
Abstract
Study Design
Cross sectional comparative study.
Objectives
The current study aims to explore the calcification potential (BMP2 expression) of intervertebral discs and its association with the presence of vertebral endplate defects visible on MRI.
Methods
Forty-seven herniated lumbar disc samples obtained from patients aged 20-76 (31 M/16F) undergoing surgery. Five-µm thin sections were stained with H&E in order to assign a histological degeneration score (HDS) from 0-15 on the basis of cell density (0-5), structural alterations (0-4), granular changes (0-3) and mucus degeneration (0-3). Sections were immuno-stained with anti BMP-2 antibodies to observe the calcification potential in these discs. In addition, pre-operativeT2-T1 W MRI images of the lumbar spine were analyzed for the presence and type (typical or atypical) of vertebral endplate defects, grade of disc degeneration (Pfirrmann grade I-V), presence of high intensity zones (HIZ), and Modic changes at the operated level.
Results
Vertebral endplate defects, Modic changes & HIZ were observed in 81%, 29% and 21% of patients respectively. Mean HDS & BMP-2 expression was 9 ± 2 and mean 71 ± 36 spots/mm2 respectively. Discs with adjacent vertebral endplate defects showed increased cell density (P = .004), mucus degeneration (P = .002), HDS (P = .01) and BMP-2 expression (P = .01). Discs with HIZ also had increased HDS, but significance was seen with increased BMP2 expression (P = .006). HDS showed a positive correlation with BMP 2 expression (r = .30, P = .04).
Conclusion
These findings suggest that the altered mechanical environment of discs is strongly associated with BMP-2 expression which is an important marker of intervertebral disc calcification.
Introduction
Intervertebral disc calcification is one of the key degenerative features that has recently been documented as the potential source of discogenic back pain.1,2 Calcified disc is not a frequent finding in clinical settings probably due to the limitations of the imaging diagnostics,2-4 however, recent report suggests that incidence of calcified herniated discs in lumbar region is increasing and has younger trends. 5 The microscopic and micro-CT evaluation of the herniated and degenerated discs obtained from surgical patients revealed its presence in 54 to 81% of the samples along with the raised expression of osteogenic markers indicating osteogenic potential of the degenerative discs.6-8 The calcified herniated disc tends to harden posing a great challenge to surgeons and there is always a high risk of nerve root injury during surgery. 9
The probable mechanism of pain in calcified discs is not very clear but reports suggest that patients with calcified discs usually have chronic complaints of variable degree of back and leg pain. 10 It is assumed that inflammation associated with calcification might be a factor leading to increased sensitization of nerve endings and neo-innervation potentially causing discogenic back pain. 11
The etiology of disc calcification is uncertain, whether it is a cause or consequence of disc degeneration is not known. Nevertheless, presence of disc calcification in scoliotic patients raises the possibility of its association with abnormal mechanical loading leading to stress alterations. The altered mechanics of the intervertebral discs reduces the production of proteoglycans and hydration of the discs surging the local concentration of calcium and Pi ions which might be a causative factor in more pronounced calcification on the side of the concavity in scoliotic disc.4,12,13 The occurrence of mineralized spots close to the fissures and tears further strengthens the notion as the presence of radial and circumferential tears in the annulus are associated with inter-laminar shear stresses 14 and presence of rim lesions, circumferential tears and radial lesions are said to have specific and sensitive effects on disc biomechanics. 15
Vertebral endplates play a crucial role in the distribution of intradiscal stress, various mechanical studies have noted that even minor endplate damage may lead to ‘‘high stress gradients’’ within the nucleus and discs that precipitate disc degeneration and failure,16,17 therefore, it can be a strong contributing factor in disc calcification. Since the pathogenesis and mechanisms of disc calcification is still not very clear, it is assumed that it can be linked with abnormal mechanics of the spine or inflammation.
Keeping these things in mind the current study was planned. The basic purpose was to develop the relationship between intervertebral disc calcification with the vertebral endplate phenotype on MRI findings. Since any defect in the vertebral endplate may alter the mechanics and may predispose to calcification. We hypothesize that in patients with vertebral endplate defects there will be increased tendency of discs to calcify.
Methods
Study Population
The study was approved by the Ethical Committee of the relevant institute and informed consent was taken from the patients prior to surgery for collection of data and sample post-surgery and its use for the research purpose. Lumbar disc samples of adult male and female patients having confirmed diagnosis of herniated discs on lumbosacral spine MRI and undergoing discectomy (disc excision) in our hospital were included in the study. Samples with congenital spine defect, visible spine anomaly like scoliosis, diseases with diverse etiology in which intervertebral disc calcification can occur like metabolic bone disease, congenital bone malformation, gout, renal dysfunction, or hypercalcemia, etc. were excluded. The sample size was calculated using the SRS method keeping 95% confidence interval and margin of error 5%.
Demographic characteristics of each patient were recorded in detail including age, sex, and duration of low back pain, body mass index (BMI) and history of smoking. Moreover, occupational information, including various work types, manual handling of heavy objects at work, and hours of deskwork per day, was further investigated.
Visual Analog Scale (VAS) scores was recorded by using professional numerical rating scales. VAS scores (0, no pain, to 100, worst pain) were applied for evaluating back pain. The VAS scale comprised of a 100-mm horizontal line, one end having 0 was marked with the words “no pain” and at the other end having 100 was marked with the words “worst pain imaginable.” The patient was asked to mark the line at the point that best represented the intensity of his or her pain. The VAS numeric value was obtained in millimeters at the point marked by the patient on the scale. 18
MRI Evaluation and Assessment of Parameters
T1&T2 weighted lumbar sagittal MRI of all the patients were assessed in Radi-Ant-Dicom software. The affected level was assessed for the disc degeneration grades using Pfirrmann grading system from grade I to grade V. 19
Vertebral endplates were assessed for the presence and absence of endplate defects. Any break in the endplates were recorded as presence of endplate defect. The number and side of the vertebral endplate defects whether cranial, caudal or both were also noted. Endplate defects were also categorized as typical & atypical Schmorl nodes. 20 Any change in the signal intensity (hypo or hyper) of vertebral endplate on T1 & T2 W MRI were recorded as Modic changes. 21 Their presence and absence were noted. High intensity signal changes were also assessed in the intervertebral discs and their presence or absence were recorded as high intensity zone (HIZ). 22 HIZ present anterior or at posterior aspect were noted and recorded. Thirty-five radiographs were randomly selected and assessed twice by the observer (UZ) to determine the intra-observer reliability, while inter-observer reliability was determined on 20 radiographs by another independent observer (MSI).
Histological and Immunohistochemical Evaluation
Tissue samples obtained were fixed in 10% formalin, they were processed, and paraffin embedded blocks were sectioned and stained with H&E Alcian blue PAS, Alizarin Red and for anti-BMP 2 for immunohistochemistry.
Histological degeneration scoring (HDS) 23 based on cell density, presence of tears and fissures, granular changes and mucus degeneration was done from 0-15. Inflammation was also scored based on the presence of inflammatory cells on an ordinal scale from 0-3 from no inflammation to mild, moderate and severe inflammation. 24 Presence & absence of calcification was also noted on Alizarin red stained sections. All slides were assessed twice by the observer (SI) to determine the intra-observer reliability, while inter-observer reliability was determined on 25 slides by another independent observer (UZ).
BMP-2 spots were analyzed and quantified/mm2 on immunohistochemical stained sections.
Statistical Analyses
The data has been entered and analyzed using SPSS 21.0. Mean and SD were used for numeric variables (Age, HDS, Pffirrmann score etc.). Means between two groups were compared using Independent Sample t test, whereas mean between three groups were compared using One Way ANOVA with Post Hoc Tukey Test. Correlation be-tween continuous variables was performed using Pearson’s Product correlation. For inter- and intra-observer reliability testing of imaging and histological parameters, the strength was noted based on kappa testing: excellent (k > .90), good (k > .80), fair (k > 70), and poor (k < .60). P < .05 was considered statistically significant.
Results and Observations
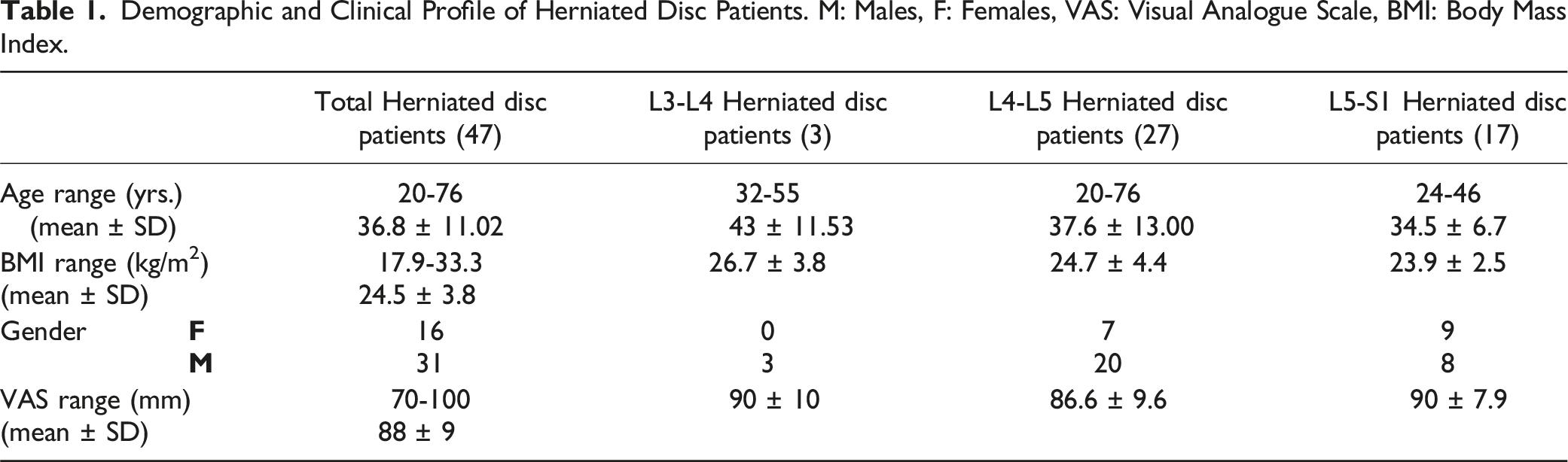
Patients Clinical and Demographic Profile
Demographic and Clinical Profile of Herniated Disc Patients. M: Males, F: Females, VAS: Visual Analogue Scale, BMI: Body Mass Index.
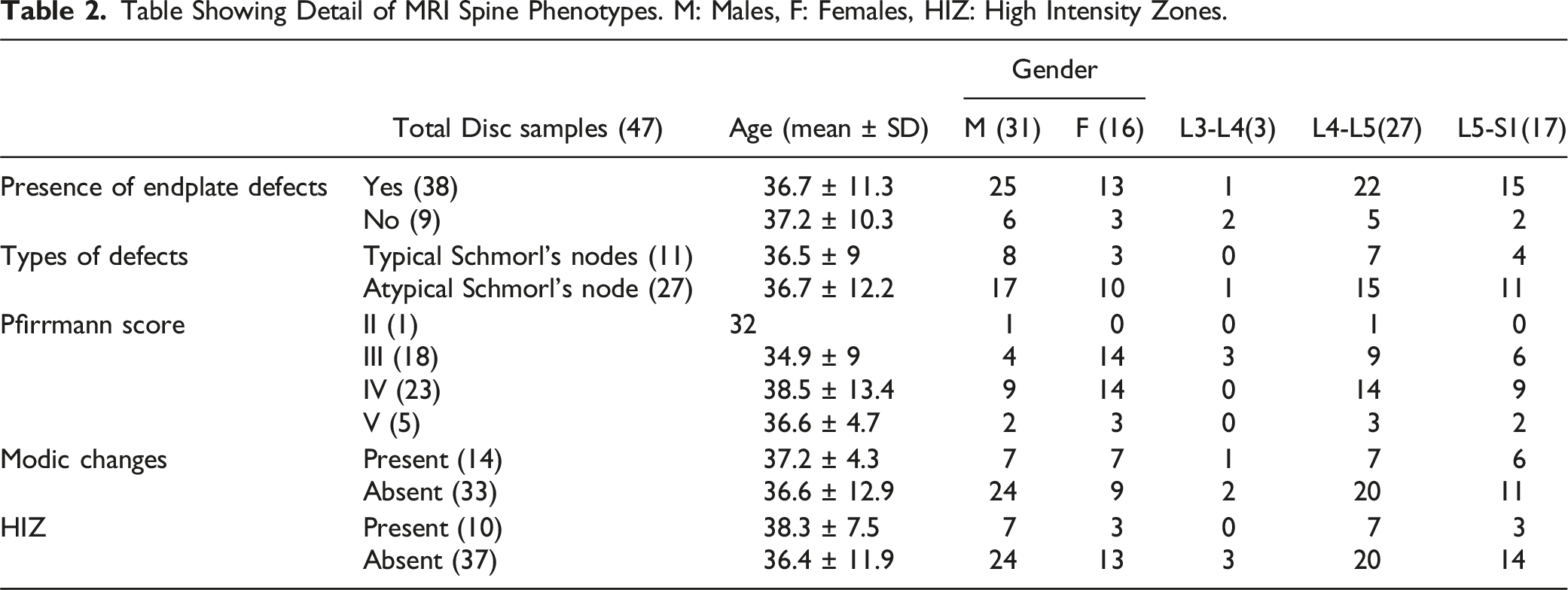
MRI Findings
Table Showing Detail of MRI Spine Phenotypes. M: Males, F: Females, HIZ: High Intensity Zones.
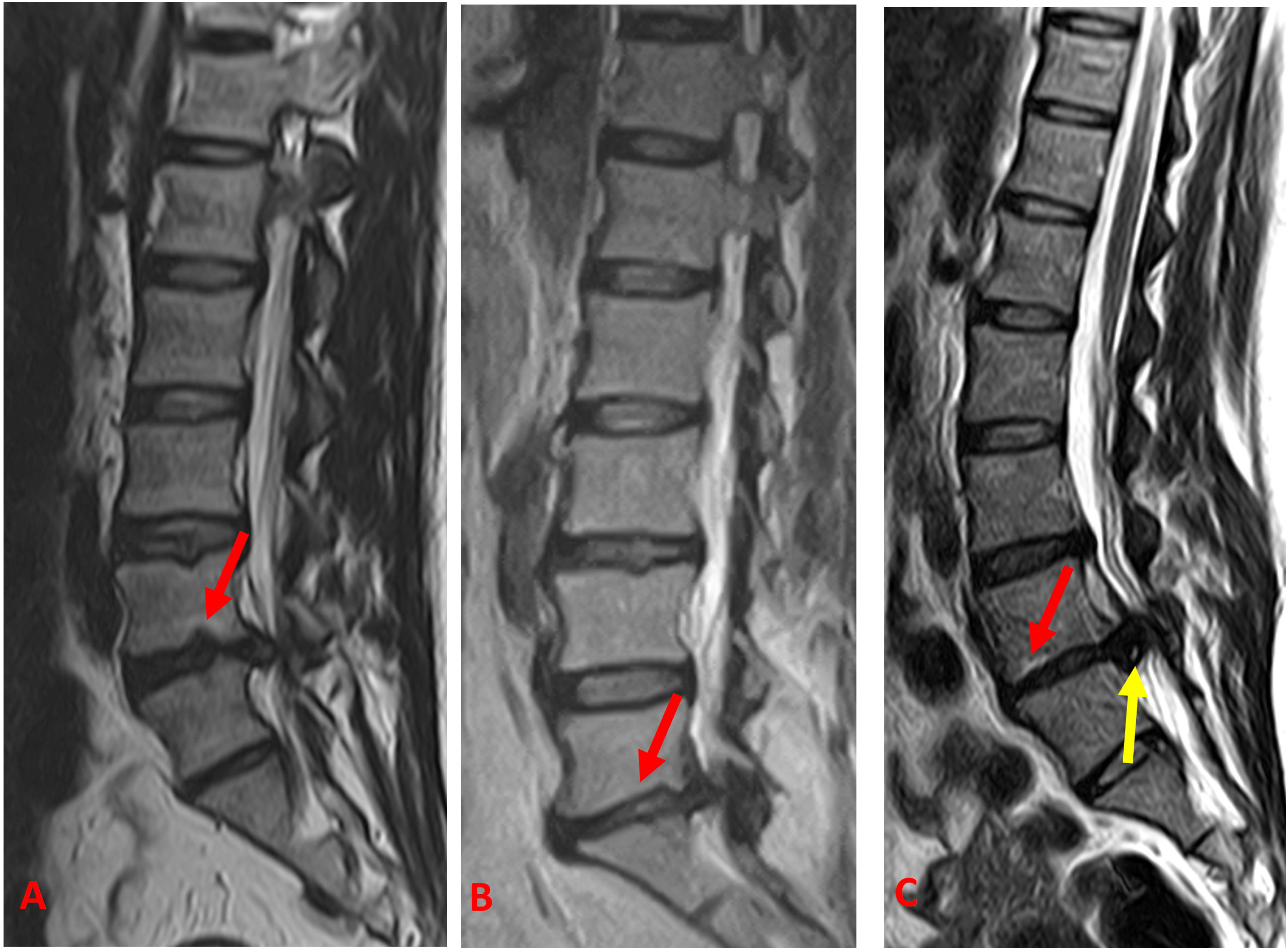
Lumbar sagittal T2W MRI of (A) a 43-year-old male showing typical Schmorls node (red arrow) (B) 45-year-old female with atypical Schmorls node (red arrow) and of (C) a 38-year-old female showing Modic changes (red arrow) and high intensity zone (HIZ) (yellow arrow) at the affected levels.
Age, gender, BMI, spinal level, VAS, smoking status, and occupation of the subjects did not show any significant difference with presence, type and side of vertebral endplate defects, Pfirrmann grading, Modic changes and HIZ.
Histological and Immunohistochemical Findings
Density of cells were seen to be increased in many samples, but the most common degenerative feature was cell cluster formation. These clusters were accumulation of chondrocytes from 4 up to 25 cells. Structural alterations in the form of fissures and tears were observed in the tissue sections. Granular changes were observed as eosinophilic-staining amorphous granules while mucus degeneration was recognized on the basis of dark blue stained oval or irregular areas (Figure 2). Based on these features, histological degeneration scores were assessed and found to be in the range of 5-12 (mean ± SD; 8.5 ± 1.9). Age, gender, spinal level, VAS, smoking status, and occupation did not show any significant effect on histological degeneration scores (Table 3). H&E-stained images of intervertebral surgical disc tissue showing (A) Presence of variable sized cell clusters (yellow arrows) (B) Structural alterations with granular changes (black arrows). (C) inflammatory cells and small blood vessels (black arrows) Scale bar 100 µm. Histological Evaluation Details of all Surgical Samples. M: Males, F: Females, HDS: Histological Degeneration Scores.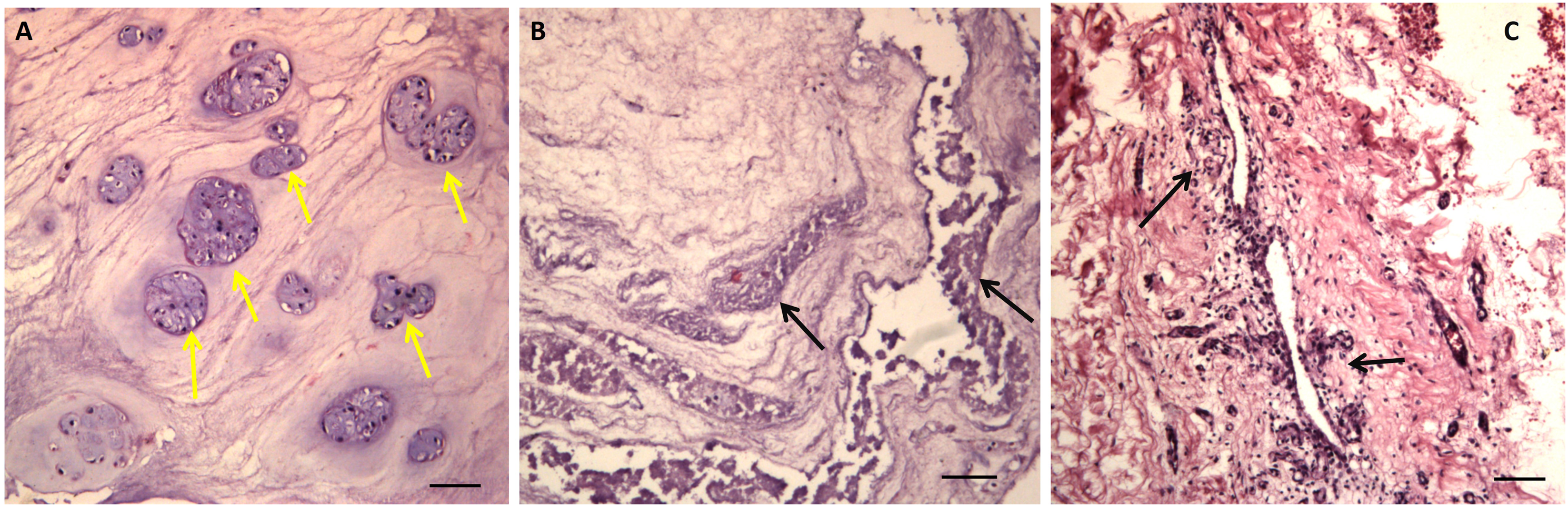
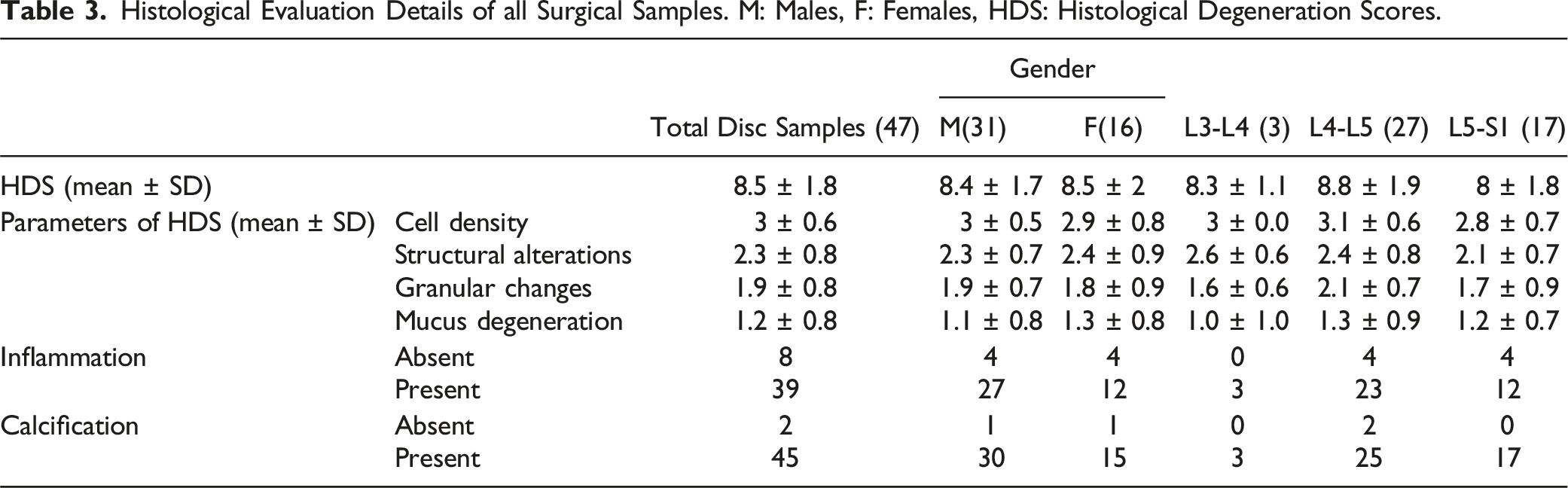
Inflammation was found in almost 83% of the samples. It was scored on an ordinal scale of 0-3 from none to severe. In almost 17% of the samples no inflammatory cells were evident, 49% of the samples with mild inflammation, 25.5% had moderate inflammation and 8.5% showed severe inflammation (Figure 2). There was not any significant effect of age, gender, spinal level, VAS, smoking status and occupation on presence and absence and scores of inflammations (Table 3).
Alizarin red staining showed calcified spots in almost 96% of the samples (Table 3) while all the samples showed positive BMP-2 staining for calcification. Range of BMP-2 spots/mm2 was from 22.4 to 222.4 with mean ± SD; 71.4 ± 36.3 spots/mm2. Calcification discerned, as brown spots were present in nucleus pulposus, inner and outer annulus (Figure 3). The expression was seen to be highly increased in the region of inflammation. Immunohistochemical expression of BMP-2 visible as brown spots (red arrows) in the intervertebral disc tissue (A) near inflammatory infiltrate and (B) in the inner annulus. Scale bar 100 µm.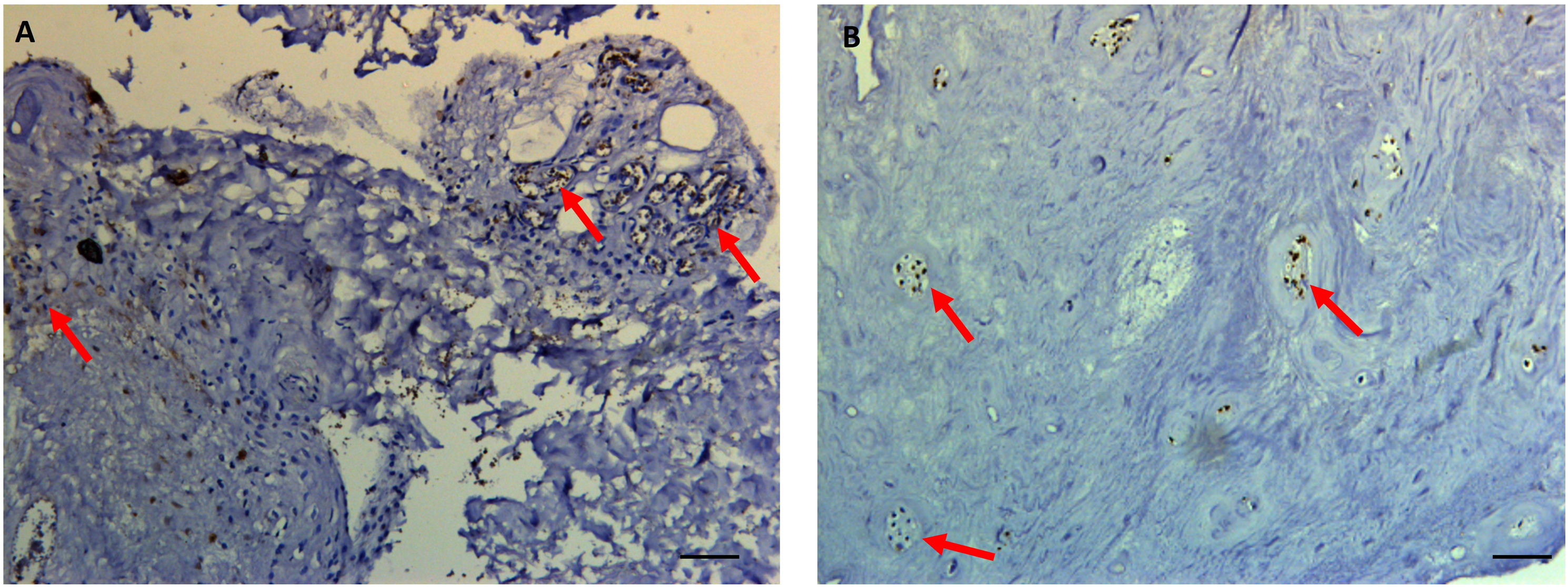
Inter & intra observer agreement for various histological parameters were found good to excellent with kappa value ranged from .83 to .95.
Age had a positive correlation with BMP-2 expression with borderline significance (r = .27, P = .06) while gender, spinal level and BMI did not have any impact on calcification expression.
Association of MRI and Histological Parameters
Discs with adjacent endplate defects showed increased cell density (P = .004), mucus degeneration (P = .002) and HDS (P = .01). Type and side of defects did not have any significant effect on any parameter of HDS, HDS and inflammation. Inflammation scores were increased in the discs with adjacent VEP defects, but significance was not seen. No significance was achieved between Modic changes and any parameter of HDS. Inflammation was increased with Modic changes with borderline significance (P = .09). Discs with HIZ also had increased structural alterations, granular changes, mucus degeneration, HDS and inflammation but significance was not seen. Mean HDS increased with increasing grades of Pfirrmann though statistically significant difference was not obtained. Pfirrmann grades were highly significantly increased in specimens with VEP defects (P < .001) and Modic changes (P = .03).
Association of BMP-2 with MRI and Histological Parameters
Showing the Association of MRI Parameters and BMP-2.
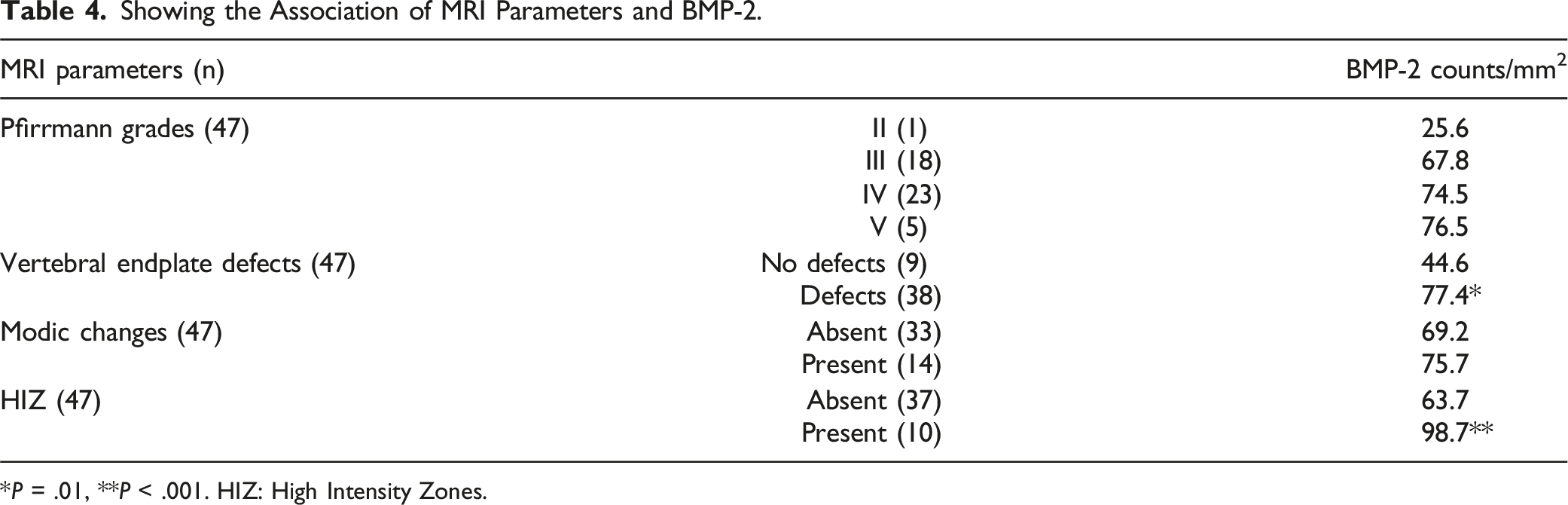
*P = .01, **P < .001. HIZ: High Intensity Zones.
A significant relationship of cell density with increased expression of calcification (P = .03) was observed. Pearson correlation showed positive correlation between HDS and calcification expression (r = .29, P = .04) (Figure 4). The samples with inflammation showed significantly higher BMP-2 expression as compared to those without inflammation (P = .02). Graph showing significant positive correlation between histological degeneration scores and BMP 2.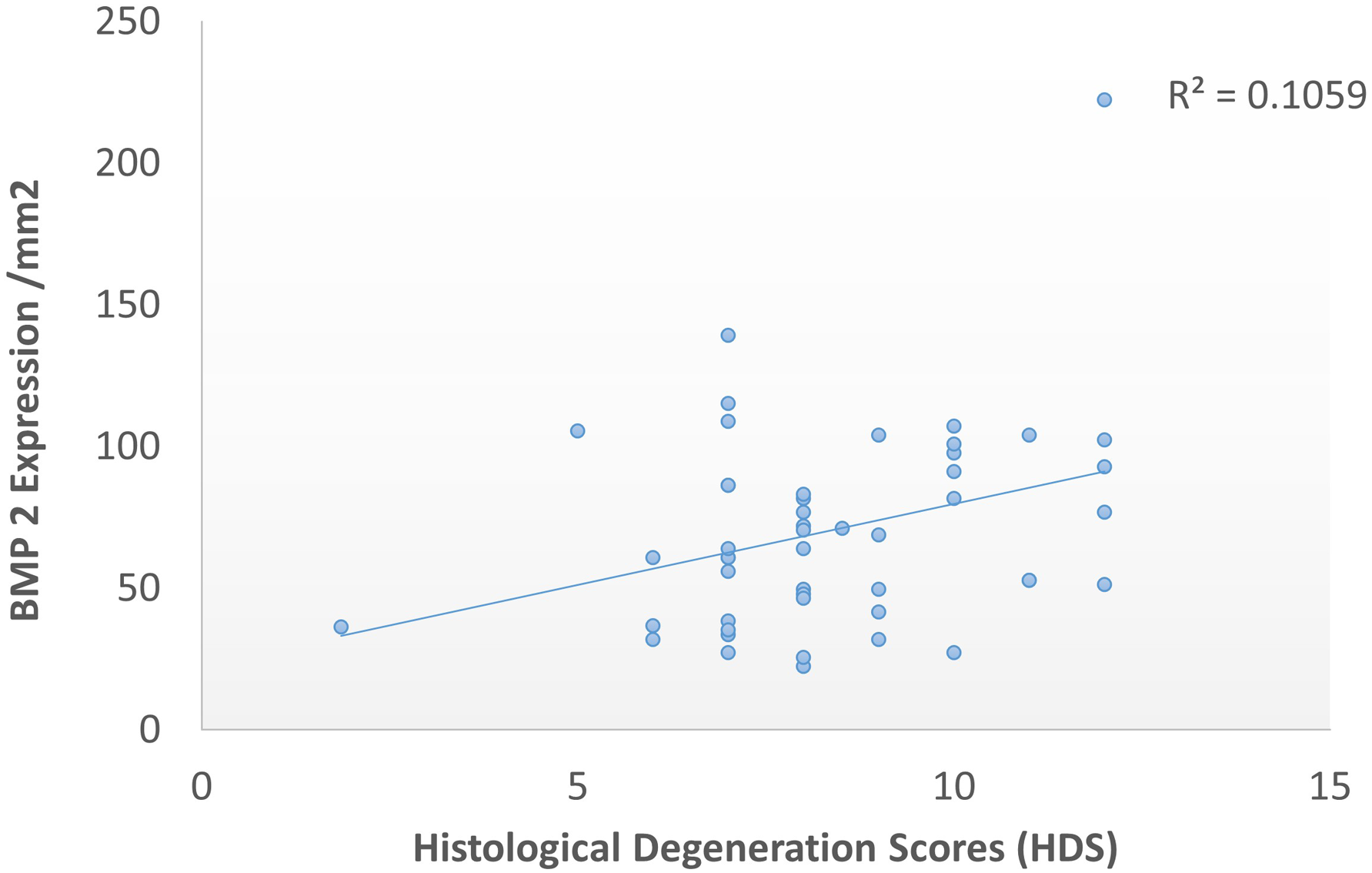
Discussion
The present study revealed a significant relationship between vertebral endplate defects with BMP-2 expression signifying calcification potential and histological disc degeneration scores.
Bone morphogenetic protein 2 (BMP-2) belongs to the family of transforming growth factor beta (TGFβ), which has been tested on various intervertebral disc models and resulted in controversial findings. Few studies report that BMP-2 can increase the chondrogenesis and extracellular matrix formation,25,26 while at the same time its inability to prevent intervertebral disc degeneration and potential of intervertebral disc ossification have also been shown in the literature.27,28 Multiple studies have observed the upregulated signaling of BMP2 in degenerative specimens and positive correlation with the Pfirrmann MRI grading of disc degeneration6-8 which was also evident in the current study. It is assumed this increased expression of BMP-2 is most likely an insufficient anabolic response to injury 8 in relation to its capability to promote cellular proliferation with increased production of aggrecan and type II collagen, as well as an increase in proteoglycan synthesis in intervertebral discs. 26 In addition, many in-vivo animal experimental studies found out that BMP-2 has the potential to provoke accelerated degenerative process and spontaneous osseous fusion. 27 This response of BMP-2 may possibly be due to its capacity in osteoinduction. Results of the previous studies demonstrate that BMP-2 induces mineralization with deposition of calcium salts of the annulus more pronounced at the anchorage of the annulus fibers with the vertebral endplate. The followed expression levels of Osterix and Osteocalcin to BMP-2, confirm that the BMP-2 level is consistent with the osteogenic potential of degenerated discs. Therefore, it is hypothesized by previous authors that BMP-2 plays two roles in degenerated discs: one is compensatory, in which BMP-2 accelerates cartilage repair, and because this compensatory expression cannot completely reverse the degeneration, overexpression of BMP-2 finally leads to the ossification of discs as a side effect. 7
The signaling of BMP-2 is strongly evident to be regulated by mechanotransduction pathways, stimulation of BMP-2 with concurrent mechanical loading leads to osteoblastic differentiation via regulation of the early BMP target gene inhibitor of differentiation 1 (Id1).29,30 The mechanical alteration produced by vertebral defects can be the potential reason to modulate the expression of BMP-2 in the intervertebral discs. 30 In the current study the increased expression of BMP-2 in the discs with vertebral endplate defects are highly suggestive of this notion. Structural integrity of the endplate is important to maintain the internal environment of the discs including a uniform intradiscal stress distribution and regulating the transport of disc nutrients and metabolites. 31 The vertebral endplate defects creates abnormal stress distribution 17 which may lead to the activation of BMP-2 pathways. Studies suggest that BMP signaling disturb the inflammatory process and once the inflammation is settled, the osteogenic properties of BMPs may take the lead. 30
Previously, the pathogenesis of calcification of scoliotic intervertebral disc are linked with altered mechanical loading12,32 similar phenomenon can be predicted in the current study. This is highly likely that the altered mechanical stresses due to vertebral endplate defects might have increased the BMP-2 expression in our samples leading to disc calcification. The herniated discs with vertebral endplate defects could calcify if retained for a longer period. The orthopedic surgeons should consider this possibility while keeping the patients on conservative management and proper follow up should be planned. However, prospective studies are essential to establish the causal relationship between vertebral endplate defects and intervertebral disc calcification. We do not intend to convey that these patients should be followed for an extended period to allow disc calcification. Rather, our recommendation is that patients with prolapsed discs and VEP defects, if managed conservatively, should be closely monitored as disc calcification may occur over time.
This is the first study, which has highlighted the association of vertebral endplate defects with BMP-2 expression in the degenerated discs, but like every other study, there were certain limitations. Slightly large sample size could have improved certain associations and generalizability of the findings. The addition of other calcification and stress markers may have been more useful to further explore this association.
Conclusion
Our study demonstrates that strong association exists between vertebral endplate defects and BMP-2 expression suggesting the possibility that mechanical alteration induced by vertebral endplate damage can be a factor, which can further enhance the process of disc degeneration by inducing calcification markers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Pakistan Science Foundation grant number PSF//Res//P-UHS//Med (518).
IRB Approval Number
UHS/Reg-18/ERC/2434