
Abstract
Study Design
Retrospective cohort study.
Objective
To compare the results of revision extension of fusion surgery using the newly designed revision rod and implant-replacement surgery in thoracolumbar spine.
Methods
Thirty-one patients who underwent extension of fusion surgery using the revision rod for adjacent segment disease were included in this study. Thirty-one patients who underwent implant-replacement revision surgery were selected as a control group by matching age, sex, preoperative diagnosis, and number of revision segments.
Results
The mean age was 70.7 ± 8.0 years in the revision rod (RR) group and 69.0 ± 8.4 years in the control group. Preoperative diagnoses, underlying diseases, and mean number of revision segments (2.2 ± 1.1) were similar in both groups. The change of hemoglobin (1.0 ± 1.9 vs 2.5 ± 1.5 g/dl; P < .01), hematocrit (4.1 ± 4.9 vs 7.2 ± 4.4 % P < .01) and albumin (.8 ± .9 vs 1.3 ± .4 g/dl; P < .01) levels before and after surgery showed significant differences between the two groups. Hemovac drainage was significantly less in the RR group (P = .01). The mean operative time was shorter in the RR group (203.5 ± 9.5 min vs 233.5 ± 8.7 min; P = .12) with no statistical difference. Radiological results showed that the average lumbar lordosis 2 years after surgery was lower in the RR group compared to the control group (25.1 ± 9.9° vs 32.9 ± 9.8°; P = .02). Union rates and clinical outcomes were not different between the two groups.
Conclusion
Revision extension of fusion surgery using a newly designed revision rod had less hemovac drainage and superior laboratory findings compared to implant-replacement revision surgery.
Introduction
Spinal fusion surgeries for lumbar spinal diseases have increased over the past decades in parallel with the aging society. Despite advances in surgical techniques and instruments, revision surgery after primary lumbar fusion has also increased.1,2
The success rate for revision surgery of the lumbar spine is variable (range 40 to 94%) and the outcomes of revision surgery are not as good as those of primary surgery.3-5 Cho et al 6 reported that revision surgery achieved average improvements of 4.1 points on the Oswestry Disability Index (ODI) scale compared to primary surgery with 12.4 ODI scale improvement. Unsatisfactory surgical outcomes after revision surgery might be associated with more postoperative complications, prolonged operative time, and a greater risk of hemorrhage.6,7
Adjacent segment disease (ASD) is one of the most common causes of revision surgery. The revision surgery for ASD includes decompression surgery alone or decompression and fusion surgery. Although it has not been determined which surgical method is optimal for ASD, revision surgery often requires fusion extension.3,8-10 There are two options for fusion extension surgery: implant replacement and implant preservation technique. Implant replacement technique involves removing the existing rods and replacing it with a new longer rods, which increases surgical time and blood loss. On the other hand, implant preservation technique reduces bleeding and shortens operative time by avoiding the need to remove the existing rod.7,11
One method of implant preservation technique is to connect the new rod to the existing rod using one additional rod and two side-to-side connectors (Figure 1A). Another method is to connect the new rod directly to the existing rod using end-to-end connector (Figure 1B). However, implant preservation technique using additional rods and side-to-side connectors like Figure 1A is not applicable to single level fusion extension, even though ASD occurs most commonly in one segment proximal to the previous fusion. Implant preservation technique using an end-to-end connector like Figure 1B is also not applicable to single level fusion extension. Another limitation of technique using end-to-end connectors is that they can only be used if the end of an existing rod is long enough to attach.
7
Implant preservation techniques for fusion extension surgery. (A) Connect a new rod to an existing rod using an additional satellite rod with two side-to-side connectors (B) Connect a new rod directly to an existing rod using an end-to-end connector.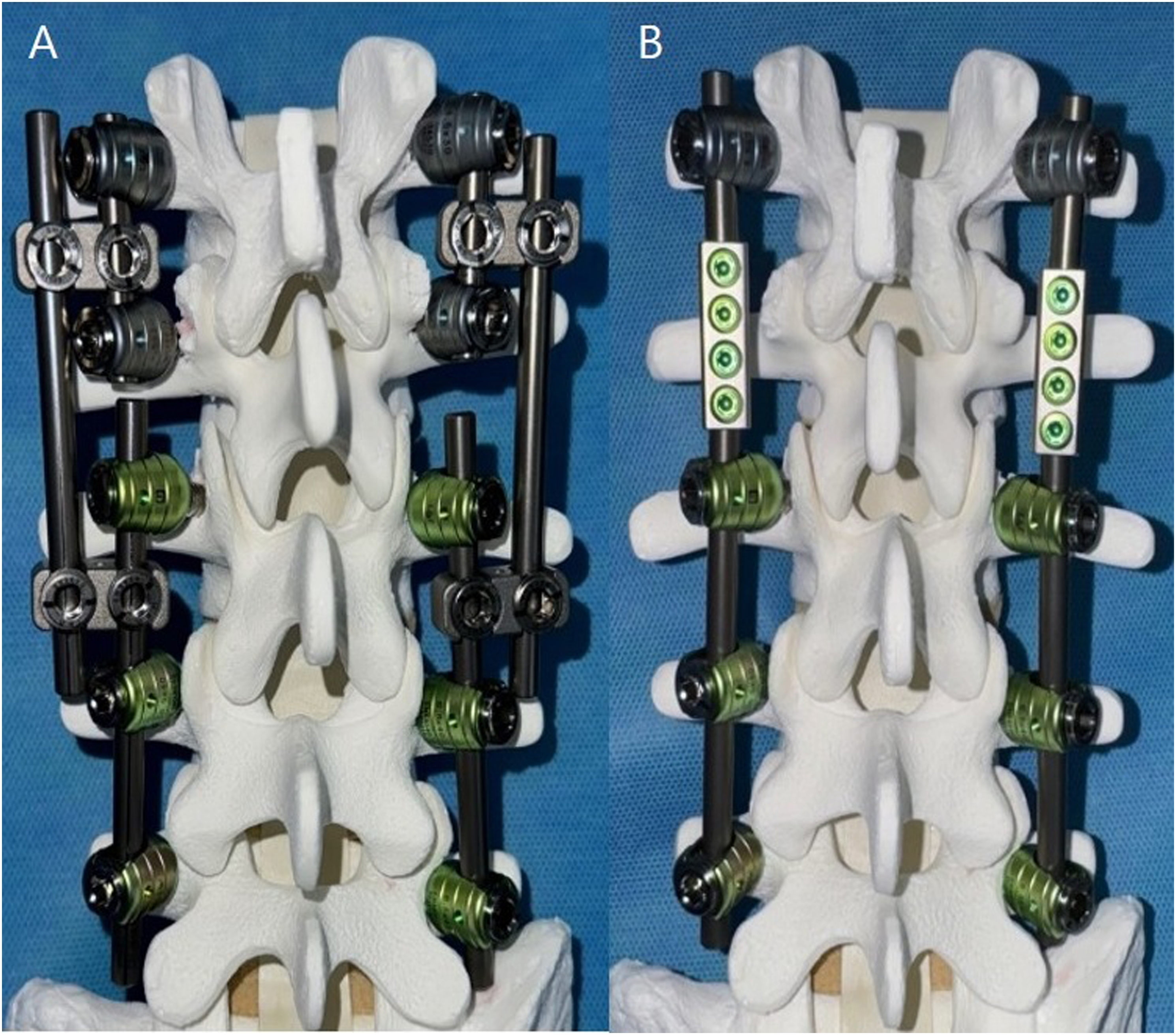
A revision rod (LEDTM, Level Extension Device, South Korea) was designed by cutting a thick rod into the shape of a lightning-bolt (Figure 2). This design’s rod allows for single level fusion extension, and the revision rod and the existing rod to be connected with one offset connector, enhancing construct stability (Figure 3). A preliminary study about revision fusion surgery using this revision rod was published in 2020 after 1-year follow-up period on 21 patients who underwent surgery at two university hospitals.
12
This study showed that thoracolumbar revision surgery using the revision rod achieved successful bony union with good clinical outcomes. No mechanical complications related to the revision rod were observed. Newly designed revision rod. (A) Revision rod with a shape of a lightning bolt. (B) Fusion extension surgery using revision rod. A: A 69-year-old female patient underwent fusion surgery from L3 to S1 for degenerative spinal stenosis. B: The patient underwent revision extension of fusion surgery for adjacent segment disease at L2-3 using newly designed revision rod 12 years after primary surgery, and showed complete bony union.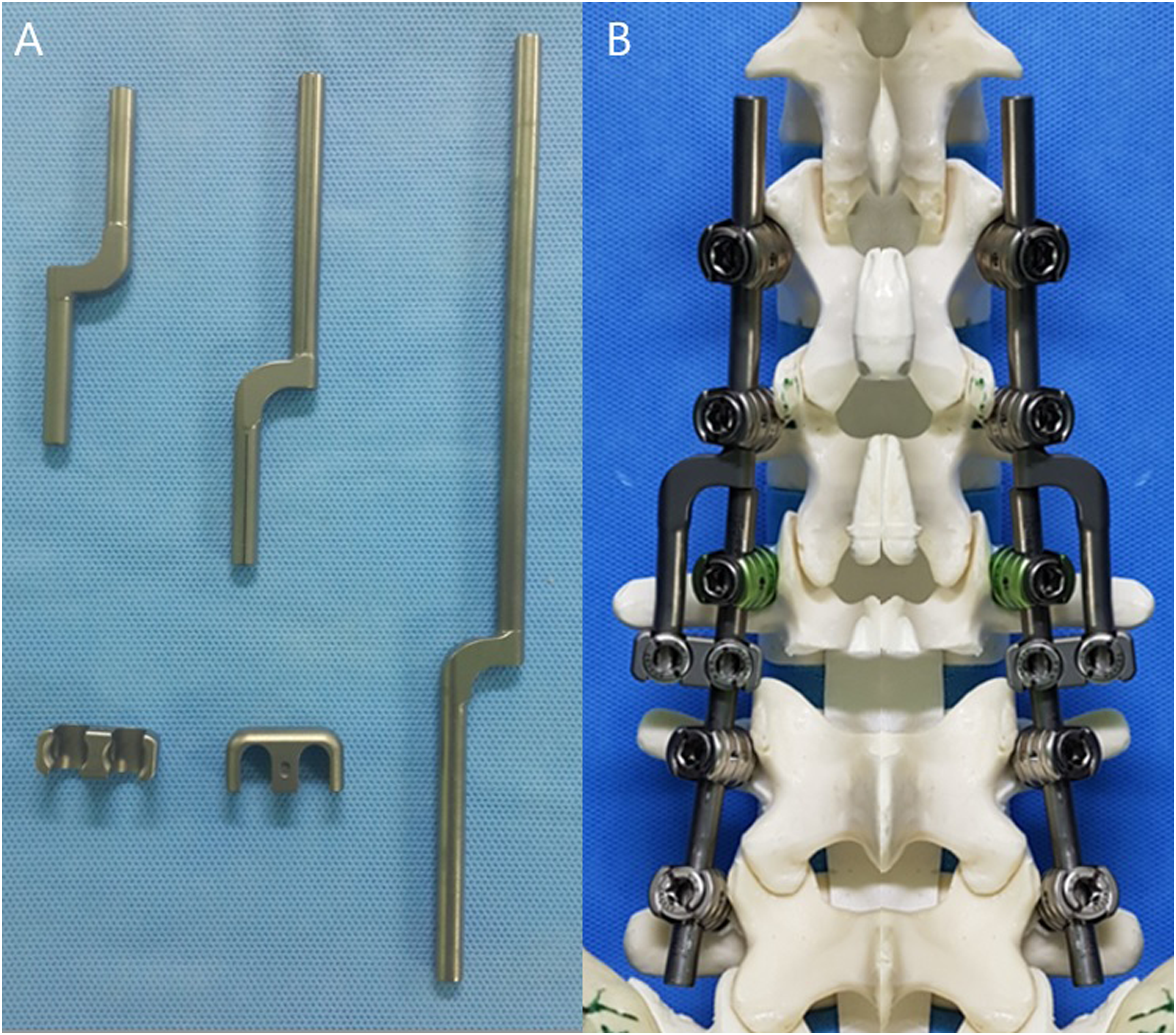
The purpose of this study was to evaluate the laboratory, radiological, and clinical results of revision extension of fusion surgery using the newly designed revision rod, and to compare the results with implant replacement revision surgery.
Materials and Methods
This study was approved by the Institutional Review Board (IRB) at Inha University Hospital (2020-03-017) and the requirement for written informed consent was waived by the IRB.
Patient Selection
The medical and surgical records of the patients that underwent revision surgery after primary fusion in a single hospital were analyzed. Thirty-one patients who underwent revision fusion surgery using a revision rod under a diagnosis of adjacent segment disease with a minimum 2-year follow-up were included from September 2014 to December 2020. For comparison, 31 patients who underwent implant-replacement revision surgery were selected as controls. These two groups were matched for age, BMI, sex, diagnosis, underlying disease, and number of revision segments.
Design of the Revision Rod
The newly designed revision rod was made in the shape of a lightning bolt. (Figure 2) It was manufactured by carving a thick rod to prevent the strength of the rod from weakening at the bent part of the rod. One end of the rod is connected to the pedicle screw at the revision site, and the other end is connected to the existing rod using offset connectors at the previous surgery. Biomechanically, rod connection using offset connector is a secure method for extension of the construct and is equivalent to a conventional continuous rod construct.13,14 To maintain construct stability, the nuts on the offset connectors must be the same size as those used on pedicle screws.
The mechanical evaluation of the revision rod and offset connector were performed. Compression bending fatigue test was set up on a universal testing machine. (Figure 4) At a compression fatigue load at 133N, any failure of revision rod, offset connectors, and other components was not observed until 5,000,000 cycles. The fatigue load was the same as the maximum run out load of existing straight rod. This test showed the revision rod assembly had mechanical performance that was substantially equivalent to the straight rod for spinal pedicle screw system. As a result of this mechanical test, the use of the revision rod assembly was approved by the Korean National Ministry of Food and Drug Safety test (99-194). Test set-up for compression bending fatigue test apparatus.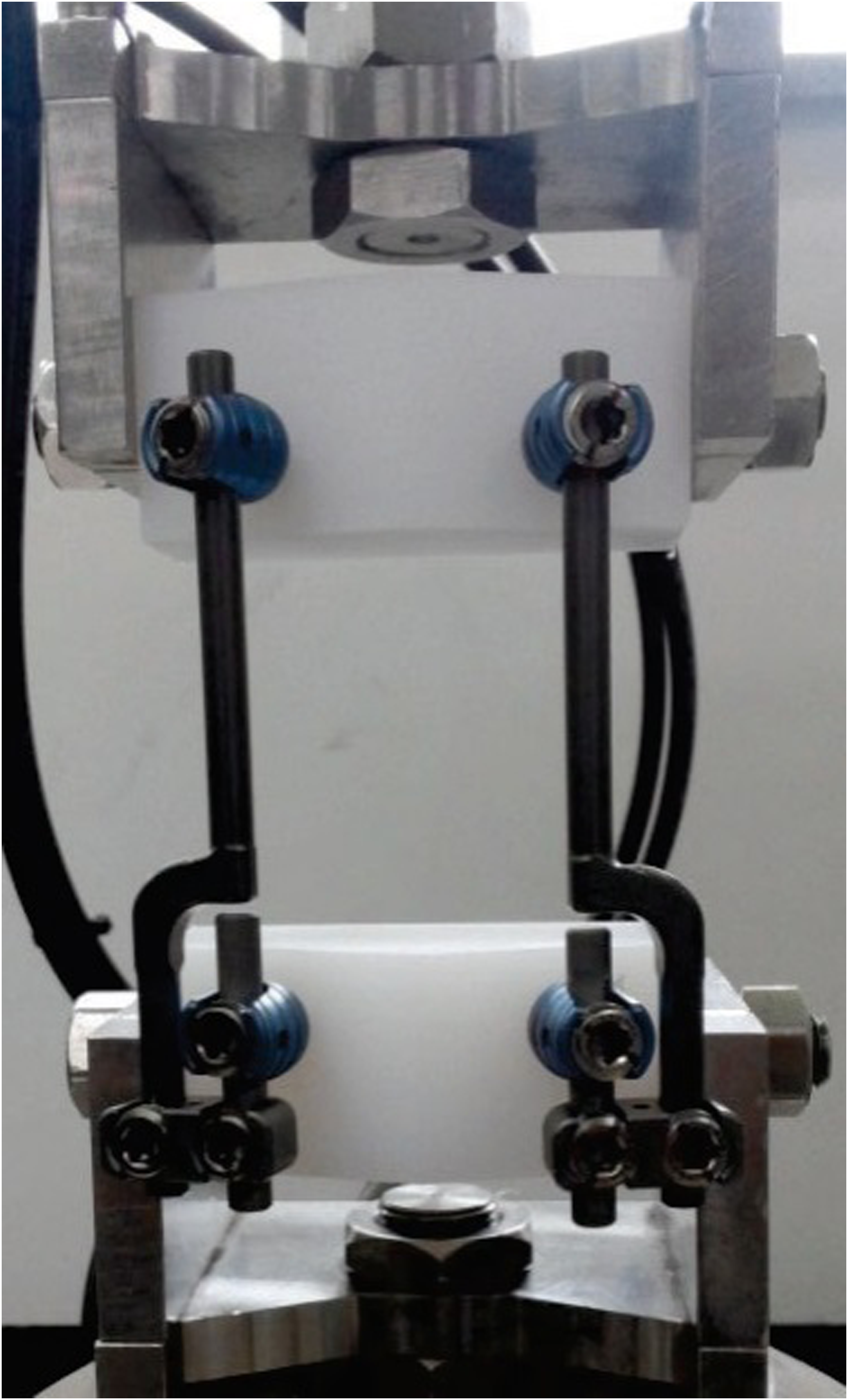
Surgical Technique
A single senior surgeon performed all operations. Spinal decompression and posterolateral inter-transverse fusion were performed through the posterior approach. In some patients, transforaminal lumbar interbody fusion using hyper-lordotic angle cages was added to achieve lumbar lordosis restoration. The instrumentation procedures were identical in the two groups, except for revision rod use.
Hemodynamic Assessment
Hemoglobin (Hb), hematocrit (Hct), and albumin, and estimated blood loss (EBL) were evaluated before surgery, immediately after surgery, and on postoperative days 2 and 3. Operative times, hemovac drainage amounts, and perioperative transfusion requirements were also analyzed. Packed RBCs were transfused when a Hb level was <8 g/dL
Radiological and Clinical Assessment
Radiological evaluations were performed before surgery and at 1- and 2-year follow-up visits. The following were measured: (1) Lumbar lordosis (LL, the angle between tangent lines to the superior endplate of L1 and superior endplate of S1). (2) T5-12 kyphosis (the angle between the endplates of T5 and T12. (3) Proximal junctional kyphotic angle (PJK angle; the angle between the lower endplate of the uppermost instrumented vertebra to the cephalad endplate of the two upper instrumented vertebrae (UIV+2) (4) Pelvic incidence (PI, the angle between the line perpendicular to the sacral endplate and the line joining the middle of the sacral endplate and the hip center). (5) Pelvic tilt (PT, the angle between the vertical and the line from the middle of the sacral endplate to the hip center). (6) Sacral slope (SS, the angle between the sacral endplate and the horizontal). (7) Posterolateral union rate (grade 1 was defined as complete bone union; grade 2 as partial bone resorption; and grade 3 considerable bone resorption). (8) Interbody fusion rate (grade 1 was defined as complete trabecula bone bridging; grade 2 as incomplete interbody trabecula bone formation; and grade 3 as non-formation of interbody trabecula bone). Interbody bone formation was confirmed inside and outside the cage. Clinical outcomes were evaluated using Oswestry disability indices (ODI) and a numeric rating scale (NRS) before operation and at 1-year and 2-year follow-up visits.
Statistical Analysis
The chi-squared test was used to determine the significances of differences between group categorical variables (preoperative diagnosis leading to spinal revision surgery, and pre-existing medical comorbidities), and the student’s t-test was used to compare laboratory, radiological, and clinical results. The analysis was performed using SPSS ver. 10.0 (IBM Corp. Armonk, New York, USA) using a confidence interval of 95%. Statistical significance was accepted for P values <.05.
Results
Patient Demographics
Patient Demographics of the Revision Rod and Control Groups.
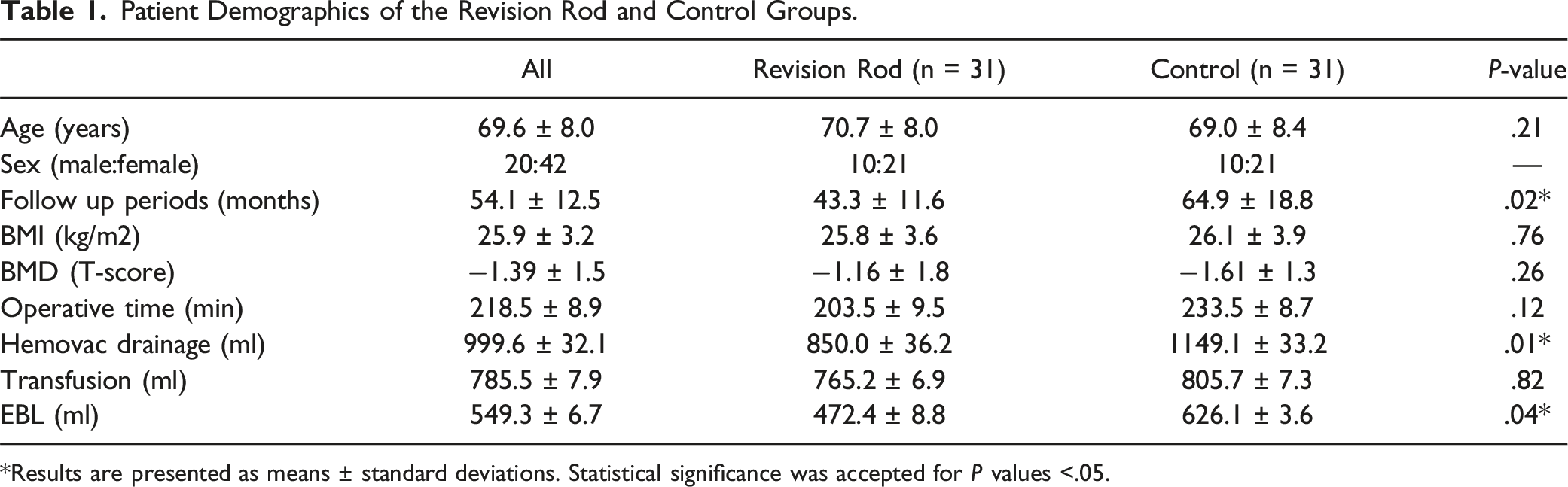
*Results are presented as means ± standard deviations. Statistical significance was accepted for P values <.05.
Mean numbers of revision segments in the RR and control groups were 2.2 ± 1.1 (range: 1-5-segments) and 2.2 ± 1.1 (range: 1-5-segments), respectively. In both groups, 10 patients underwent 1-segment revision, 10 underwent 2-segment revision, 6 underwent 3-segment revision, 4 underwent 4-segment revision, and 1 patient underwent 5-segment revision surgery.
Laboratory Outcomes
Hemodynamic Finding
Laboratory Outcomes of the Revision Rod and Control Groups.

**Results are presented as means ± standard deviations. Statistical significance was accepted for P values <.05.
Radiologic Outcomes
Lumbar Lordosis (LL)
Radiologic Outcomes of the Revision Rod and Control Groups.
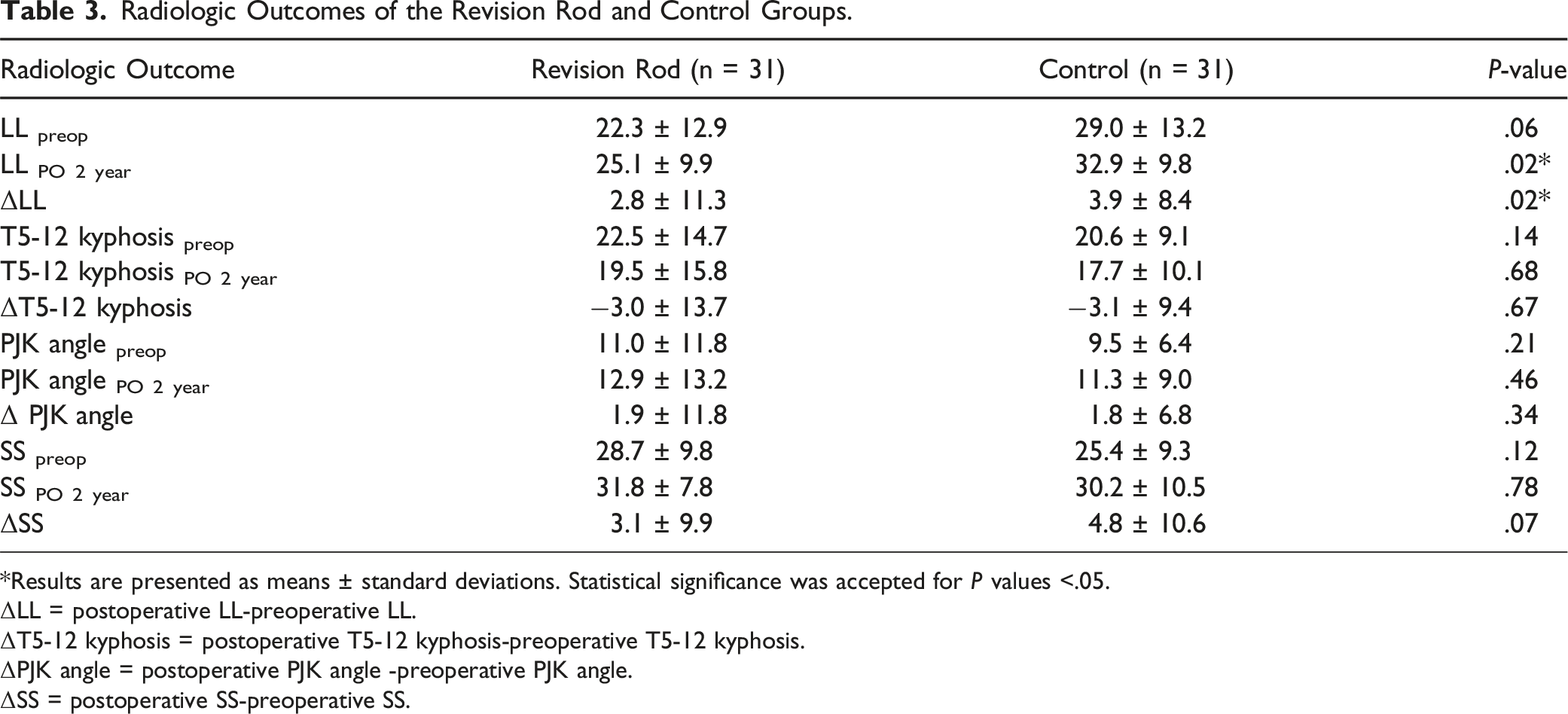
*Results are presented as means ± standard deviations. Statistical significance was accepted for P values <.05.
ΔLL = postoperative LL-preoperative LL.
ΔT5-12 kyphosis = postoperative T5-12 kyphosis-preoperative T5-12 kyphosis.
ΔPJK angle = postoperative PJK angle -preoperative PJK angle.
ΔSS = postoperative SS-preoperative SS.
T5-12 Kyphosis
Mean preoperative T5-12 kyphosis angle was 22.5 ± 14.7° in the RR group and 20.6 ± 9.1° in the control group with no statistical difference (P = .14). Mean T5-12 kyphosis angle at 2 years after surgery was 19.5 ± 15.8° in the RR group and 17.7 ± 10.1° in the control group with no statistical difference (P = .68). Corrections of T5-12 kyphosis by revision surgery were similar in the two groups (P = .67) (Table 3).
Proximal Junctional Kyphotic Angle (PJK Angle)
Mean preoperative PJK angle was 11.0 ± 11.8° in the RR group and 9.5 ± 6.4° in the control group with no statistical difference (P = .21). Mean PJK angle at 2 years after surgery was 12.9 ± 13.2° in the RR group and 11.3 ± 9.0° in the control group with no statistical difference (P = .46). PJK angle corrections after revision surgery were not different between the two groups (P = .34) (Table 3).
Sacral Slope (SS)
Mean preoperative SS was 28.7 ± 9.8° in the RR group and 25.4 ± 9.3° in the control group with no statistical difference (P = .12). Mean SS at 2 years after surgery was 31.8 ± 7.8° in the RR group and 30.2 ± 10.5° in the control group with no statistical difference (P = .78). SS correction after surgery was not different in both groups (P = .07) (Table 3).
Union Rates
Union Rates for Interbody and Posterolateral Fusion After Revision Surgery.

*Results are presented as means ± standard deviations. Statistical significance was accepted for P values <.05.
Clinical Outcomes
Clinical Outcomes of the Revision Rod and Control Groups.
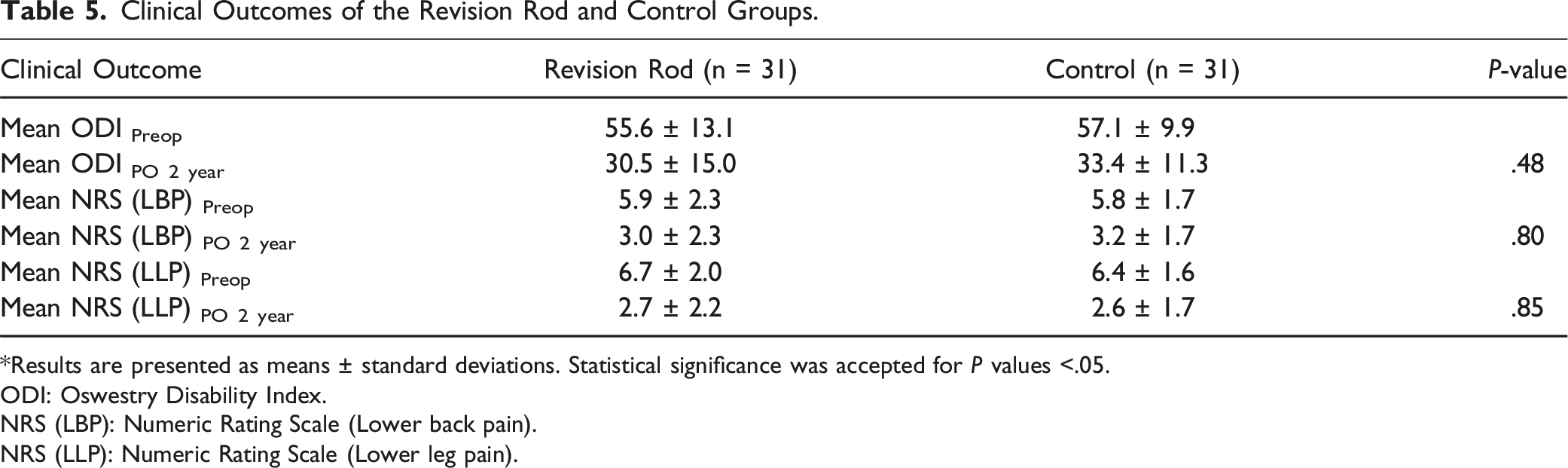
*Results are presented as means ± standard deviations. Statistical significance was accepted for P values <.05.
ODI: Oswestry Disability Index.
NRS (LBP): Numeric Rating Scale (Lower back pain).
NRS (LLP): Numeric Rating Scale (Lower leg pain).
Discussion
Revision surgery after primary lumbar fusion is increasing. 12 Martin et al reported that the reoperation rate at 11 years after fusion surgery was 19%, and Kim et al reported a rate of 22.9% at 10 years after surgery.1,2 Adjacent segment disease (ASD) accounts for 5% to 43% of revision surgery cases.8,15,16 According to Maruenda et al, the revision rate for ASD increased from 9.6% at 5 years to 24.6% at 19 years postoperatively. 15
Two surgical options have been used for ASD revision surgery; decompression alone or decompression with fusion extension. Ryu at al. reported that limited revision surgery without fusion showed a high risk of failure. 10 In their study, twenty-eight of 50 patients that underwent decompression surgery developed recurrent radiculopathy, and 78.6% of the 28 patients required revision surgery. Thus, extension of fusion surgery is advised for revision surgery for ASD.3,7,10
Extension of fusion surgery includes implant preservation technique and implant replacement technique. Compared to implant preservation technique, implant replacement technique requires exposing the entire previous surgical site, takes longer operative time, and causes more intraoperative blood loss, especially in the previous long fusion patients. This study demonstrated that implant preservation technique using revision rod was superior to the implant replacement technique in terms of reducing intraoperative bleeding and postoperative hemovac drainage. Also, the revision rod group had a shorter operative time. The revision rod was more effective for revision fusion surgery than implant preservation technique.
Conventional implant preservation technique uses additional rods and side-to-side connectors to assemble the fusion construct (Figure 1A). Having the existing rods in the primary site, new rods in the revision site, and additional rods with connectors may alter stress distribution in the instrument, which may lead to rod breakage or screw dislodgement. Rod failure commonly occurs near the connectors in multiple rod constructs as stresses are concentrated in connectors. 17 If fusion extension is required over long segments, the stability of the instrumentation may be questionable.
The newly designed revision rod was made in the shape of lightning bolt to reduce the number of connectors and increase construct stability. One end of the revision rod is directly assembled to the screw of the revision site, and the other end is connected to the existing rod with offset connector (Figure 5). A preliminary report
12
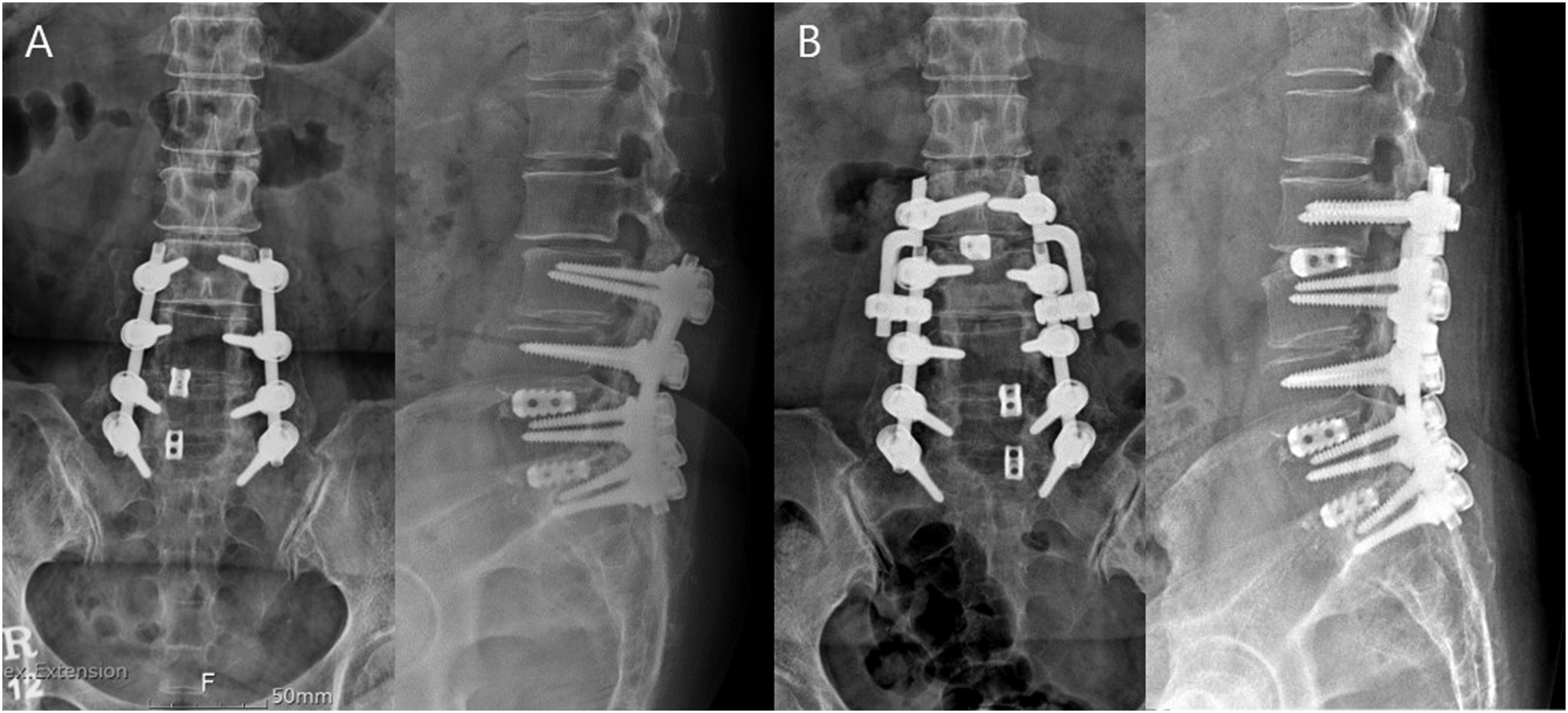
and this present study found no mechanical complications associated with the revision rod. (A) 76-year-old female patient underwent lumbar fusion surgery from L1 to S1 for spinal stenosis. (B) Three month after surgery, proximal junctional failure with L1 compression fracture occurred. (C) Revision extension of fusion surgery using revision rod was performed to T10. When performing fusion extension surgery over a long segment, the stability of the instrument can be increased by using two connectors between the revision rod and the existing rod. Although this case was not included in the study material, revision rod is a good option for patients with previous long fusion construct.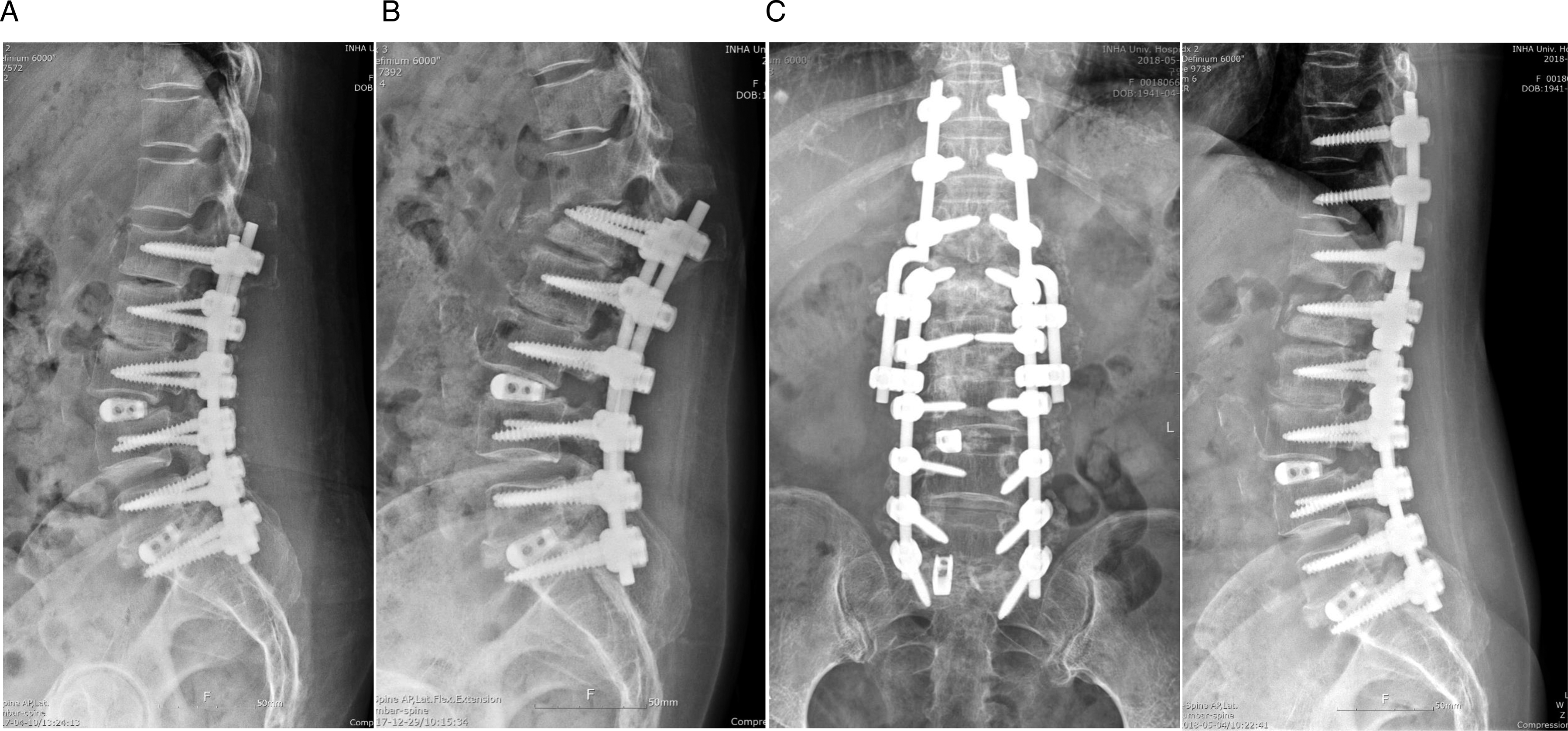
In the implant preservation technique using additional rods, the rods occupy the space needed for bone grafting in the posterolateral inter-transverse area, which may hinder bone union.7,17 When the revision rod was first introduced, bone union was also a major concern because the thick bent part of the revision rod could limit bone graft placement. In the present study, however, sufficient bone formation was observed beyond the revision rod in most patients. Posterolateral fusion was performed in 31 patients, and complete bone union was obtained in 28 patients at last follow-up visit. Twenty-two patients underwent interbody fusion, and complete bone union was observed in all patients. A previous study on implant replacement techniques reported revision surgery union rates of 90 to 95%, 18 showing similar results to this technique using newly designed revision rod.
The disadvantage of the newly designed revision rod was that the restoration of lumbar lordosis was not satisfactory compared to implant replacement technique. It is presumed that it was difficult to bend the rod to obtain sufficient lumbar lordosis because the bent part of the rod was thick. This limitation can be overcome by interbody fusion using a hyper-lordortic cage. Nevertheless, revision surgery using revision rods is not recommended for patients with kyphotic deformity requiring a high level of lumbar lordosis restoration.
This study has several limitations. First, this study does not have enough cases because it used a newly designed implant for the first time in surgery. This study demonstrated satisfactory results, and additional research is planned as the number of cases is expected to increase. Second, postoperative complications may have been influenced by the follow-up periods. Long-term comparative studies are needed to clarify this issue.
Conclusions
Compared to implant replacement technique, revision extension of fusion surgery using a newly designed revision rod shortened operative time, reduced blood loss during the procedure, and provides better laboratory findings after surgery. In the revision rod group, the decrease in hemoglobin, hematocrit, and albumin immediately after surgery was smaller than that in the control group. Additionally, successful union was achieved in the revision extension surgery using revision rods.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Inha University Research Grant.