
Abstract
Study Design
Retrospective Cohort Study.
Objective
Single Photon Emission Computed Tomography/Computed Tomography (SPECT/CT) is emerging as a valuable imaging test for identifying pain generators within the lumbar spine. The relationship between radiotracer uptake on SPECT/CT and anatomic biomechanical parameters has not been previously studied.
Methods
We performed a retrospective review of all patients seen at our institution between 2021-2023 who obtained SPECT/CT scans for workup of thoracolumbar back pain. Patient data including demographic, clinical symptoms, and surgical history were collected. Radiology reports were reviewed for evidence of pathologic degeneration and increased bone metabolism on SPECT/CT. Biomechanical parameters were measured from standing scoliosis plain radiographs. Patients were stratified into two cohorts by either presence or absence of asymmetric coronal uptake on SPECT/CT.
Results
160 patients met inclusion criteria. Patients were primarily male (55%) with average age 55 ± 15 years. 87 (54%) patients demonstrated asymmetric uptake on SPECT/CT. These patients were older (P < 0.001), but with similar gender, prior fusion history, sacroiliitis, adjacent segment degeneration, and pseudoarthrosis (P > 0.05). This cohort had more disc disease, facet arthropathy, and greater degree of coronal scoliosis and coronal imbalance (P < 0.001). There were significantly more sites of uptake in the asymmetric cohort, and uptake was preferentially observed in the concavity of the lumbar curve (P < 0.001). There were no significant differences in sagittal balance or spinopelvic mismatch between cohorts (P > 0.05).
Conclusion
Asymmetric uptake on SPECT/CT was associated with coronal deformity in patients with low back pain. Further prospective studies are warranted to assess the effect of coronal deformity on pain generation.
Keywords
Introduction
Low back pain (LBP) is the leading cause of disability in the adult population, with estimated spine care-related expenditures exceeding US$80 billion annually.1,2 Despite the prevalence of LBP, identifying patient-specific lumbar pain generators remains a challenge with conventional imaging.3-5 Determining the source of pain is an essential first step in guiding individualized management and providing optimal patient outcomes. Plain radiography, Computed Tomography (CT), and Magnetic Resonance Imaging (MRI) are useful imaging modalities to detect facet arthropathy (FA) and degenerative disc disease (DDD), but radiographic findings with these modalities are unable to differentiate between incidental and clinically relevant pathology.6-8 Traditionally, the gold standard for diagnosis of LBP in equivocal cases has required invasive diagnostic procedures including discograms and targeted injections. Furthermore, guidelines regarding the role of surgical intervention in the setting of isolated axial LBP are not currently well supported by evidence.9-11
One recent advance helping identify pain generators is Single Photon Emission Computed Tomography (SPECT) with computed tomography overlay (SPECT/CT) which combines functional and structural imaging. A variety of conditions, including degenerative disease, neoplastic processes, infection, inflammation, metabolic disease, and trauma result in increased osteoblastic activity compared to normal bone. SPECT imaging relies on principles of bone scintigraphy using bisphosphonate radiopharmaceuticals, analogs of calcium pyrophosphate, which are deposited with a greater affinity to sites of active pathologic osteoblast differentiation and calcium mineralization.12-14 Specifically, Technetium-99m is a highly sensitive agent used in planar bone scintigraphy with radioactivity detected by gamma cameras. While planar bone scintigraphy is highly sensitive for depiction of early functional derangements of bone, it is limited by the anatomic precision of the area of uptake. Combined SPECT/CT overcomes this limitation by combining the functional information of SPECT with precise localization and morphologic characterization of CT to better localize the site of uptake. The diagnostic value and complimentary nature of combined functional and anatomical imaging is increasingly recognized. 13 SPECT/CT has demonstrated with high sensitivity and specificity, up to 100% and 71% respectively,15,16 that relative bright signal from radiotracer uptake can identify potential pain generating lesions. 17 Accordingly, several studies have sought to evaluate the utility of adjunct SPECT/CT as a diagnostic and surgical planning tool for LBP to guide interventions.18-22
In parallel with the development of SPECT/CT, our understanding of spinal alignment and its importance in patient reported outcomes has evolved in the last two decades. Global spinal alignment and spinopelvic mismatch strongly influence biomechanical stresses and spine degeneration rates, which have become the dominant focus of surgical management in adult spinal deformity 23 The authors believe SPECT/CT identifies areas of active osteoblastic remodeling, which suggest these sites as biomechanical stress points.24-26 This study investigated the anatomic and pathophysiologic patterns of increased uptake on SPECT/CT and its association with measured spinopelvic parameters.
Methods
Patient Cohort
A retrospective analysis of all patients who obtained SPECT/CT for workup of LBP was undertaken at a single institution from January 1, 2021 to December 31, 2023. Adult patients (greater than 18 years) with available SPECT/CT of the thoracolumbar spine and corresponding standing scoliosis radiographs were included in this analysis. Pediatric patients, patients with recent thoracolumbar trauma history, and patients with SPECT/CT of cervicothoracic anatomy alone were excluded. Patients with SPECT/CT scans obtained for workup of infection, inflammatory, or neoplastic disease were also excluded. Patient demographic data including age, sex, and prior fusion history were acquired from chart review of the electronic medical record. Informed consent was waived by the nature of the retrospective study design, which was approved by the Institutional Review Board of Kansas University Medical Center in Kansas City, KS (IRB#00150790).
SPECT/CT Review
SPECT/CT scans were performed over several institutional sites with different machines, but with a standardized protocol. Each patient undergoing imaging received a weight-based dose of intravenous Technetium 99m and were observed for 3 hours prior to planar bone scintigraphy and subsequent CT imaging. All SPECT/CT studies were interpreted by one of 5 board-certified staff nuclear medicine radiologists. The output of each SPECT scan generated a heat map of the relative radiotracer standard uptake value. Radiologists interpreted these SPECT heat maps with CT overlay to identify sites of relative increased uptake compared to absent or normal physiologic levels. The authors independently reviewed the radiology reports to identify foci of increased uptake within the vertebral body, intervertebral disc, sacroiliac joints, or facet joints between L1-S1. Reports were also reviewed for radiographic diagnosis of FA, DDD, sacroiliitis, adjacent segment disease, and pseudoarthrosis. No measures were taken to evaluate consistency in the reporting of radiotracer uptake between radiologists.
Biomechanical Parameters
All standing scoliosis x-rays were reviewed by the authors (AD, AG). If multiple standing x-rays were available in the chart, the imaging obtained nearest the date of SPECT/CT acquisition was chosen for analysis. Biomechanical parameters, including pelvic incidence (PI), sacral slope (SS), pelvic tilt (PT), lumbar lordosis (LL), primary and secondary lumbar curves, coronal balance (CB), and sagittal vertical axis balance (SVA) were measured from standing scoliosis plain films using Sectra IDS7 imaging software.27,28
PI, SS, PT, LL, SVA, and spinopelvic mismatch were determined from standing lateral x-rays. PI was defined as the angle subtended by a line drawn from the center of the femoral heads to the midpoint of the sacral endplate and a line perpendicular to the center of the sacral endplate. SS was measured as the angle between the superior sacral endplate and a horizontal reference line. PT was calculated as the algebraic difference between PI and SS in degrees. LL represented the Cobb angle between the superior endplate of L1 and the superior endplate of S1. SVA was measured as the distance from a vertical plumb line at the center of the C7 vertebrae to the posterior edge of the upper sacral endplate surface in millimeters. Positive values indicated that the plumb line was anterior to the posterior edge of the upper sacral endplate surface, whereas negative values designated that the plumb line was posterior. Spinopelvic mismatch was calculated as the algebraic difference between the pelvic incidence and the lumbar lordosis.
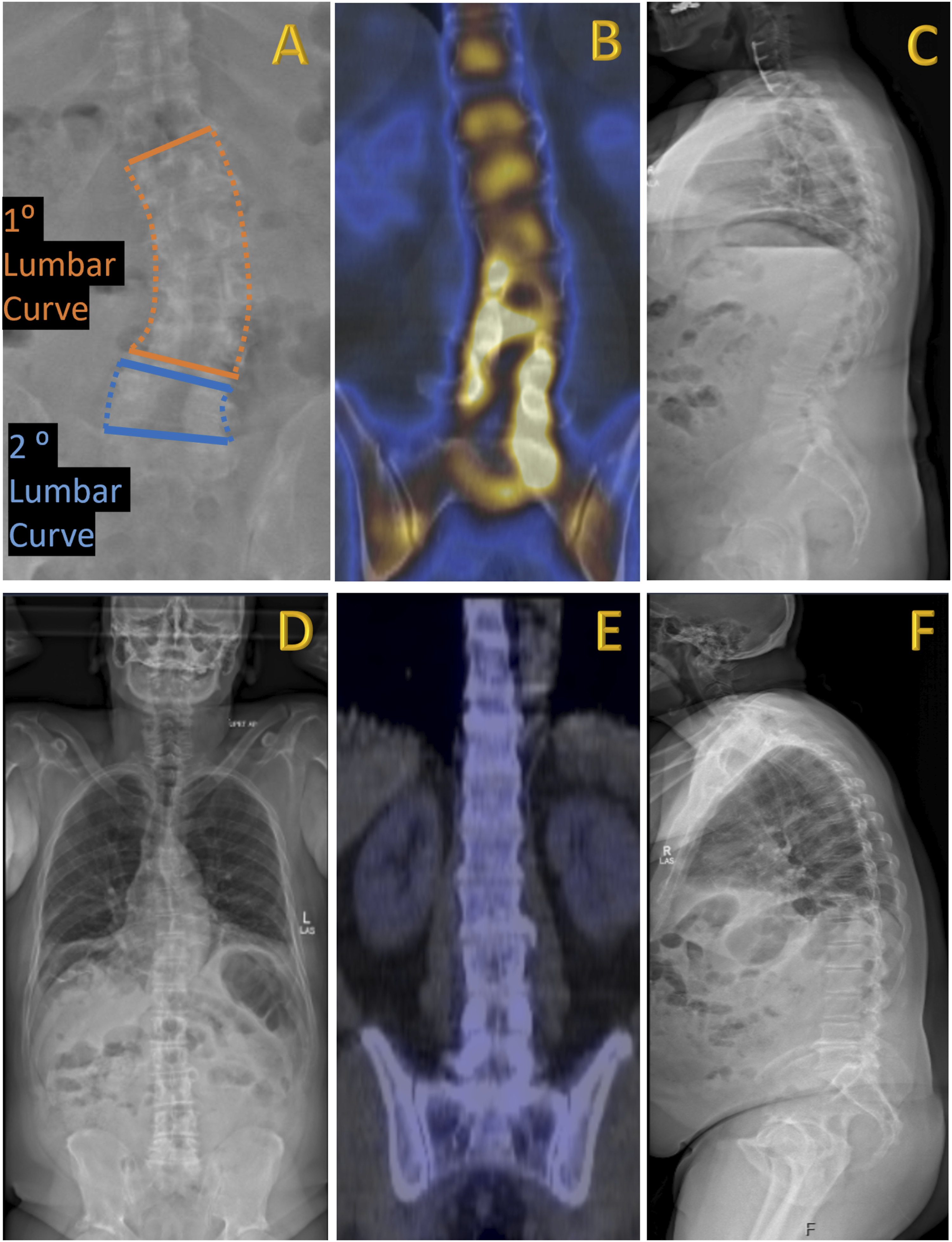
CB, primary and secondary lumbar curves were determined from standing antero-posterior x-rays. CB was measured as the horizontal distance in millimeters from the c7 plumb line to the sacral midpoint. The primary lumbar curve was defined as the curve of the continuous lumbar levels which encompassed the maximum segmental coronal cobb angle in degrees. The secondary lumbar curve represented the curve of the lumbar levels adjacent to the primary lumbar curve. We denoted whether corresponding uptake on SPECT/CT was located on the convexity or the concavity of the primary or secondary lumbar curves. An example of measurements, lumbar curves, and radiotracer uptake are illustrated in Figures 1 and 2. Illustrative case of radiographic parameters measured on standing scoliosis radiographs. (A) Lateral view standing X-ray. Red – pelvic incidence angle. The red circle demarcates the femoral head. Blue – pelvic tilt angle. Green – sacral slope angle. Orange – lumbar lordosis angle. Yellow – horizontal line demarcates the distance measurement for sagittal vertical axis balance. (B) Anterior-posterior view standing X-ray. Orange – solid lines indicate primary lumbar Cobb angle. Blue – solid line indicates the secondary lumbar Cobb angle. Dotted lines depict the corresponding coronal curvatures. Yellow – horizontal line demarcates the distance measurement for the coronal balance. (A) Anterior-posterior view standing X-ray in a patient with a leftward coronal scoliosis. Orange – solid lines indicate primary lumbar Cobb angle. Blue – solid line indicates the secondary lumbar Cobb angle. Dotted lines depict the corresponding coronal curvatures (B) Coronal view SPECT/CT with increased radiotracer uptake predominantly in the concavities of the primary and secondary curves. Radiologists reviewed increased uptake at the L2-3 right facet, L3-4 right disc, L3-4 right facet, L4-5 right facet, L4-5 left facet, L5-S1 left disc, and L5-S1 left facets. (C) Corresponding lateral view X-ray demonstrating patient without spinopelvic mismatch and appropriate sagittal balance. (D) Anterior-posterior view X-ray in another patient with appropriate coronal balance and minimal primary lumbar Cobb angle. (E) Corresponding coronal view SPECT/CT with no identified sites of increased radiotracer uptake and (F) lateral view X-ray showing that the patient has sagittal imbalance and flat back.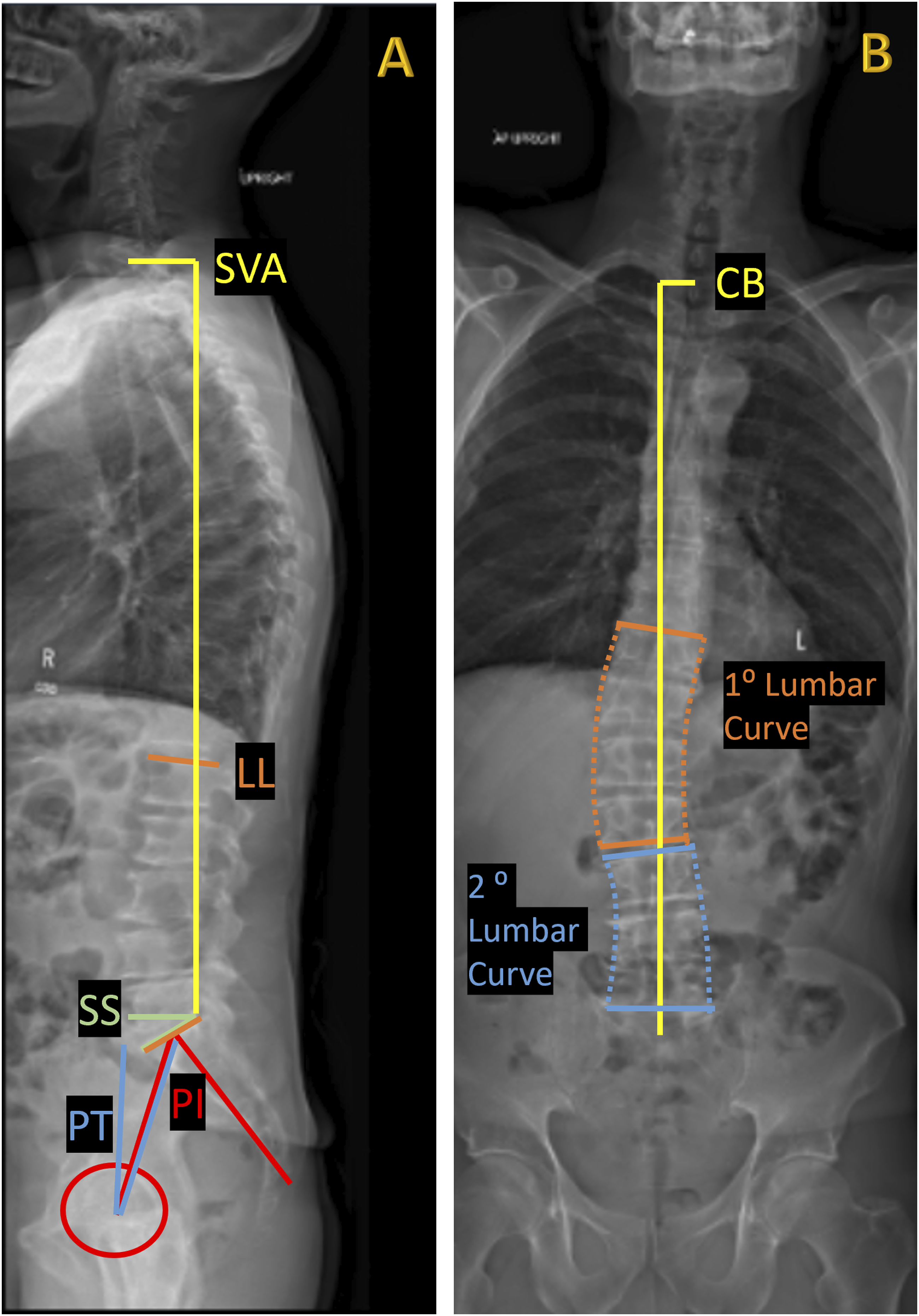
Statistical Analysis
Patients were stratified into asymmetric and symmetric coronal uptake cohorts. Patients with symmetric uptake had an equal number of right and left uptake sites on SPECT/CT, whereas the asymmetric cohort did not.
Data of each cohort were reported as mean with standard deviation or frequency with percent for continuous and categorical variables, respectively. The Pearson Chi-square test was used to assess the difference between proportions in categorical variables. An unpaired t test was used to assess differences between cohorts for continuous variables. P-value <0.05 was deemed statistically significant. The data was analyzed using the International Business Machines (IBM)® Statistical Package for the Social Sciences (SPSS)® software (IBM, New York, U.S.).
Results
Patient Demographics
Overall Patient Demographics, Fusion History, and Sites of Increased Uptake on SPECT/CT.
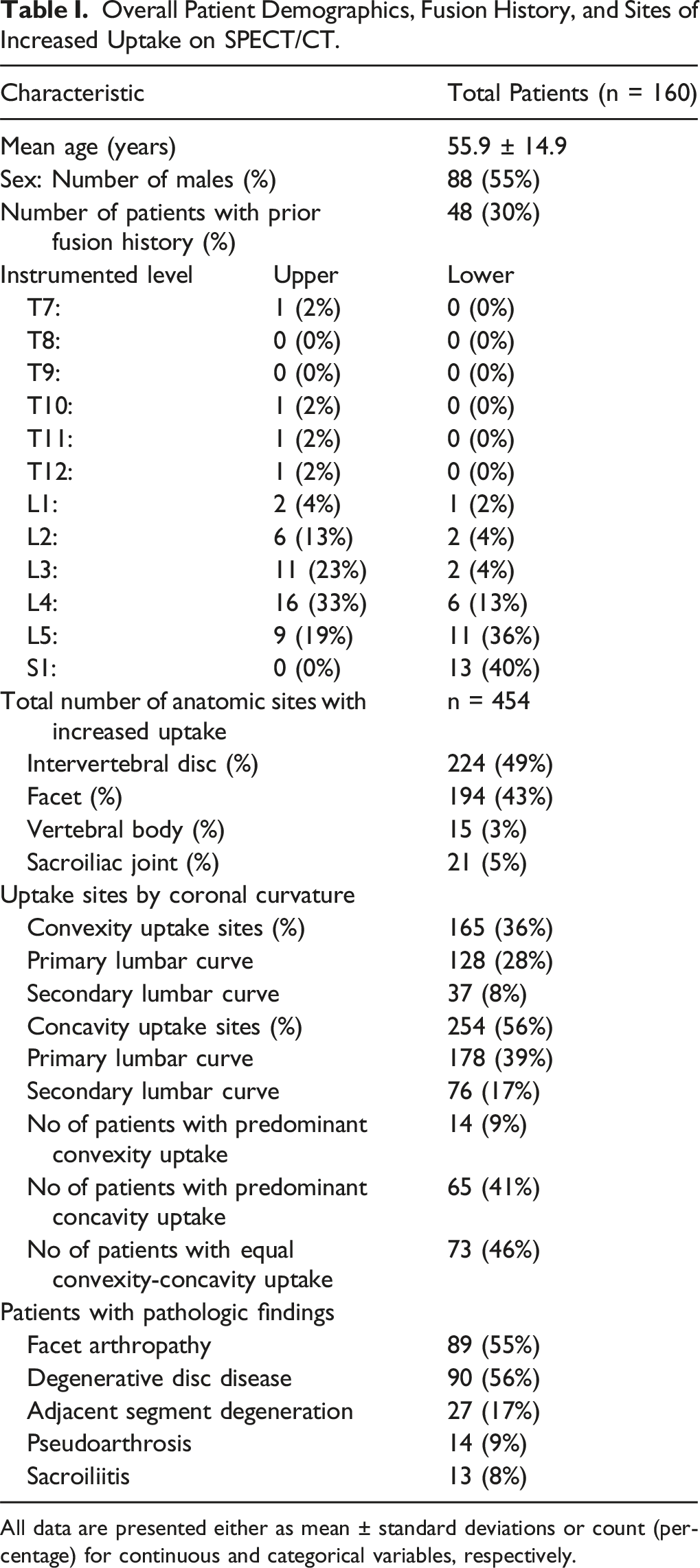
All data are presented either as mean ± standard deviations or count (percentage) for continuous and categorical variables, respectively.
Asymmetric v. Symmetric Coronal Uptake on SPECT/CT
Demographic, Spinopelvic Radiographic Parameters, and Pathologic Findings of Patients Stratified by Asymmetric v. Symmetric Coronal Uptake on SPECT/CT.
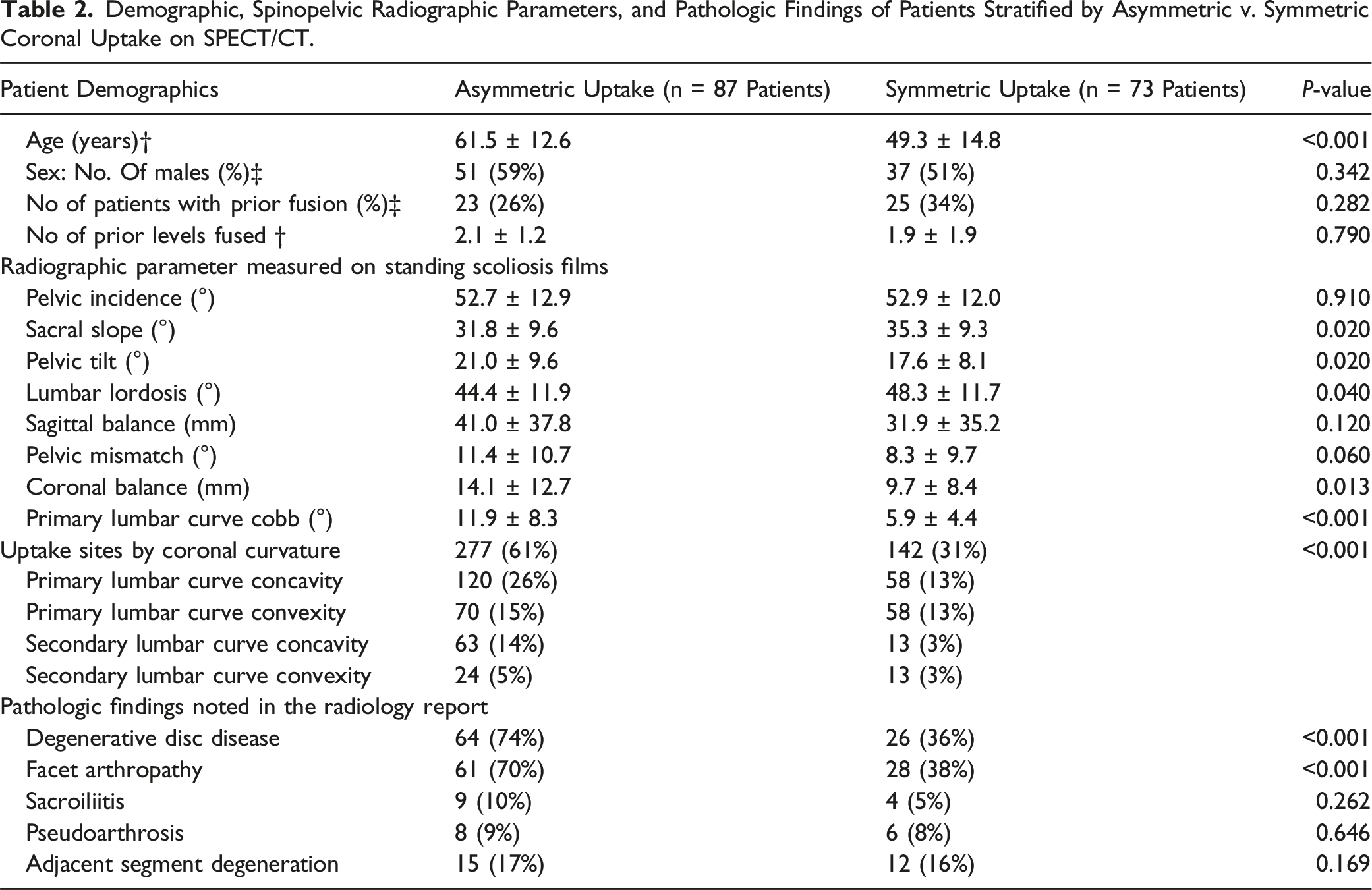
There were no statistically significant differences between the asymmetric and symmetric uptake cohorts with regards to pelvic incidence (52.7 ± 12.9° ± 52.9 ± 12.0°), sagittal balance (41.0 ± 37.8 mm vs 31.9 ± 35.2 mm), or spinopelvic mismatch (11.4 ± 10.7° v. 8.3 ± 9.7°) (P > 0.05). The asymmetric cohort had a smaller sacral slope (31.8 ± 9.6° vs 35.3 ± 9.3°) and lumbar lordosis (44.4 ± 11.9° vs 48.3 ± 11.7°), but greater pelvic tilt (21.0 ± 9.6° vs 17.6 ± 8.1°) than the symmetric cohort. The asymmetric cohort had significantly greater degree of coronal imbalance (14.1 ± 12.7 mm vs 9.7 ± 8.4 mm, P = 0.013) and coronal primary lumbar curve cobb angle (11.9 ± 8.3° vs 5.9 ± 4.4°, P < 0.001). The asymmetric cohort had significantly greater number of uptake sites than the symmetric cohort (277 [61%] vs 142 [31%], P < 0.001). The symmetric cohort had equal number of uptake sites on the concavity and convexity of the curve, but in the asymmetric cohort, the predominant uptake was observed on the concavity in 65 patients (74%) compared to 14 patients (16%) which had predominant convexity uptake (P < 0.001). The remaining (10%) had equal sites of uptake on the concavity and concavity.
Discussion
Although prior studies have investigated the role of SPECT/CT in the diagnosis and management of LBP, these studies have been limited in their ability to explore associations of uptake on SPECT/CT and patient specific spinopelvic alignment.29-31 Given the increasing focus of sagittal deformity correction for patients undergoing spine surgery, we had initially postulated that sites of uptake reflect biomechanical stress points associated with sagittal spinopelvic disequilibrium. Surprisingly, however we found that measures of coronal deformity were associated with asymmetric radiotracer uptake and may be sources of biomechanical stress leading to pain generation. Our results demonstrated that asymmetric coronal radiotracer uptake was associated with a greater degree of coronal lumbar segmental scoliosis and coronal imbalance in addition to increased incidence of radiographic DDD, and FA. Notably, increased uptake sites were predominantly observed on the concavity of the lumbar scoliosis within the intervertebral discs and facet joints. These findings support the use of SPECT/CT for patients with equivocal LBP as it provides additional, complementary information that traditional imaging modalities may not.
Surgical correction of sagittal misalignment has attracted increasing attention because of its association with negative quality of life (QOL) and increased disability. 32 Loss of sagittal balance is postulated as an etiology of LBP as patients must compensate for this misalignment to maintain an upright posture, putting greater strain on the muscles of the lower back. 33 Associations of coronal deformity and quality of life have been underreported in comparison to sagittal deformity. Nevertheless, emerging literature has demanded greater attention to coronal deformity and its correction.34,35 The results of this study suggest that these two deformities could be representing independent generators of LBP.
Spinal stability relies on the articulation of the facet joints and integrity of the intervertebral discs. In the lumbar spine, facet joints are oriented in the sagittal plane. With a coronal deformity, the curvature of the spine is oriented perpendicular to the lumbar facet alignment, which results in differential compressive and distracting stresses along the curvature. Compressive stresses occur on the concavity of the curve in the ipsilateral facet joints and discs. Asymmetric loads lead to progressive degeneration of the facet joints and intervertebral discs, which may create multi-segmental micro-instability that is sensed as back pain.36,37 We hypothesize that the body attempts to counteract these stresses via bone remodeling at compressive sites and sites of micro-instability. The active bone deposition is what is detected on SPECT/CT. We conjecture that the coronal deformity observed in the asymmetric cohort is a driver of greater facet arthropathy and degenerative disc disease in these patients.
Our results align with the review proposed by Aebi et al, which found LBP localized at the concavity the curve. 38 In our study, the asymmetric cohort had larger primary coronal lumbar cobb angles with uptake predominantly located on the concavity of the curves. In addition to the primary lumbar curvature, we defined an adjacent secondary coronal lumbar curve. The secondary curve was in the opposite direction of the primary lumbar curve and helped to reduce pelvic obliquity. This counter curvature primarily occurred between L4-S1, which withstand the greatest physiologic axial loads. In the secondary curvature, we also found increased uptake on the concavity of the curve.
The established classification systems of coronal deformity were proposed by the original works of Bao et al and Obeid et al.34,35 Bao identified global coronal balance exceeding 4 centimeters as a positive predictor for worsened outcomes and need for additional surgery. They further emphasized the importance of distinguishing between convex and concave coronal malignment, developing different surgical treatment paradigms for each. However, in our study, only 3 patients had global coronal balance exceeding 4 centimeters, prompting a more nuanced segmental measurement of coronal lumbar scoliosis. In the Obeid classification system, a primary thoracolumbar coronal curve was defined, but several modifiers for stiffness, lumbosacral junction mobility, and degeneration limit the clinical applicability of their treatment-oriented guidelines. Nevertheless, these studies were foundational in acknowledging a need for coronal deformity correction to prevent further coronal decompensation, implant failure, and decreased health related QOL.
Surgical arthrodesis for SPECT/CT uptake was previously reported for single level uptake in the SPINUS I study. 9 In this prospective study, patients with single level SPECT/CT positive lumbar DDD were offered posterior interbody fusion at the level of increased uptake. Fusions resulted in substantial clinical improvement, which persisted at 3-year follow up. The study called for evaluating the role of fusion procedures in patients with multi-level uptake on SPECT/CT. In patients with asymmetric multi-level uptake, our results suggest that coronal deformity may be an independent driver of low back pain. Asymmetric uptake on SPECT/CT may call for fusion with surgical procedures aimed at reducing the coronal deformity with asymmetric cage designs while simultaneously treating sagittal deformity. 39
Overall, our findings support the authors’ notion that the use of SPECT/CT enhances the diagnostic and decision-making capabilities when planning surgical intervention for patients with LBP. Precise localization of active degenerative sites obviates the need for repeated or invasive tests and enables targeted and individualized interventions. Delineating patterns of increased uptake on SPECT/CT may better characterize etiologies of LBP and improve surgical outcomes.
Limitations
The authors recognize several inherent limitations in the present study. The retrospective and exploratory nature of our study design prevents generalizability of our findings and lacks granularity for a more nuanced analysis of each patient’s diagnostic and treatment algorithm. Furthermore, we acknowledge a referral bias, as the spine surgeon selected which patients may benefit from undergoing SPECT/CT imaging. Additionally, radiologist reports of SPECT/CT uptake were interpreted by several nuclear medicine radiologists, which may have led to subjective variation in the interpretation of increased tracer uptake. Moreover, the SPECT/CT images were collected with standardized acquisition protocols but with different machines and different radiology technicians over several institutional facilities. Radiotracer uptake values are variable based on attenuation, which is dependent on the patient’s anatomy and renal function, as well as the pharmaceutical dose, time from administration to image capture, and gamma camera resolution. This is why we favored relative uptake for each individual patient over quantifying the standard uptake value, which would otherwise have introduced biases comparing against imaging obtained from different machines and different radiotracer doses. While a more systematic, quantitative SPECT/CT protocol is achievable, it is more expensive, lengthier, and requires greater technical expertise. Therefore, in this experimental design, standard uptake value units were not measured. Lastly, this study did not explore correlations of increased radiotracer uptake with clinical outcomes such as need for subsequent surgical treatment or patient reported pain measures such as visual analog scale scores.
Conclusions
Hybrid SPECT/CT is an emerging and valuable diagnostic tool in the workup and clinical management of LBP, which helps identify anatomic pain generating sites. Although often overlooked and combined with sagittal deformity, coronal deformity is a distinct entity that may contribute to pain generation with bony remodeling from heightened mechanical stresses. Future studies are warranted to better characterize the clinical applications of these findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.