
Abstract
Study Design
Narrative review.
Objectives
This article aims to provide a narrative review of the current state of research for liquid biopsy in spinal tumors and to discuss the potential application of liquid biopsy in the clinical management of patients with spinal tumors.
Methods
A comprehensive review of the literature was performed using PubMed, Google Scholar, Medline, Embase and Cochrane databases, and the review was limited to articles of English language. All the relevant articles which were identified to be related to liquid biomarker study in spinal tumors, were studied in full text.
Results
Liquid biopsy has revolutionized the field of precision medicine by guiding personalized clinical management of cancer patients based on the liquid biomarker status. In recent years, more research has been done to investigate its potential utilization in patients with tumors from the spine. Herein, we review the liquid biomarkers that have been proposed in different spine malignancies including chordoma, chondrosarcoma, Ewing sarcoma, osteosarcoma, astrocytoma and ependymoma. We also discuss the wide window of opportunity to utilize these liquid biomarkers in diagnosis, treatment response, monitoring, and detection of minimal residual disease in patients with spinal tumors.
Conclusions
Liquid biomarkers, especially blood-derived circulating tumor DNA, has a promising clinical utility as they are disease-specific, minimally invasive, and the procedure is repeatable. Prospective studies with larger populations are needed to fully establish its use in the setting of spinal tumors.
Keywords
Introduction
In the last decade, precision medicine has emerged as an innovative approach in which the diagnostics and treatments are tailored to individual patients based on their unique genetic and physiologic characteristics. The application of precision medicine relies on an in-depth understanding of the tumor profile and its molecular characteristics. 1
Tissue biopsy is the gold standard method to obtain a sample of tumor in order to assist with diagnosis and molecular characterization. 2 Yet, tissue biopsy remains a somewhat invasive procedure, and the biopsy area may only represent a small geographic portion of a heterogenous lesion. In addition, repeated sampling of the tumor is generally not acceptable. 3 In this context, liquid biopsy has become an important tool for precision oncology in the current clinical realm. Liquid biomarkers can be identified non-invasively from a myriad of body fluids such as blood (plasma or serum), cerebrospinal fluid (CSF), urine, saliva, pleural fluid, ascitic fluid and breast milk. 4 The liquid biopsy, especially through identification of blood-based biomarkers, has demonstrated utility as a non-invasive and repeatable diagnostic test. The widespread use of liquid biopsy in the oncology setting relies heavily on the development of comprehensive genomic profiling assays. 5
The development of a liquid biopsy for spine tumors is challenging. Spinal neoplasms represent a molecularly heterogenous group of tumors with varied genetic makeup. The incidence of tumors of the spine is far lower than more common cancers such as those involving the lung or colon, and to this end have arguably been under-funded and under-studied, even though they carry significant morbidity and mortality. 6 Furthermore, as it is often challenging to measure biomarker molecules that are in low concentration in the biofluids, decades of biomedical research have focused on refining the methodologies and techniques in order to detect liquid biomarkers sensitively without compromising the specificity.
In this narrative review we discuss the current state of the research, focusing on the liquid biopsy in spinal tumors. We provide an overview of the research efforts that have been performed in chordoma, chondrosarcoma (CS), osteosarcoma (OS), Ewing sarcoma (EWS) and ependymoma/astrocytoma. Of note, the literature investigating the role of liquid biopsy for CS, OS and EWS is largely derived from the appendicular musculoskeletal oncology literature. We also elaborate on the potential future applications of these biomarkers. The aim of this paper is to generate awareness and galvanize interest about these novel technologies and encourage future clinical trials to bring these technologies into the clinical realm.
Materials and Methods
This study was performed in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. 13
Literature Search
An online search was performed by authors RCM and SKT on in the PubMed/Medline, EMBASE, and Web of Science databases. Publications available on March 30, 2023 were reviewed. No limits on publication dates or languages were applied. The searches were performed for each specific primary tumors: chordoma, chondrosarcoma, osteosarcoma, Ewing sarcoma and ependymoma/astrocytoma. Each individual pathology was searched in combination with the following keywords: liquid biopsy, circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), circulating cell free DNA (cfDNA). For ependymoma/astrocytoma, the search included the additional following keywords: cerebrospinal fluid (CSF) biomarkers, CSF CTCs and CSF ctDNA.
Inclusion and Exclusion Criteria
Eligible studies included patients with the following tumors: chordoma, chondrosarcoma, osteosarcoma, Ewing sarcoma and ependymoma/astrocytoma. Studies specifically investigating the role of liquid biopsies were included. The following type of studies were excluded: abstracts; editorials or commentaries; systematic reviews; and narrative reviews.
Study Selection
Studies were screened based on their title and abstract for potential eligibility based on our inclusion criteria. All potentially relevant studies were downloaded, and full texts reviewed.
Primary and Secondary Questions
The primary question was to review the current state of the literature on liquid biopsy for primary tumor of the spine. The secondary aims were to review the various types of liquid biopsy and their potential clinical applications.
Analysis
A narrative review was performed. Informed consent or Institutional Review Board approval were not required due to the nature of the study.
Results
Type of Biomarkers
Circulating Tumor Cells
The first circulating tumor cell (CTC) was discovered in 1869 from the blood of a metastatic cancer patient. 7 CTCs have a median half-life of approximately 1-2.5 h and are released into the blood from either the primary tumor site or any metastatic site. 8 The concentration of CTCs in blood is generally very low, with a range of only 1-10 CTCs per ml of blood, even in patients with metastatic disease. 9 Given the low abundance of CTCs, highly sophisticated isolation technologies are required to identify them, which can limit throughput and increase cost. 10 When single cell genomic analysis is performed on a single CTC, huge variability and heterogeneity are observed among different cells. 11 This means that a blood sample may contain multiple subpopulations of tumor cells and the analysis of a single CTC is not a comprehensive representation of the overall tumor biology. 12 Thus, to date CTCs have had limited clinical utility for most tumors, especially in the diagnosis of early stage cancers or in assessing for minimal residual disease (MRD).
Cell-Free DNA and Circulating Tumor DNA
Genome-wide sequencing of various tumors has identified specific somatic mutations that are harbored by different types of malignancies.
13
Circulating tumor DNA (ctDNA), a subpopulation of cell-free DNA (cfDNA) that is derived from neoplastic cells, are short DNA fragments (70-200 base pairs) which carry the tumor somatic mutations in the circulation.14–16 ctDNA is released into the bloodstream by dividing, necrotic or apoptotic tumor cells, and thus can be used to track the dynamic changes during tumor progression (Figure 1).
16
Its half-life is short (between 15 min to 2.5 h) and its concentration in the blood ranges from 0 ng/mL to 1000 ng/mL.15,17,18 The concentration of ctDNA is higher in metastatic patients than in patients with localized disease.
19
Of the liquid biopsies, the ctDNA is the most investigated and has been shown to have accurate representation of the tumor characteristics. It has been used in the setting of a variety of tumors such as colorectal, ovarian, lung, oropharyngeal, prostate, pancreatic, breast and melanoma.20–26 A schematic diagram of the different clinical stages where a liquid biopsy can be potentially utilized in patients with spinal tumors.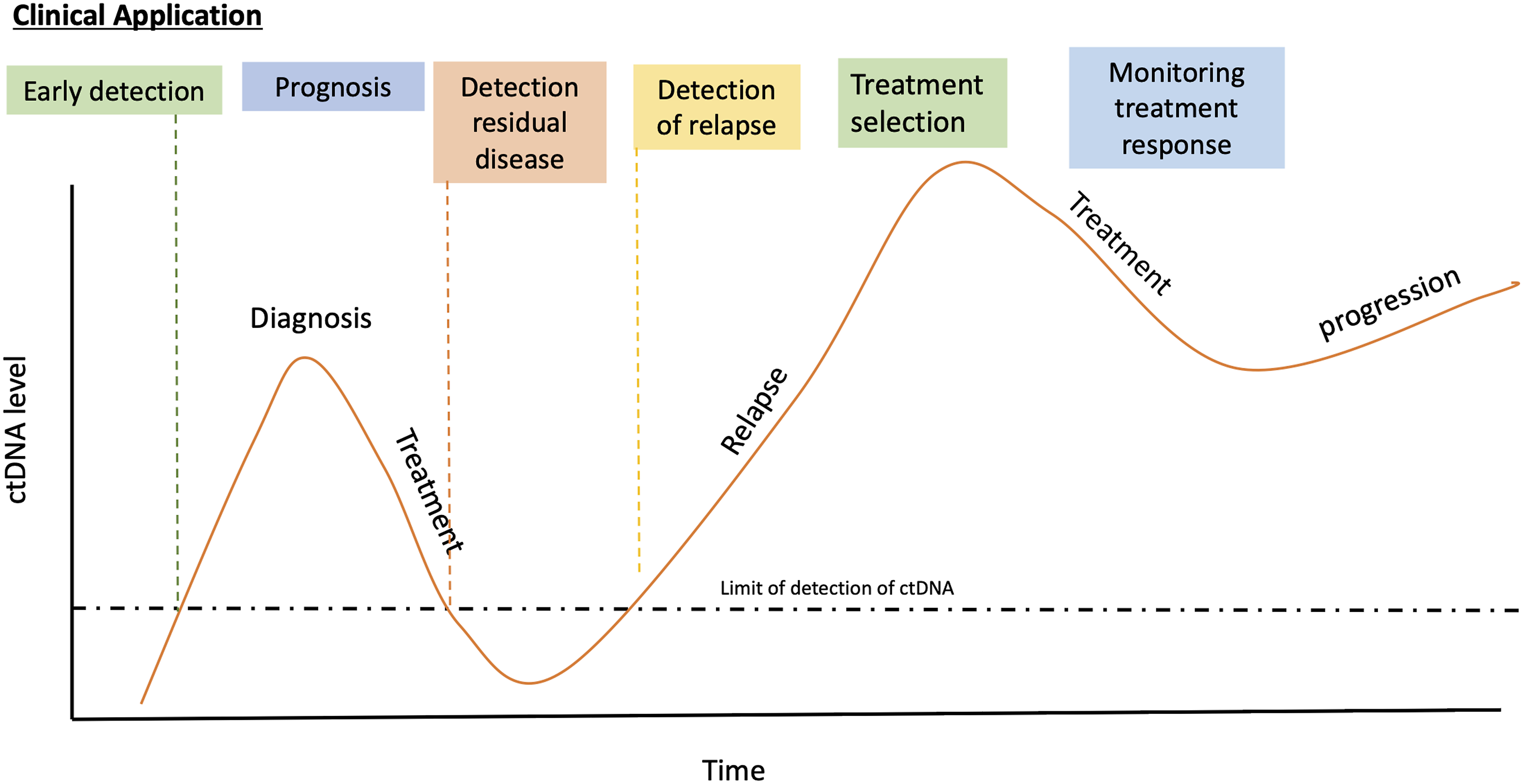
Many different technologies have been developed to assess clinically-relevant molecular alterations. These can be divided into two broad categories: the polymerase chain reaction (PCR) methods and Next Generation Sequencing (NGS) methods. PCR relies on the development of DNA probes that specifically target known mutations. Some of the commonly used PCR methods are real-time quantitative PCR (qPCR), digital PCR (dPCR) and droplet digital PCR (ddPCR). Different PCR-based sequencing methods that work with low amount of DNA, such as Safe-Sequencing System (Safe-SeqS) and Repetitive Element AneupLoidy Sequencing System (RealSeqS), have been developed to accurately identify the rare variants in ctDNA while minimizing errors.27,28 The PCR-based assays are sensitive and convenient, but they can only target a limited number of known molecular alterations. 29 For example, dPCR assays have been developed for chondrosarcomas as these tumors often carry canonical IDH1 or IDH2 mutations. 30 This type of assay generally provides a high sensitivity and specificity, but is not applicable to tumors like chordoma which do not have a recurrent gene signature that is easily identifiable. A second approach is to develop a tailored PCR assay based on the specimen tumor profiling. These assays are patient-specific, and they provide a high sensitivity. The NGS technology is a high throughput DNA sequencing method that relies on massive parallel sequencing of millions of different DNA fragments and can be used to identify known or unknown molecular alterations. Since this is a disease-independent method to examine tumor agnostic somatic events (for example, copy number changes), this approach has a higher discovery value.
Although blood-based ctDNA detection has been the most extensively investigated, ctDNA in CSF also has great potential. CSF may be used as liquid biomarker in malignancies of the central nervous system (CNS) and spinal cord tumors due to the vicinity of these tumors to CSF.31–33
Other Biomarkers
Cell-free RNA (cfRNA), including micro-RNA (miRNA) and long non-coding RNA (lncRNA) are also actively investigated as new potential liquid biomarkers in cancer biology.34–36 In addition to being a representation of gene expression, cfRNA could inform the more complex underlying pathogenesis process such as alternative splicing or A-to-I RNA editing, providing a more comprehensive understanding of the tumor. 35 Furthermore, extracellular vesicles such as exosomes have also been shown to be means of communication between tumor cells and other parts of the body cells, this can be utilized as biomarkers when detected in the peripheral circulation.37,38 Circulating protein and metabolites are also good biomarker sources, but the stability of these molecules remains a challenge to be fully optimized for liquid biomarker assay development.
Current State of the Research
Summary of the Findings for the Liquid Biopsies in Primary Spinal Tumors.
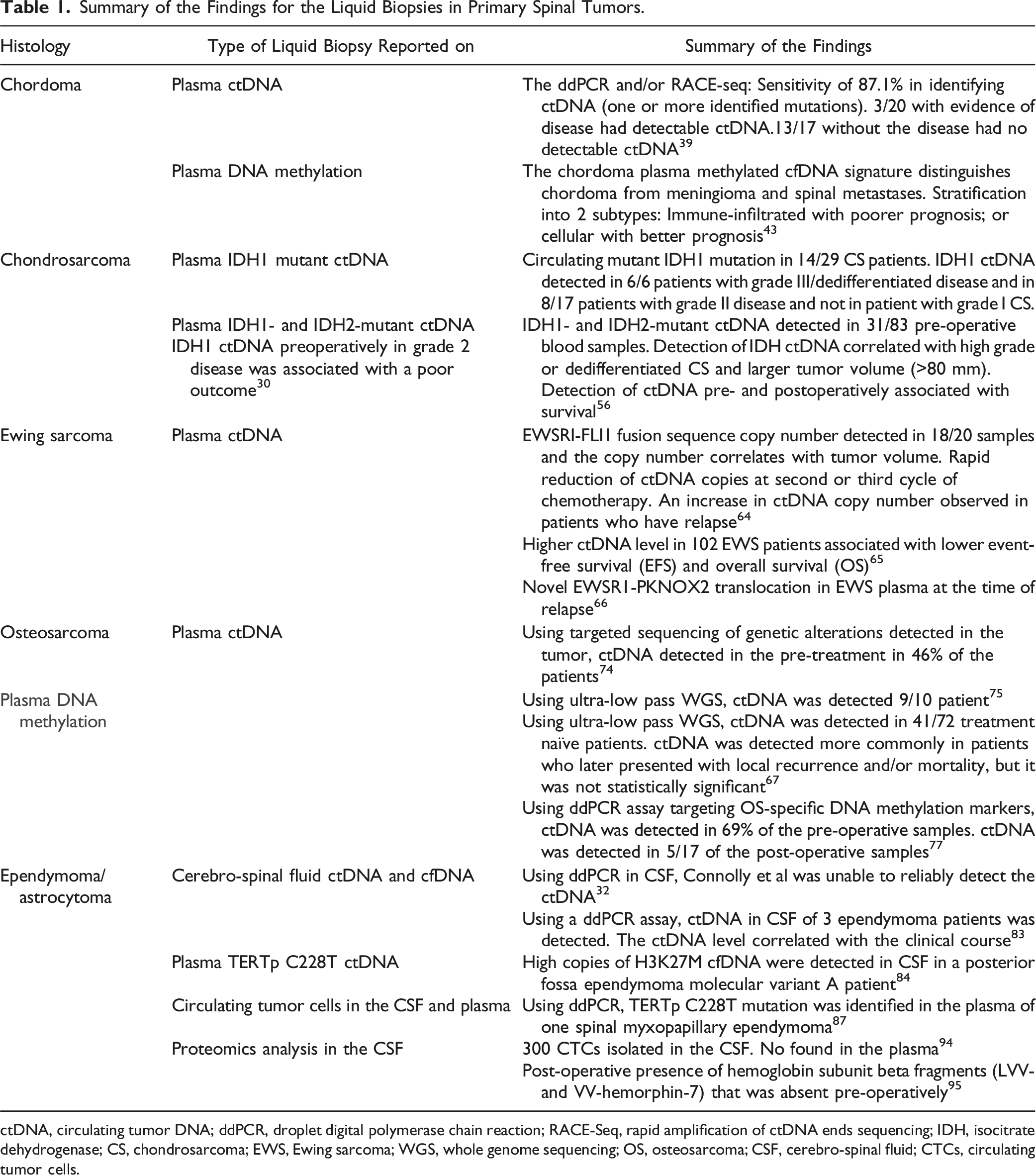
ctDNA, circulating tumor DNA; ddPCR, droplet digital polymerase chain reaction; RACE-Seq, rapid amplification of ctDNA ends sequencing; IDH, isocitrate dehydrogenase; CS, chondrosarcoma; EWS, Ewing sarcoma; WGS, whole genome sequencing; OS, osteosarcoma; CSF, cerebro-spinal fluid; CTCs, circulating tumor cells.
Chordoma
Chordoma is a rare primary bone tumor arising from remnants of embryonic notochord. 39 It affects approximately 300 individuals in the US annually. 40 The typical age group presentation is 40 to 60 years old with higher prevalence in men than women. 39 This tumor is often managed with aggressive surgical resection (en bloc resection if feasible) with the possible addition of neoadjuvant or post-operative radiation to minimize recurrence rate, but the recurrence rate of this very infiltrative tumor remains high with the median progression free survival of only 5 years. 41 The key in treating chordoma is to identify the patient population that has the highest chance of recurrence, as adjuvant treatment may be considered (post-operative radiotherapy and/or chemotherapy). The current clinical practice involves performing pre-operative tissue biopsy to confirm the diagnosis which theoretically could be accompanied with an increased risk of tumor seeding and spreading. 39 Further, tissue biopsies often cannot easily be performed in cases of clival chordoma. Therefore, a non-invasive method to diagnose chordoma is needed.
Understanding the genetic information of chordoma is essential in guiding therapeutic treatment. For example, the presence of 1p36 and p21 deletions suggest that patients with skull base chordoma would experience minimal benefits from radiation therapy. 42 SNP rs32305089 in the brachyury gene has also been shown to be highly sensitive and specific to differentiate chordoma from other chondroid tumors, which have different management and prognosis. 41 In addition, mutations in the promoter region of hTERT are found in approximately 10% of spinal chordomas and may identify patients with improved overall prognosis (30976795). However, detection and application of these mutations in the peripheral circulation remains elusive.
In a cohort of 32 chordoma patients at a single institution, Mattox et al 39 first identified the somatic mutation in chordoma tumors by whole exome sequencing, and later performed ddPCR and/or rapid amplification of ctDNA ends sequencing (RACE-Seq) to quantify the ctDNA mutation in the matched plasma. They demonstrated that the chordoma patients with positive plasma ctDNA were more likely to have higher mutant allele fractions (MAF) detected in the corresponding primary tumor. Three hundred and seventy-nine (379) somatic mutations were identified in the chordoma tumor, with most of the recurrent mutations occurring in epigenetic regulation genes such as ARID1A, ARID1B and PBRM1 in at least a quarter of the tumors sequenced. The ddPCR and/or RACE-Seq assays had a sensitivity of 87.1% in identifying ctDNA based on one or more identified mutations. Three out of 20 chordoma patients had evidence of radiographic disease at the follow up blood draw, and one or more mutations was identified in all the plasma samples at various timepoints, suggesting 100% positive predictive value and 0% false negative rate. In the 17 patients who had no radiographic recurrence, 13 had no detectable patient-specific mutation, demonstrating specificity of 76%. The authors also showed that the ctDNA level correlated with radiographic tumor remission or recurrence in 2 cases, suggesting significant potential of ctDNA as a reliable tool for spinal chordoma disease monitoring. This study is limited by the relatively small cohort that presented with recurrent disease and thus warrants further investigation.
DNA methylation signatures have also been shown to be helpful in primary CNS tumor classification. The largest chordoma methylation signature study was recently performed by Zuccato et al 43 using 69 chordoma tumor and matched plasma from three international centers. Using cfMeDIP-seq method, they found a high correlation between the chordoma tumor methylation values and the corresponding plasma cfMeDIP-seq signals. The chordoma plasma methylated cfDNA signature can reliably distinguish chordoma from meningioma and spinal metastases, with mean area under the ROC curve of .84 (95% CI: .52-1.00). The chordoma plasma methylome can be used to stratify chordoma patients into two subtypes with different prognosis: cluster 1 (immune-infiltrated) with poorer prognosis; or cluster 2 (cellular) with better prognosis. The ability to subtype chordoma based on a methylated cfDNA signature could impact clinical management, however further investigation is warranted.
Chondrosarcoma
Chondrosarcomas (CSs) are a heterogenous group of cartilaginous tumors with variable malignant potential. CS occurs in 1 out of 1 000 000 patient annually, of which 6.5%-10% will arise in the mobile spine and 5% in the sacral region. 44 CS most conventionally presents in patients in their fourth through sixth decade of life. CS can be either primary or secondary when it arises from a previous lesion (enchondroma or osteochondroma). Patients with enchondromatosis (e.g. Ollier disease, Mafucci syndrome) are at higher risk of malignant transformation (15%-30%) and those presenting with multiple hereditary exostosis (MHE) are also at slightly higher risk of malignant transformation (1%-3%).45,46 The histologic grading of conventional CS is challenging and relies on the cellularity, number of mitoses, matrix characteristics and degree of cellular atypia. Additionally, the interaction between the lesion and the host bone can assist in determining the degree of malignancy. A previous study has demonstrated a poor interobserver reliability between the radiologist and pathologist in grading cartilaginous tumors.47,48
Isocitrate dehydrogenase (IDH) is an enzyme of the Krebs’s cycle which catalyzes isocitrate to α-ketoglutarate. It was reported that approximately 50% of CSs overexpress IDH1 or IDH2. 49 IDH1 and IDH2 mutations present with similar frequencies among benign and malignant cartilage tumors. 50 Importantly, IDH1/IDH2 mutations are associated with shorter overall survival in CS patients. 51 Recently, Zhu et al 49 reported that while IDH1/IDH2 was not associated with overall survival, these mutations were correlated with longer relapse-free and metastasis-free survival in high-grade CSs. Other genetic alterations identified in CS include: COL2A1 (37%), TP53 (20%), RB1 pathway (33%), and Hedgehog pathways (18%).52–54 Additionally, TERT promoter mutation was found to be associated with higher-grade CS. 55
To investigate the potential use of IDH1/IDH2 as blood biomarkers, Gutteridge et al 30 developed ddPCR assays for the detection of wild type and all common IDH1 mutations (R132C, G, H, L and S). The group was able to detect and quantify circulating mutant IDH1 mutation in 14 out of 29 CS patients. Additionally, it showed a clear correlation with tumor grade. IDH1 ctDNA was detected in all patients with grade III and dedifferentiated disease (n = 6) and in 8/17 patients with grade II disease, but not observed in patient with grade I CS. Detection of mutant IDH1 ctDNA preoperatively in grade 2 disease was associated with a poor outcome. Subsequently, the same group led a multicentric prospective study to investigate IDH1- and IDH2-mutant ctDNA as well as GNAS hotspot mutation (as CS may occur in a small proportion of patients with fibrous dysplasia). 56 Of the 104 patients, they excluded 21 patients with tumors that did not express the mutations of interest. IDH1/IDH2 ctDNA was detected in 37% (31/83) of the pre-operative blood samples. Similar to their previous finding, the detection of IDH ctDNA was correlated with high grade or dedifferentiated CS but it was also associated with larger tumor volume (>80 mm). The detection of ctDNA pre- and postoperatively was correlated with survival. Of note, all patients (n = 11) who had persistent ctDNA post-operatively developed a relapse (recurrence or metastasis). Altogether, these findings suggest that the detection of IDH1/IDH2 hotspot mutation in patient blood predicts the disease aggressiveness and is a negative prognosis factor in CS.
Ewing Sarcoma
Ewing sarcoma (EWS) is the second most common primary bone tumor and almost half of all the EWS patients are diagnosed as adolescents. 57 Neoadjuvant chemotherapy with a multi-agent regimen is standard of care for EWS patients. 57 En bloc resection (complete surgical excision in a single piece) is the best modality to achieve local control.58,59 Intralesional resection should be avoided as there is no benefit compared to radiation therapy alone. 59 Radiation therapy alone as the definitive treatment should be considered when resection is not deemed possible. 60 Approximately 85%-90% of EWS harbor EWSR1 chromosomal translocation t (11;22) (q24;q12), producing the EWS-FLI1 fusion protein; and the remaining 10% of EWS has EWSR1-ERG products. 61 Refinement in EWS diagnostics have recently identified entities that are now regarded as distinct cancers. These include the round cell sarcoma with EWSR1-non-ETS fusion, CIC-rearranged sarcomas and the sarcomas with BCOR alterations. 62
In 1995, a study by Peter et al 63 showed that the EWSR1 rearrangement can be detected by reverse transcriptase-polymerase chain reaction (RT-PCR) followed by nested PCR in the peripheral blood. Almost a decade later, Krumbholz et al 64 validated and reported that ctDNA using EWSRI-FLI1 fusion sequence copy number can be detected in 18 of 20 plasma samples and the copy number correlates with tumor volume. In the EWS follow-up patients, they also observed a rapid reduction of ctDNA copies in the majority of the patients at the start of second or third cycle of chemotherapy. An increase in ctDNA copy number was also observed in patients who experienced relapse. In a more recent study by the same author, higher ctDNA level in 102 EWS patients was correlated with lower event-free survival (EFS) and overall survival (OS). 65 In addition to its potential use as a prognostic biomarker, the ctDNA analysis also revealed novel EWSR1-PKNOX2 translocation in EWS plasma at the time of relapse. 66 Although chromosome translocation is well recognized as a driver of cancer, the role of this translocation is still unexplored.
Using a NGS hybrid capture assay and an ultra-low pass whole-genome sequencing (WGS) assay, Shulman et al 67 also showed that more than half (53%) of 94 patients with newly diagnosed EWS had detectable ctDNA. The detection of ctDNA in localized EWS portends worse 3-year event free survival. Similar results were reported by Shah et al, 66 who showed that ctDNA can be used as predictive biomarker for relapse in EWS. Altogether, these findings suggest the high potential of ctDNA as a liquid biomarker for EWS patients.
Osteosarcoma
Osteosarcoma (OS) is the most common primary malignant bone tumor in childhood and adolescent but is rarely encountered in the spine (between 3%-5% of all spine malignancies).68–70 The treatment of OS is multimodal and generally involves a combination of surgery and chemotherapy. The 5-year survival is roughly 70% and nearly 30%-40% of patients with OS will succumb to disease. 71 OS has a complex genome caused by extensive chromosomal rearrangement that frequently affect RB1 and the p53 pathway. 72
In 2010, McBride et al published the first report to detect ctDNA using qPCR in an OS patient with known genomic alterations. 73 Using targeted sequencing of genetic alterations detected in tumors from 10 OS patients, Barris et al 74 reported that ctDNA was detected in the pre-treatment blood in approximately half of the patients (46%). With refinement of technologies and using ultra-low pass WGS, ctDNA was detected in the blood of treatment naïve patients in 57% (41/72) and 90% (9/10) of cases.67,75 Shulman et al observed that ctDNA in OS was detected more commonly in patients who later presented with local recurrence and/or mortality, but this did not reach statistical significance.
DNA methylation is an epigenetic modification that plays an important role in regulating gene expression. The cancer genome is often characterised by global hypomethylation and focal hypermethylation, leading to genomic instability and transcriptional repression. 76 Lyskjær et al 77 investigated the application of methylation-based biomarkers to detect ctDNA in patients with OS. Through a personalized ddPCR assay targeting OS-specific DNA methylation markers, ctDNA was detected in 69% of the pre-operative blood sample. ctDNA was detected in 5/17 (29%) post-operative plasma samples from patients, which in four cases were associated with or preceded the disease relapse. ctDNA detection in OS patients also significantly predicted overall survival. Thus, ctDNA has tremendous potential for application in OS, particularly in monitoring tumor response to chemotherapy and may be translated into an individualized chemotherapy regimen in the future.
Ependymoma/Astrocytoma
Ependymoma, when it occurs in the spinal cord, is an intramedullary-intradural tumor that arises from ependymal cells of the central canal of the spinal cord, constituting approximately 15% of all spinal cord tumors. 78 While the recurrence rate of ependymoma can be diminished by 90%-100% if gross total resection (GTR) is performed, higher grade tumors usually have unclear margins, rendering GTR without postoperative deficits very difficult.79,80 The patients who receive subtotal resection are then closely monitored by MRI for recurrence, but the sensitivity of this imaging modality is very limited, especially in those with microscopic residual disease. 81 A less invasive method is needed to understand the genetic basis of ependymoma and to aid in determining recurrence and/or resistance to treatment.
cfDNA from CSF has been utilized for liquid biomarker development in intramedullary spinal ependymoma because it has reduced background noise as compared to plasma cfDNA. In a cohort of 3 patients with grade 2 spinal ependymomas, Connolly et al 82 was unable to reliably detect the ctDNA using ddPCR in CSF of these patients. They suggested that (1) the anatomical location of this tumor could have limited the diffusion of cfDNA into the CSF, and (2) lower ctDNA abundance is available overall due to the lower grade tumor investigated. 32 However, Kojic et al detected ctDNA in CSF of 3 ependymoma patients, similarly using a ddPCR assay. The ctDNA level correlated with the clinical course. 83 A study by Zaytseva et al 84 later demonstrated that high copies of H3K27M cfDNA were detected in CSF in a posterior fossa ependymoma molecular variant A patient, most likely due to the proximity of this tumor to the fourth ventricle. Identification of MYCN amplified spinal ependymomas, which carry an aggressive clinical course, would be critical in precision management of patients.85,86 Telomerase-reverse transcriptase gene promoter (TERTp) mutations have been reported to be high in a subset of ependymoma, termed spinal myxopapillary ependymoma (SP-MPE). 87 Deniel et al 87 reported a case of SP-MPE in which TERTp C228T mutation was identified in the plasma using ddPCR. Although genome-wide DNA methylation signatures and TERT promoter methylation marks are established epigenetic alterations in ependymoma, their translational potentials as liquid biomarkers are still not fully explored. 88
Astrocytoma comprises 30%-40% of intramedullary spinal cord tumors and it is the most common pediatric intramedullary tumor. 89 Although genetic alterations including von-Hippel Lindau (VHL) and neurofibromatosis (NF) type 1 and 2 have been consistently reported in hereditary subgroups of spinal astrocytoma, these aberrations are rarely detected in sporadic cases. 90 Genetic mutations found in intracranial astrocytoma often do not translate to the counterpart spinal tumors. 90 In order to better understand astrocytoma molecular profiles, Zhang et al 90 performed whole exome sequencing (WES) on 16 astrocytoma tumor samples (2 glioblastoma, 2 anaplastic astrocytoma, 5 grade II astrocytoma and 7 pilocytic astrocytoma) and WGS on 3 astrocytoma (2 pilocytic astrocytoma and 1 grade II low grade glioma). Very few somatic mutations were detected in this cohort of intramedullary astrocytomas; none of the common mutations encountered in intracranial astrocytoma were found (H3F3A, IDH1/2, BRAF, PTEN or CDKN2A/B).90–92 The absence of recurrent genetic aberrations in spinal astrocytoma as compared to intracranial astrocytoma could suggest that an alternative pathway is responsible for the development of these intramedullary tumors. A recent study by Biczok et al 93 found H3F3A mutations in 5/26 spinal astrocytomas; homozygous CDKN2A/B and ATRX mutations in a subgroup of high-grade spinal astrocytomas with piloid features; and PIK3CA mutations in more than half of spinal pilocytic astrocytomas (rare for pilocytic astrocytoma outside spinal cord). Due to the rarity of this tumor, more work needs to be done to identify the tumor biomarkers before we can successfully translate it into the liquid biopsy realm.
Without the restriction of the blood-brain barrier, it is believed that CTCs can be detected at higher amounts in CSF than in blood, suggesting a role for CTCs in biomarker detection of ependymomas. In 2020, Zhao et al 94 reported more than 300 CTCs were isolated from CSF of patients with anaplastic ependymoma, while minimal amounts could be detected in the blood. Proteomics analysis of 3 CSF samples of ependymoma patients also revealed that the hemoglobin subunit beta fragments (LVV- and VV-hemorphin-7) were absent before surgery but present after surgery. 95 This further demonstrates that CSF samples can be used as another important source of liquid biopsy in primary CNS tumors and highlights the potential for this to be combined in a multi-analyte assay for better sensitivity.
Discussion
Clinical Application
Liquid biopsy has a tremendous potential to be applied in the clinical management of spine tumors. Investigations to date have focused mainly on technological developments and proof-of-concept; larger clinical studies are required in order to accelerate the translation of this research into clinical care. There are multiple potential applications of the liquid biopsies: diagnostics, prognosis, treatment response and monitoring and detection of minimal residual disease (MRD) (Figure 2). However, the low tumor burden that is frequently observed with spinal tumors has limited the widespread application of this liquid biopsy. Lastly, as with any laboratory value or genetic marker, studies with large data are subject to great uncertainty. Not every correlation has causality and the markers found for a particular should also be logically related to the underlying disease. An example of a chordoma case. (A) Patient presenting with a C3-C4 and C5 chordoma treated with en bloc resection in 2019. (B) Local recurrence at C2 in 2022.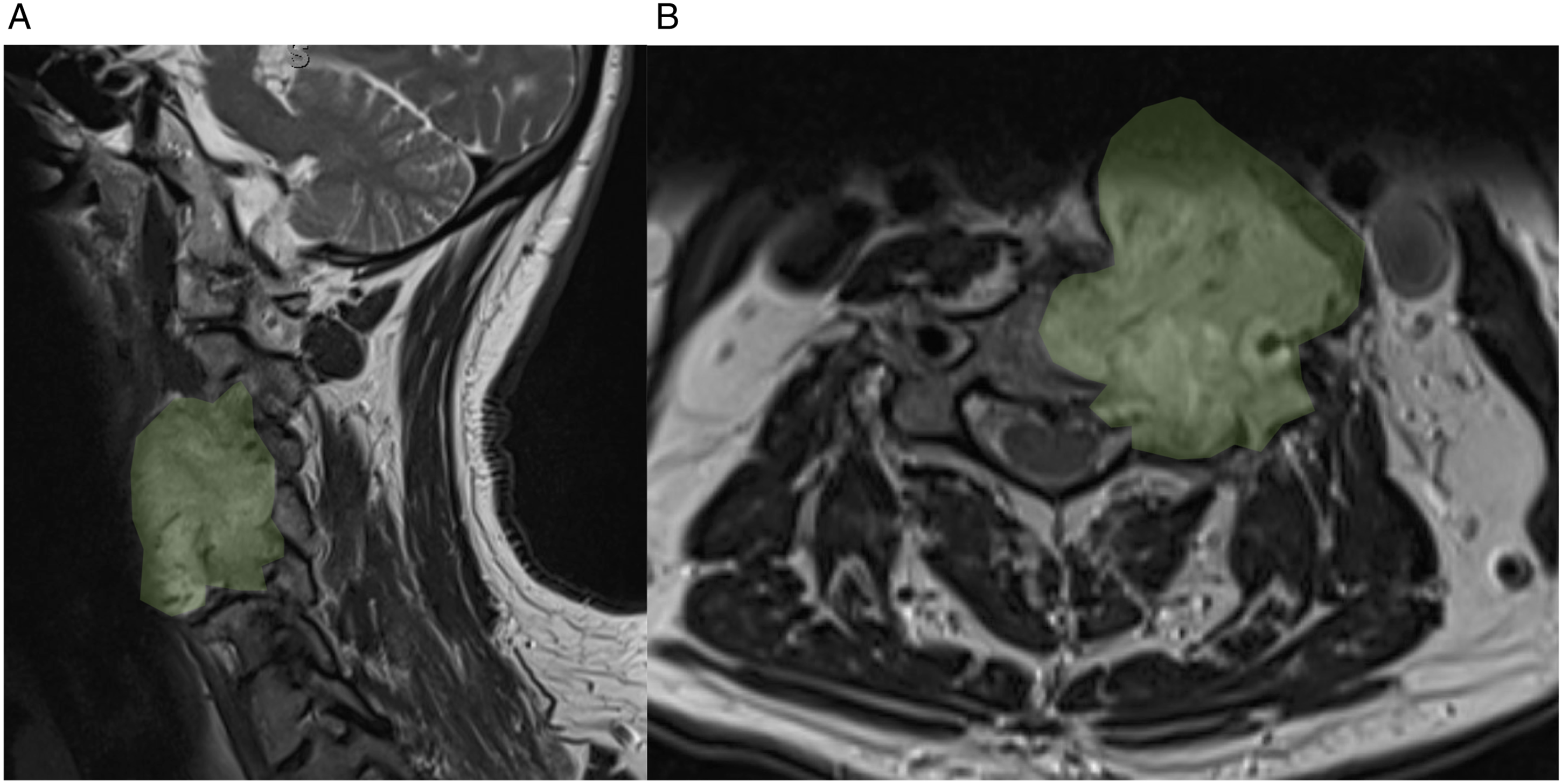
Diagnostics and Prognosis
The use of ctDNA biopsy has been heavily investigated for the early detection of solid cancers. For example, Cohen et al 96 demonstrated the ability to detect 8 different cancers (ovary, liver, stomach, pancreas, esophagus, colorectum, lung, or breast) with a specificity of >99% and a sensitivity of 68%-98% using the CancerSEEK platform. It would be highly valuable to develop such a tool for the spinal tumor population, especially for lesions that are difficult to biopsy. Because of the heterogeneity of this population and the absence of a clear molecular signature for some of these tumors, it is challenging to develop a broad blood assay that will provide a rapid diagnosis for all spinal tumors. However, the use of liquid biopsy with a targeted panel can still benefit this patient population (e.g., by differentiating high vs low grade CS). 56
While it remains supported by many small studies, the growing body of literature in the spinal tumor population suggests that the presence of ctDNA prior to any treatment is a negative prognostic factor. 30 In a soft tissue and bone sarcoma study of 64 patients, it was recently demonstrated that a cfDNA of <6 ng/ml at presentation was associated with improved disease-free survival. 97 The role of ctDNA needs to be further characterized; it will likely help guide selection of adjuvant treatment in the near future.
Treatment Response Evaluation/Monitoring
Surveillance imaging is often used to detect local recurrence and monitor treatment response. In the spine, the quality of post-operative imaging is commonly affected by the use of spinal implants, rendering assessment of local control difficult. ctDNA could be used as a repeatable personalized tumor-specific marker as the half-life of ctDNA is short and can mirror the tumor burden in a more acute setting. Although limited tumor shedding (low concentration of ctDNA) could be an issue, repeated liquid biopsy over time may offer the clinician a dynamic “real-time” evolution of the tumor. It has been demonstrated in several cancer types that the level of ctDNA will change depending on tumor response, and this can be observed before it is detected on surveillance imaging.98–101 Local recurrence or tumor progression has been reported as detectable by the liquid biopsy for chordoma, CS, OS and EWS.56,66,77
Residual Disease Detection
Determining the extent of tumor resection (residual disease) is extremely challenging. The conventional method to determine the completeness of resection involves the surgeon and pathologist examining the resected specimen and determine if the margins are free of tumor. However, this method is inherently unreliable as the entire margin of the tumor cannot be feasibly examined histologically. Thus, a liquid biopsy could serve as a reliable way to assess the presence of MRD in the future. The role of ctDNA to detect MRD has been investigated not only for prognostic value, but also for escalation or de-escalation of certain treatments.102,103 Patients with detectable ctDNA post treatment could benefit from an escalation of treatment; whereas in the absence of detectable post-treatment ctDNA, de-escalation of treatment may be advisable (for example, no post-operative radiation for chordoma in the absence of detectable MRD).
Conclusion
In this era of precision-medicine, cancer genomic profiling provides critical information for clinical decision-making. Liquid biopsies have emerged as an innovative tool to assist in tailoring cancer treatments. Liquid biopsy can be derived from multiple sources of biofluids. Currently, the ctDNA blood biomarker has gained the most traction as it is dynamic, minimally invasive, and repeatable. Application of the liquid biopsies for spine tumors remains in its infancy, but there is a growing body of literature supporting and investigating their use. Future clinical trials will be required to bring these promising approaches into the clinical realm.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Tumor, a focused group of international Tumor experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization.
Correction (June 2025):
This article has been updated to correct the affiliation for Alessandro Gasbarrini. A correction has been published.