
Abstract
Study Design
Retrospective case series.
Objective
To the best of our knowledge, the prevalence of lumbar spondylolysis in white and black populations has never been studied using computed tomography (CT). The purpose of this study was to examine and compare the prevalence and characteristics of lumbar spondylolysis in white and black patients.
Methods
This study is a cross sectional study. Patients aged 20-79 who underwent abdominal and pelvic CT for trauma screening in the New York City area and whose race was classified as “white” and “black” on the questionnaire were recruited to the study. A total of 1200 white patients (600 women, 600 men) and 1200 black patients (600 women, 600 men) were included for the analysis. The presence of lumbar spondylolysis, level, unilateral/bilateral, and the presence of spondylolisthesis at lumbar spondylolysis level were evaluated using CT.
Results
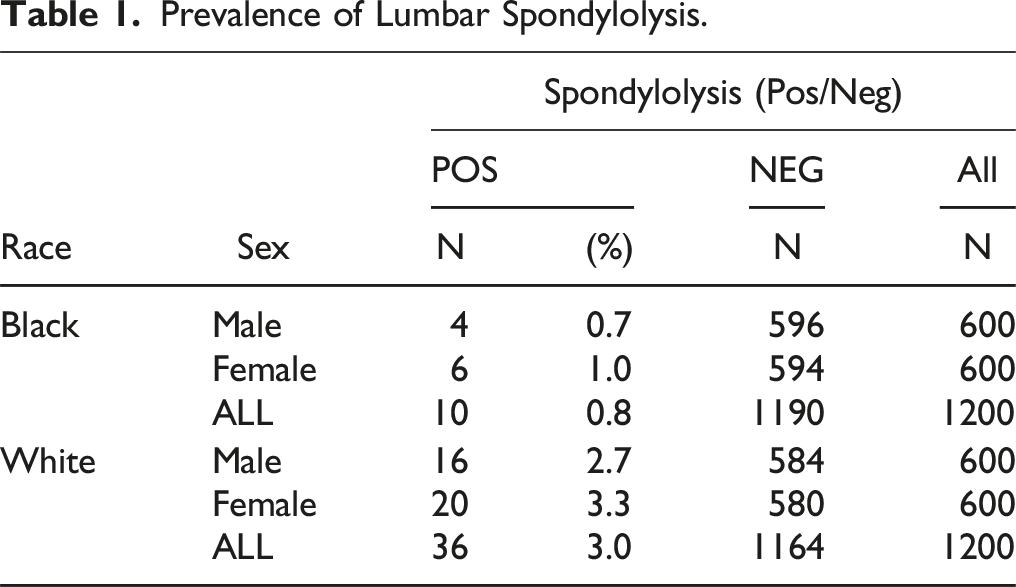
The prevalence of lumbar spondylolysis was 3.0% (n = 36) for white patients and .8% (n = 10) for black patients, with 3.3% (n = 20) and 1.0% (n = 6) for white and black females, respectively; and 2.7% (n = 16) and .7% (n = 4) for white and black males, respectively. The prevalence of lumbar spondylolysis was significantly higher in white patients compared with that in black patients (P < .0001). Lumbar spondylolysis was at L5 in 44/46 patients (95.7%) and bilateral in 41/46 patients (89.1%). Spondylolisthesis at lumbar spondylolysis level was found in 40/46 patients (87.0%).
Conclusions
The prevalence of lumbar spondylolysis was 3.0% for white patients and .8% for black patients. The prevalence of lumbar spondylolysis was significantly higher in white patients compared with that in black patients.
Introduction
Lumbar spondylolysis is a defect of the pars interarticularis and is generally caused by repetitive stress to the pars interarticularis, especially due to hyperextension. Decreased strength of the neural arch at a young age predisposes children and adolescents to a higher risk of fracture. 1 In the acute phase, bony union can be expected with conservative treatment; however, some cases, or untreated cases, can develop nonunion/pseudoarthrosis. 2 Furthermore, lumbar spondylolysis can progress to lumbar spondylolisthesis.
Previous epidemiological studies have investigated the prevalence of lumbar spondylolysis.3-8 The evaluation was traditionally conducted by plain radiographs. However, more recently, computed tomography (CT) scans are being used for the evaluation of lumbar spondylolysis. The diagnosis using CT scan images is more reliable than that by conventional radiographs. While the prevalence of lumbar spondylolysis using CT scans was reported in the Japanese population or mixed population,7,8 there is no study that specifically reported the prevalence of lumbar spondylolysis in the white and black population using CT analysis.
The purpose of this study was to examine the prevalence and characteristics of lumbar spondylolysis in white and black patients in the New York City area who underwent multi-slice abdominal and pelvic CT for trauma screening, and to compare between the white and black patient populations.
Material and Methods
Study Participants
This study was approved by our institutional review board (Kings County Hospital Center, STUDY00002324) and exempt from the requirement of informed consent. A cross-sectional review of a prospectively registered database in New York City Health and Hospitals (11 hospitals in New York City) was performed. All methods were carried out in accordance with relevant guidelines and regulations. Patients aged 20-79 who underwent abdominal and pelvic CT for trauma screening and whose race was classified as “white” or “black” on the hospital intake questionnaire were recruited in the study from Mar 2019 to Mar 2020. We used “black” because this was the term used on the questionnaire and “black” can include “African-American” and “Caribbean-American.” Patients with previous lumbar spine surgery were excluded from the study. Demographic data including age and sex were recorded. These data were based on a questionnaire completed at the initial visit to the trauma center.
Radiographic Assessment
All CT scans were acquired using a multi-detector CT with the following parameters: slice thickness, 1.25 mm; pixel size, .352 mm; tube rotation speed, .5 seconds; tube current, 200 mA; beam collimation, 40 mm; beam pitch, .9; and voltage, 120 kV. Axial and reconstructed sagittal images were analyzed with a Picture Archiving and Communication System (PennsylvaniaCS) viewer.
The entire lumbar spine was reviewed for each case using bone windows. Both axial and sagittal images were used to confirm the presence of lumbar spondylolysis. Lumbar spondylolysis was diagnosed as a linear lucency defect extending through the pars interarticularis. Lumbar spondylolysis was marked as present or absent on the right side, left side, or bilateral at each lumbar level. The diagnosis of spondylolisthesis at the level of lumbar spondylolysis was defined as a slippage of >3 mm.
Images were first reviewed by W.Y., who was trained by an experienced orthopaedic spine surgeon (H.Y.) to identify lumbar spondylolysis via CT scan. All positive and equivocal cases were reviewed and confirmed by E.H., V.N., and H.Y.
Statistical Analysis
Student t test and χ2 test were used when appropriate. Fishers exact test was used when the count was below the expected normal. The Cochrane Armitage trend test was used to determine if there was a significant difference in the trend of lumbar spondylolysis incidence across different age groups. A P value of less than .05 was considered statistically significant. Statistical analysis was performed using JMP Pro, Version 15 software (JMP®, Version 15. SAS Institute, Cary, NC).
Results
Demographic Data
A total of 1200 white patients and 1200 black patients were included for the analysis. Of the 1200 white patients, 600 were females and 600 were males, with a mean age of 48.3 ± 20.1 years (range, 20-79). Of the 1200 black patients, 600 were females and 600 were males, with a mean age of 49.1 ± 18.4 years (range, 20-79).
Prevalence and Characteristics of Lumbar Spondylolysis
Prevalence of Lumbar Spondylolysis.
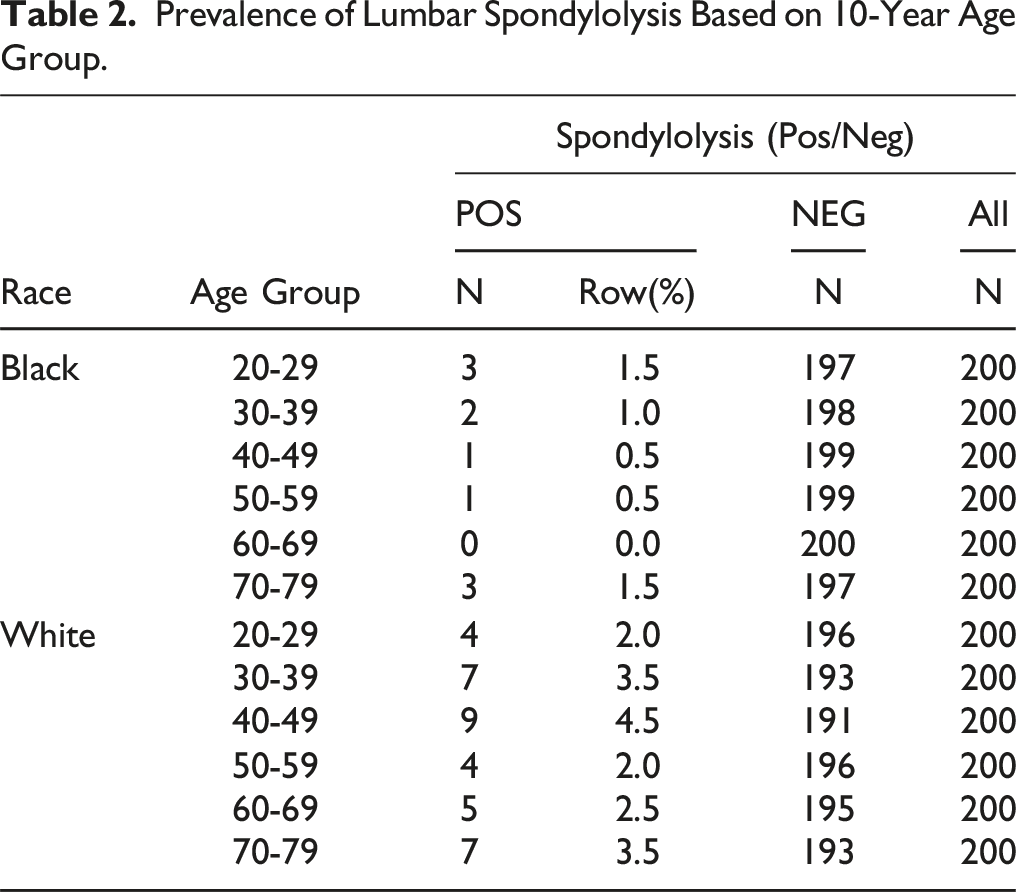
Prevalence of Lumbar Spondylolysis Based on 10-Year Age Group.
The prevalence of lumbar spondylolysis was significantly higher in white patients compared with that in black patients (3.0% vs .8%, P < .0001). The prevalence of lumbar spondylolysis was significantly higher in white female patients compared with that in black female patients (3.3% vs 1.0%, P < .05). The prevalence of lumbar spondylolysis was significantly higher in white male patients compared with that in black male patients (2.7% vs .7%, P < .05). No difference was found in the prevalence of lumbar spondylolysis between white female and male patients (P > .05). No difference was found in the prevalence of lumbar spondylolysis between black female and male patients (P > .05).
Lumbar spondylolysis was not present at L1, L2 or L3, and was present at L4 in 2 patients (4.3%) and L5 in 44 patients (95.7%) among 46 patients with lumbar spondylolysis (Figure 1). Lumbar spondylolysis was at bilateral in 41 patients (89.1%). Spondylolisthesis at the level of lumbar spondylolysis was found in 40/46 patients with lumbar spondylolysis (87.0%). CT imaging of lumbar spondylolysis L5 in 33 years old black male (left: axial, right: sagittal).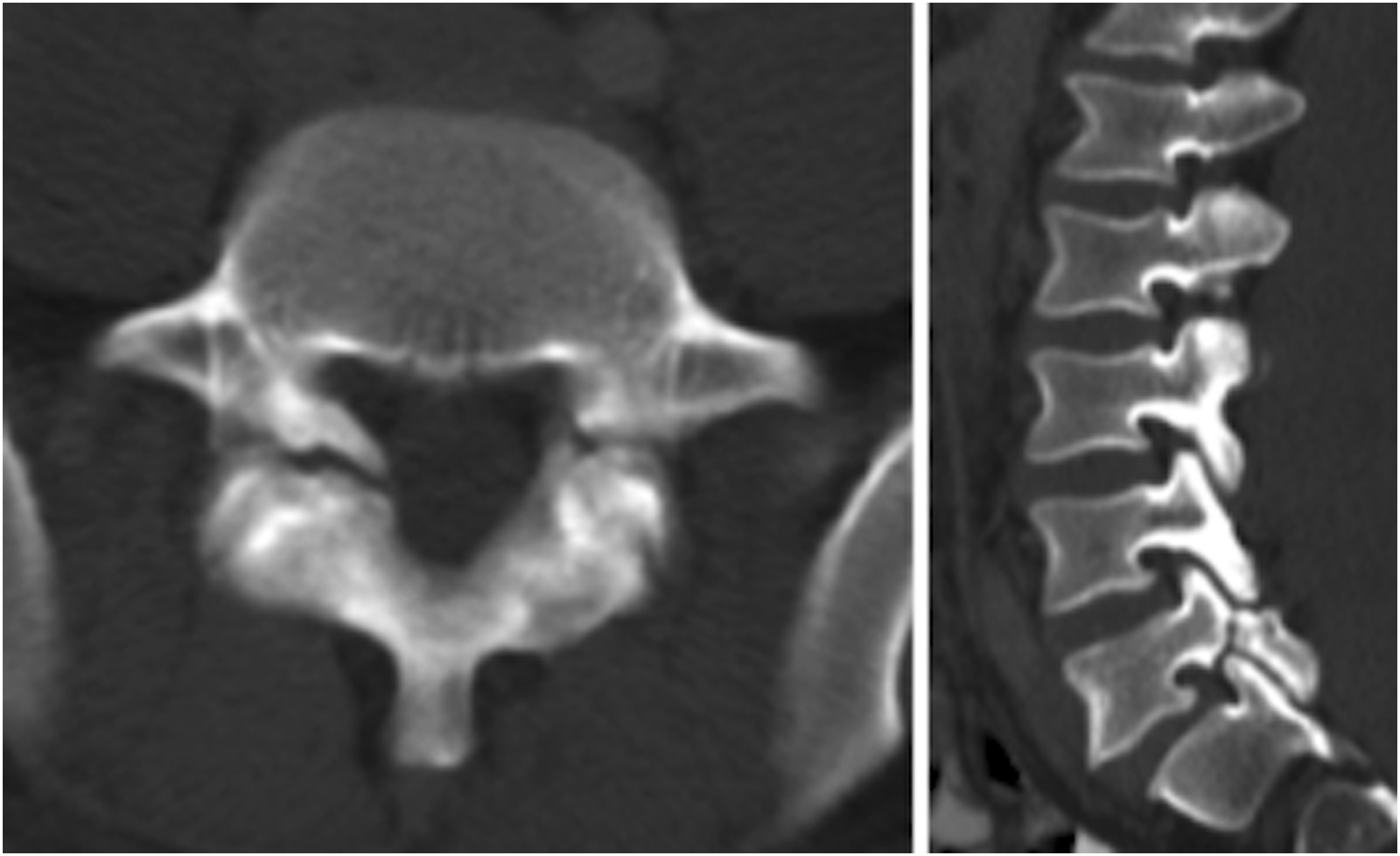
Discussion
The Prevalence of Lumbar Spondylolysis in the General Population.
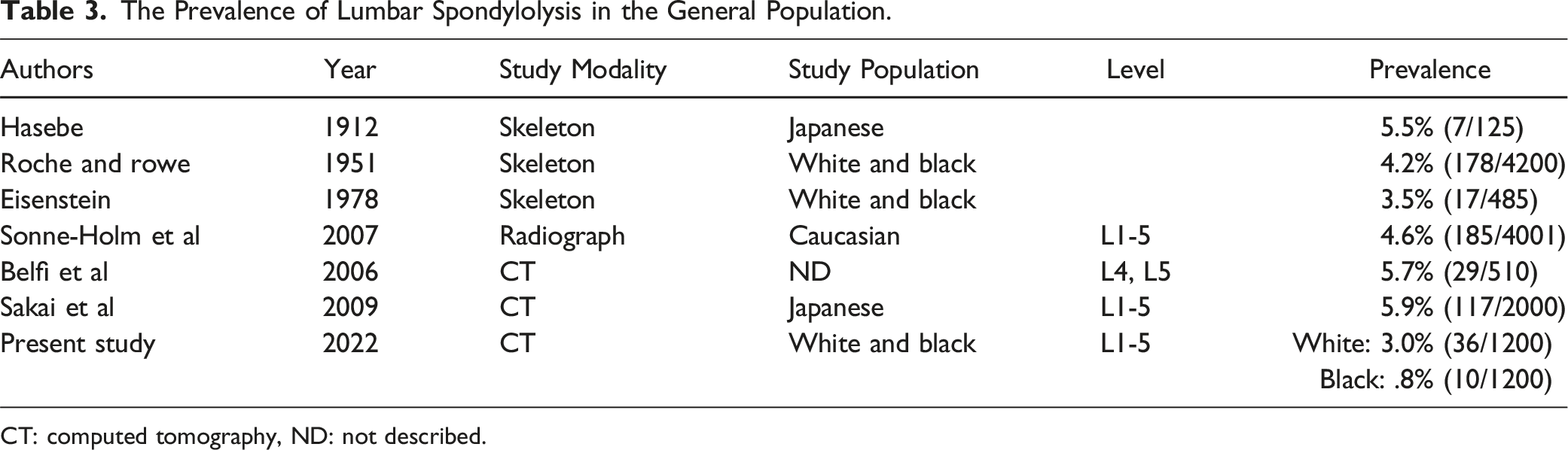
CT: computed tomography, ND: not described.
It is interesting that our study results showed a lower prevalence of lumbar spondylolysis in both white and black patients compared with that in the previous studies, despite a higher detection of lumbar spondylolysis when using CT. While several study findings suggest a genetic predisposition to lumbar spondylolysis,9-11 the main pathomechanism of lumbar spondylolysis is a stress fracture at the pars interarticularis due to repetitive mechanical stress. 12 In 1975, Wilse et al 13 suggested that spondylolysis began as a fatigue fracture of the pars interarticularis and frequently occurs in athletes with repetitive trunk movement. The conclusion that lumbar spondylolysis is caused by mechanical stressors can be drawn from the fact that lumbar spondylolysis has been shown to be absent at birth and that the incidence of lumbar spondylolysis in a patient population of 143 adults who had never walked was 0%. 14 Furthermore, decreased strength of the neural arch at a young age predisposes children and adolescents to a higher risk of fracture. 1 Previous studies demonstrated successful healing of lumbar spondylolysis at early stage by conservative treatment consisting of bracing, activity restriction, physical therapy and pain control.15,16 Based on these, possible explanations for lower prevalence of lumbar spondylolysis in our study may include less strenuous childhood/adolescent activities and/or early detection/treatment of lumbar spondylolysis in our New York City cohort.
The prevalence of lumbar spondylolysis was significantly higher in white patients compared with that in black patients (P < .0001). Previous studies consistently found the same trend.4,5 Roche and Rowe 4 found that the prevalence of lumbar spondylolysis was 6.4% in white men, 2.8% in African-American men, 2.3% in white women, and 1.1% in African-American women. Eisenstein 5 reported the prevalence was 3.8% in white men, 3.5% in African men, 5.7% in white women, and 2.6% in African women. Genetic predisposition to lumbar spondylolysis may play a role in this difference between white and black patients.
In our study, there was no significant difference in the prevalence of lumbar spondylolysis between females and males for both white and black patients (3.3 vs 2.7% in white patients, 1.0 vs .7% in Black patients). This is an interesting finding as most previous epidemiological studies showed the dominant prevalence of lumbar spondylolysis in males than in females.6-8 In the Sonne-Holm et al 6 study, men were significantly more at risk of L5 spondylolysis compared to women. Belfi’s study 7 demonstrated a male-female ratio of lumbar spondylolysis to be 2:1. Sakai et al 8 also reported that the male-female ratio was 2:1. However, we have no specific explanation for our results.
The prevalence of lumbar spondylolysis did not reveal any age-related trend in our study. This is consistent with previous studies.4,8 Lumbar spondylolysis generally develops at a young age. Fredrickson et al 9 performed a prospective study on 500 first graders and found a prevalence of 4.4% at the age of 6 years which increased to 6% by the time adulthood was reached. Roche and Rowe 4 summarized that the frequency of occurrence of lumbar spondylolysis is shown to remain almost constant regardless of age periods (adult life) represented by their skeletal study. In the study by Sakai et al, 8 the prevalence of lumbar spondylolysis is similar in each 10-year age group although trend analysis was not performed.
Lumbar spondylolysis occurs at the L5 vertebra most commonly. Our study also revealed that lumbar spondylolysis occurred at L5 in 44/46 patients (95.7%). In the study by Sakai et al, 8 the L5 vertebra accounted for 90.3% (112/124 vertebrae with lumbar spondylolysis). Sonne-Holm et al 6 found 1 case at L1, 2 at L2, 7 at L3, 52 at L4, and 123 at L5. In our study, lumbar spondylolysis was bilateral in 41/46 patients (89.1%). Roche and Rowe 4 reported 151/183 (82.5%) of lumbar spondylolysis were bilateral in their skeletal analysis. In the CT study by Belfi et al, 7 lumbar spondylolysis was bilateral in 23 of the 29 patients with lumbar spondylolysis. Using CT analysis, Sakai et al 8 found 91 subjects (79%) had bilateral lumbar spondylolysis in their 117 subjects with lumbar spondylolysis.
In our study, spondylolisthesis at the level of lumbar spondylolysis was found in 40/46 patients (87.0%). This ratio is higher than that of previous studies. In the study by Belfi et al, 7 spondylolisthesis was demonstrated in 16 of the 29 patients with lumbar spondylolysis. Sakai et al 8 reported that 75/124 (60.5%) vertebrae with lumbar spondylolysis showed low-grade spondylolisthesis.
Our study has several limitations. First, this study population may not represent the general population and may have a selection bias due to the limited area (New York City). However, as it is unethical to perform CT scans on normal volunteers, we consider that our study participants may represent the best possible random sampling for the general population. Second, although the ratio of spondylolisthesis at the level of lumbar spondylolysis in our study was higher than that of previous studies, actual spondylolisthesis prevalence may be even higher because identification of spondylolisthesis could be reduced due to the supine positioning in the CT scanner. Third, Kappa analysis to determine intraobserver reliability was not performed because the expected prevalence was quite low; however, controversial cases were discussed and determined by all authors. Fourth, this study is subject to errors that can occur while patient reporting (filling up the questionnaire), data retrieval, and analysis by the observer. Despite these limitations, we believe that our data are invaluable because this is the first study to examine and compare the prevalence of lumbar spondylolysis using CT analysis in the white and black populations.
Conclusion
The prevalence of lumbar spondylolysis was 3.0% for white patients and .8% for black patients in the New York City area. The prevalence of lumbar spondylolysis was significantly higher in white patients compared with that in black patients. The prevalence of lumbar spondylolysis was significantly higher in white females compared with that in black females and in white males compared with that in black males. Lumbar spondylolysis was at L5 in 44/46 patients (95.7%) and bilateral in 41/46 patients (89.1%).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.