
Abstract
Study Design
Literature review with clinical recommendations.
Objective
To highlight important studies about osteoporotic spinal fractures (OF) that may be integrated into clinical practice based on the assessment of the AO Spine KF Trauma and Infection group key opinion leaders.
Methods
4 important studies about OF that may affect current clinical practice of spinal surgeons were selected and reviewed with the aim of providing clinical recommendations to streamline the journey of research into clinical practice. Recommendations were graded as strong or conditional following the GRADE methodology.
Results
4 studies were selected. Article 1: a validation of the Osteoporotic Fracture (OF)-score to treat OF fractures.
Conclusions
Management of patients with OF is still complex and challenging. This review provides some recommendations that may help surgeons to better manage these patients and improve their clinical practice.
Introduction
In the setting of an ever-expanding elderly population, the incidence of osteoporotic vertebral body fractures continues to rise.1-3 Recent studies have shown an increasing prevalence from 2009 to 2019, especially among individuals over 70 years.1-3 These injuries are usually a result of low energy trauma and have the potential to significantly increase morbidity and mortality by up to 15%.2,3 Despite their biomechanical stability, these common fractures can cause debilitating pain and a significant reduction in the quality of life as well as the independence of patients. The optimal management algorithm, encompassing both medical and surgical interventions, is yet to be clearly defined.
To improve the treatment of osteoporotic vertebral fractures worldwide, the development of simple, clinically useful classifications and therapeutic algorithms are required. Schnake et al have pioneered the new AO Spine-DGOU Osteoporotic Fracture (OF) Classification System. 4 The gradated introduction of osteoporotic fractures across 5 categories provides clinicians with a structured hierarchical measure of the severity of osteoporotic fractures. 4 To standardize treatment approaches, the authors identified critical factors that influence decision-making in these patients using the Osteoporotic Vertebral Fracture Score (OF-Score) system. Clinical evaluation of the OF treatment score is discussed in Article 1. 5
To provide some answers to the debate around conservative vs surgical management, current guidelines including those proposed by the American Academy of Orthopaedic Surgeons, aim to recommend certain interventions such as bed rest, analgesics or even orthoses. 6 While clinical practice guidelines intent to optimize patient care, the current available guidelines in the management of osteoporotic vertebral fractures remain ambivalent and unable to definitively recommend certain interventions. 6 With its well-known inhibiting effect of bone resorption, Bisphosphonates have been the cornerstone of osteoporosis treatment for decades. However, decisions around when to start, stop or change the bisphosphonate therapy are challenging due to limited evidence and concerns about long-term safety, including rare but serious adverse events such as atypical femoral fractures and osteonecrosis of the jaw, have prompted the exploration of alternative, and potentially more effective, treatment options. 7 Therefore, the role of combining bisphosphonates with anabolic agents in the management of osteoporotic vertebral fractures is discussed in Article 2. 8
In addition to implementing appropriate endocrinological management, spinal orthoses can have a supportive role in improving biomechanical outcomes by minimizing the range of motion, promoting alignment and reduce the risk of post-traumatic kyphotic deformity while allowing time for vertebral fracture to heal. Article 3 discusses a systematic review reporting on the existing evidence of spinal orthoses in the treatment of osteoporotic thoracolumbar vertebral fractures. 9
Irrespective of the treatment approaches, the treatment goals include pain relief, restoring mobility and body image, and avoiding further fractures. While most patients will benefit from conservative treatment, there is a risk of post-traumatic deformity when conservative treatment fails, leading to serious complications. Therefore, the role of pre-injury use of steroids for middle column injuries and its associated risk on post-traumatic deformity is discussed in Article 4. 10
In this context, this review has as the main goal to evaluate important studies related to classification and treatment algorithms, the use of bisphosphonate and orthoses and avoiding post-traumatic deformity, extracting strong to conditional clinical recommendations that may be useful for surgeons in their clinical practice by considering patient preferences and values, risk/benefit, feasibility, and resource implications.
Article 1
Clinical Evaluation of the Osteoporotic Fracture Treatment Score (OF-Score): Results of the Evaluation of the Osteoporotic Fracture Classification, Treatment Score and Therapy Recommendations (EOFTT) Study. Ulrich BW et al. Global Spine J 2023 Apr 13(1):29S-35S(1) 5
Clinical Rationale
Osteoporotic Vertebral Fracture Score (OF-Score).
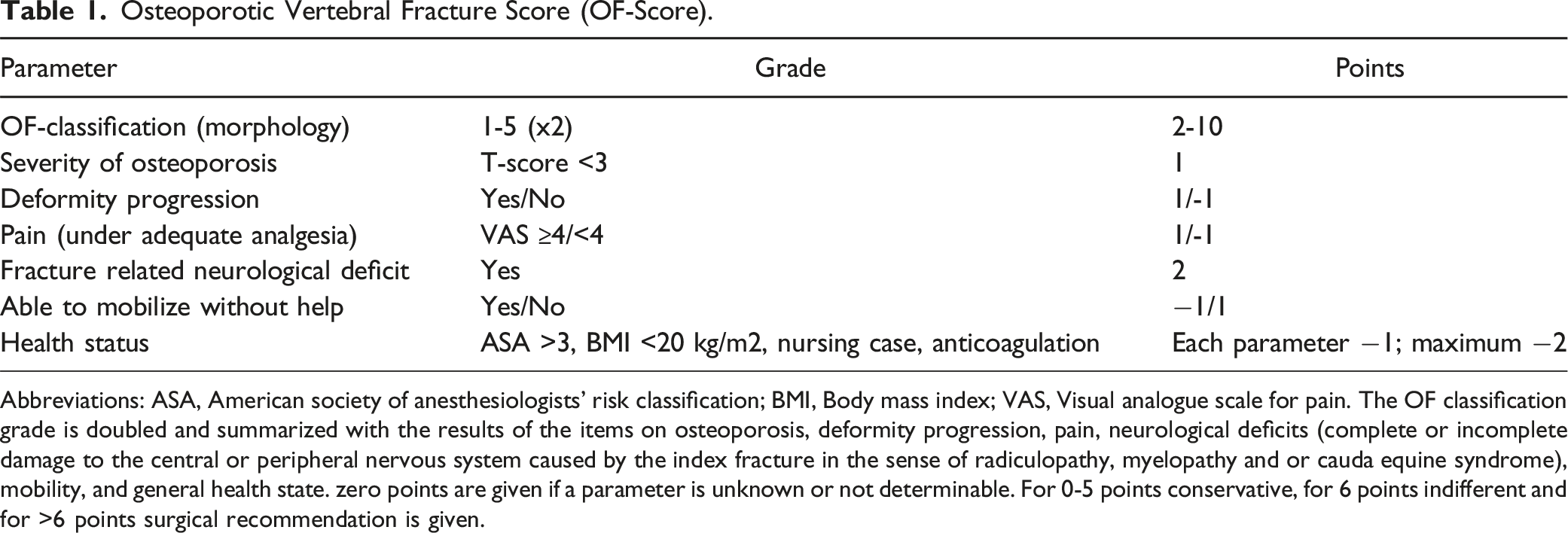
Abbreviations: ASA, American society of anesthesiologists’ risk classification; BMI, Body mass index; VAS, Visual analogue scale for pain. The OF classification grade is doubled and summarized with the results of the items on osteoporosis, deformity progression, pain, neurological deficits (complete or incomplete damage to the central or peripheral nervous system caused by the index fracture in the sense of radiculopathy, myelopathy and or cauda equine syndrome), mobility, and general health state. zero points are given if a parameter is unknown or not determinable. For 0-5 points conservative, for 6 points indifferent and for >6 points surgical recommendation is given.
With this article, they summarized and recommended the findings of a large multicenter observational prospective cohort study - The
Clinical Summary
The authors found improved pain and clinical parameters in every group observed. However, patients treated according to the OF-Score recommendation improved better, especially regarding early mobilization and less pain at 5 months follow-up. 5
The authors evaluated the concordance between the OF-Score recommendation (conservative or surgical) and the final treatment. 5 In this regard, 71% of the patients were treated in accordance with the treatment recommendation. 5
In 86% of cases, the score clearly recommended either surgery or conservative treatment. 5 The score was intermediate in 14% of cases, leaving the recommendation to the treating physician. 5 This distribution shows that the OF-Score is valid for discriminating between the groups for therapy recommendation. This is probably due to the narrow indeterminate range (score of 6), decreasing the likelihood of falling into this category. Interestingly, the authors found that patients in the conservative non-compliant group had a significantly higher level of pain and a poorer quality of life at the beginning of the observation. The surgical non-compliant group patients were healthier and had less pain than the corresponding compliance group. This suggests that the most influential factors in treatment decision-making are pain and health-related quality of life. As a result, in the revised AO Spine-DGOU OF-Score the threshold for pain on VAS was elevated from 4 to 5. 12
Urinary tract infections were the most frequent complications in the conservative and surgical group. 5 1 percent of surgically treated patients needed revision surgery due to a deep wound infection. 5 Adjacent level fractures were more frequent in the surgical (8%) than in the conservative group (4%). 5
This study does not report and evaluate the various surgical treatments used and is limited to reporting the clinical parameters after 5 months only. However, most of the clinical pain from traumatic injuries occurs in the first few months after injury.
The authors state that, besides the severity of the fracture according to the OF classification, back pain and disability were the most important factors when reevaluating the decision-making process. 5 This might leave some room for improvement of the score by giving these factors more weight within the score.
Methodological Review
The EOFTT study was conducted as a prospective multicentric observational study, to externally validate the OF Classification. The study included 17 centers in Germany and Switzerland. Although not the highest quality of evidence, this study design enhances generalizability and lends itself to surgical trials. The study included patients older than 18 years hospitalized for a traumatic or low energy trauma OF and a proven diagnosis of osteoporosis. In patients with more than 1 OF, the most severe fracture based on the OF classification was used for evaluation and treatment decisions. The 2 cohorts were those patients treated according to the OF-Score and those not.
The sites recorded the OF-Score, type of treatment (conservative/surgical), Oswestry Disability Index (ODI), visual analogue scale subjective health state form EQ5D (VAS-EQ(5D)), EQ5D- 5L index value, Barthel, Timed up and go test (TuG) and Pain at visual analogue scale (VAS-P). 5 4 follow up visits were scheduled (6 and 12 weeks and 6 and 12 months). If not all 4 visits were made, the last 1 was used for data analysis.
Based on treatment performed and OF-Score recommendation, patients were classified in 6 groups. 5 The first group’s recommendation and treatment were conservative (conservative-compliant); the second group’s recommendation was conservative, but the treatment was surgical (conservative-noncompliant); the third group’s recommendation was indifferent (indifferent-conservative) and received conservative treatment; the fourth group’s recommendation was also indifferent (indifferent-surgical), but received surgical treatment; the fifth group’s recommendation was recommendation and treatment were surgical (surgical-compliant); and the sixth group’s recommendation was surgical, but received conservative treatment (surgical-noncompliant).
Recommendation for Integrating into Your Clinical Practice
Patients with an osteoporotic thoracolumbar fracture usually improve in pain and clinical parameters over time regardless of the treatment chosen. The OF-score is a simple and reliable tool to recommend treatment in these patients. Treatment according to the OF-score led to less pain and better quality of life than treatment of patients who were not treated according to the score at 5 months of follow-up, improving recovery time. The revised OF-Score can be found on the AO Spine website.
12
We
Article 2
Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis. Saag KG, et al. N Engl J Med. 2017 Oct 12;377(15):1417-1427. 8
Clinical Rationale
Romosozumab is an anabolic agent, approved by the Food and Drug Administration (FDA) in 2019. As a monoclonal antibody, it binds to and inhibits sclerostin, increasing bone formation and decreasing bone resorption. The FRAME study previously demonstrated the efficacy of romosozumab for the prevention of new vertebral fractures in osteoporotic women in comparison to placebo. 13 However, few studies directly compare the efficacy of anti-resorptive and anabolic agents for the prevention of vertebral compression fractures.
The Active-Controlled Fracture Study in Postmenopausal Women with Osteoporosis at High Risk (ARCH) 14 compares the effectiveness of a treatment regimen starting with romosozumab and transitioning to alendronate alone. 8 Alendronate, a bisphosphonate, is commonly used as first-line therapy for osteoporosis and has been proven effective in reducing the risk of osteoporotic associated fractures among postmenopausal women. 15 Improving bone quality with anabolic agents can reduce the chances of fractures but also prevent complications in selected patients with osteoporosis who may require spinal instrumentation.
Clinical Review
The main goal of the study was to prove the clinical superiority of initiation therapy with anabolic agents in the management of osteoporotic patients. 8 The authors aimed to show romosozumab initiation therapy for 12 months is better at lowering the risk of subsequent fractures compared to alendronate for 12 months, an antiresorptive agent (bisphosphonate). After initiation with either medication, both groups of patients were then treated with alendronate until the completion of the study.
The results show that the use of romosozumab-alendronate over 24 months led to a 48% decreased risk of new vertebral fractures when compared to the alendronate-alendronate group, a statistically significant result (6.2% vs 11.9%, respectively, P < 0.001). 8 Additionally, in terms of a clinically important fracture (defined as a nonvertebral fracture or a symptomatic vertebral fracture), the romosozumab-alendronate group exhibited 27% lower risk compared to alendronate alone patients (P < 0.001). When comparing bone mineral density changes between groups, the romosozumab-alendronate patients exhibited greater gains from baseline throughout the studied period and measured sites compared to the patients that only received alendronate (P < 0.001). Finally, the levels of bone-forming markers were increased, and the levels of bone resorption markers decreased in the group that received romosozumab. These are relevant observations when considering managing patients with osteoporosis suffering from spinal pathology, as there may be a benefit in considering anabolic agent use to lower suboptimal patient outcomes.
Although the incidence of adverse events was overall similar between the 2 groups, the study did identify an imbalance in serious cardiovascular adverse events in the romosozumab-alendronate group in comparison with alendronate-only group. In all, 0.8% of patients in the romosozumab group and 0.3% in the alendronate-alone group suffered from cardiac ischemic events and/or cerebrovascular events; while other cardiovascular events were lower in the romosozumab group (such as heart failure, peripheral vascular ischemic events and noncoronary revascularization).
Methodological Review
This is a phase 3, multicenter, international, randomized, double-blind trial, where women were randomly assigned, in a 1:1 ratio to receive monthly subcutaneous romosozumab (210 mg) or weekly oral alendronate (Merck; 70 mg) for 12 months. 8 After completion of the double-blind trial period, all the patients received open-label weekly oral alendronate (70 mg) until the end of the trial, with blinding to the initial treatment assignment maintained. Patients received daily calcium (500-100 mg) and vitamin D (600-800 IU).
Patients enrolled included women from ages 55-90 years who had at least 1 of the following criteria: (1) bone mineral density T score of −2.5 or less at the total hip or femoral neck and either 1 or more moderate or severe ventral fractures or 2 or more mild vertebral fractures, (2) a bone mineral density T score of −2.0 or less at the total hip or femoral neck and either 2 or more moderate or severe vertebral fractures or a fracture of the proximal femur sustained 3 to 24 months before randomization. Patients were excluded if they had a history of metabolic bone disease or conditions affecting bone metabolism, osteonecrosis of the jaw, a 25-hydroxyvitamin D level of less than 20 ng per milliliter, current hypercalcemia or hypocalcemia, recent use of drugs affecting bone metabolism, or inability to take alendronate.
The trial’s primary outcome was the cumulative incidence of new vertebral fracture at 24 months and the cumulative incidence of clinical fracture (nonvertebral and symptomatic vertebral fracture). Secondary outcome was bone mineral density at the lumbar spine, total hip, and femoral neck at 12 and 24 months. Lateral radiographs of the thoracic and lumbar spine were obtained at screening and every 12 months thereafter until the time of primary analysis. Bone mineral density was evaluating using dual-energy X-ray absorptiometry at baseline and every 12 months thereafter.
The sample size of the study was substantial, with a total of 4093 participants randomized into the 2 treatment arms. The trial was adequately powered, with 94% power to detect a 30% lower risk of clinical fracture and 95% power to detect a 50% lower risk of new vertebral fracture of 24 months for the romosozumab-to-alendronate group compared to the alendronate only group.
Recommendation for Integrating into Clinical Practice
A
Article 3
Spinal Orthoses in the Treatment of Osteoporotic Thoracolumbar Vertebral Fractures in the Elderly: A Systematic Review with Quantitative Quality Assessment. Pieroh P, et al. Global Spine J 2023, Vol. 13(1S) 59S–72S. 9
Clinical Rationale
Despite the lack of solid and robust evidence, many surgeons are prescribing spinal orthosis or corset for patients with OF fractures. The results of previous studies are controversial and factors that may influence orthosis prescription such as injury site, time of treatment, number of injuries, among others, were not consistently reported and are based on limited evidence.15-17 In this context, Pieroh et al. published a systematic review with the primary aim of reporting on the existing evidence on spinal orthosis treatment in OVFs and describing the treated population, fracture morphology and type of orthotic treatment. 9 The secondary aim was to grade the examined publications using quantitative quality scores. The tertiary aim was to analyze and qualitatively grade previous systematic reviews. The main question to be answered with that systematic review was: “Does spinal orthoses improve the outcome of patients suffering from thoracolumbar spinal fragility fractures and related deformities?”
Clinical Summary
Thirteen studies (5 RCTs, 3 non-RCTs, 5 prospective studies) and 8 systematic reviews were included in the study (mean age above 65 years of age in all assessed studies). 9 5 studies investigated the impact of applying a spinal orthosis after thoracolumbar fragility fractures without comparison and showed generally more gait stability, a decrease in falls as well as an increase in back extensor muscle strength. Improvements in QoL measurements were not convincingly observed, however, a significant decrease in pain was observed. Use of an orthosis resulted in a success rate of >80%, and high-intensity T2-weighted MRI and vertebral instability of >5° at 3-week follow-up were identified as risk factors for treatment failure. Three studies compared the impact of different orthosis systems (Spinomed; 3-point orthosis; soft brace). Spinomed orthosis showed better FEV1 lung functions compared to the 3-point orthosis. Radiological parameters like anterior vertebral body percentage or Cobb`s angles did not differ significantly between the different types of orthoses after 6 months. Independent of the kind of orthoses, pain decreased significantly over time and the Spinomed orthosis showed significantly better pain reduction at 3- and 6-month follow-up compared to the 3-point orthosis. Improvements in QoL measurements were inconsistent and not significantly different between the different types of orthoses. Five studies investigated the difference between orthosis and no orthosis in the conservative treatment of thoracolumbar fragility fractures. Wearing of an orthosis did not have an impact on QoL, pain reduction, radiological assessments or minimized opioid intake in 3 of the assessed studies. In contrast, 2 studies with probably identical cohorts showed significant differences in pain decrease, radiological parameters, QoL and muscle strengths in favor of the orthosis group. Pain and QoL measures improved over time irrespective of orthotic treatment.
The comparison to other systematic reviews (n = 8) revealed that according to the PRISMA score, 6 reviews were graded low, each 1 moderate and high. 9 Furthermore, 5 of the assessed reviews detected low evidence of orthoses in the treatment of thoracolumbar fragility fractures and still recommended their use.
They concluded that spinal orthoses decreased pain and improved QoL over time, but there were no differences in the outcome of patients treated without it. 9 A general prescription for using a spinal orthosis was not possible in treating osteoporotic fractures.
Methodological Review
Looking at the inclusion and exclusion criteria of that systematic review, 1 of the strenghts of this study is the inclusion of both English and German language articles, in contrast to the majority of systematic reviews which include only English articles. 9 However, all study designs were included, only narrative reviews and case reports were excluded. It would have been more in line with the study question to include only comparative studies comparing the use of orthosis to no orthosis which would have provided more clinically relevant studies. Additionally, given that the study is orthotic-related, excluding studies funded or sponsored by orthotic manufacturers would have eliminated a major source of bias.
Multiple quality assessment tools were used in assessing the finally included articles, which provided an in-depth assessment of the studies and shed more light on possible weak points. A meta-analysis was not feasible due to the heterogeneous nature of the outcome assessment tools. Examining the extracted data from the studies, we find that there is non-conformity in the use of spinal orthosis, as the duration of orthosis application varied from 15 minutes per day to the whole day, with 3 studies not defining the duration of the application and also the duration of treatment varied from 2 months to 12 months.18-24 Additionally, only 3 studies reported a fracture classification system which is integral in decision-making in osteoporotic fractures.22,23,25
Generally, the methodology of this study has a clear study background, question and rationale. The steps of conducting the systematic review were clearly explained and properly conducted. Additionally, the assessment tools and statistical analysis employed by the authors for this investigation appear to be appropriate.
Recommendation for Integrating into Clinical Practice
Based on the currently available literature, the study generally supports the benefits of soft or active orthosis early application in improving both pain and QoL in patients with osteoporotic fractures. Considering the inconsistencies and lack of high-quality data obtained in these studies, we believed that a
Article 4
Impact of Insitial Conservative Treatment Interventions on the Outcomes of Patients with Osteoporotic Vertebral Fractures. Hoshino et al. Spine (Phila Pa 1976) 2013 May 15;38(11): E641-8. 10
Clinical Rationale
Although most osteoporotic vertebral fractures are expected to heal uneventfully, 15%–35% can result in adverse sequelae as these fractures heal in varying degrees of kyphosis. 26 This can result in chronic pain, poor chest function, decreased appetite, kyphotic deformity, fatigue, and functional neurological disturbances. Several studies have shown that osteoporotic fractures affect the local and global sagittal balance of the spine. So, the aim of treatment should not only focus on fracture healing but also the eventual sagittal spinal alignment. De Gendt et al highlighted the importance of minimizing post-traumatic deformity and argued that even a minimal amount of kyphosis can deteriorate into progressive traumatic deformity which may or may not be symptomatic in the future. 27 Considering the potential impact of quality of life and risk of clinical and neurological deterioration, evaluating the risk factors for spinal deformity for OF are necessary.
Clinical Summary
This prospective multicentre study recruited 485 patients aged 65 years and older from 25 institutes in Osaka with conservatively managed osteoporotic vertebral fractures. 10 The definition utilized is consistent with existing literature and secondary to low energy trauma following which patients were afflicted by acute back pain, deformed vertebral body on radiograms and abnormal vertebral body intensity on magnetic resonance imaging (MRI).28,29
The authors recorded 6-month patient outcomes following the initial injury which were dichotomized into patient-reported outcomes measures as well as objective biomechanical measures. 10 The Short Form-36 (SF-36) physical component summary (PCS) and mental component summary (MCS), activities of daily living (Japanese long-term care insurance system), back pain as measured on the visual analogue scale and cognitive status (mini-mental state examination) were self-reported by patients at final follow-up. The authors also defined vertebral collapse as a ≤50% anterior vertebral collapsing ratio on plain radiographs in the standing position, or the anterior height of the fractured vertebral body was ≤50% of the adjacent intact vertebral bodies. 10
Although all treatments were non-operative, several individual treatment factors were analysed with multivariate logistic regression analysis. These encompassed brace types with multivariate logistic regression analysis. These encompassed brace type utilized, hospitalization, bisphosphonates usage or presence of middle-column injury. 10 The role of previous steroid use was also examined as a secondary measure. The authors carefully documented their inclusion and exclusion criteria and follow-up at each stage. The cohort’s mean age was 76.3 years (range 65-83 years) and fractures at the thoracolumbar junction were the most observed (75.1%). The middle column was affected in 30.4% of patients and at final 6-month follow-up it was noteworthy that 31.2% of patients had experienced vertebral collapse. Intriguingly, the only independent risk factor associated with poorer clinical and radiological outcomes (SF-36 PCS ≤40, reduced activities of daily living, prolonged back pain and vertebral collapse) was the radiological finding of middle-column involvement on the initial radiograph. Post-traumatic deformity or delayed vertebral collapse was not affected by any of the other variables in this landmark study.
Methodological Review
All included patients had an MRI to confirm abnormal intensity within the vertebral bodies. 10 This would not necessarily be routinely performed in neurologically intact elderly patients who sustain an osteoporotic vertebral body fracture in all centers.30-32 For this reason, there may be a degree of external validity loss secondary to the inability to generalize the authors’ findings to other international hospitals. Also, the definition of an osteoporotic fracture is nebulous in this study. The authors have included spinal fractures in people aged >65 years following a low energy trauma. Objective measures to document the bone density are missing.
Furthermore, the decision to conservatively manage individual patients was decided by the doctors based on their clinical experience in this study. No formal or standardized treatment algorithm was utilized based upon a combination of clinical and radiological factors. Although all treating decisions were determined by specialist orthopaedic surgeons, the lack of uniformity results in the potential for selection bias. The readers should therefore be aware that the selected cohort of patients is heterogenous. More than this, the authors did not specifically state that patients were consecutively recruited or in any block fashion to further minimize the risk of non-random selection bias.
On the contrary, the statistical methodology in this article appears sound. Multivariate logistic regression analysis for relevant treatment factors were constructed with the standard statistically significant threshold of P < 0.05. However, an additional potential concern with this study is the attrition rate with a total of 485 patients being enrolled. 10 Only 420 patients completed the 6-month follow-up due to a variety of reasons include 15 being deceased, 11 excluded due another disease (heart failure, cerebral infarction, pulmonary emphysema) and 39 patients lost to follow-up. 10 Moreover, only 362 patients eventually completed all the required data. 10 Whilst a 86.6% follow-up is acceptable, it is difficult for readers to interpret the meaning of the collected data given the censored patients may have skewed the results either way. On 1 hand, it is possible that patients with conservatively managed OVFs may have such significant pain that they were bedbound and therefore experienced greater medical complications such as fluid overload in heart failure. On the other hand, excluding these medically unwell patients with poorer quality of physical and mental health may have resulted in falsely positive outcomes on follow-up of these conservatively managed OVFs. A larger study with improved follow-up would assist in mitigating these uncertainties raised by the attrition bias of this study.
Finally, the follow-up time for this study of 6 months is relatively short with longer-term clinical and radiological outcomes still being of interest. It is also striking that the brace was recommended in the majority of cases with only 35 patients being treated without an orthosis. There is also no clear mention of the rehabilitation programs instituted following the fracture or whether standard referral to a specialist endocrinologist for optimization of bone health was performed across all 25 participating sites. A comparison treatment group which underwent surgical intervention would also be useful to directly determine whether any of the patient-reported outcomes significantly differed between conservative and operative intervention.
A clinically relevant conclusion of middle-column injury and the pre-injury use of steroids being negative prognostic factors for both clinical and radiological outcomes is demonstrated. It is striking that other factors, such as brace type or bisphosphonate use, were not shown to affect post-traumatic deformity or vertebral collapse in this study.
This study would have been strengthened with a longer follow-up time, consecutive recruitment to minimize selection bias and a standardized treatment algorithm rather than individual clinicians determining whether patients received conservative or operative management. Post-traumatic deformity seems to occur in patients who sustained osteoporotic vertebral fractures in which the middle-column is affected, but other important risk factors require further investigation.
Recommendation Regarding Impact on Clinical Practice
A
Footnotes
Acknowledgements
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma & Infection, a focused group of international experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the AO Spine, AO Network Clinical Research.