
Abstract
Study Design
Retrospective cohort study.
Objective
Osteoporotic vertebral compression fractures (VCFs) are prevalent among the elderly population, and Balloon kyphoplasty (BKP) is a minimally invasive solution for these. However, Polymethylmethacrylate (PMMA) leakage is a significant complication with potentially severe consequences. This study compares the safety and efficacy of manual balloon tamp system (MTS) and hydraulic Polymethylmethacrylate pressure delivery system (HPDS) in BKP.
Methods
A retrospective study involving 160 patients, comparing MTS (2008-2014) and HPDS (2016-2020) cohorts, assessed PMMA leakage, radiation exposure, and surgery duration.
Results
PMMA leakage occurred in 52.8% of MTS and 62.5% of HPDS cases. Intradiscal leakage was the most common pattern in both groups. Multivariate logistic regression revealed that multilevel BKP and HPDS were associated with higher PMMA leakage rates. Radiation exposure was significantly lower with HPDS, while surgery duration was shorter.
Discussion
This study provides novel insights into PMMA leakage and radiation exposure in BKP. HPDS was associated with a higher PMMA leakage rate. HPDS, however, offers advantages in terms of reduced radiation exposure and shorter surgery duration. Multilevel BKP also increased the risk of leakage. Further investigation is needed to better understand the impact of HPDS on PMMA leakage.
Conclusion
This study underscores that while HPDS offers advantages regarding radiation exposure and surgery duration, it is associated with a higher PMMA leakage rate.
Introduction
Osteoporotic vertebral compression fractures (VCFs) represent a significant clinical challenge, impacting a substantial portion of the elderly population worldwide. 1 These fractures not only contribute to chronic pain and reduced quality of life but also pose a considerable burden on health care systems.2,3 In recent decades, balloon kyphoplasty (BKP) has emerged as a minimally invasive surgical intervention to alleviate pain and restore vertebral body height in patients with VCFs. 4 This procedure involves the percutaneous insertion of a balloon into the vertebral body, followed by the injection of polymethylmethacrylate (PMMA) to stabilize the fracture. While balloon kyphoplasty (BKP) has demonstrated efficacy in reducing pain and restoring vertebral body height, it is not without complications.
Among the most notable complications of BKP is the leakage of PMMA. The clinical implications of PMMA leakage in BKP are multifaceted. While many cases of leakage are clinically asymptomatic, there is a potential for serious complications that can negate the benefits of the procedure. PMMA leakage into the surrounding vascular and spinal structures can lead to severe clinical implications, ranging from asymptomatic incidents to critical outcomes such as pulmonary embolism5,6 or nerve compression.7,8 The incidence of PMMA leakage varies widely across studies,9–14 with some reporting rates as high as 74%.
PMMA leaks have been studied and classified as intradiscal, epidural, foraminal, perivertebral venous and paravertebral by some studies. 9 Other studies emphasized the vascular involvement of the PMMA leak, 15 such as segmental or paravertebral veins, which drain into the azygos, hemiazygos, and accessory hemiazygos veins or directly into the inferior vena cava, leading to pulmonary cement embolism. Other studies used other PMMA leakage anatomic classifications: basivertebral vein, segmental vertebral vein, anterior external vertebral venous plexus, radicular vein, posterior external vertebral venous plexus, and azygos vein. 16
Several preventive measures were described to reduce the percentage of PMMA leakage. Albers et al. 17 proposed vertebral body lavage to reduce PMMA leakage by reducing vertebral bone marrow, with an odds ratio of 3.49. Limited PMMA volume injected per session18–20 and high PMMA viscosity during injection21–23 were also studied. Sequential PMMA injection was also described as reducing the relative risk of PMMA leakage. 22
Balloon kyphoplasty evolved; initially, PMMA was injected manually using plungers (MTS, manual tamp system), followed by hydraulic Polymethylmethacrylate pressure delivery systems (HPDS). The potential benefits of the HPDS include higher volume injection, a more gradual PMMA injection, the injection of a higher viscosity PMMA with less effort, the reduction of the need for the fluoroscopically assisted sequential placement of tamps in MTS, and the option of PMMA injection through extension tubing, thus reducing surgeon’s radiation exposure. Comparisons of HPDS and MTS were made, showing the benefits of the HPDS.21,24 Although HPDS has been used for several years, there is some deterrence of use due to fear of a higher percentage of PMMA leakage. The studies assessing HPDS vs MTS did not elaborate on this issue, underscoring the need for a deeper understanding of the implication of the PMMA delivery system on leakage and its significance.
In our Center, we used MTS for BKP from 2008 to 2014, and in 2015, we started transitioning to an HPDS. Since 2016, we have been using HPDS alone for BKPs. This study compares the safety of a manual balloon tamp system vs a hydraulic Polymethylmethacrylate pressure delivery system, i.e., PMMA leakage and radiation exposure. Our study hypothesis was that there is no difference in PMMA leakage between PMMA delivery systems, while HPDS allows for a shorter surgery time and less radiation exposure.
Methods
Our institutional review board approved the study and informed consent was not required from patients (WOMC-0020-24).
A retrospective study compared a cohort of patients who underwent BKP in 2008-2014 using MTS to those who underwent BKP in 2016-2020 using HPDS. Patients who underwent BKP in 2015 were excluded since the PMMA delivery system was either MTS or HPDS, and the distinction between them is unavailable. Additional exclusion criteria included patients who lacked intraoperative and postoperative imaging studies. Two fellowship-trained spine surgeons performed surgeries using the same manufacturer’s MTS and HPDS BKP systems.
The cohort’s electronic medical records were evaluated for sex, age, BMI, fracture morphology (the involved endplate, vertebral height loss, fractured level), and the need for further surgery or pain clinic procedures to address post-surgical complications due to PMMA leakage. As available, patients’ post-surgical imaging studies were evaluated for PMMA leakage on fluoroscopy, x-rays, or CT scans. A spine surgeon classified PMMA leakage as intradiscal, epidural, external vertebral venous plexus, ascending lumbar vein, vertebral segmental vein, continuous anterior perivertebral, perivertebral and foraminal. In multilevel fractures, a PMMA leak was considered positive even when the leak involved a single vertebra. PMMA leakage volume was not measured; only the PMMA leakage location was measured.
Study data statistical analyses were carried out using SPSS 23.0 and G*power statistical software. Numerical variable
differences were calculated using the student's t-test. Categorical parameters were assessed using the Chi-square test or Fisher exact tests. Multivariate logistic regression was used to assess the correlation between fracture level, PMMA delivery system and PMMA leakage.
Results
One hundred and sixty patients were included in this study; 72 underwent BKP during 2008-2014 using a manual balloon tamp system, and 88 under BKP during 2016-2020 using a Hydraulic Polymethylmethacrylate pressure delivery system. The cohort’s average age was 78.7 ± 7.5, and 76.1% were females. Fractured vertebrae distribution was mainly in the thoracolumbar junction in both cohorts (Figure 1). Some patients had more than a single vertebral fracture (Table 1), but 80.6% of patients had a single fractured vertebra. The fracture level distribution of both cohorts was statistically similar (P = .09), as well as multilevel fractures (P = .392). Fractured Vertebral level distribution (%) in each cohort. MTS - manual balloon tamp system; HPDS - hydraulic Polymethylmethacrylate pressure delivery system. Number of Fractures Treated at a Single Procedure. MTS - manual balloon tamp system. HPDS - hydraulic Polymethylmethacrylate pressure delivery system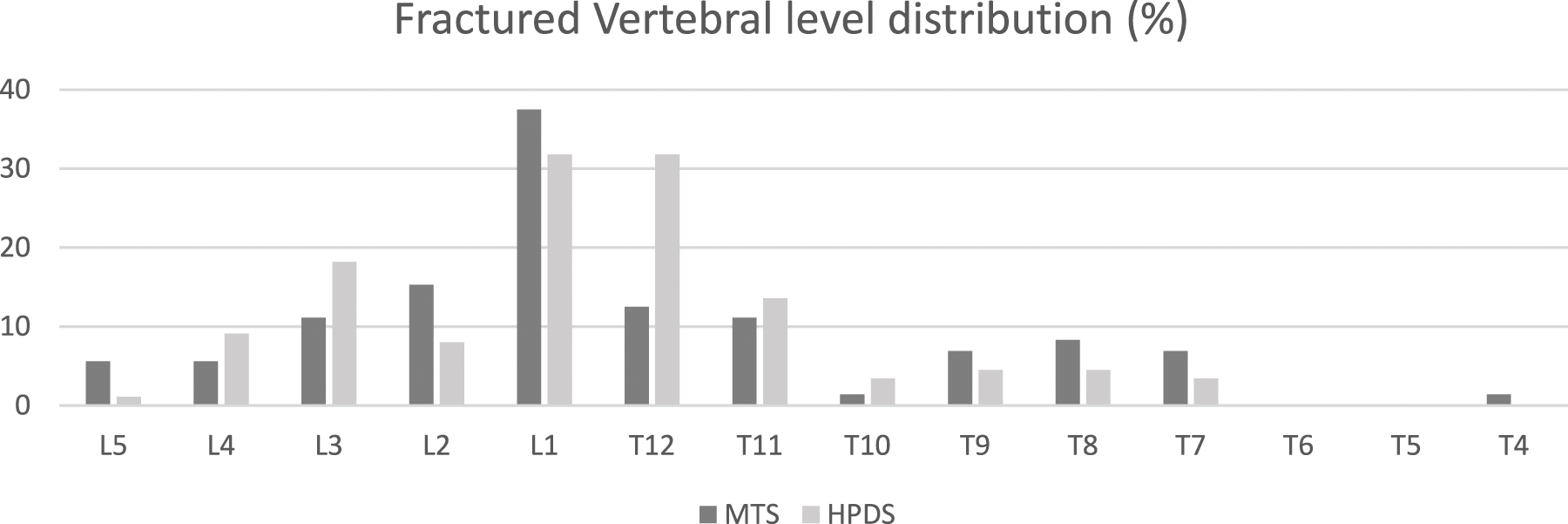

PMMA Anatomical Leakage Patterns.
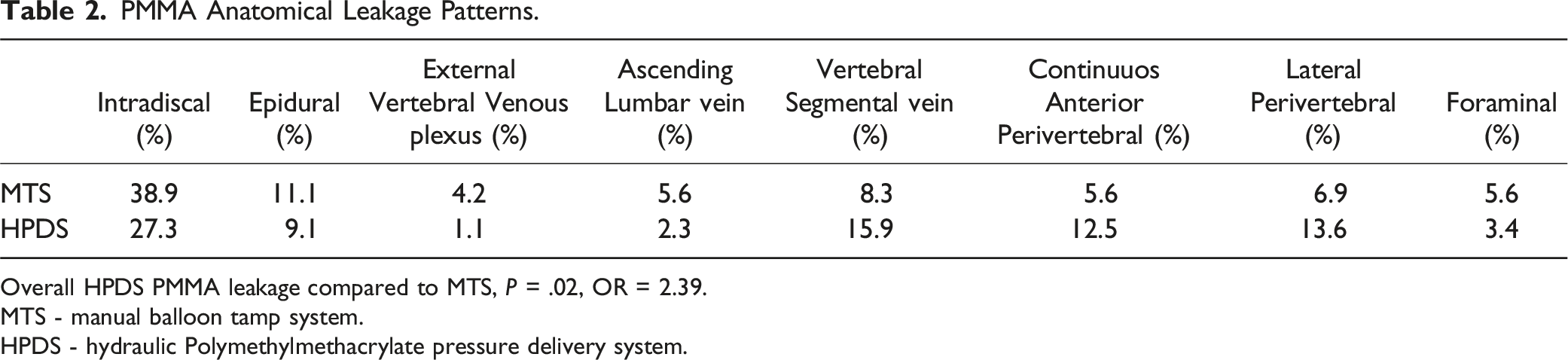
Overall HPDS PMMA leakage compared to MTS, P = .02, OR = 2.39.
MTS - manual balloon tamp system.
HPDS - hydraulic Polymethylmethacrylate pressure delivery system.
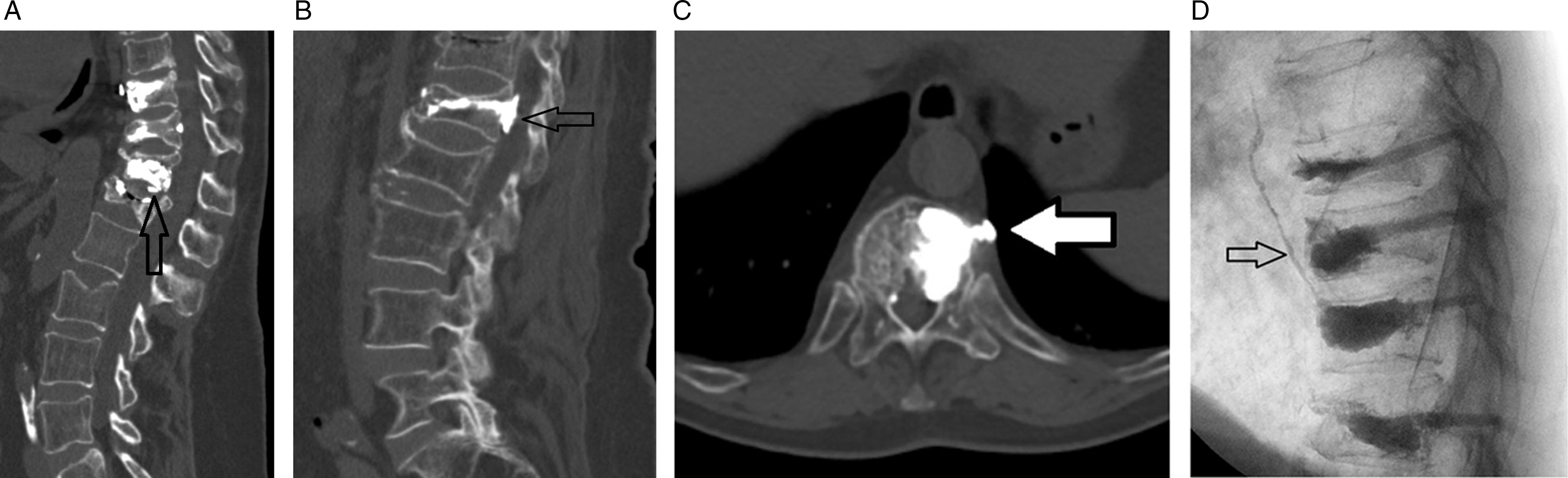
Examples of PMMA leakage. (a) Intradiscal PMMA leakage. (b) Epidural PMMA leakage. (c) Anterior peri-vertebral continuous PMMA leakage. (d) Ascending lumbar vein PMMA leakage.
PMMA Leakage Patterns.

MTS - manual balloon tamp system.
HPDS - hydraulic Polymethylmethacrylate pressure delivery system.
When performing a Chi-square test on PMMA leakage for a single-level BKP using MTS and HPDS, the P-value was .162, meaning that leakage rates were statistically similar. The same was valid for combining all fracture levels, P = .215. However, when performing a multivariate logistic regression on both cohorts for fracture level, number of fractured vertebrae, age, sex, and days from fracture to surgery, we found that BKP for more than a single vertebral fracture is more prone to PMMA leakage, P = .03 and an Odds Ratio of 2.79. The same was true for higher PMMA leakage rate with PHDS compared to MTS, P = .02 and Odds Ratio of 2.39. We found no statistical significance in relating fractured vertebral levels to the percentage of PMMA leaks.
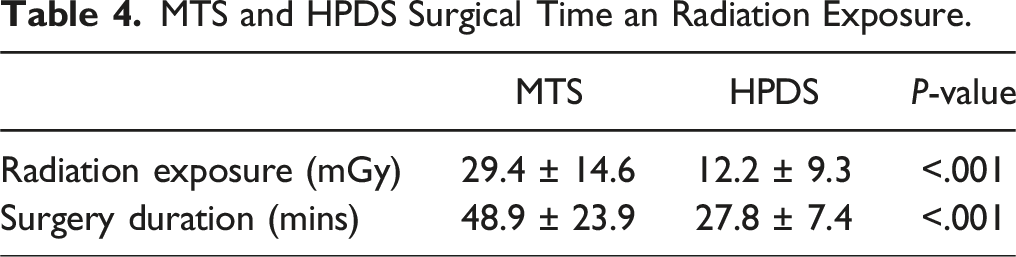
MTS and HPDS Surgical Time an Radiation Exposure.
When evaluating the need for revision surgery or pain clinic intervention, such as selective nerve root block, following BKP, MTS and HPDS, none of the subjects in either cohort required such an intervention. All PMMA leaks in our cohorts were asymptomatic regarding neurological compromise, radiculopathy or claudication.
Statistical power analysis using the goodness-of-fit tests with a medium effect size of .3, an α probability of .05, one degree of freedom and power (1-β error probability) of .9 requires a sample size of 117 patients; our study included 160 patients, thus the results obtained are significant.
Discussion
The current study provides valuable insights into the safety and complications associated with balloon kyphoplasty, mainly focusing on polymethylmethacrylate leakage and radiation exposure during surgery. The comparison between a manual balloon tamp system (MTS) and a hydraulic PMMA pressure delivery system (HPDS) in the treatment of osteoporotic vertebral compression fractures (VCFs) offers a comprehensive understanding of the evolution and optimization of this minimally invasive procedure. This comparison is novel; no prior study has compared PMMA manual and hydraulic delivery systems.
PMMA leakage, a significant concern in BKP, was relatively high in our study, 58.1% overall. The PMMA leak rate was higher in the HPDS cohort than in the MTS cohort (OR = 2.39). This finding contradicts the initial assumption that advanced technology would reduce or not change complication rates. It underscores the complexity of PMMA handling and the need for precision in its application. Another study’s finding is that a higher rate of PMMA leakage is associated with multilevel BKPs, as indicated by the odds ratio of 2.79, emphasizing the importance of surgical strategy and patient selection for PMMA leakage studies, particularly in cases involving multiple vertebral fractures.
The classification of PMMA leaks into various types, such as intradiscal, epidural, and venous, aligns with previous studies’ findings9,15,16 and highlights this complication’s multifaceted nature. The relatively high PMMA leakage rate with no clinical complications reassures that stopping PMMA injection upon leakage identification reduces clinically significant sequela. While our study showed that most PMMA leaks were asymptomatic, the potential for severe complications like pulmonary embolism and nerve compression remains a critical consideration. This highlights the necessity of intraoperative vigilance to minimize the risk of leakage and its potential consequences.
The introduction of HPDS in BKP, despite its association with higher leakage rates, showed notable benefits in terms of reduced radiation exposure and shorter surgery duration, probably due to reducing the need for repositioning PMMA plungers following refill. This finding is significant given the concerns regarding radiation exposure to patients and surgeons in interventional radiology procedures. The efficiency and ease of use of HPDS, as demonstrated by the reduced surgery time, may contribute to its preference in clinical practice, although its impact on PMMA leakage warrants further investigation.
Limitations of this study include its retrospective nature and the exclusion of patients from 2015 due to the transition period between MTS and HPDS. This exclusion potentially introduces a selection bias, as it omits a subset of patients who might have provided additional insights into the comparative effectiveness and complications of the two systems during their concurrent use. Lastly, the study did not account for potential confounding factors such as the severity of osteoporosis, the presence of comorbidities, or variations in surgical technique, all of which could influence the incidence of PMMA leakage and other complications. This study evaluates only the immediate surgical implications of PMMA leakage and does not evaluate the long-term effect of MTS and HDPS. A more nuanced understanding of these factors could enhance the interpretation of the results and their applicability to patient care. Future studies should focus on prospective data collection, including a more diverse patient population, to comprehensively assess the long-term outcomes and complications associated with different PMMA delivery systems in BKP.
In conclusion, while HPDS in BKP offers advantages regarding reduced radiation exposure and surgery duration, it is associated with a higher PMMA leakage rate than MTS. Surgeons considering technique change may find this study valuable regarding advantages and pitfalls. Multilevel BKP doubles the rate of PMMA leakage. Our results underscore the importance of careful patient selection, particularly in multilevel fracture cases, and highlight the need for continued innovation and refinement in BKP techniques to optimize patient outcomes while minimizing complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Edith Wolfson Medical Center IRB committee gave IRB approval, Holon, Israel, affiliated with The Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.