fracture (145.6 vs 199.4). 7 Overall, these studies suggest the utility of using CTHU on opportunistic CTs when a formal DEXA is not available.
Quantitative computed tomography (QCT) is another imaging modality used to assess BMD. QCT offers a volumetric analysis of trabecular bone mineral density which has been shown to be more precise when compared to DEXA scan. A QCT measurement of BMD <90 mg/mL is shown to have an increased risk of pedicle screw loosening as opposed to >120 mg/mL. 41 However, its limited availability, higher cost, and increased radiation prevent QCT from being used as a standardized screening and diagnostic tool.
Another opportunistic method of assessing bone health of the spine is the Biomechanical Computed Tomography analysis (BCT).42-48 BCT performs a measure of the vertebral body strength using finite element analysis (FEA) and also measures the vertebral trabecular BMD.46,47 BCT has been reported to predict the risk of vertebral body fracture independent of the BMD. 46 In a recent retrospective observational cohort, patients who tested positive for osteoporosis using BCT were found to have a 5 times higher risk of vertebral fractures after undergoing spinal fusion and had an up to 4 times risk of reoperation. 47
Due to the wide availability of DEXA scans, the guidelines published in 2022 recommend Hip and Spine DEXA scan for diagnosing osteoporosis along with a vertebral fracture assessment. 28 They recommend using the Z score for patients aged 20 to 50 and T score for patients older than 50. 28 Finally, they recommend using CTHU for opportunistic screening if a DEXA is not available. 28
Adverse Events Related to Osteoporosis
Osteoporosis is linked to several complications in APUSRS such as vertebral fractures (Figure 4), instrumentation failure, pseudarthrosis, proximal or distal junctional kyphosis (PJK/DJK), and unplanned reoperation (Figure 3).5-14 Patients with osteoporosis and osteopenia are at a 2 times higher risk for pseudarthrosis and 3 or more times higher risk for revision surgery compared to those with normal bone density likely due to deficient or inadequate mechanical support from the instrumentation.5,10-12 Osteopenia, however, has not been found to be a risk factor for pseudarthrosis.
5
CT scan of a patient with osteoporosis with sacral fracture and bilateral S1 screw loosening after instrumentation from L4-S1. X-rays (A) and CT scan (B) of a patient with multiple osteoporosis related fractures at L1, L2, L4. Retropulsed fragment into the canal can be seen at L1 causing severe stenosis.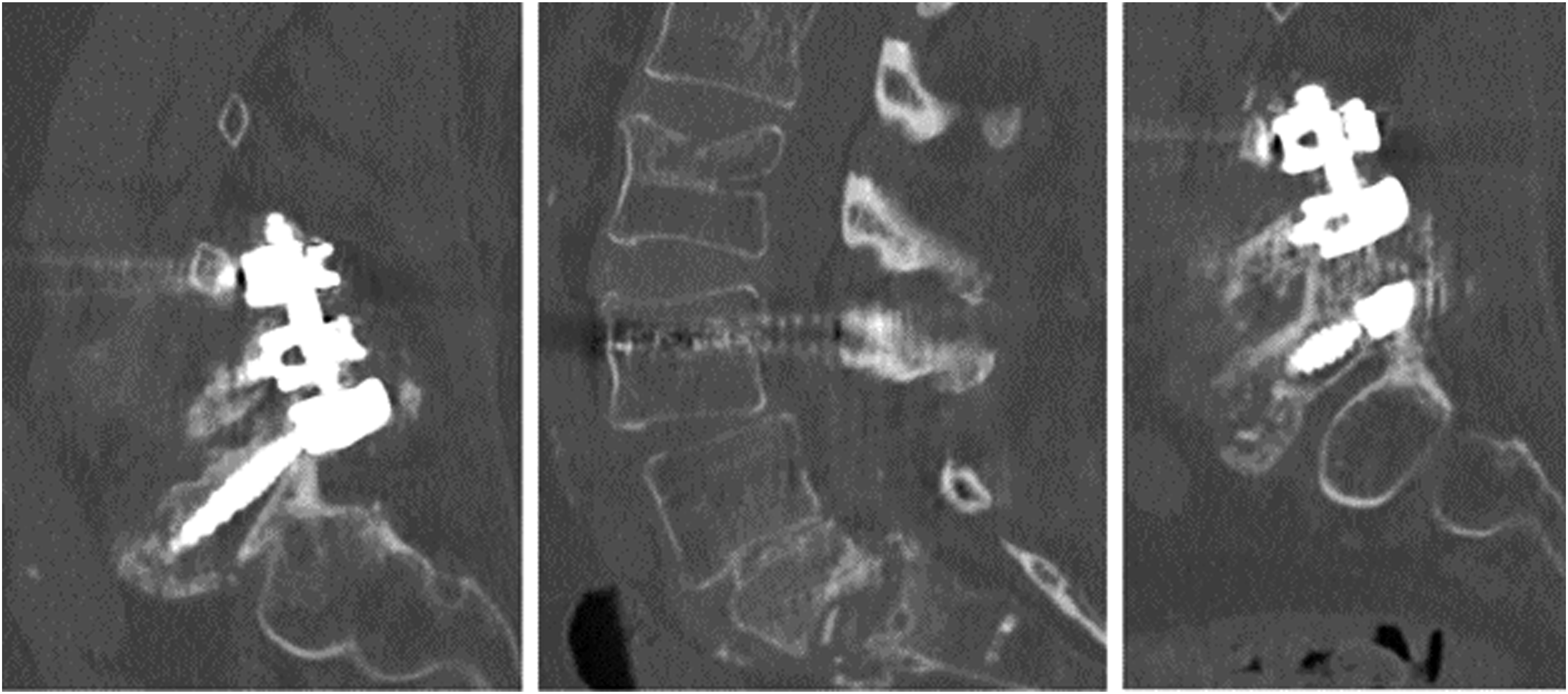

Low BMD is considered a risk factor for the development of PJK (Figure 5).8,9,49,50 Patients with osteoporosis are estimated to have up to 2-times the risk of PJK compared to patients with normal BMD.8,9 The average T score was found to be significantly lower in patients with fracture at the top of the construct as opposed to those without a fracture (−1.73 vs −0.58) in patients who had undergone surgery for adult spinal deformity.
13
Osteoporosis and low bone mineral density (BMD) are more likely to occur in older patients, and as such have been a commonly reported risk factor for the development of PJK.51-53 However, PJK is related to multiple factors, therefore, a few other studies failed to identify osteoporosis as an independent risk factor for PJK.9,51,54 A patient with compression fracture at the Upper Instrumented Segment leading to Proximal Junctional Kyphosis.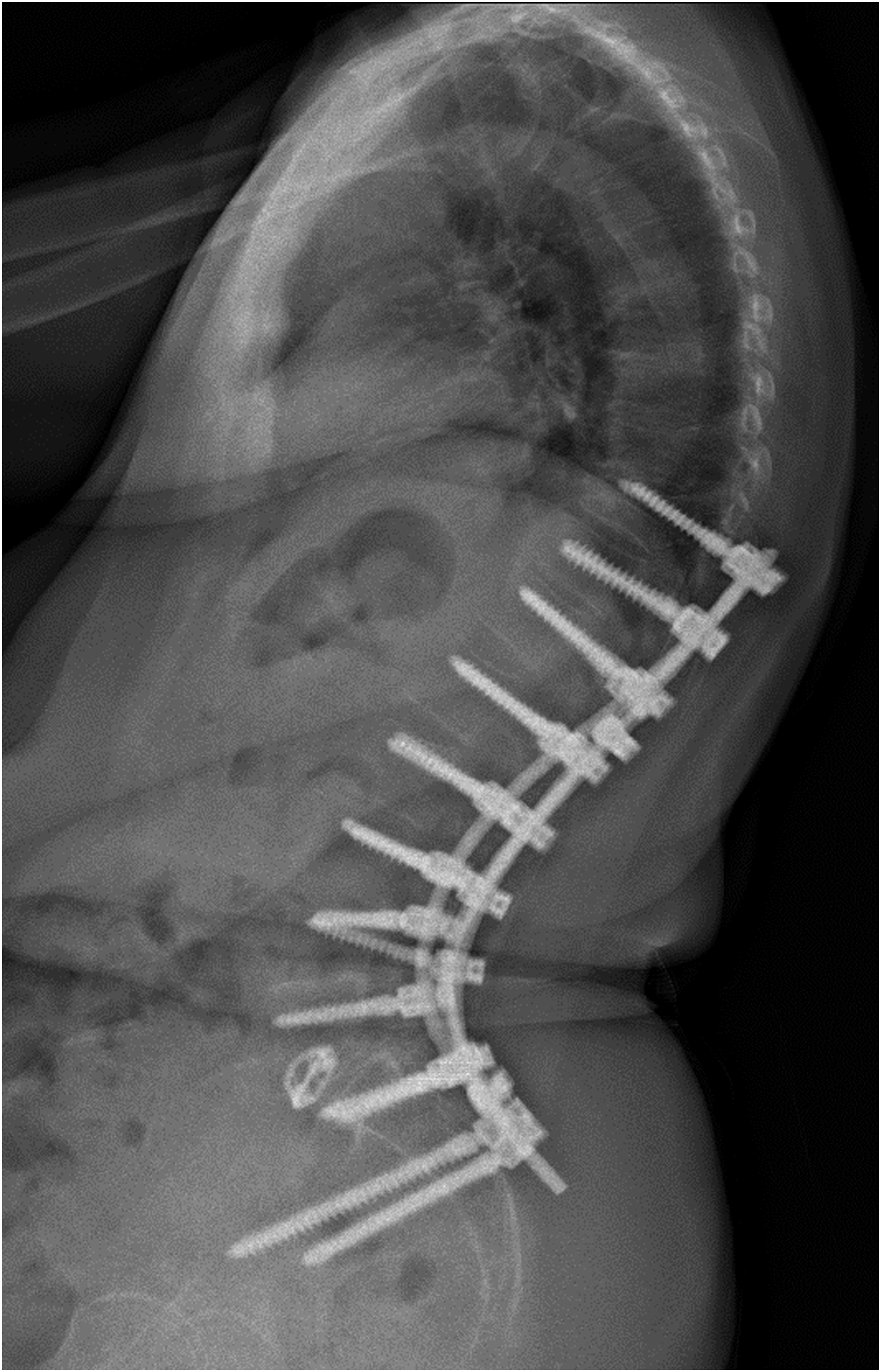
Medical Treatment of Osteoporosis Prior to Surgery
Osteoporosis remains underdiagnosed and undertreated prior to spine surgery.12,19,55 Patients should be appropriate screened for osteoporosis prior to spine surgery and should receive medical treatment for the osteoporosis prior to spine surgery. 24 This treatment is often guided by a bone health specialist such as an endocrinologist or rheumatologist. 24 A review of 849 patients with osteoporosis undergoing spinal fusion found that only 14.3% of patients received medical treatment for osteoporosis prior to surgery and 43% of those patients had ongoing prescriptions for medical management of osteoporosis at 1 year after surgery. 55 Another study reported that only 27% of patients with a diagnosis of osteoporosis and 10% of patients with osteopenia were using medications for treatment of bone health. 12 Amongst the few on medications, bisphosphonates were the most commonly utilized medications accounting for 95%–98.8%. 12
Some facilities have developed a service to formally evaluate patients for osteoporosis prior to spine surgery. 19 In a review of 124 patients above age 50 who were candidates for joint arthroplasty or spine surgery, 91% were found to meet the national osteoporosis foundation (NOF) criteria for requiring medical treatment for osteoporosis. 19 On the other hand, most spine surgeons may prefer to have their patients referred to other bone health specialists, such as endocrinologists or rheumatologists, for medical treatment of osteoporosis. 21
Multiple studies have reported on the benefits of medical treatment for osteoporosis prior to spine surgery.55-57 The patients who underwent osteoporosis treatment prior to surgery have been reported to have a significantly lower rate of complications and revision surgery compared to those who have not been treated. 55 This study and others indicate the potential benefit of osteoporosis treatment in spine surgery, specifically by anabolic medications, and the need for additional studies.56,57
Teriparatide, a parathyroid hormone analog, has been studied in the context of spine surgery. Its anabolic mechanism suggests it may promote fusion after surgery, unlike bisphosphonates (BPs), which primarily help maintain bone mass.58-61
Medical treatment with Teriparatide perioperatively has been shown to result in a decrease in complication rates including screw loosening, rod fracture, adjacent vertebral fracture, and pseudarthrosis when compared to bisphosphonates or no treatment.57,59,62-64 Four studies identified a shorter time to bone union and 4 studies identified a higher overall rate of fusion with TP as compared to BPs or no medical treatment.58-61,65,66 Inoue et al. 67 uniquely studied insertional torque of pedicle screws for patients treated preoperatively with TP for 1 month and found a higher insertional torque as compared to patients with no medical treatment. Recently, a retrospective study reported on the benefits of medical management with TP prior to long segment posterior spinal fusion defined as 8 or more levels. 16 The study compared patients with osteoporosis treated with TP against those with Osteopenia and those with normal BMD. 16 Interestingly, patients with osteoporosis treated with TP had better patient reported outcomes and lower reoperation and symptomatic pseudarthrosis rate compared to those with osteopenia. 16 Whereas, the outcomes of those with osteoporosis treated with TP were equivalent to patients with normal BMD. 16
Studies with short term use of TP postoperatively have not found a benefit of TP on fusion rate or instrumentation complications.68,69 These studies suggest that longer than 6 months of postoperative dosing is likely required, as was done in the other studies which found a significant difference in patients receiving TP post operatively. TP was well tolerated in all studies, with primarily nausea, anorexia, and fatigue cited as side effects in two studies.59,65
Abaloparatide is an isolated human parathyroid hormone that is also an anabolic, bone forming medication. The effectiveness of Abaloparatide in improving BMD and decreasing vertebral fractures has been proven in many studies.70-73 Abaloparatide is considered an alternative to teriparatide due to its similar mechanism of action. However, at present, there is no available literature on the use of Abaloparatide in spine surgery.
Bisphosphonates are the most common medications used in treating osteoporosis. 21 There are multiple studies regarding the efficacy and safety profile of bisphosphonates in spine surgery.74-82 Alendronate was shown to improve fusion rates after spine surgery in 2 studies and decreased the incidence of cage subsidence and vertebral fracture in one.74,75 One study demonstrated no effect of alendronate on fusion rate. 76 Zoledronate was shown to shorten the time to fusion and improve fusion rate in 3 studies, and to decrease the incidence of complications including cage subsidence, pedicle screw loosening, and vertebral compression fracture.77-79,82 However, another 3 studies found that zoledronate did not affect fusion rate.80-82 No study thus far has shown a negative effect of bisphosphonate use on fusion in spine surgery. However, several studies have demonstrated a superior outcome with Teriparatide use in spinal fusion when compared directly to bisphosphonates.59-62,64,66,69,83
Denosumab is similar to bisphosphonates in that it works as an antiresorptive medication. One study of denosumab in spine surgery exists where denosumab is combined with teriparatide (n = 9) and compared to teriparatide alone (n = 9), finding that the combination group had a higher lumbar interbody fusion rate and femoral neck BMD at 6 months. 84 Aside from this study, the effectiveness of denosumab in preventing vertebral compression fractures and other osteoporotic fractures has been well demonstrated in the Freedom Trial. 85
Romosozumab, a monoclonal anti-sclerostin antibody, is a newer medication that has both anabolic and antiresorptive effects.31,86-88 Mikula et al. 88 reported that treatment with Romosozumab for a mean duration of 10.5 months in 32 patients with osteoporosis resulted in a mean lumbar spine (L1-L4) CTHU improvement of 26% from baseline. It has not been specifically studied in spine surgery, however, its efficacy in preventing vertebral compression fractures has been well studied as it has been shown to decrease new vertebral fractures by 73% at 12 months.86,87
The guidelines by Sardar et al. 28 recommend using Teriparatide or Abaloparatide as the first line agent for the treatment of osteoporosis in adult patients planning to undergo spinal reconstruction. Antiresorptive agents such as Denosumab or Zoledronate are recommended if there are contraindications to the use of anabolic agents or if the patients are unable to tolerate the anabolic agents. 28
Optimizing Vitamin D and Calcium Levels Prior to Surgery
Vitamin D deficiency is commonly seen in patients undergoing spinal surgery and is often not diagnosed prior to the surgery.89-91 Assessment and treatment of low serum 25-hydroxyvitamin D levels is important prior to spine surgery and is an important component of the medical treatment of osteoporosis. Panjoka et al found that surgeons requested serum calcium levels in 67% of cases and vitamin D levels in 59% of patients. 21 The literature regarding vitamin D deficiency in spine surgery is limited. Several studies have demonstrated that higher vitamin D levels are linked to improved clinical outcomes, including better ODI scores and reduced pain after spine surgery.91-94 Ravindra et al found a statistically significant association between vitamin D deficiency and both nonunion and longer time to fusion within the first year following spinal fusion surgery. In contrast, Donnally et al. 95 reported no significant differences in spinal fusion rates, revision surgeries, or instrumentation failure after one year. Vitamin D supplementation is suggested for those with Vitamin D insufficiency.28,93,96
Fixation Strategies in Osteoporotic Bone
Multiple techniques to improve fixation in the osteoporotic spine have been developed. These include sublaminar wiring, cement augmentation of pedicle screw fixation (Figure 6), hook fixation, conical screws, hydroxyapatite-coated screws, fenestrated screws, expandable screws, and circumferential fusion (Figure 6).10,97,98 Other techniques employed to improve fixation in osteoporotic bone include using pedicle screws of larger diameter and length, limited tapping of the pedicle, achieving bicortical fixation, and creating a longer instrumented spinal construct.41,97,98 Example of Cement augmentation and anterior column support to improve fixation in patients with Osteoporosis.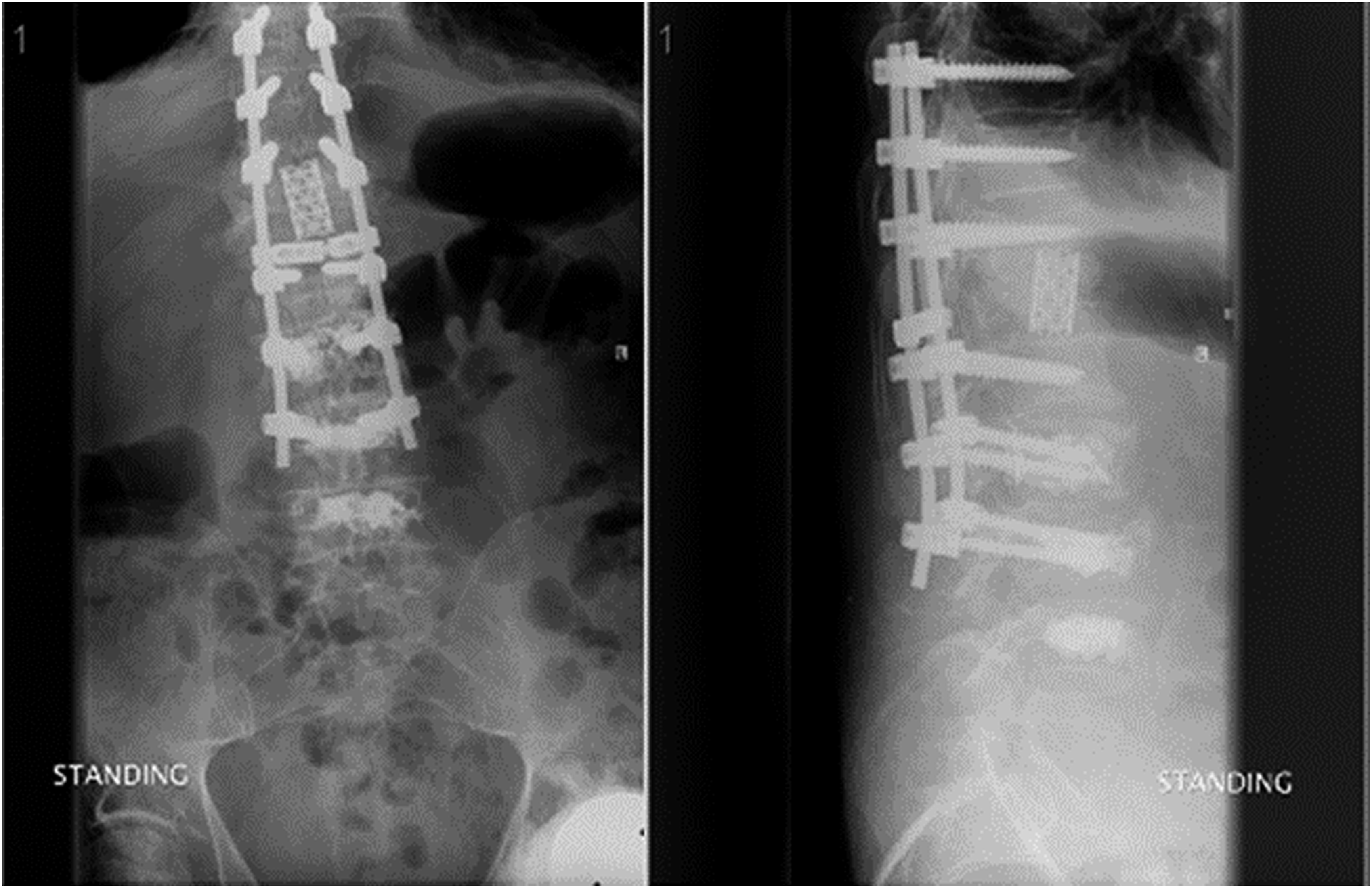
Iliac or pelvic fixation is important in patients with osteoporosis if a multisegmented fusion to the sacrum is being planned.98,99 This can avoid subsequent S1 screw loosening or sacral fractures which can be seen in patients with osteoporosis undergoing spinal fusions to the sacrum (Figure 3).98-101
Cement augmentation of the vertebral bodies at UIV and UIV +1 has been studied in the context of decreasing proximal junctional kyphosis in patients with osteopenia or osteoporosis.102-104 Findings support a lower incidence of early junctional failure and junctional kyphosis within 6 months of surgery with cement augmentation of both UIV and UIV +1 as opposed to no cement augmentation or cement augmentation of only the UIV.102-104 The UIV in these studies was in the lower thoracic spine.102-104 Unfortunately, a 5 year follow up study did not show a significant difference in PJK or PJF rates. 105
A survey of Spanish surgeons concluded that only 48% of members modified their surgical strategy in patients with osteoporosis and 70% of those would choose cement augmentation of the pedicle screws as their preferred technique (Figure 6). 22
A survey of 349 surgeons belonging to AO Spine Latin America reported that when treating patients with osteoporosis, 65.3% of surgeons extended instrumentation to incorporate additional levels and 63.8% utilized cement augmentation of vertebral bodies. 21 However, only 21% of surgeons believed that osteoporosis was the main cause of a poor final surgical outcome.
Circumferential fusion is another strategy noted to be employed for fusion in patients with osteoporosis. In a nationwide inpatient sample of patients undergoing cervical spine surgery from 2002 to 2011, Osteoporotic patients were more than 2 times likely to undergo posterior cervical spine fusion and 3 times more likely to undergo combined anterior/posterior fusion compared to those without osteoporosis. 10
Management of patients with osteoporotic vertebral fractures leading to sagittal plane deformities is not very well defined. Anterior reconstruction with strut graft or a cage has been shown to be effective in managing osteoporotic fractures with kyphosis. 106 For patients with severe kyphotic deformity and neurologic compromise, posterior closing wedge osteotomy has demonstrated better outcomes compared to combined anterior-posterior procedure with a lower blood loss and shorter operative time. 107
Summary
The incidence of osteoporosis in patients undergoing spinal reconstruction is significant and is reported between 10%-50%. Bone mineral density testing (BMD) using a DEXA scan is recommended for all patients over the age of 65 planning to undergo ASD surgery. Those younger than 65 with a risk factor should also undergo BMD testing. Such risk factors include: previous low energy fracture, history of metabolic bone disease, chronic corticosteroid use, smoking, excessive alcohol use, chronic kidney disease, prior failed surgery (fracture, pseudarthrosis, instrumentation failure), history of cancer treatment, chronic kidney disease, active smoker. Opportunistic CT based Hounsfield units can be used to get an estimate of the patient’s bone health and can lead to formal assessment in those with low CTHU values. Patients who qualify for medical treatment of osteoporosis prior to surgery should receive medical treatment for optimization prior to surgery. The duration of treatment may depend on the type of agent used. Anabolic agents such as Teriparatide and Abaloparatide can decrease the risk of osteoporosis related complications such as instrumentation loosening, proximal junctional kyphosis, and pseudarthrosis if used for the appropriate period before and after ASD surgery.
Techniques to improve fixation in the osteoporotic spine include sublaminar wiring, cement augmentation of pedicle screw fixation, hook fixation, conical screws, hydroxyapatite-coated screws, expandable screws, and circumferential fusion. Screw fixation can be further optimized by using pedicle screws of larger diameter and length, limiting tapping of the pedicle, and achieving bicortical fixation. Iliac or Pelvic fixation should be strongly considered in patient osteoporosis undergoing a long segment fusion to the sacrum.
Future Directions and Research
Future directions should involve studying the optimal duration of preop and postop treatment with anabolic agents such as Teriparatide. Further research is also needed to establish thresholds for bone mineral density that would lead to adverse outcomes in patients undergoing spinal reconstruction. Additionally, new bone mineral density thresholds need to be identified to trigger medical treatment of patient with osteopenia due to the non-physiologic stress placed on vertebra after spinal reconstruction even if they don’t meet the WHO definition for osteoporosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.