
Abstract
Study Design
Retrospective multicenter study.
Objectives
To investigate the treatments of the geriatric population with hangman’s fractures using a multicenter database under the Japan Association of Spine Surgeons with Ambition (JASA).
Methods
The multicenter database included data from 1512 patients. We employed the Levine and Edwards classification for categorizing hangman’s fractures. The study incorporated epidemiological data, including the prevalence of hangman’s fractures, patient age, and follow-up duration. Bony fusion rates and length of hospitalization were recorded for Type I and Type II fractures, and the degree of neurological impairment was assessed.
Results
Hangman’s fractures represented 62 cases, accounting for 7.4% of all cervical spine injuries. The patients had an average age of 76.6 ± 6.5 years, and the mean duration of follow-up was 21.5 ± 23.6 months. The study found that the bony fusion rate for hangman’s fractures in the geriatric population was 88.9%. Surgical treatment was associated with a shorter hospitalization period for Type II fractures compared to conservative treatment. Thirteen cases of hangman’s fractures in the geriatric population, accounting for 21%, were complicated by spinal cord injury.
Conclusions
This is the largest study to date on hangman’s fractures in geriatric population ≥65 years. Type I and Type II fractures, according to the Levine and Edwards classification, had a bony fusion rate of up to 90%. In patients with Type II fractures, surgical treatment led to a shorter initial hospital stay. Geriatric patients are at risk of spinal cord injury due to hangman’s fractures.
Keywords
Introduction
Hangman’s fractures have been used to describe traumatic spondylolisthesis in C2 since they were first described by Schneider et al in 1965. 1 They are defined as bilateral fractures of the pars interarticularis.2,3 Hangman’s fractures account for 4%-8% of whole spinal trauma at the cervical spine and 15%-21% of C2 fractures.4–7 They can be caused by a traffic accident or falling from a height. Hangman’s fracture is the second most common fracture of the upper cervical spine, followed by an odontoid fracture.
The treatment strategy for hangman’s fractures is based on a classification of fracture types originally devised by Effendi and modified by Levine and Edwards.8,9 For stable injuries with no neurological deficits and no signs of subsequent instability, such as Type I or Type II fractures, it was claimed that fixing the cervical spine with external fixation or halo vest for a period is sufficient.10,11 Surgical fixation is recommended for instability with significant dislocation or possible subsequent instability, such as Levine-Edwards Type IIa and III fractures.5,12–18 The goals for treating hangman’s fractures are to stabilize the fracture and restore painless function while maintaining cervical spine alignment. Various surgical or conservative treatments have been described to achieve these goals, but considering the patient’s age and comorbidities, treatment strategies for hangman’s fractures remain controversial. Especially in the geriatric population, the risk of complications is high, and it is unclear whether surgical or conservative treatment is better.
The purpose of the present study was to describe the treatments in the geriatric population with hangman’s fractures using a multicenter database and to discover the optimal treatment for each Levine and Edwards classification.
Methods
Data Source
This retrospective, multicenter, observational study of cervical spine injuries in the geriatric population was conducted under the Japan Association of Spine surgeons with Ambition (JASA). The JASA database offers comprehensive coverage of cervical spine injuries occurring in individuals aged 65 years or older, encompassing cases with or without fractures or spinal cord injury. It contains a wealth of crucial information, including detailed descriptions of injury mechanisms, comprehensive imaging evaluation data such as CT and MRI, extensive documentation of spinal cord injury occurrence, concurrent complicating injuries, diverse treatment modalities, and comprehensive patient outcomes data. The institutional review board of a representative facility reviewed and approved this study (No. 3352-1). Because this was a retrospective study, informed consent was not required for submission.
We identified patients treated for hangman’s fractures at 33 institutes between January 2010 and March 2021. The inclusion criteria were patients over 65 years old, requiring hospitalization, and follow-up for at least 3 months (excluding death during hospitalization).
Patients With Hangman’s Fractures
We identified 1512 patients, from which patients with hangman’s fractures were selected. We collected epidemiological data such as the proportion of hangman’s fractures and patient characteristics such as age and sex, the mechanism of fractures, the Levine and Edwards classification of the fracture, associated injuries, and neurological outcome. The neurological impairment was assessed according to the American Spinal Cord Injury Association impairment scale (AIS). 19
Therapeutic options were reviewed in detail. For the conservative treatment, immobilization with a halo vest, hard collar, or soft collar was performed, and the immobilized period was noted. For the surgical treatment, the approach, the number of fusion vertebrae, operative time, and total blood loss were noted. Data were also collected on perioperative complications, bony fusion rate, and length of hospitalization in the initial hospital.
The treatment of hangman’s fracture by the Levine and Edwards classification and the bony fusion rate was investigated. Due to the small number of cases in Type IIa and Type III, it was not possible to examine each treatment method in detail.
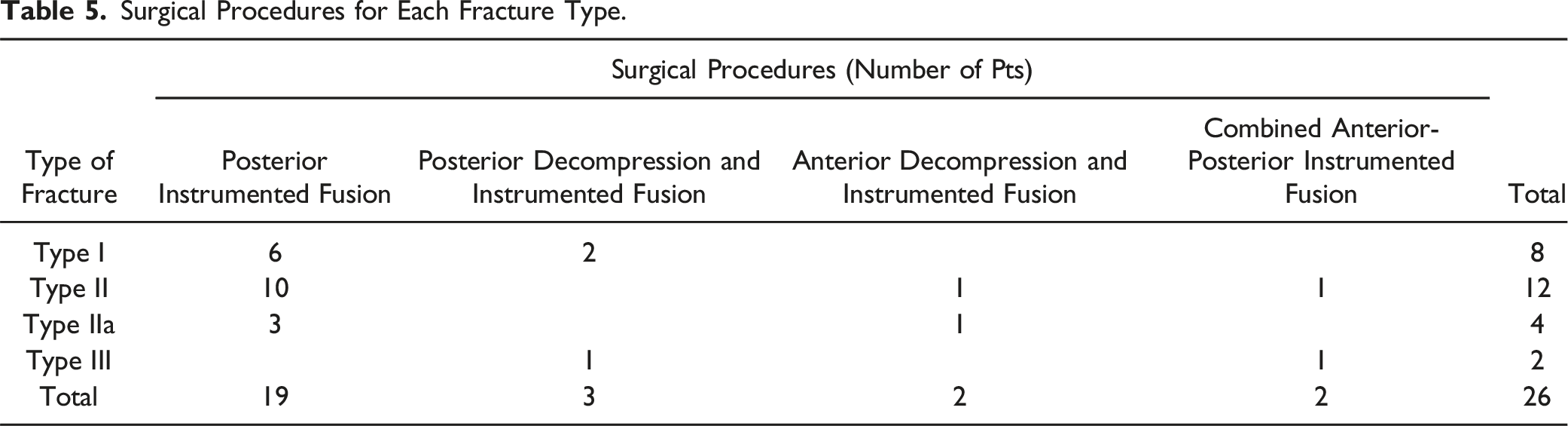
The diagnosis of hangman’s fracture and the Levine and Edwards classification of the fracture, the method of treatment, and the diagnosis of the bony fusion were at the discretion of each hospital. Likewise, each hospital had the discretion to choose the surgical approach method, whether it was anterior instrumented-fusion, posterior instrumented-fusion, posterior decompression and instrumented fusion, or a combined anterior-posterior approach.
Statistical Analysis
All statistical analyses were performed using JMP software (version 15.0.0; SAS Institute, Cary, NC). The 𝜒2 test was adapted to compare bony fusion rates and complications. The Wilcoxon test was used to compare the hospitalization periods. The data are presented as mean ± standard deviation. P < .05 was defined as significant.
Results
Epidemiological Data
Of 1512 patients, 834 had cervical fractures. Of these 834 patients, 314 had C2 fractures. Of these 314 C2 fractures, 62 patients had hangman’s fractures. There were 7.4% of hangman’s fractures among cervical spine injuries and 19.7% of hangman’s fractures among C2 fractures. The patients were 33 women and 29 men, with a mean age of 76.6 ± 6.5 years. Their mean duration of follow-up was 21.5 ± 23.6 months.
Low-energy injuries, such as falling from a standing position or a short fall, accounted for 13 and 11 cases, respectively, and high-energy injuries, such as falling from a height or a motor vehicle accident, accounted for 20 and 18 cases, respectively.
Type of Fractures
According to the Levine and Edwards classification, Type I was the most common in 34 cases (54.8%), followed by Type II in 20 cases (32.3%), Type IIa in 5 cases (8.1%), and Type III in 3 cases (4.8%).
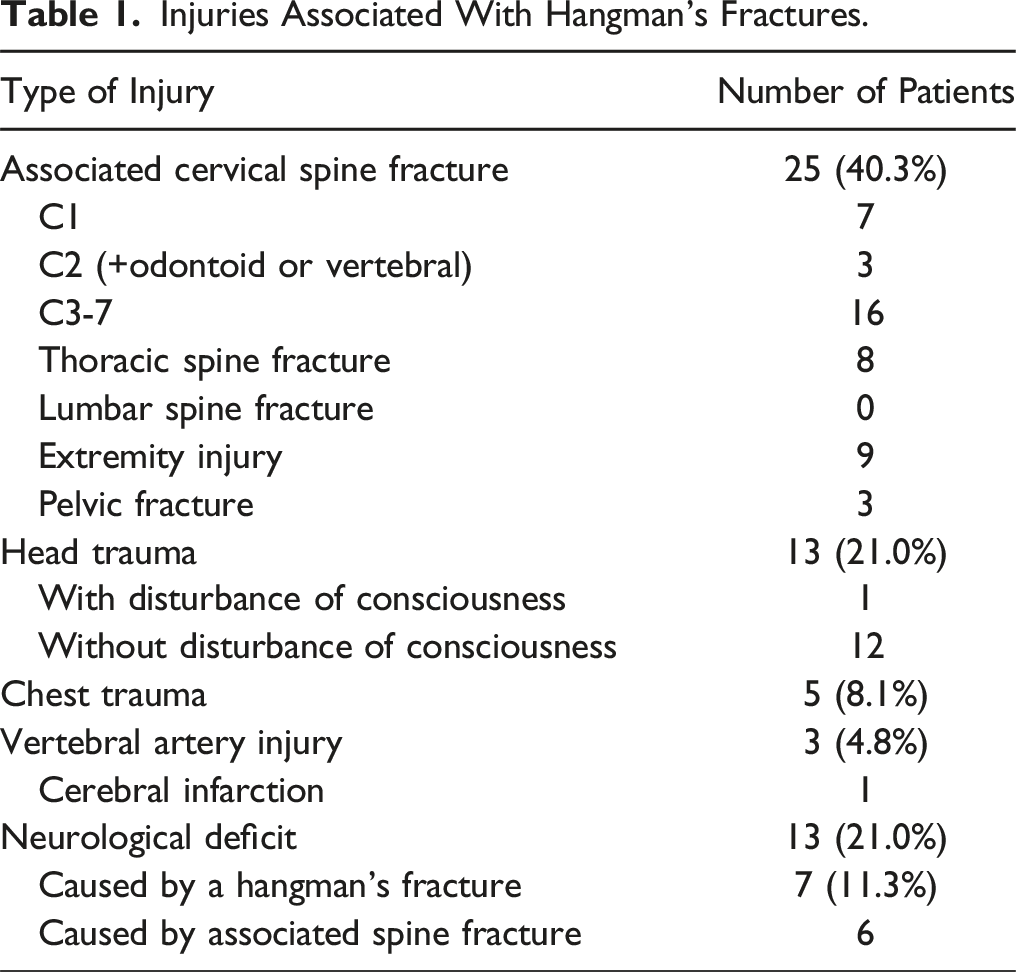
Associated Injuries
Injuries Associated With Hangman’s Fractures.
AIS at Admission.
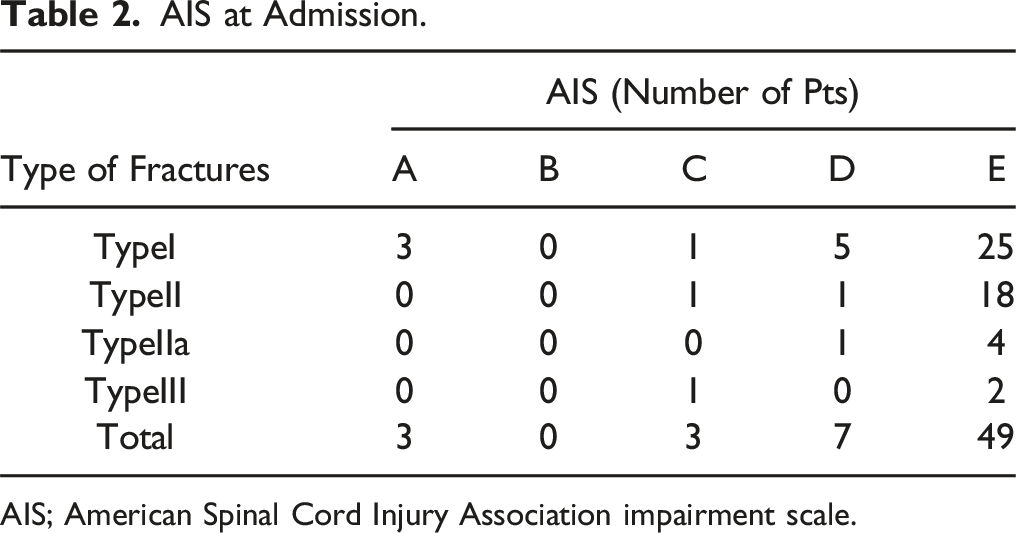
AIS; American Spinal Cord Injury Association impairment scale.
Management
Treatment Methods for Each Levine and Edwards Classification.
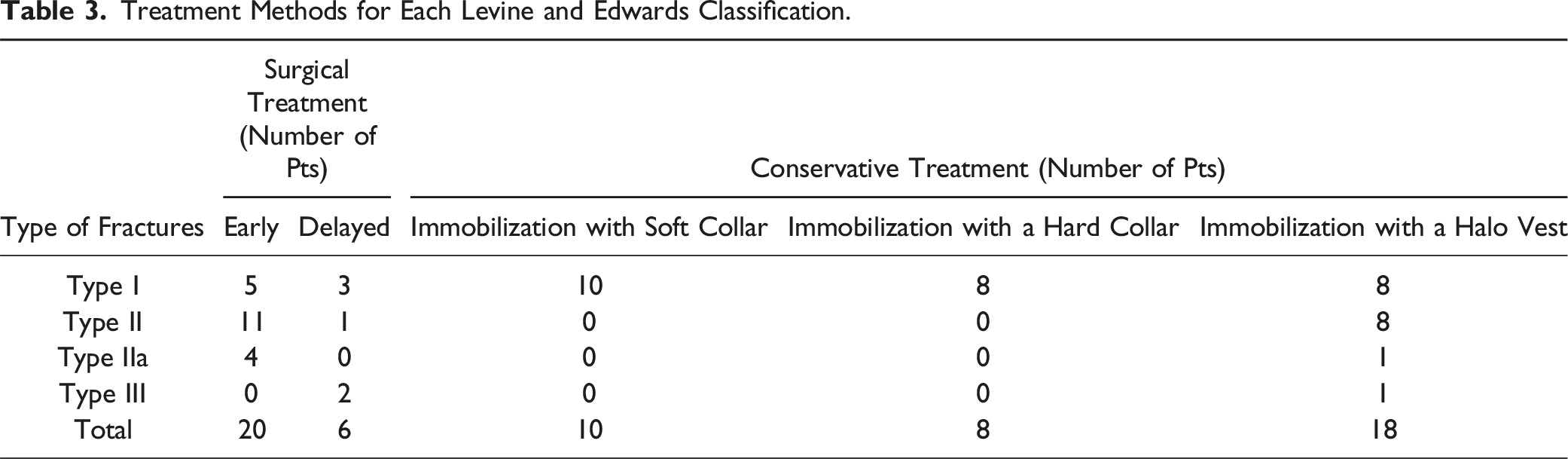
The “Delayed” group in Table 3 is the group in which the treatment method was changed from conservative to surgical treatment. Conservative treatment was selected more than surgical treatment for Type I fractures, and surgical treatment was selected more than conservative treatment for TypeII, IIa, and III fractures.
Conservative Treatment
Conservative treatment was immobilization with a halo vest or cervical spine collars (hard or soft). The average duration of halo vest immobilization was 73.4 ± 32.5 days, hard collar immobilization was 100.4 ± 39.8 days, and soft collar immobilization was 66.3 ± 30.5 days. Conservative treatments for Type II, IIa, and III fractures were all immobilization with a halo vest.
Surgical Treatment
Surgical Procedure.
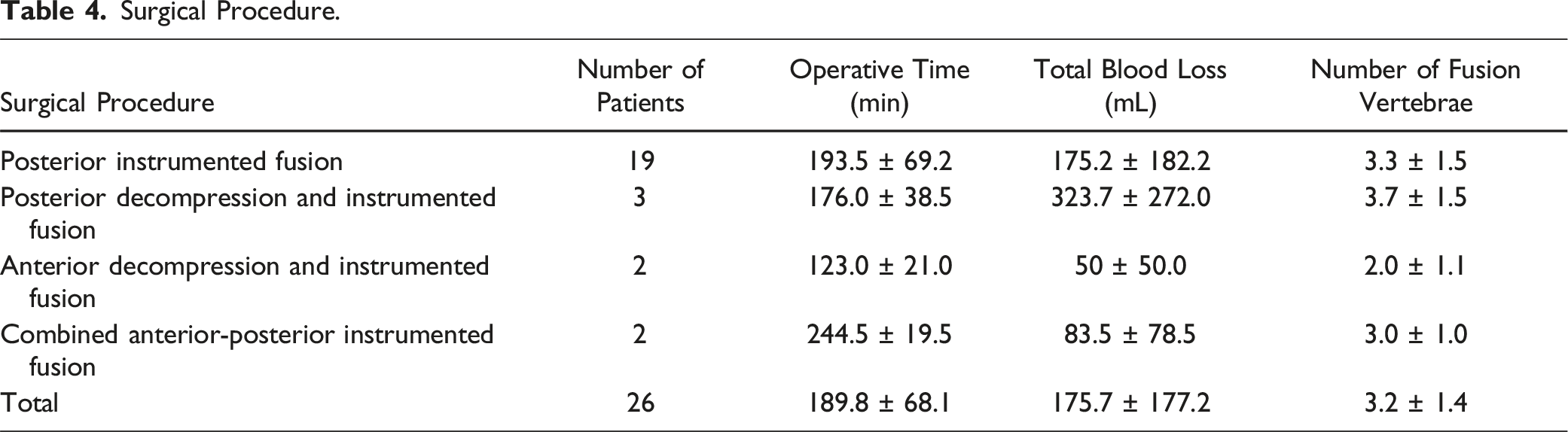
Surgical Procedures for Each Fracture Type.
Bony Fusion Rate
Bony Fusion Rate.

Complications
Complications.
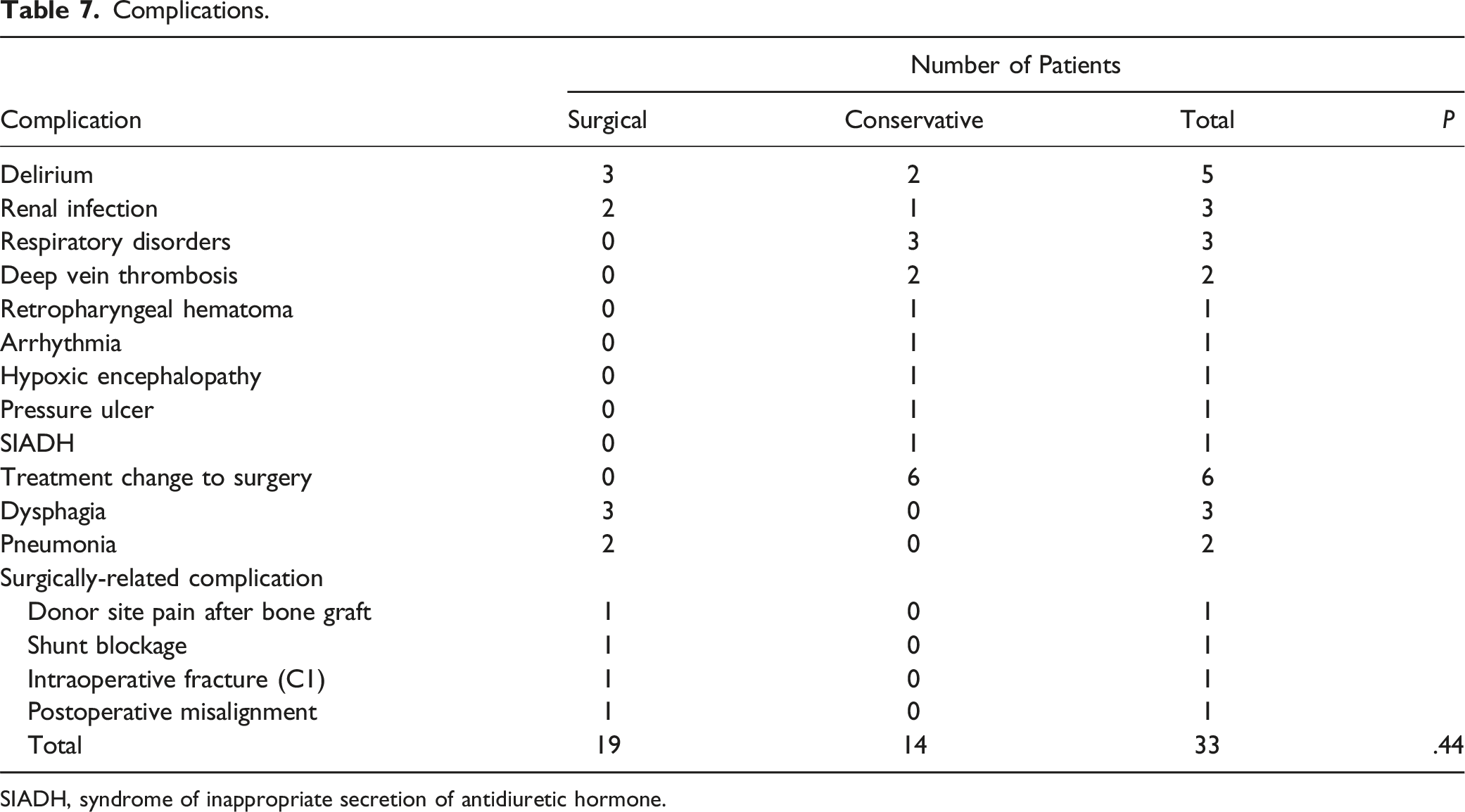
SIADH, syndrome of inappropriate secretion of antidiuretic hormone.
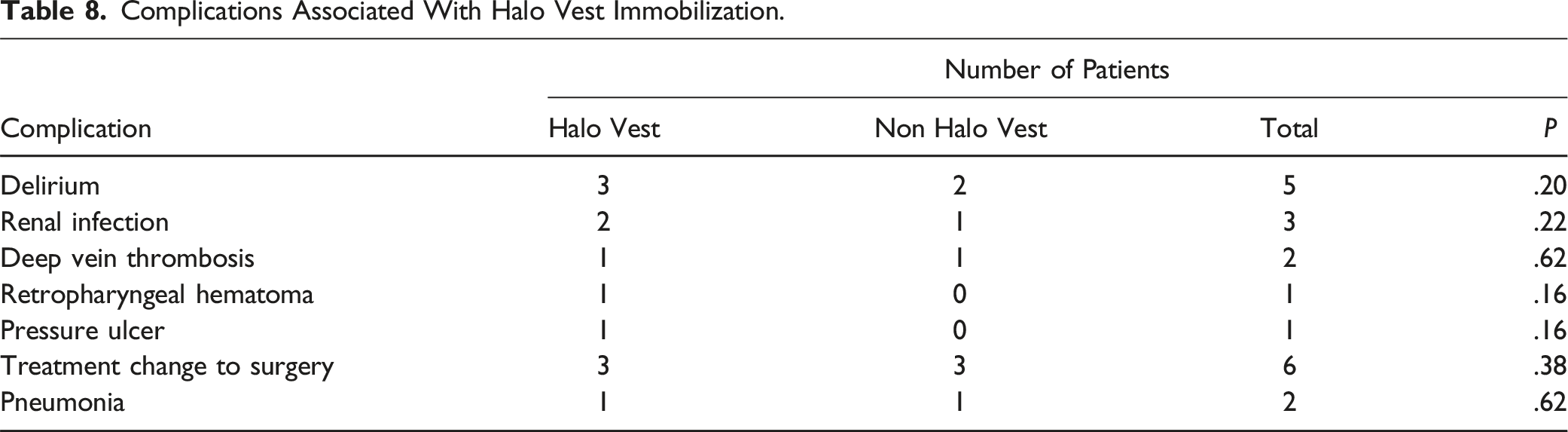
Complications Associated With Halo Vest Immobilization.
The Length of Hospitalization and Outcome
The average hospitalization was 36.0 days in the surgically treated group and 69.0 days in the conservatively treated group. Eight patients in the surgically treated group were discharged home, and 18 patients were transferred to another hospital for continued rehabilitation. In the conservatively treated group, 16 patients were discharged home, and 19 patients were transferred to another hospital for continued rehabilitation.
Figure 1 shows the length of hospitalization in Type I and Type II initial hospitals divided into surgical and conservative treatments. For Type I fractures, the surgically treated patients were hospitalized for a mean of 38.0 days, and the conservatively treated patients for a mean of 53.0 days, with no significant difference between the 2 groups. For Type II fractures, the surgically treated patients were hospitalized for 38.0 days and the conservatively treated patients for 110.0 days, with those in the surgical treatment group having a significantly shorter hospital stay (P = .0003). The length of hospitalization in the initial hospital for Levine and Edwards Type I and Type II fractures is shown. For patients with Type II fractures, the length of hospitalization was significantly shorter after surgical treatment. Asterisks denote significant intergroup differences (P < .05).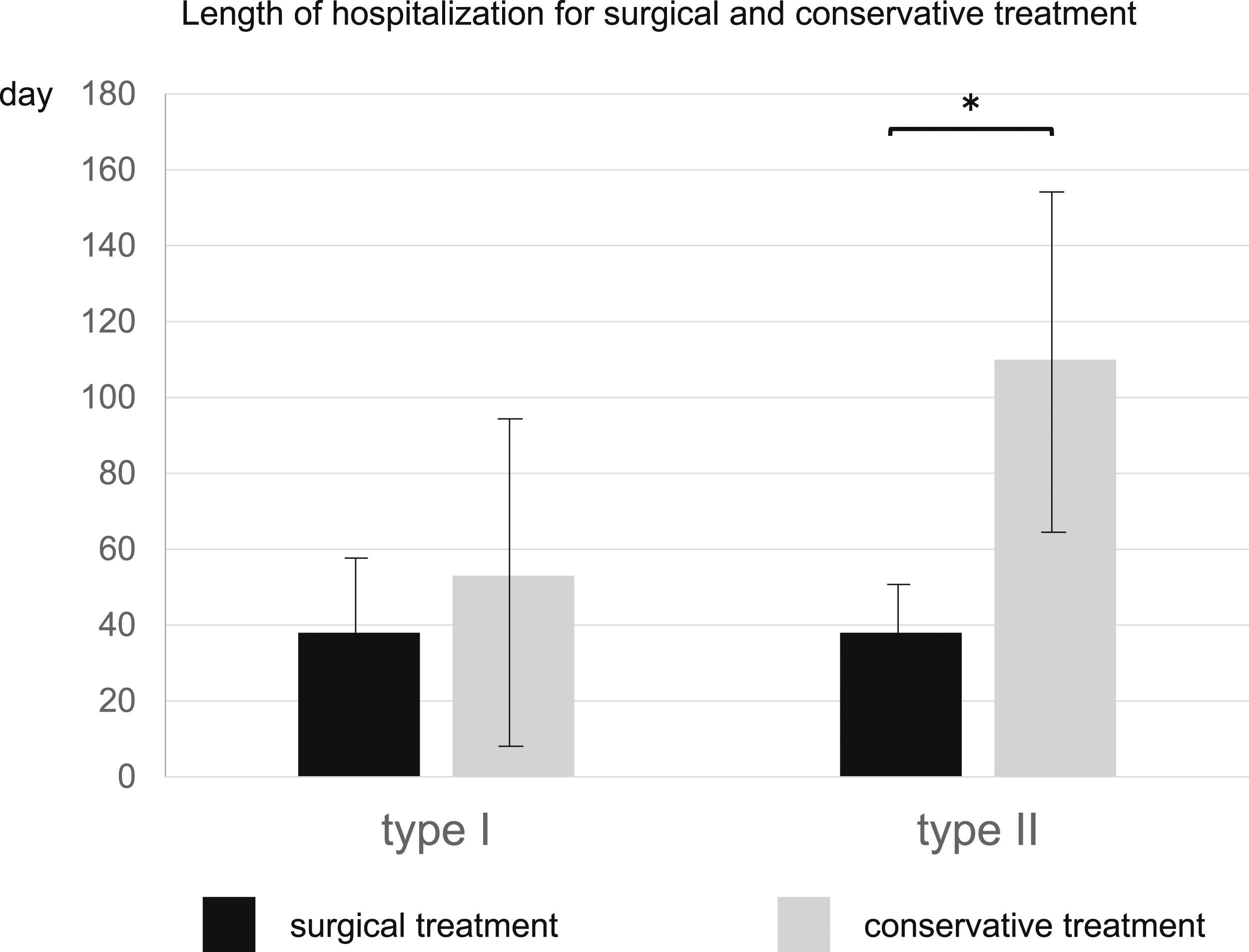
Discussion
This study is the largest study of hangman’s fractures and includes patients aged ≥65 years. The present study showed that the bony fusion rate of hangman’s fractures was as high as 90% in the geriatric population, and for Type II fractures, the length of hospitalization for surgical treatment was significantly shorter than that for conservative treatment. We found that hangman’s fractures are frequently accompanied by cervical spine injuries, requiring careful consideration of such injuries in the treatment planning process, and that hangman’s fractures alone can cause spinal cord injury in the geriatric population.
In their study of C2 fractures in geriatric patients, Radovanovic et al. examined 141 patients aged 70 years and older, including 11 cases of hangman’s fractures. 20 Their findings indicated minimal distinctions between hangman’s fractures and other C2 fractures in terms of injury etiology, predisposing factors, and mortality rates. Our current study collected a substantial dataset comprising 62 patients aged ≥65 years, all exclusively diagnosed with hangman’s fractures. This sizable sample is noteworthy for a study focused on geriatric patients with this type of fracture.
Bony fusion was observed in 49 (88.9%) of 55 patients. A review of hangman’s fractures reported that bony fusion rates were 94.14% for conservative treatment and 99.35% for surgical treatment, and patients treated surgically were less likely to have nonunion. 21 C2 lateral fractures are known to result in good bony fusion due to the composition of cancellous bone and abundant blood supply, and a high bone fusion rate was observed regardless of the treatment method. 22 The present study showed a high fusion rate of approximately 90% in the initial treatment. We observed slightly lower bony fusion rates compared to the existing literature on hangman’s fractures. However, it is important to note that our data are specific to patients aged ≥65 years. Notably, there are no previous articles in the literature that discuss bony fusion rates for hangman’s fractures in geriatric population, making it challenging to directly compare our findings with studies that include younger patients. Many factors can contribute to healing disorders in geriatric patients, but there is evidence that age is an independent factor that can delay the bony fusion of fractures. For example, studies in rats show that older rats have reduced expression of bone-forming BMP-2, and the serum of older donors is not a potent stimulator of osteoblast differentiation when compared with younger donors.23,24 Nikolaou et al. reported that patients older than 65 years had a significantly longer duration of bone healing than patients aged 18-40 years. 25 In light of the comparatively lower bony fusion rates observed in geriatric population, as demonstrated in our study, we can assert that our data revealing an approximate 90% bony fusion rates are indicative of a favorable outcome.
Li et al, in a systematic review of hangman’s fractures, have stated that the bony fusion rate with conservative treatment in Type III is less than 50%. 10 In this study, only 1 (33.3%) of 3 cases had bony fusion, and the remaining 2 cases required surgical treatment. It was found that Type III requires surgical treatment, even in geriatric patients. Bony fusion after surgical treatment was observed in all 55 patients (100.0%), and it was found that bony fusion was good even in hangman’s fractures of geriatric patients with appropriate treatment.
Conservative treatments for Type II, IIa, and III fractures were immobilization with a halo vest. AI-Mahfoudh et al reported that halo vests and hard-collar orthotics result in universally good bony fusion, 6 and Vaccaro et al. reported that halo vest immobilization is effective for bony fusion in most cases of hangman’s fractures. 11 They explained that rigid immobilization is required for conservative treatment. Moreover, fractures in geriatric patients are challenging to heal. It might be better to use a rigid immobilization, such as halo vest immobilization, from the onset to avoid bony fusion failure. Nevertheless, halo vest immobilization in geriatric patients has a higher incidence of death, pneumonia, and acute heart or respiratory failure than in patients treated with surgery or hard collars; the indications for halo vest immobilization need to be carefully considered. 26 Although this study did not find any specific complications associated with halo vest immobilization, it is prudent to be cautious when using halo vest immobilization in geriatric patients.
The length of hospital stay was not significantly different between surgical and conservative treatments for Type I fractures but was significantly shorter in the surgical group for Type II fractures. Surgical treatment has proven helpful for older patients, as early discharge to the home reduces complications and mortality. The previous research revealed that, in the case of C2 fractures, patients in the surgically treated group had a longer average hospital stay of 8.9 days, compared to 6.4 days for those in the halo vest group. 27 In contrast, the surgically treated group had an average hospitalization period of 36.0 days, whereas the conservatively treated group had an average of 69.0 days. This discrepancy can be attributed to the common practice in Japan of admitting patients to the hospital while they are wearing a halo vest.
Hangman’s fractures are complicated by other cervical spine injuries. In the present study, 40% of the cases were complicated by cervical spine fractures. Hence, the mean count of fused vertebrae was 3.2 ± 1.4, reflecting the frequent need for surgery that extended across multiple vertebrae, encompassing not only a single level (C2-3) or 2 levels (C1-3). Spinal cord injury can also be a complication and was present in 21% of the patients in this study. Most previous treatment literature classified patients based on fracture type and did not consider other concomitant injuries. Therefore, the present study included a survey of concomitant injuries to characterize hangman’s fractures in the geriatric population.
Spinal cord injury was observed in 13 patients (21%). Seven patients (11.3%) had hangman’s fractures that were the cause of spinal cord injury. Previous reports have stated that hangman’s fractures do not cause neurological deficits because the vertebral foramen is wide enough at this level, and the fractures tend to separate, thereby not compressing the spinal canal.1,18,28 By contrast, another report has shown a higher prevalence of upper cervical spine injuries and SCIs in the geriatric population than in other adults. 29 The geriatric population is more likely to have spinal cord injury due to loss of spinal flexibility and gain of rigidity due to aging, and there are cases of spinal cord injury due to hangman’s fractures.
There are some limitations to the present study. First, this was a multicenter database study, making it difficult to examine each case in detail. Although it was difficult to examine cases in detail, data from 33 institutes were available. The data are from a large number of institutes, so the results are derived from a certain consensus of data in Japan rather than from the biased treatment policies of a single institute. Second, it remains unclear which Type of atypical cases are classified when the fracture line extends into the vertebral body. In this study, atypical cases were not classified to simplify the study, and the Levine and Edwards classification was at the discretion of each institution, so it is possible that fracture lines extending into the vertebral body are not clearly classified. Lastly, a minimum follow-up duration of 3 months has been established. It is conceivable that an extended follow-up period will be imperative for assessing and addressing potential long-term complications and challenges arising from hangman’s fractures.
Conclusion
In conclusion, our study is the most extensive study to date on hangman’s fractures in the geriatric population ≥65 years. Our findings show that geriatric patients presenting with Type I and Type II fractures of the Levine and Edwards have high rates of bony fusion, up to 90%. They also show that bony fusion can be ensured by choosing the appropriate treatment modality. Notably, surgical treatment in cases of Type II fractures significantly shortened length of stay in the initial hospital. Furthermore, our study challenges the conventional notion that hangman’s fractures are unlikely to cause spinal cord injury. Instead, we provide evidence that such fractures can indeed cause spinal cord injury in geriatric patients. This discovery bears paramount significance and possesses the potential to shape the future management of hangman’s fractures in geriatric patients.
Footnotes
Acknowledgments
We thank all members of the Japan Association of Spine Surgeons with Ambition (JASA) for collecting the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.