
Abstract
Study Design
Retrospective cohort study.
Objective
The study aimed to compare the radiological parameters, clinical outcomes, and long-term effects of the posterior osteosynthesis with polyaxial screw-rod system and the monoaxial screw-rod system in the treatment of unstable atlas fractures.
Methods
We retrospectively analyzed the clinical data of 33 patients with posterior ORIF for unstable atlas fractures in our hospital from August 2013 to June 2020, with a minimum of 3 years of follow-up. Polyaxial screws (group A) were used in 12 patients and monoaxial screws (group B) in 21 patients. Perioperative data, radiological parameters, and clinical outcomes were collected and compared between the 2 surgical approaches.
Results
The operative time, blood loss, time of screw-rod system placement, and hospital stay were significantly lower in group A than in group B. At the last follow-up, the visual analog scale (VAS) score and anterior arch reduction rate of the atlas in group A were lower than those in group B, while the lateral mass displacement (LMD) in group A was higher than that in group B. There was no significant difference between Group A and Group B in terms of the anterior atlantodental interval (AADI), posterior arch reduction rate of the atlas, range of motion (ROM), and neck disability index (NDI).
Conclusions
Monoaxial screws can achieve better reduction results for unstable atlas fractures, especially for the anterior arch of atlas. However, the surgical operation of monoaxial screws is more complicated than that of polyaxial screws and has more complications. Appropriate implants should be selected for the treatment of unstable atlas fractures based on the type of atlas fracture, the experience of surgeons, and the demands of patients.
Keywords
Introduction
Unstable atlas fractures generally refer to a fracture of the atlas other than a single fracture of the anterior arch of the atlas or a single fracture of the posterior arch with the transverse atlantal ligament (TAL) intact. 1 Non-surgical treatment is selected for the early unstable atlas fractures, but the effect of non-surgical treatment is poor, which may lead to fracture nonunion or malunion.2-4 Therefore, surgical treatment is the main clinical choice at present.
Unstable atlas fractures are often accompanied by damage to the TAL, which has always been considered the most important stable structure of the atlantoaxial joint. Therefore, the traditional surgical methods are mainly atlantoaxial fusion or occipitocervical fusion.5-7 However, fusion surgery has significant trauma and causes patients to lose upper cervical motion function, especially the rotation function of the atlantoaxial joint. 8 In recent years, an open reduction and internal fixation (ORIF) has been proposed for unstable atlas fractures to preserve the motor function of the atlantoaxial joint, which has achieved satisfactory clinical results. The clinical follow-up found no significant atlantoaxial instability in patients with TAL injuries.9-17
Currently, most surgeons choose posterior ORIF for the unstable atlas fractures. The posterior approach generally involves implanting polyaxial pedicle screws into the lateral masses on both sides of the atlas, which are connected by a titanium rod and then reduced and fixed under compression force. During surgery, posterior arch fractures of the atlas can be easily reduced under direct vision, but due to the tail swing during compression with the polyaxial screws, anterior arch fractures of the atlas are often not fully reduced. For this purpose, we achieved an almost anatomical reduction of anterior and posterior arch fractures of the atlas through a simple posterior approach surgery using monoaxial screws.
However, it is unclear which is actually the preferred option: although monoaxial screws achieve an approximate anatomical reduction of the anterior arch fracture of the atlas, the monoaxial screw-rod system, which is currently widely used, has a high internal fixation notch, tends to lead to difficult postoperative paravertebral muscle reduction, chronic bursitis, and neck pain, and is surgically demanding. To our knowledge, there are no reports comparing the outcomes of the 2 procedures for unstable atlas fractures.
The purpose of this study was to compare the surgical outcomes of the treatment of unstable atlas fractures with polyaxial and monoaxial screws and to provide a detailed analysis of imaging indicators and cervical motor function to provide guidance for clinical decision-making.
Materials and Methods
Study Design and Patients
This retrospective comparative study was approved by the institutional review board of the First Affiliated Hospital of Anhui Medical University, Hefei, China (approval number: 2023-07-65). Thirty-three consecutive cases of atlas fractures in our hospital between August 2013 and June 2020 were analyzed. Of these cases, 12 patients were treated with polyaxial screws (group A) in the early stage, and 21 patients were treated with monoaxial screws (group B) in the later stage. The aim was to assess the postoperative outcome of the 2 different types of internal fixation.
This study included patients with at least 3 years of follow-up. Pre-operatively, basic information was collected on the patient’s gender, age, body mass index (BMI), type of fracture, type of TAL injury, time from injury to surgery, cause of injury, combined injuries, adverse hobbies, and imaging data. Perioperative information was collected on operative time, blood loss, time of screw-rod system placement, and hospital stay. All operations were performed by a senior surgeon (Y-S.Z.).
Patients who met the following criteria were included in the study: (1) diagnosed with unstable atlas fractures through cervical imaging examination; (2) complete follow-up information and signed informed consent; and (3) no previous cervical spine disease or cervical spine trauma or surgery. Exclusion criteria: (1) severe organ damage that cannot tolerate surgery; (2) combined with occipital condylar and odontoid fractures; (3) combined with infection and tumor; (4) neurological dysfunction due to spinal cord injury; and (5) less than 3 years post-operative follow-up.
Surgical Technique
The procedure for the treatment of unstable atlas fractures is approximately the same for the polyaxial screws and the monoaxial screws, both consisting of 2 screws with titanium rods and with a screw diameter length of 3.5 mm. Both internal fixation devices are manufactured by Fule Company in Beijing, China.
The patients were placed under general anesthesia in a Mayfield head holder with skull traction in a prone reverse-Trendelenburg position, thereby achieving partial skull traction. This helps to obtain a good exposure of the posterior arch of the atlas and facilitates partial traction reduction before surgery. A 10-cm long posterior midline incision was made from the occipital bone to the C3 spinous process. The skin, subcutaneous tissue, and deep fascia were incised layer by layer, and subperiosteal dissection was performed, exposing the C1 posterior arch approximately 3-cm lateral to the midline and preserving the extensor muscle insertion on the C2 spinous process as far as possible. Based on the measurements of preoperative computed tomography (CT) and three-dimensional printing models, the ideal entry point, the screw direction, and the screw length were determined. The pedicle cortex was first ground with a grinding drill, and then the guidewire was inserted after slow drilling with a hand drill. Two screws with a diameter of 3.5 mm were inserted into the posterior arch of the C1 using the notching technique separately, 18 and the 2 screws were connected with titanium rods, which were prefabricated to adapt to the curve of the C1 posterior arch. One of the nuts was first tightened, then a compressor device was used to gently apply a compressive force to 2 screws, and the other nut was tightened subsequently. Intraoperative fluoroscopic open-mouth posteroanterior view or C-arm three-dimensional imaging fluoroscopy showed good screw length and angle.
Postoperative Treatment
All patients were encouraged to get out of bed the first day after surgery and the drainage tube was removed 24-48 hours after surgery (drainage <50-mL) depending on the amount of drainage. Prophylactic antibiotics were routinely administered for 48 hours postoperatively to prevent infection. CT scans were performed within 1 week after surgery to evaluate the effectiveness of fracture reduction and the accuracy of 2 types of screw insertion. Each patient was fixed with a Philadelphia neck brace for 4-6 weeks. After 3 months, CT scans and three-dimensional reconstructions were performed on the upper cervical spine to evaluate the reduction of the fracture. At the final follow-up, the anterior atlantodental interval (AADI) and lateral mass displacement (LMD) were calculated based on radiography and CT, and the level of neck pain was evaluated using a 10-point visual analog scale (VAS) score. The patient’s cervical motor function was evaluated using a three-dimensional range of motion (ROM).
Evaluation Index
The primary comparison indicators were neck disability index (NDI) score (compared with the patient test scores at preoperative and final follow-up), VAS score (compared with the score at preoperative and final follow-up), ROM of the cervical (including flexion-extension and axial movements, based on dynamic radiographic measurements), LMD (calculated from coronary CT reconstruction images), AADI (calculated from lateral radiographs), and bone reduction rate (reduction of anterior and posterior arch of atlas). Secondary evaluation indexes were as follows: (1) Intraoperative conditions: operation time, blood loss, time of screw-rod system placement, and hospital stay (2) The internal fixation was observed for loosening or rupture at follow-up, and intraoperative and postoperative complications were observed.
Statistical Analysis
Statistical analysis was conducted using SPSS statistical software (version 23.0; SPSS, Chicago, Illinois, United States). The measurement data were expressed as mean ± standard deviation and independent t-tests were used to compare continuous variables between groups A and B. Count data were expressed as frequencies and percentages, and chi-square or Fisher-exact tests were used to compare categorical variables. Paired t-tests were used to compare NDI and VAS scores preoperatively and at the final follow-up. A P-value less than .05 was statistically significant.
Results
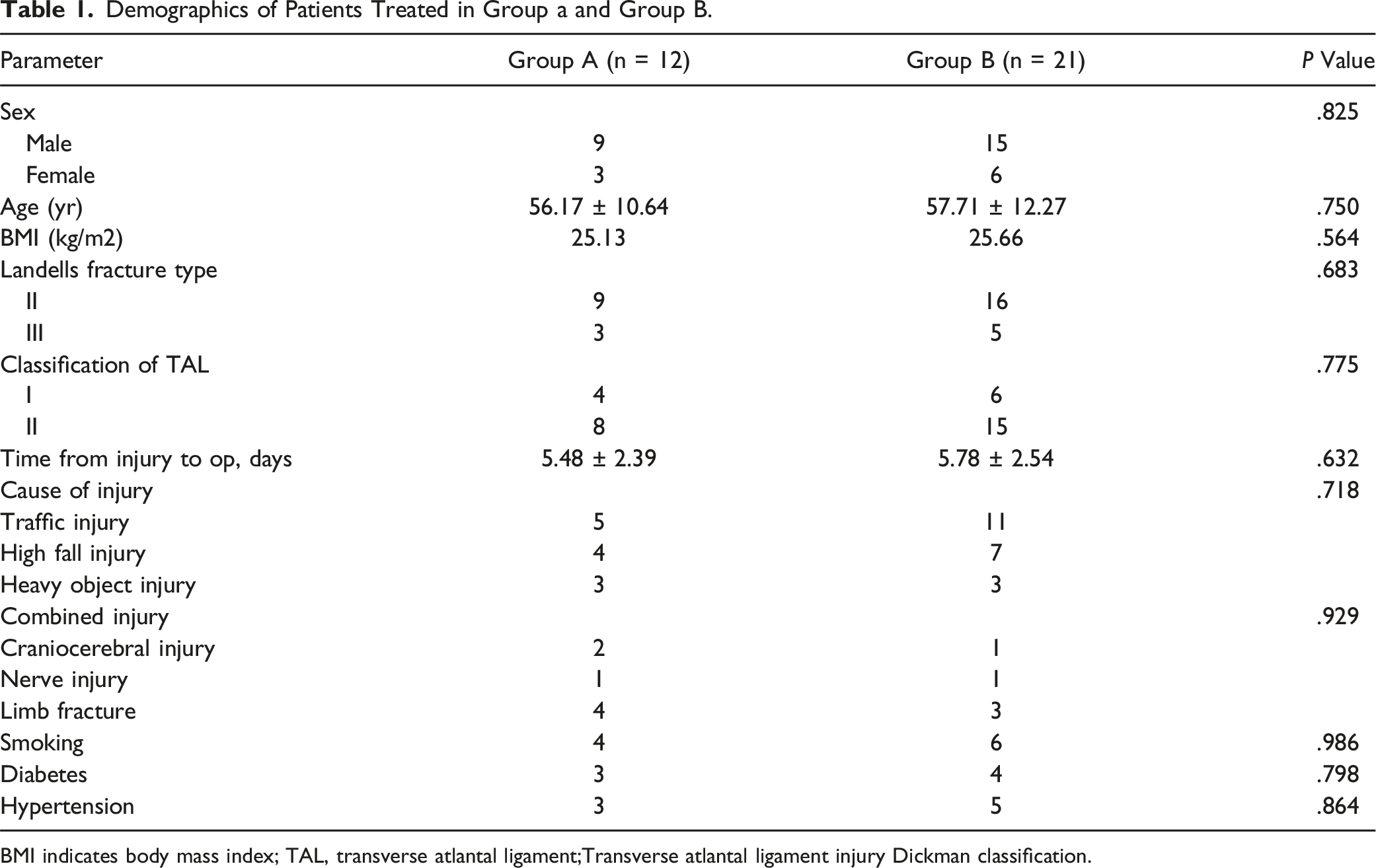
A total of 39 patients with the atlas fracture were included during the reference period. After screening, 33 of these patients (12 in group A and 21 in group B) who met the study criteria enrolled in the study (Figure 1). A total of 6 patients in both groups were excluded because of less than 3 years of follow-up or the combination of other cervical fractures. Among the 33 patients, 24 were males and 9 were females, with a mean age of 56.90 years (range 27-77) and a mean BMI of 25.30 (range 19.64-30.31). The mean time from injury to surgery was 5.90 days (range 2-11). According to Landells’ fracture type,
19
there were 25 cases of type II fractures and 8 cases of type III fractures. According to Dickman’s classification,
20
there were 10 cases of type I TAL injuries and 23 cases of type II injuries. Of the 33 patients, 16 were injured in traffic accidents, 11 were injured in high falls, and 6 were injured by heavy objects. Among the compound injuries, 3 patients had combined craniocerebral injuries, 2 patients had nerve injuries, and 7 patients had limb fractures. The demographic data of patients are summarized in Table 1, and there were no statistical difference in the data between the 2 groups. Flowcharts for 2 groups of patients. Demographics of Patients Treated in Group a and Group B. BMI indicates body mass index; TAL, transverse atlantal ligament;Transverse atlantal ligament injury Dickman classification.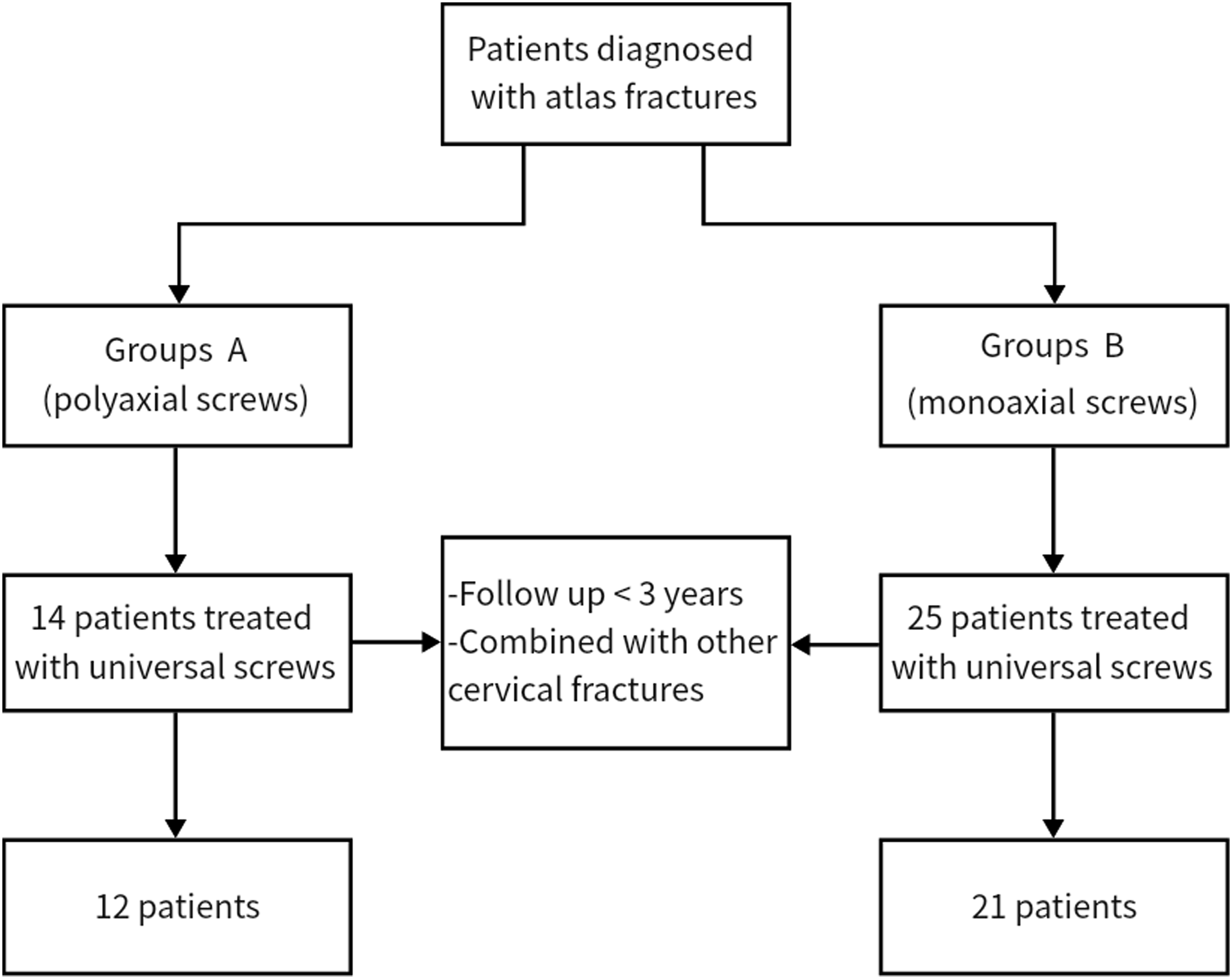
Perioperative Data Assessment
Perioperative Data for Group a versus Group B.

Comparison of Radiographic Parameters
Postoperative Radiological Parameters and Clinical Outcomes in Groups a and Group B.
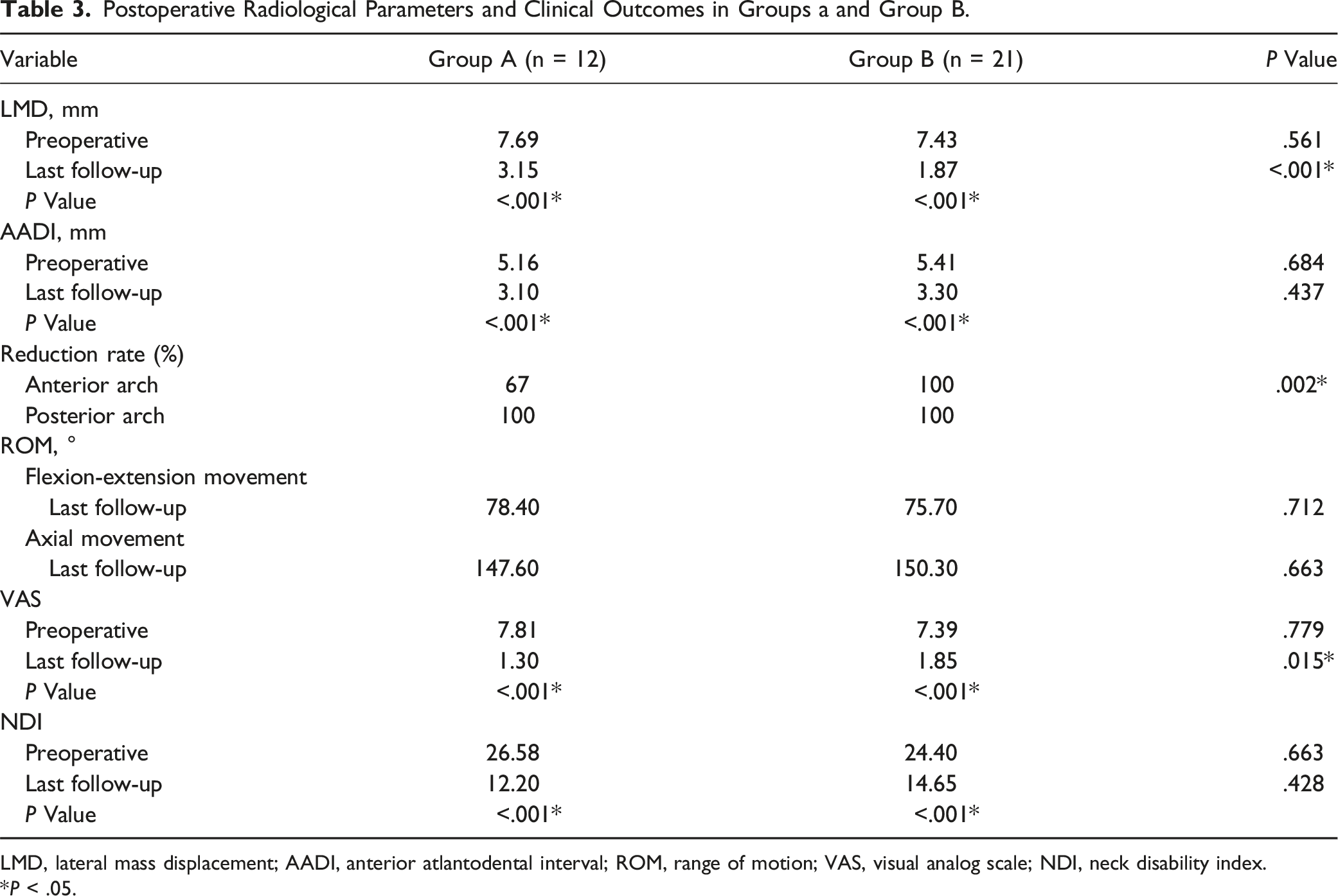
LMD, lateral mass displacement; AADI, anterior atlantodental interval; ROM, range of motion; VAS, visual analog scale; NDI, neck disability index.
*P < .05.
According to CT scans and three-dimensional reconstruction at 3 months after surgery, the reduction rate of the anterior arch of atlas in Group A (8/12, 67%) was significantly lower than that in Group B (21/21, 100%) (P = .002). However, the reduction rate of the posterior arch of atlas in both Group A and Group B reached 100%. A typical case is shown in Figure 2. (A) 41 year-old female patient was admitted to the hospital 6 hours after complaining of neck pain due to injuries sustained in a traffic accident. (A, C) Lateral mass displacement. (B, D) Postoperative open-mouth and lateral X-ray image. (E, G) Preoperative CT scans revealed a fracture of the right anterior and posterior arch of the atlas. (F, H) 3 months after surgery, CT scans and three-dimensional reconstruction images showed satisfactory fracture reduction. (I-L) At the last follow-up, the patientfully recovered the full range of motion of the cervical spine without pain.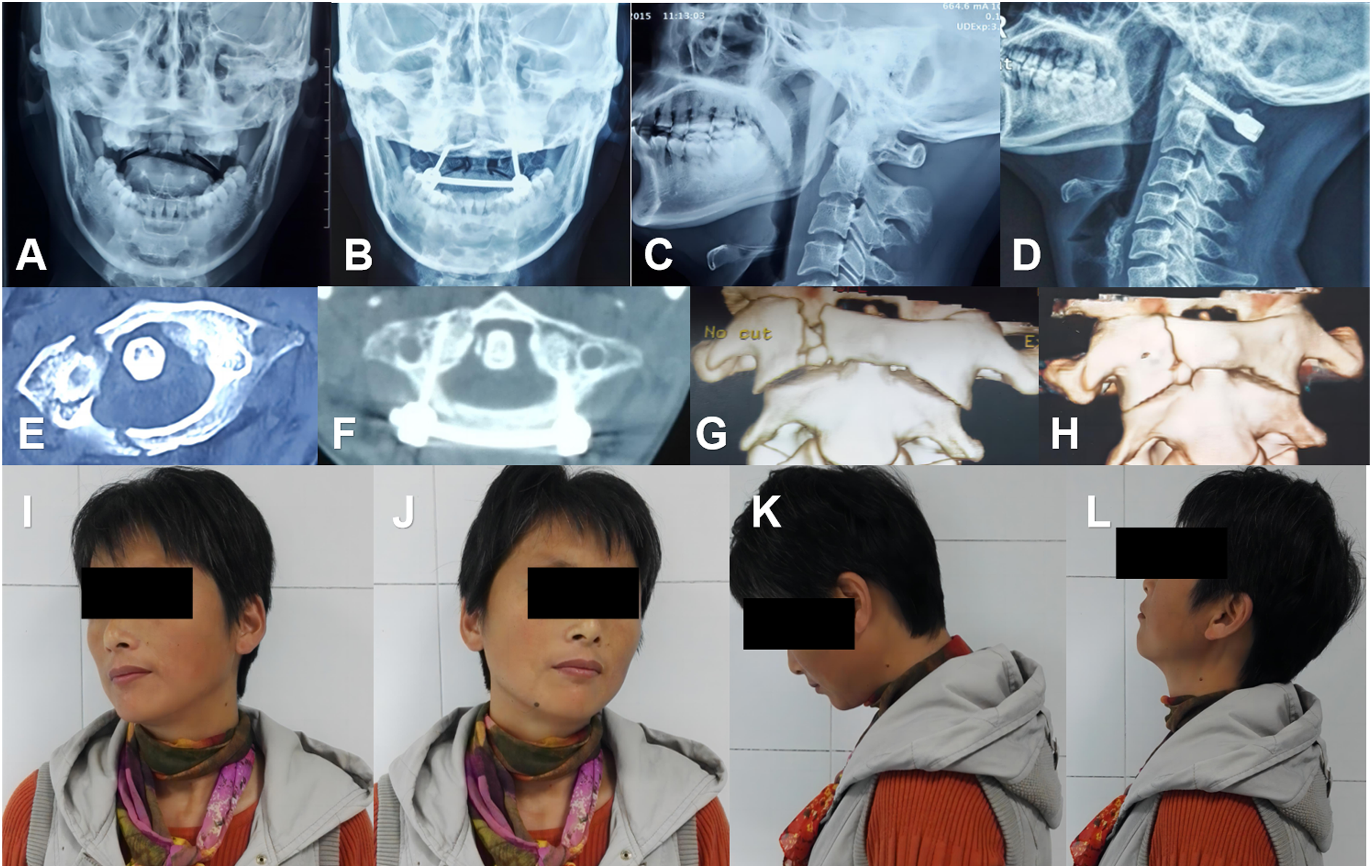
Cervical Motor Function and Neck Pain Assessment
There was no significant difference in the preoperative VAS score between the 2 groups, and the postoperative score was lower than the preoperative score in both groups. At the last follow-up, the VAS score for neck pain was lower in both groups than postoperatively, and the VAS score for neck pain was lower in Group A than in Group B, with a statistically significant difference. The mean preoperative NDI score was 26.58 in Group A and 24.40 in Group B, with no statistical significance (P = .663). The mean NDI score of Group A and Group B was 12.20 and 14.65 at the last follow-up, with no statistical significance (P = .428). In each group, the NDI score at the last follow-up was significantly lower than before surgery (P < .001).
As shown in Table 3, the average ROM of cervical flexion-extension and axial in Group A at the last follow-up were 78.40 and 147.60, respectively, while those in Group B were 75.70 and 150.30 (Figure 2). The various activities of the cervical vertebrae in both groups basically returned to normal. There was no statistically significant difference in postoperative cervical mobility between the 2 groups of patients.
Complications
Postoperative CT confirmed that the screws used in both study groups were well positioned. In Group A, 33% of patients (4 out of 12) who used polyaxial screws experienced anterior arch bone nonunion of the atlas 1 month after surgery. At the last follow-up, CT confirmed bone fusion, but the reduction effect of the anterior arch of the atlas was not satisfactory. No other complications (neurologic deficit, vertebral artery injury, or wound infection) occurred. In group B, all patients achieved good bone fusion, as confirmed by CT at the last follow-up. However, 6 patients complained of greater occipital nerve neuralgia after surgery, which gradually disappeared 1 month after surgery. Four patients had occipitocervical discomfort and limited mobility, and their symptoms gradually improved after physiotherapy and analgesics. Chronic bursitis occurred in 3 patients.
Discussion
In recent years, the use of posterior polyaxial screws osteosynthesis for unstable atlas fractures has been recommended by many surgeons with good clinical results in order to preserve the motor function of the atlantoaxial and atlantooccipital joints.1,10,12,21-27 However, most of these previous studies were case reports or case series, lacking control groups and long-term follow-up. We have previously reported the use of posterior monoaxial lateral mass screw-rod system osteosynthesis for unstable atlas fractures, 9 which can maintain normal function at C0-2 and has gradually been promoted and applied in clinical practice. In this study, a retrospective, controlled method was used to compare the long-term clinical effects of posterior internal fixation using the polyaxial screws technique and monoaxial screws technique. This is the first innovative study to compare 2 technologies.
Polyaxial Screw-Rod System
ORIF is an emerging surgical technique in recent years, and scholars have experimented with a variety of surgical approaches and methods.11,28,29 Posterior ORIF is a fixation technique based on atlas lateral mass screws and pedicle screws. The technique of atlas lateral mass screws implants is relatively mature, with high screw fixation strength and a large operation space during posterior surgery, and the internal fixation is not easy to loosen after surgery. In addition, posterior surgery has a lower risk of infection than transoral surgery. However, when ORIF with posterior polyaxial screws is performed, although lateral displacement of the lateral mass to the sides can be effectively reduced by lateral compression with the aid of instruments, the reduction of the anterior arch fracture line is often unsatisfactory when the separation of the anterior arch fracture is large, resulting in longer fracture healing times or even non-union of the fracture. After applying pressure to the tail of the screw, the fracture of the posterior arch is reduced. However, due to the pendulum effect at the tail of the polyaxial screw, the front of the screw cannot be adducted, preventing a satisfactory reduction of the fracture of the anterior arch (Figure 3(A)). The anterior arch of the atlas is more important for the stability of the atlantoaxial, so for unstable atlas fractures, the importance of surgical reduction of anterior arch fractures is much greater than that of posterior arch fractures.
30
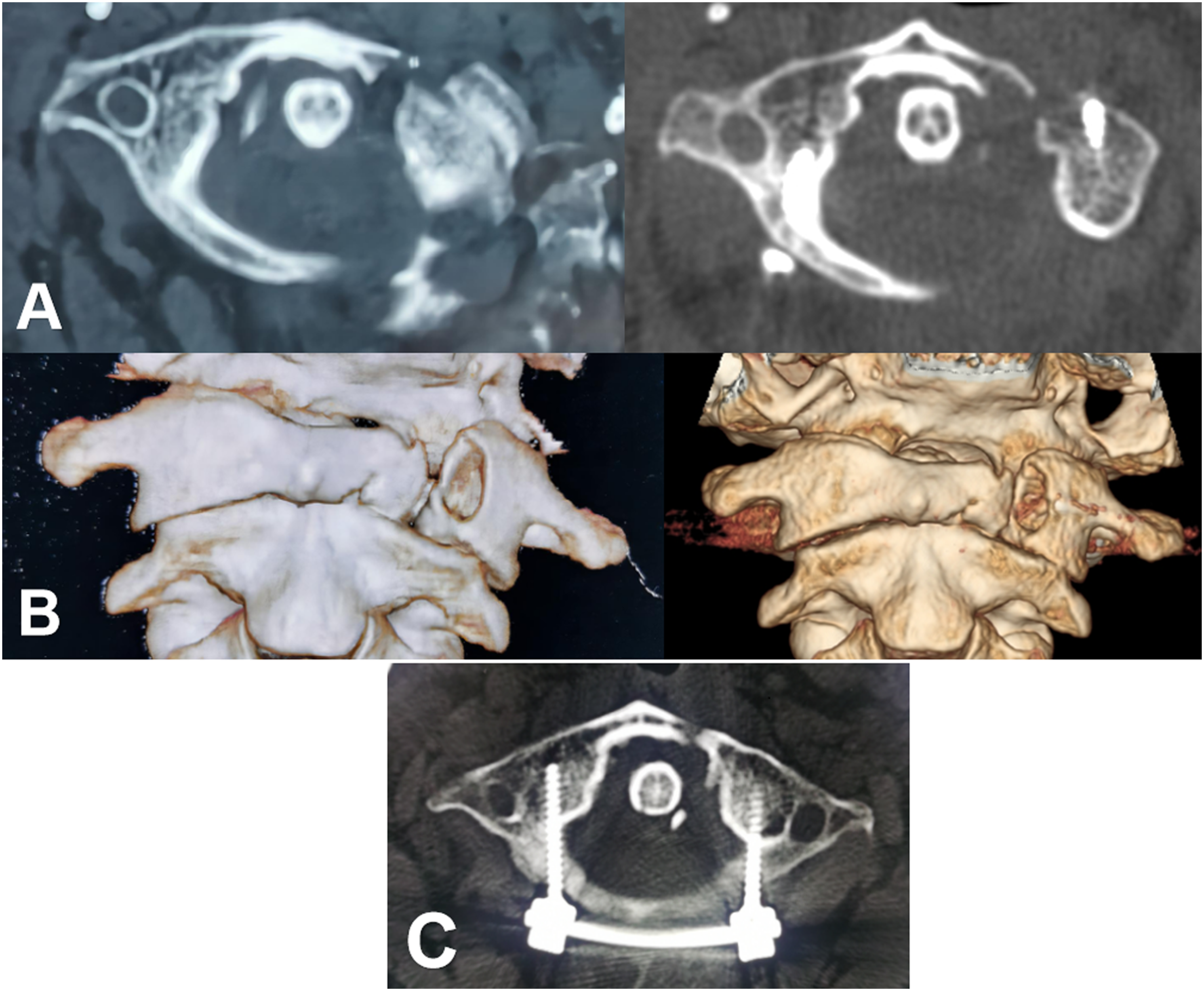
In our study, there were also 4 patients who were unable to achieve a good reduction of anterior arch fractures of the atlas due to the use of polyaxial screws (Figure 4). In a follow-up of at least 3 years, we found that patients who used polyaxial screws had a significant increase in LMD compared to monoaxial screws. Previous studies have also shown that posterior ORIF used polyaxial screws, and during the final compression, the anterior arch compression was often not ideal. The separation of the fracture of the anterior arch not only affected fracture healing but also led to an unsatisfactory recovery of LMD.1,25 At a later stage, we will also perform some biomechanical cadaver studies to verify this. (A) α repres ents an obtuse angle; the tail of the polyaxial screws swings. (B) β Angle is maintained at 90°; monoaxial screws can produce an adduction force. (A) 49 year-old male patient presented to our hospital with a neck injury caused by a heavy object. (A, B) Preoperative CT scan showed a fracture of the left anterior and posterior arch of the atlas, which was treated with a polyaxial screw-rod system for internal fixation. Three-month postoperative CT and three-dimensional reconstruction images revealed poor reduction of the anterior arch fractures of the atlas. (C) A CT image shows poor reduction of the anterior arch fracture 3 years later, showing sclerosis at the fracture end.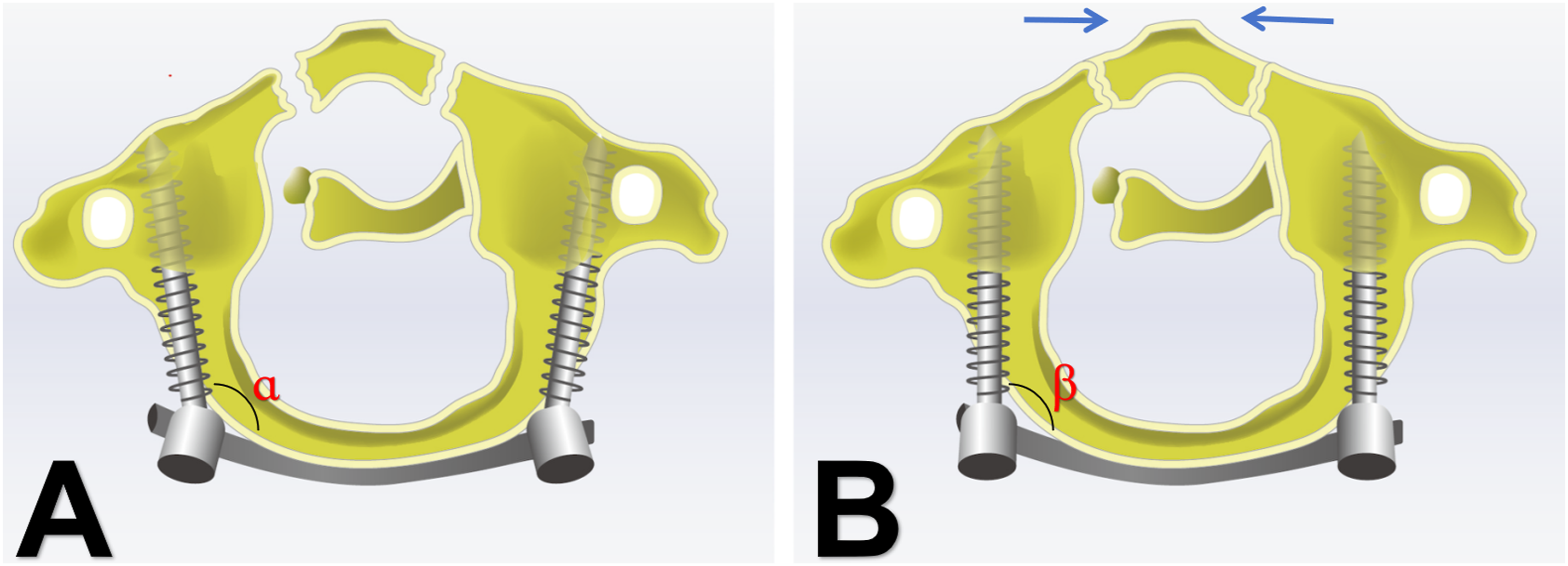
Monoaxial Screw-Rod System
To prevent the problem of poor reduction of the anterior arch fractures of the atlas, we modified this technique by using monoaxial pedicle screws for better reduction and possibly better stability. Based on the compression between the screws to reduce the posterior arch fracture, the locking screw process, because the monoaxial screw will not swing the head, so that the front of the screw produces an adduction force, so that the anterior atlas arch fracture is reduced (Figure 3(B)).
According to the results, the reduction effect of atlas anterior arch fractures by the monoaxial screw achieves an almost anatomical reduction. However, the posterior cervical screw-rod system, which is widely used today, has a high internal fixation notch. In addition, when a long-tail monoaxial pedicle screw is used for reduction, it is necessary to place the long-arm sleeve on the tail of the screw with a large swing angle to both sides to achieve lever reduction. Meanwhile, the assistant should hold on both sides of the screw with the compression pliers to maintain pressure and also prevent the rotation of the connecting rod. Therefore, this system is not only difficult to operate during surgery but also prone to injury to the atlantoaxial venous sinuses, which are prone to massive bleeding. The length of the connecting rods is also difficult to control, and they are often reworked for insufficient length or too long to stimulate the paravertebral muscles. Combined with the high notch at the tail of the screw, it is easy to lead to postoperative paravertebral muscle reduction difficulties, chronic bursitis, and neck pain. Intraoperative bending of the connecting rod is required in advance because, on the 1 hand, the rod can be attached to the posterior arch to avoid spinal cord compression, and on the other hand, the angle between the screw and rod can be an obtuse angle to produce a better compression effect on the anterior arch when tightening the screw plug. In the long term, there is a risk of compression of the spinal cord if the rod is rotated. In short, the monoaxial screw-rod system still has obvious shortcomings and high technical operation requirements.
Our results showed that the LMD in group B was lower than in group A at the last follow-up, which indirectly confirms that monoaxial screws have a better reduction effect. However, the mean VAS score for postoperative neck pain was lower in group A than in group B at multiple follow-ups, which may be related to the high profile of the monoaxial screw-rod system and intraoperative damage to the surrounding cervical tissues.
Comparison of Perioperative Indicators and Clinical Outcomes
In terms of perioperative clinical indicators, the operative time, blood loss, screw-rod system placement time, and hospital stay were all lower in Group A than in Group B, with statistically significant differences (P < .05). The reasons for this difference may include that in Group A, the use of polyaxial screws was more widespread, and the operation was simpler than that of monoaxial screws, with a significantly smaller range of trauma and relatively fewer complications. Due to the complex operation of monoaxial screws, 6 of our patients experienced postoperative greater occipital nerve neuralgia, 4 patients experienced occipitocervical discomfort and limited mobility, and 3 patients developed chronic bursitis. This may lead to the majority of patients with pain being unwilling to exercise, greatly increasing postoperative discomfort and prolonging bed rest and hospitalization times. After multiple follow-ups, we found that the average VAS score for postoperative neck pain in Group A was lower than that in Group B.
Our results showed that the physiological motor function of the atlantoaxial joint was preserved in both groups of patients with surgical fixation. Previous biomechanical studies had also confirmed that atlas burst fractures were caused by vertical axial violence and that even if the TAL was damaged, the other occipitocervical stabilizing structures (including some atlantoaxial lateral mass articular capsule, alar ligament, apical ligament, cruciate ligament-vertical portion, and cervical muscles) only lose tension due to the subsidence of the skull after the lateral mass of the atlas was moved to both sides.13,31 After the reduction of the atlas fracture, this axial tension can be reconstructed to restore the main stable structure of the occipitocervical region. Although the TAL has not been repaired, it can still maintain the stability of the occipitocervical region under physiological stress. The cervical NDI score, AADI, and ROM of the 2 groups of studies returned to normal in the last follow-up, and there was no statistically significant difference between the 2 groups.
There is a consensus that all intra-articular fractures must be anatomically reduced as far as possible. However, in the study of Group A, there were 4 patients whose anterior arch of the atlas was not well reduced, but the axial and flexion-extension movements of both groups basically returned to normal at the last follow-up, and the prognostic effect of both groups was satisfactory. Is it necessary to achieve an anatomic reduction in the upper cervical spine as possible? We may need to conduct biomechanical experiments with different degrees of reduction in the future to verify.
Treatment Strategies
Based on our treatment experience, polyaxial screws fixation is recommended for unstable fractures with minor displacement of the anterior arch of the atlas. Not only will the fracture be reduced better, but the patient will have fewer complications. For unstable fractures with large displacement of the anterior atlas arch, monoaxial screws treatment is recommended to achieve an almost anatomic reduction of the atlas anterior arch fracture. For patients with unstable atlas fractures with a single anterior arch fracture, monoaxial screws on 1 side of the anterior arch fracture and polyaxial screws on the other side may also be a feasible option.
At the same time, in order to achieve the ideal reduction effect, simplify surgical operation, improve surgical safety, and reduce surgical trauma, an effective reduction fixed instrument may provide a new treatment strategy. During the reduction process, based on a similar principle to monoaxial screws, some polyaxial screws can switch to monoaxial mode before final fixation of the screw to the rod, which may also be an optional implantation technique for treating unstable atlas fractures.
Limitations
The study has some limitations. The retrospective study design and the recruitment of patients from a single center are the main limitations of this study. The relatively small population size due to the rarity of this type of fracture may have reduced statistical significance to some extent, but in this study, all surgeries were performed by the same surgeon, fully demonstrating the effectiveness of the surgery. More prospective and multicenter studies with larger sample sizes should be conducted in the future to obtain imaging and clinical outcomes in patients with unstable atlas fractures treated with 2 different surgical fixation methods. Nevertheless, we hope that the results of this study will be useful in the treatment of patients with unstable atlas fractures.
Conclusion
In conclusion, both polyaxial and monoaxial screw-rod system posterior osteosynthesis are effective techniques for the treatment of unstable atlas fractures. The use of the polyaxial screw-rod system is superior to the monoaxial screw-rod system in terms of operation time, blood loss, time of screw-rod system placement, hospital stay, and VAS. In terms of reduction rate and LMD of fracture, the monoaxial screw-rod system is obviously superior. The monoaxial lateral mass screw-rod system could achieve a near-anatomic reduction of unstable atlas fractures, especially anterior arch fractures of the atlas, but it has more complications. There was no significant difference between the 2 in terms of ROM, AADI, and NDI of the cervical spine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Research Projects in Colleges and Universities of Anhui Province (KJ2019A0242) and Anhui Institute of Translational Medicine (2021zhyx-C34).
Institutional Review Board
All the patients collected in this study signed the patient consent forms. And this study was approved by the Institutional Review Board of the first affiliated hospital of Anhui Medical University, Hefei, China.