
Abstract
Study Design
Retrospective case-control study.
Objective
To explore the association of early postoperative nadir hemoglobin with risk of a composite outcome of anemia-related and other adverse events.
Methods
We retrospectively analyzed data from spinal tumor patients who received intraoperative blood transfusion between September 1, 2013 and December 31, 2020. Uni- and multivariate logistic regression was used to explore relationships of clinicodemographic and surgical factors with risk of composite in-hospital adverse events, including death. Subgroup analysis explored the relationship between early postoperative nadir hemoglobin and composite adverse events.
Results
Among the 345 patients, 331 (95.9%) experienced early postoperative anemia and 69 (20%) experienced postoperative composite adverse events. Multivariate logistic regression analysis showed that postoperative nadir Hb (OR = .818, 95% CI: .672-.995, P = .044), ASA ≥3 (OR = 2.007, 95% CI: 1.086-3.707, P = .026), intraoperative RBC infusion volume (OR = 1.133, 95% CI: 1.009-1.272, P = .035), abnormal hypertension (OR = 2.199, 95% CI: 1.085-4.457, P = .029) were correlated with composite adverse events. The lumbar spinal tumor was associated with composite adverse events with a decreased odds compared to thoracic spinal tumors (OR = .444, 95% CI: .226-.876, P = .019). Compared to patients with postoperative nadir hemoglobin ≥11.0 g/dL, those with nadir <9.0 g/dL were at significantly higher risk of postoperative composite adverse events (OR = 2.709, 95% CI: 1.087-6.754, P = .032).
Conclusion
Nadir hemoglobin <9.0 g/dL after spinal tumor surgery is associated with greater risk of postoperative composite adverse events in patients who receive intraoperative blood transfusion.
Introduction
Many primary spinal tumors have already invaded the spinal canal by the time of diagnosis, and they show aggressive malignancy associated with poor prognosis.1-6 Surgery to remove spinal tumors can substantially improve prognosis, 1 but it involves extensive spinal reconstruction, which increases risk of bleeding. 7 In fact, average perioperative blood loss is 2180 ml 8 and blood loss can in rare cases exceed 5000 ml. 9 In addition, up to 40% of patients with lumbar spinal tumors experience acute postoperative hemorrhagic anemia, 10 which can cause hemodynamic imbalance and tissue hypoxia11-13 as well as increase the risk of nonfatal myocardial infarction and all-cause mortality. 12
To reduce risk of such anemia and associated tissue hypoxia, blood transfusion rates during spinal tumor surgery range from 50% to 81%. 8 However, blood transfusion, especially in larger volumes, increases risk of infection, acute lung injury and death.14,15 Therefore, it is important to optimize hemoglobin levels to improve prognosis. At present, most transfusion guidelines are based on a restrictive hemoglobin threshold of 7-8 g/dL.16-18 However, hemoglobin level early during active bleeding or hemodynamic instability may not be the most appropriate transfusion trigger, because it can lead to late or inadequate transfusion. 19 Instead, postoperative nadir hemoglobin level may more accurately indicate the need for transfusion because it reflects the mass of circulating red blood cells after fluid has had sufficient time to redistribute between the vasculature and intestinal/cellular space. 20 Indeed, one study of patients undergoing on-pump cardiac surgery associated postoperative nadir hemoglobin levels <9.0 g/dL with higher risk of composite adverse events, including new-onset stroke, myocardial infarction, and acute kidney injury in hospital. 21
Here we explored whether nadir hemoglobin level within 24 h after spinal tumor surgery was associated with higher risk of anemia-related and other adverse events. We focused on adverse events that are relatively common after such surgery, including ischemic, thrombotic, and respiratory events as well as infections.22,23 We included only patients who received blood transfusion during surgery in an effort to help guide postoperative anemia management and blood transfusion practices.
Methods
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Zhejiang University School of Medicine (0984/2021), which waived the requirement for informed consent because patients, at the time of treatment, gave written consent for their anonymized medical data to be analyzed and published for research purposes.
Study participants and Data Collection
Electronic medical records were retrospectively analyzed for patients who underwent spinal tumor surgery involving intraoperative blood transfusion at the Second Affiliated Hospital of Zhejiang University School of Medicine between September 1, 2013 and December 31, 2020. To be enrolled, patients had to be at least 18 years old and had to receive at least 1 unit of allogeneic red blood cells (RBCs) intraoperatively. Patients were excluded if they had preoperative pleural effusion or their hemoglobin levels were not assayed within 24 h after surgery. If patients underwent multiple spinal tumor surgeries, we included data only from the first procedure. Patient data were extracted from the “Do Care” System and Electronic Medical Record System at the Second Affiliated Hospital.
The following data were collected: demographic characteristics (age, sex, body mass index, history of smoking and alcohol consumption), laboratory characteristics (preoperative hemoglobin and creatinine), American Society of Anesthesiologists (ASA) classification, age-adjusted Charlson comorbidity index (ACCI), surgical characteristics (tumor type and location, epidural spinal cord compression classification, surgical approach, blood-sparing measures), and intraoperative conditions (duration of surgery, blood loss, intraoperative urine volume, type and volume of transfusion, fluid infusion, and intraoperative blood pressure). Postoperative nadir hemoglobin was defined as the lowest hemoglobin value within 24 h after surgery. Hemoglobin <130 g/L in adult males and hemoglobin <120 g/L in adult non-pregnant females are diagnosed as anemia according to World Health Organization diagnostic criteria. 24
Transfusion Strategy
Intraoperative allogeneic RBC transfusion was decided by the anesthesiologist when hemoglobin was <7.0 g/dL in the most recent analysis of blood analysis, or when it was <8.0 g/dL in the presence of cardiovascular risk, substantial hemodynamic instability or rapid massive bleeding. 25
Outcomes
The primary outcome was composite adverse events occurring between 24 h postoperatively and hospital discharge. Composite adverse events were any of the following: myocardial infarction, pleural effusion, pulmonary infection, acute respiratory distress syndrome, respiratory failure, acute kidney injury, surgical site infection, symptomatic urinary tract infection, system inflammatory reaction syndrome, sepsis, deep vein thrombosis and in-hospital death. In-hospital death was defined as a patient who died in hospital or who was released into the care of his or her family while still in critical condition. The secondary outcome was postoperative RBC infusion.
Statistical Analysis
Data were analyzed using SPSS 25.0 (IBM, Armonk, NY, USA) and R 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria), and results were considered significant if associated with P < .05. Categorical data were expressed as frequencies (percentages) and compared between groups using χ2 or Fisher’s exact tests. Continuous data were assessed for normality using the Shapiro-Wilk test. Normally distributed continuous data were expressed as mean ± SD and were compared between groups using Student’s t test. Skewed continuous data were expressed as median (interquartile range) and compared between groups using the Mann-Whitney U test.
Multivariate logistic regression was performed using stepwise arithmetic selection with nadir hemoglobin as a continuous variable and the primary outcome as the dependent variable. Covariates were other clinicodemographic variables linked to the primary outcome in the literature or based on our univariate logistic regression. Multivariate logistic regression was repeated with hemoglobin nadir defined categorically in quartiles based on our sample (<9.0, 9.0–9.9, 10.0–10.9, and ≥11.0 g/dL). Multivariate regression was also performed for subgroups of patients stratified by age, sex, ASA classification, and preoperative anemia. The influence of variables on risk of the primary outcome was expressed in terms of odds ratios (ORs) and 95% confidence intervals (CIs).
Results
Patient Characteristics
A total of 531 patients underwent spinal tumor surgery in our center between September 1, 2013 and December 31, 2020. After excluding 172 patients who did not receive allogeneic RBCs intraoperatively, 2 patients younger than 18 years, 9 patients lacking hemoglobin levels within 24 h after surgery and 3 patients with preoperative pleural effusion, we included the remaining 345 patients in the analysis (Figure 1). Flowchart of patient selection and analysis. Hb, hemoglobin; RBC, red blood cell.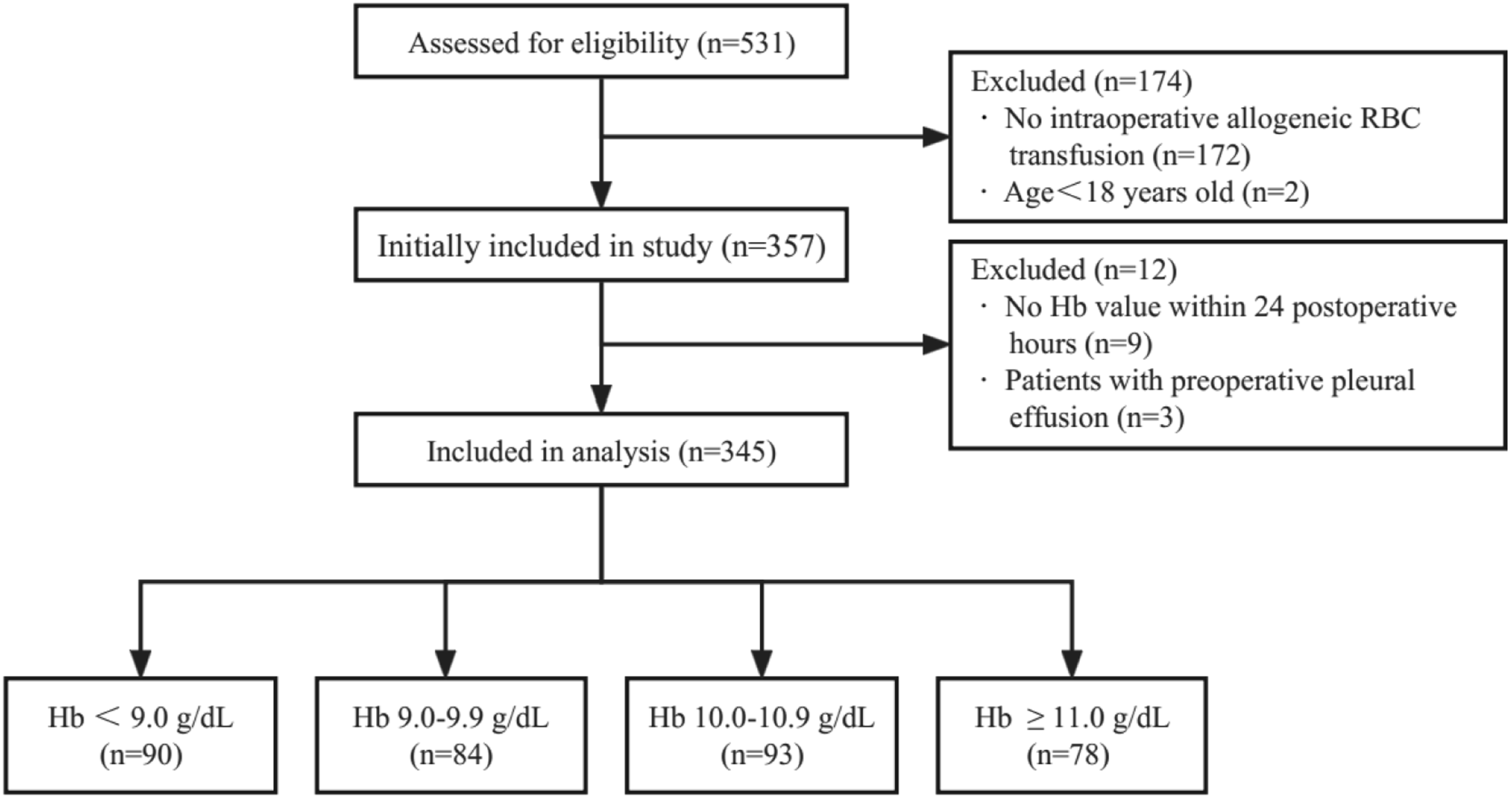
Comparison of Clinicodemographic Characteristics Between Patients Who Experienced the Primary Outcome or Not.
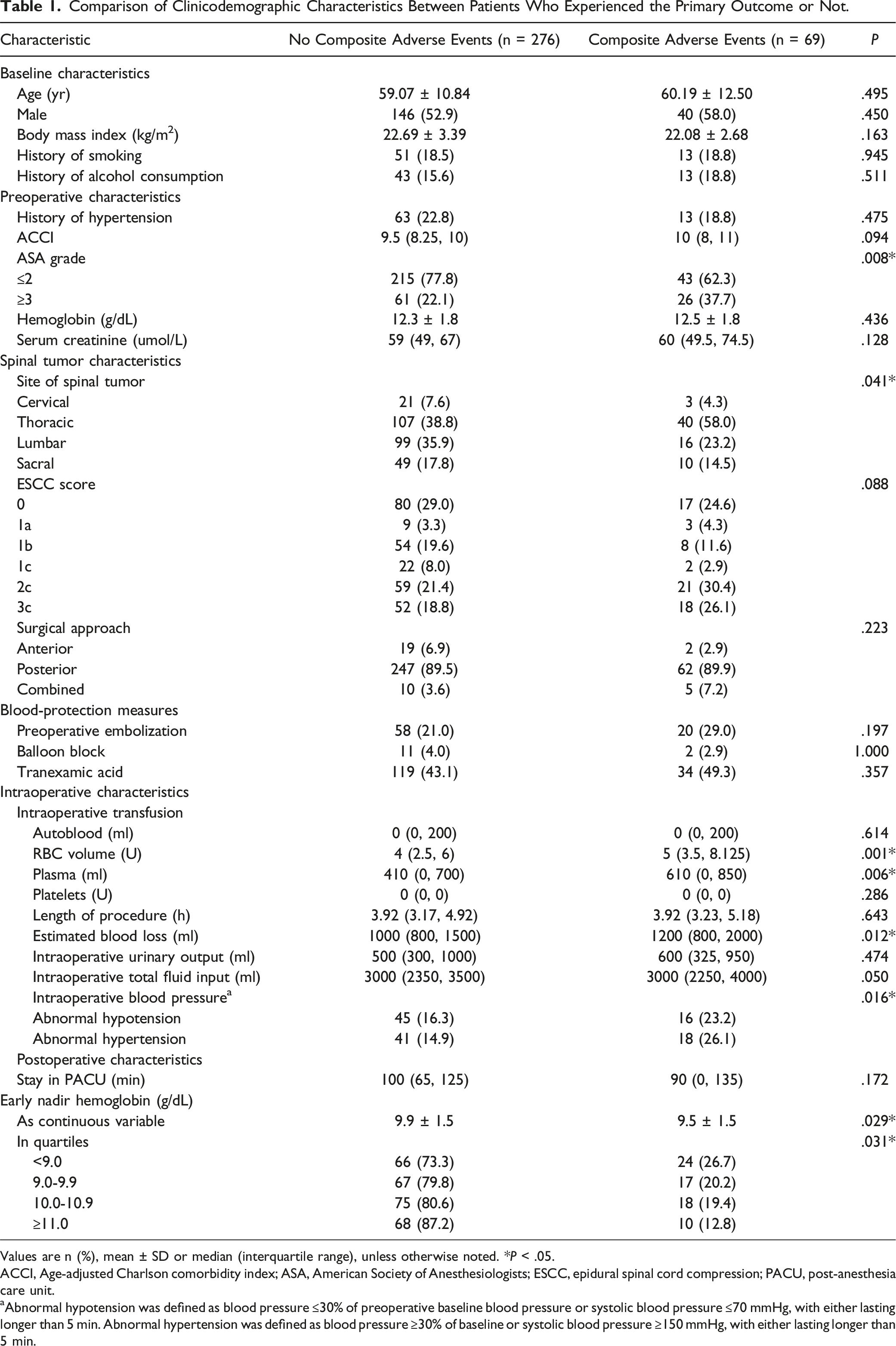
Values are n (%), mean ± SD or median (interquartile range), unless otherwise noted. *P < .05.
ACCI, Age-adjusted Charlson comorbidity index; ASA, American Society of Anesthesiologists; ESCC, epidural spinal cord compression; PACU, post-anesthesia care unit.
aAbnormal hypotension was defined as blood pressure ≤30% of preoperative baseline blood pressure or systolic blood pressure ≤70 mmHg, with either lasting longer than 5 min. Abnormal hypertension was defined as blood pressure ≥30% of baseline or systolic blood pressure ≥150 mmHg, with either lasting longer than 5 min.
Composite adverse events occurred in 13 of 62 patients with primary spinal tumors and 56 of 283 patients with spinal metastatic tumors (Supplementary Table 2). Undergoing primary, but not metastatic, spinal tumor surgery was significantly associated with composite adverse events (P = .016).
Factors Associated With Composite Adverse Events
Uni- and Multivariate Logistic Regression to Identify Factors Associated With Postoperative Composite Adverse Events.
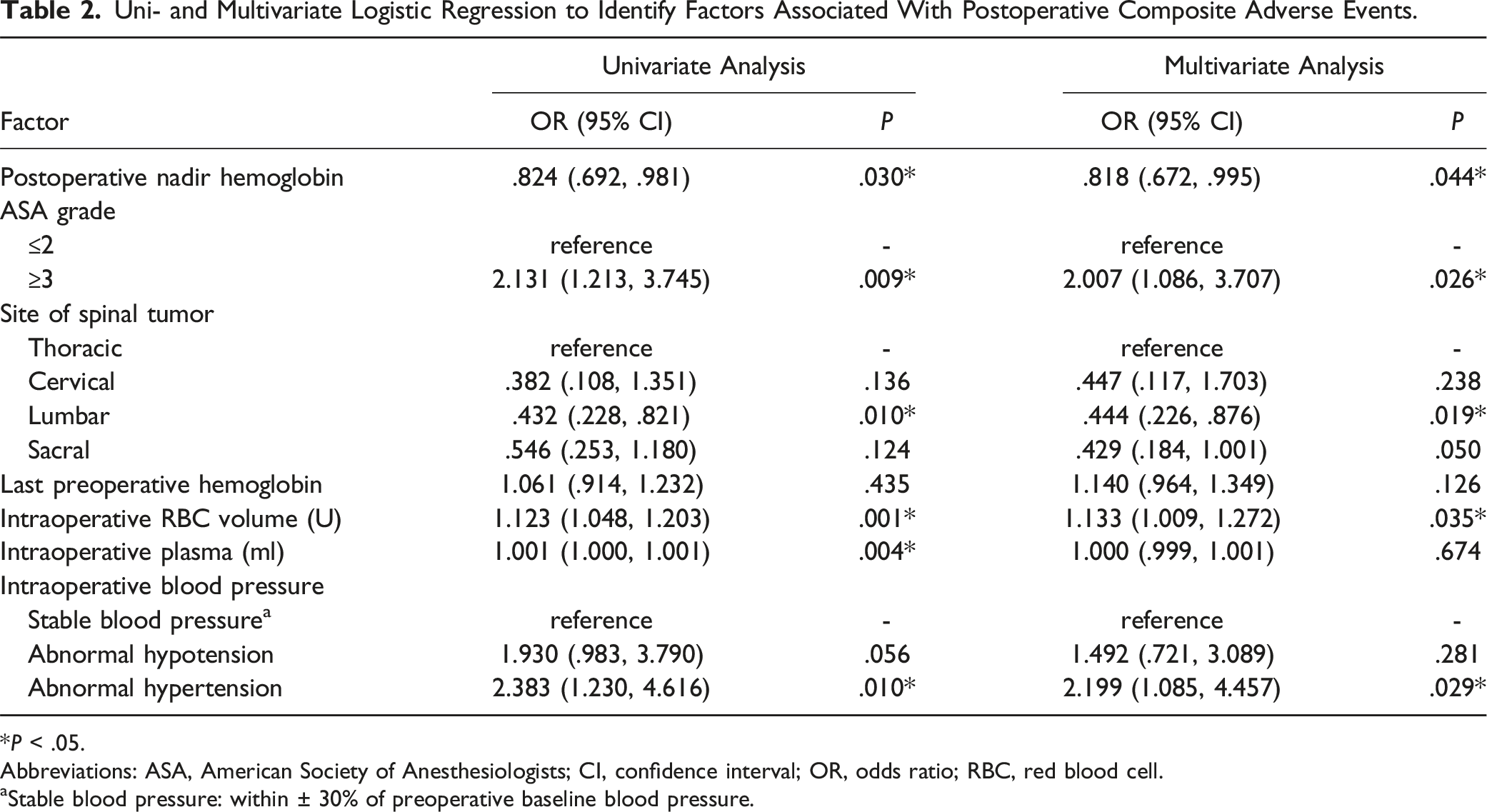
*P < .05.
Abbreviations: ASA, American Society of Anesthesiologists; CI, confidence interval; OR, odds ratio; RBC, red blood cell.
aStable blood pressure: within ± 30% of preoperative baseline blood pressure.
Influence of Early Postoperative Nadir Hemoglobin Level on Risk of Composite Adverse Events
Multivariable Regression to Assess the Association Between Postoperative Nadir Hemoglobin Level and Risk of Composite Adverse Events.
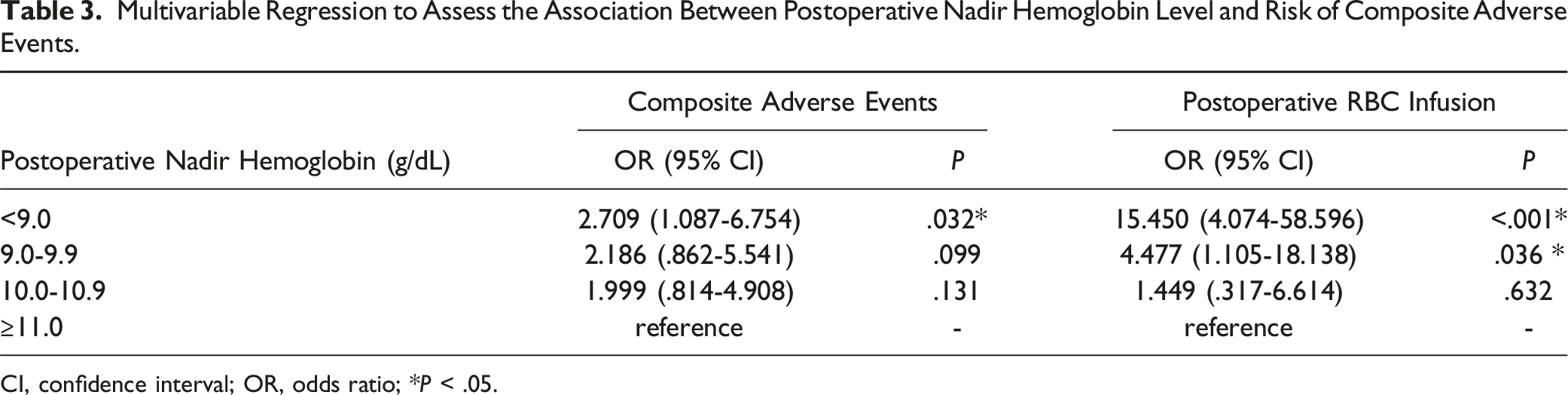
CI, confidence interval; OR, odds ratio; *P < .05.
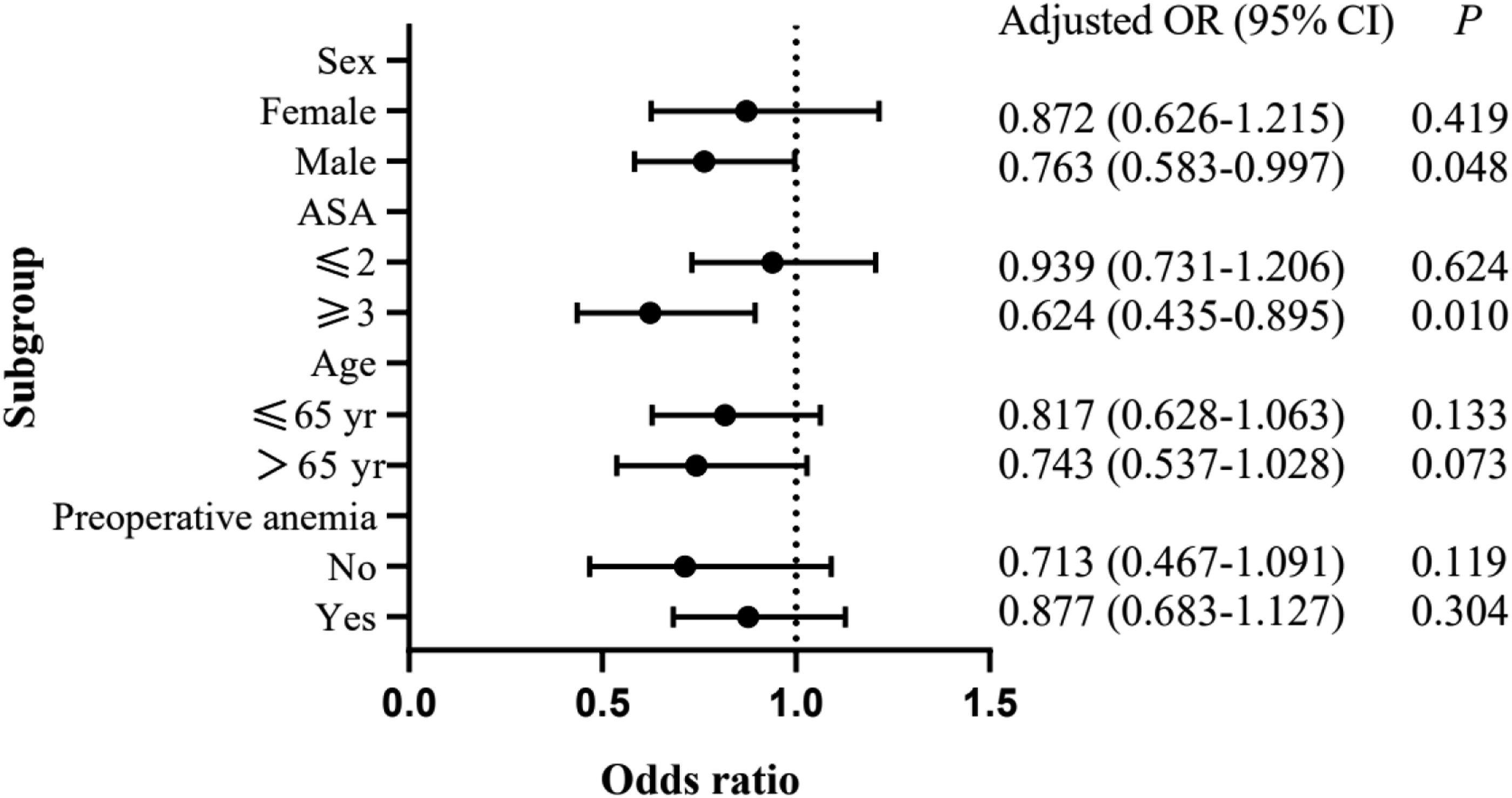
Subgroup analysis of the association between postoperative nadir hemoglobin levels on risk of composite adverse events. Analyses were adjusted for the same variables as in Table 3. ASA, American Society of Anesthesiologists; CI, confidence interval; OR, odds ratio.
Discussion
Our work identified several factors as associated with higher odds of postoperative composite adverse events among patients undergoing spinal tumor surgery involving intraoperative blood transfusion. In particular, we found that the risk of composite adverse events progressively increased with decreasing nadir hemoglobin level, especially for levels below 9.0 g/dL. These results may help identify patients at higher risk of worse prognosis and serve as a more appropriate management guide than commonly used transfusion triggers, such as perioperative hemoglobin levels below 8 g/dL. Indeed, patients with spinal tumors may require a more liberal transfusion strategy, as suggested for patients undergoing cardiac or macrovascular surgeries.11,21
Deciding on postoperative blood resuscitation based on pre- or intraoperative hemoglobin levels can lead to under- or over transfusion, either of which can result in complications. 19 Our results suggest that nadir hemoglobin levels within 24 h after surgery, especially levels below 9.0 g/dL, can predict prognosis. This may reflect the importance of the first 24 h after surgery for fluid redistribution between the vascular and intestinal/cellular spaces 20 and the body’s greater demand for oxygen during that period in order to drive inflammatory responses to surgical stress and blood transfusion. 12
The incidence of early postoperative anemia in our study was 95.9%, higher than the 43.3% in a study of the management of frail patients with lumbar spine tumors. 10 This likely reflects that all our patients experienced intraoperative anemia and therefore received intraoperative blood transfusion.
We observed a similar range of postoperative composite adverse events as in our previous work on patients undergoing spinal tumor surgery. 7 These events reflect hypoxic-ischemic damage to vital organs,11,12,26,27 related inflammation, 27 as well as slow blood flow and deep vein thrombosis arising from prolonged bed rest and hypercoagulation in spinal tumors after surgery. 28
More than half the postoperative composite adverse events in our study occurred in patients whose spinal tumors were thoracic, and just under half of the events were pleural effusion. Surgery involving the thoracic spine may involve more extensive manipulations and may take longer due to the presence of large blood vessels and mediastinal structures. This, in turn, may increase the risk of pleural effusion, anemia, lung injury, and infection.29-31 Among patients in our study whose spinal tumors were metastases of a primary cancer, the most frequent primary cancer was of the lung, and lung cancer increases risk of pleural effusion. 32
Our subgroup analyses confirmed an increasing risk of composite adverse events with decreasing postoperative nadir hemoglobin levels in men but not in women, which may reflect the higher ACCI of the men in our study. Indeed, ACCI is a good predictor of prognosis of patients undergoing spinal tumor surgery. 33 We also confirmed the association of increasing risk with decreasing nadir in patients with ASA ≥3, but not patients with milder ASA grades. This is consistent with previous reports that ASA grades 3-5 are associated with greater risk of adverse events after spinal tumor surgery.34,35 In contrast, our subgroup analysis did not detect differences in the risk association between patients older or younger than 65 years, or between patients who experienced anemia preoperatively or not. These negative results contrast with work suggesting higher incidence of serious postoperative complications among older patients undergoing radical surgery to treat spinal metastases, 36 and work linking preoperative anemia to worse prognosis among patients undergoing major non-cardiac surgery. 37 These negative results in our study should be interpreted with caution in light of our small, relatively young sample.
In fact, our work is limited by the fact that our sample came from a single center and was analyzed retrospectively. We did not collect data after discharge, nor did we analyze troponin levels or neurological indicators postoperatively, which could have detected all myocardial and cerebral ischemic events. Future work should avoid these limitations to order to clarify the prognostic usefulness of postoperative nadir hemoglobin level, and it should measure postoperative nadir levels multiple times to ensure detection of the true value. Future studies should explore whether postoperative nadir hemoglobin levels also have prognostic value for patients who do not receive intraoperative blood transfusions during spinal tumor surgery.
Conclusions
Our study suggests that patients undergoing spinal tumor surgery should maintain a hemoglobin level of at least 9.0 g/dL postoperatively in order to reduce risk of composite adverse events. This may be especially important for patients who are male or who have preoperative ASA grade ≥3.
Supplemental Material
Supplemental Material - Nadir Hemoglobin Concentration After Spinal Tumor Surgery: Association With Risk of Composite Adverse Events
Supplemental Material for Nadir Hemoglobin Concentration After Spinal Tumor Surgery: Association With Risk of Composite Adverse Events by Xuena Wang, Jiachun Tao, Yinbo Zhong, Yuanyuan Yao, Tingting Wang, Qi Gao, Guangxin Xu, Tao Lv, Xuejie Li, Dawei Sun, Zhenzhen Cheng, Mingxia Liu, Jingpin Xu, Chaomin Wu, Ying Wang, Ruiyu Wang, Bin Zheng, and Min Yan in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.