
Abstract
Study Design
Survey study.
Objectives
People living with spinal cord injury (SCI) are major healthcare and rehabilitation services consumers and have unmet healthcare needs. This study aimed to describe the socioeconomic characteristics of people living with SCI in Spain and to determine the level of use and satisfaction with the public healthcare system.
Methods
We conducted a survey (the Spanish version of the International Spinal Cord Injury Community Survey) consisting of 134 questions. We analyzed the age, sex, neurological classification of the injury on the American Spinal Injury Association Impairment Scale, time of injury, socio-occupational and socioeconomic status, and level of use and satisfaction with the public health system.
Results
472 people responded to the survey [68.9% male; mean age 51.2 years (standard deviation: 13.9 years); 61.7% with paraplegia and 38.3% with tetraplegia]. 89.2% of those surveyed were unemployed and 77.1% received a disability pension. The number of medical visits was 2.3/year, and 19.8% of the patients required at least 1 hospital admission during the previous year. 94.7% of the people with SCI considered the health care received as good or very good.
Conclusions
Respondents with SCI in Spain considered they had good access to primary and specialized care and were satisfied with the healthcare system. Notably, we observed a high average of annual visits to medical professionals but a low rate of hospitalizations. Technical aids and state services related to disability should be the most important elements to be improved.
Introduction
Up to 1 200 new spinal cord injuries (SCI) occur each year in Spain, and approximately 40 000 Spaniards live with SCI. 1 These injuries can be the consequence of an accident or traumatism, a congenital disorder, a disease, or a degenerative process. The level and intensity of the injury determine the level of motor, sensory, and autonomic nervous system damage leading to dysfunction in various organs.2-6 Because of the multifaceted nature of the injury, people with SCI are major consumers of healthcare and rehabilitation services. 7 Only a small number of patients with SCI receive healthcare from primary care8,9 or family doctors. The optimal standard of care for people with SCI is still unclear.10-12
Evidence is contradictory on the effectiveness of outreach programs in monitoring health status and preventing complications after SCI.13-16 However, regular follow-up by specialized teams and annual comprehensive health examinations by SCI specialists are obvious methodologies to achieve these goals in this group of patients.17-21 From the primary care perspective, the most common problems of people with SCI are related to neurological impairment, specifically, secondary complications (eg, neuropathic pain, spasticity, intestinal and/or bladder dysfunction, altered bone density and fractures, depression and emotional adjustment, sexual and reproductive health issues, and function alterations derived from ageing).22-24 As a result of population ageing, the number of incidents resulting in SCI is increasing since degenerative changes in the spine increase the risk of SCI.1,25 Furthermore, the elderly are more vulnerable to SCI, either from traumatic or non-traumatic events.26-29 On the other hand, evidence points towards unmet healthcare needs among people living with SCI. Specialised knowledge and expertise to manage multisystem impairments is needed to treat people with SCI, which may understandably be unreached for general practitioners.11,12
As far as we know, there is no data on the characteristics and the use of the healthcare system of people living with SCI in Spain. Few researchers have studied these epidemiological data all over the world. Both Hamilton et al 30 and Stillman et al 31 had conducted a similar survey but exclusively recruited participants from a single center in the USA. Small sample sizes (just over one hundred participants) and therefore potentially low representatives were reached. Were only Ronca et al 32 who relied on a diverse and representative sample of almost five hundred individuals with SCI in an entire country (Switzerland). They focused their research on accessibility to adequate healthcare services, thus corresponding representation of data is not reached to be comparable to our study.
The aims of this study were to describe the socioeconomic characteristics of people with SCI in Spain and to determine the level of use of the public healthcare system, both at the primary and specialized care level, as well as the degree of satisfaction of these patients with the system.
Materials and Methods
Study Design
The International Spinal Cord Injury (InSCI) Community Survey is a cross-sectional multinational study conducted in the community that includes 22 countries from the 6 WHO regions and was conducted between 2017 and 2019 to comprehensively describe the experience of people with SCI living in the community. 33 Our study used the data collected in Spain by analysing the socioeconomic characteristic of people living with SCI and their use and experience of the public health system. The sampling frame was 4 SCI units of the Spanish National Healthcare System: Hospital Universitario Vall d’Hebron (Barcelona), Hospital Universitario Virgen del Rocío (Seville), Hospital Universitario Insular Materno-Infantil de Gran Canaria (Canary Islands), and Hospital Universitario de Cruces (Bilbao). They are representative of rural and urban populations and cover different economic areas, such as agricultural activity (12.4%), industry (13.7%), services (28.3%) and construction (2.8%). In terms of coverage, these 4 healthcare facilities manage 47.5% of Spain’s total population because they are reference centers of extended densely populated Spanish areas.
The information was provided by the minimum set of basic hospital discharge data and by the database of each of the 4 SCI units. The patients were contacted in outpatient clinics and attended the interview inperson.
Participants
Eligible persons are adults >18 years of age with traumatic and non-traumatic SCI, with a neurological level of the lesion classified as A, B, C, or D in the American Spinal Injury Association Impairment Scale 34 and monitored in an SCI unit, living in the community, and whose injury happened at least 1 year before the interview. Eligible subjects lived in Spain and had to be able to respond in Spanish and give their informed consent to participate in the survey.
Excluded are persons with spinal cord damage due to congenital etiologies such as spina bifida, or neurodegenerative disorders such as multiple sclerosis, amyotrophic lateral sclerosis (ALS), or peripheral nerve damage such as Guillain-Barré Syndrome. Persons who are inpatients receiving first rehabilitation or first acute care at the time of the study are also excluded owing to lack of community experience with SCI.
Survey
Distribution of Questions of the International Spinal Cord Injury Community Survey.
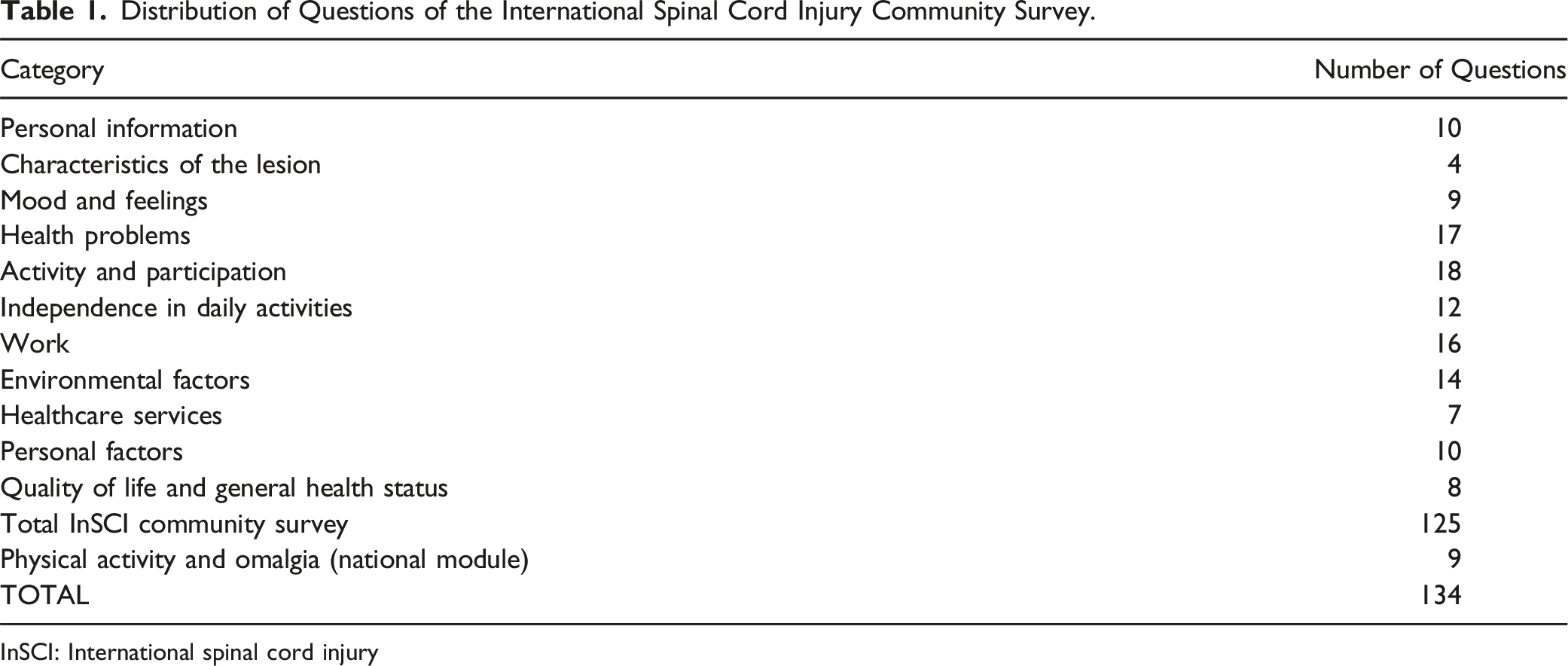
InSCI: International spinal cord injury
Statistical Analysis
We used the mean and standard deviation (SD) to describe continuous variables and the median and ranges for categorical variables. For statistical analysis, we used SPSS software (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp).
Ethics
All participants signed an informed consent form to indicate their willingness to take part in the study. The study was approved by the Clinical Research Ethics Committee of each involved Hospital: Hospital Universitario Vall d’Hebron (Barcelona) on October, 2016 (PR(ATR)285/2016); Hospital Universitario Virgen del Rocío (Seville) on March, 30th, 2017; Hospital Universitario Insular Materno-Infantil de Gran Canaria (Canary Islands) on February, 2017; and Hospital Universitario de Cruces (Bilbao) on August, 2017.
Results
Characteristics of SCI Population.
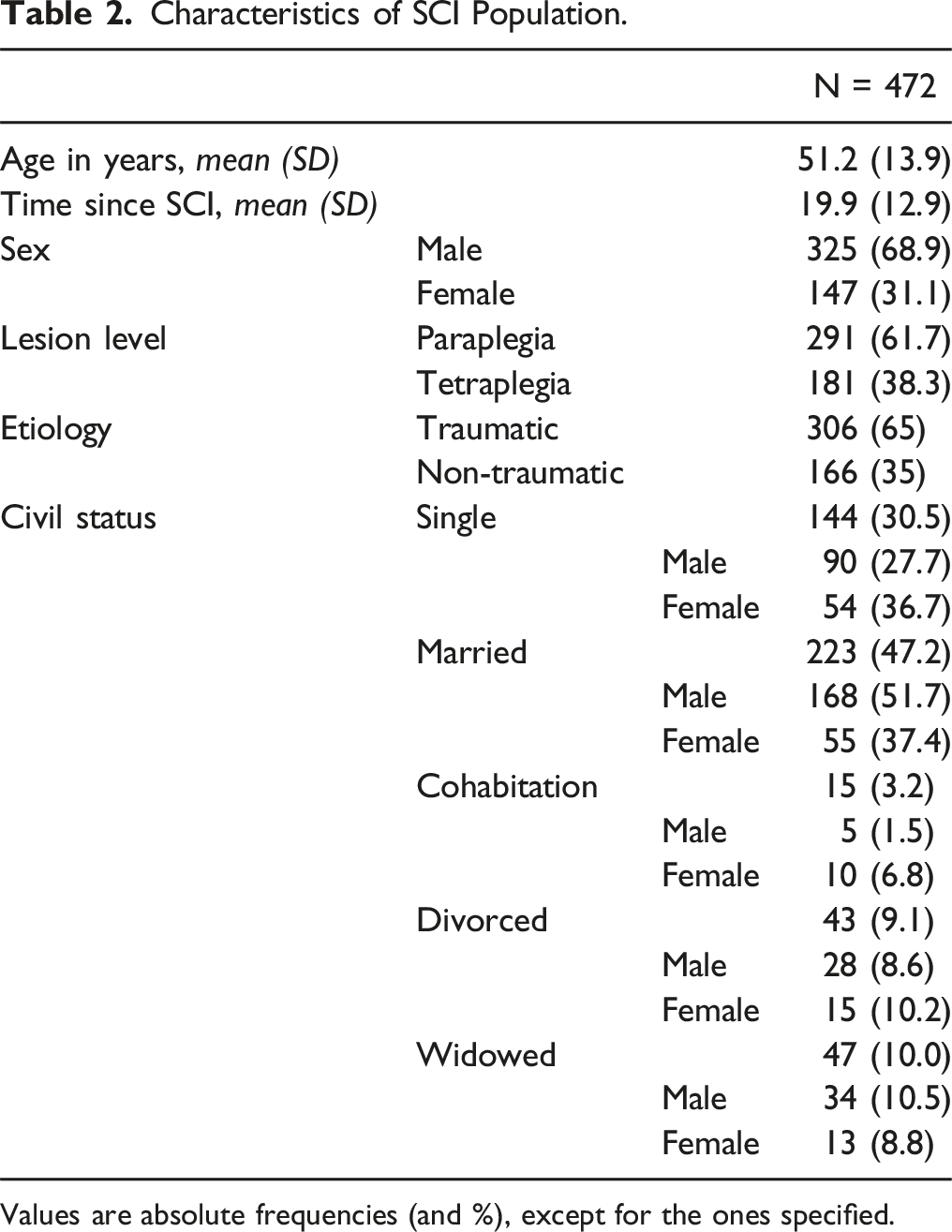
Values are absolute frequencies (and %), except for the ones specified.
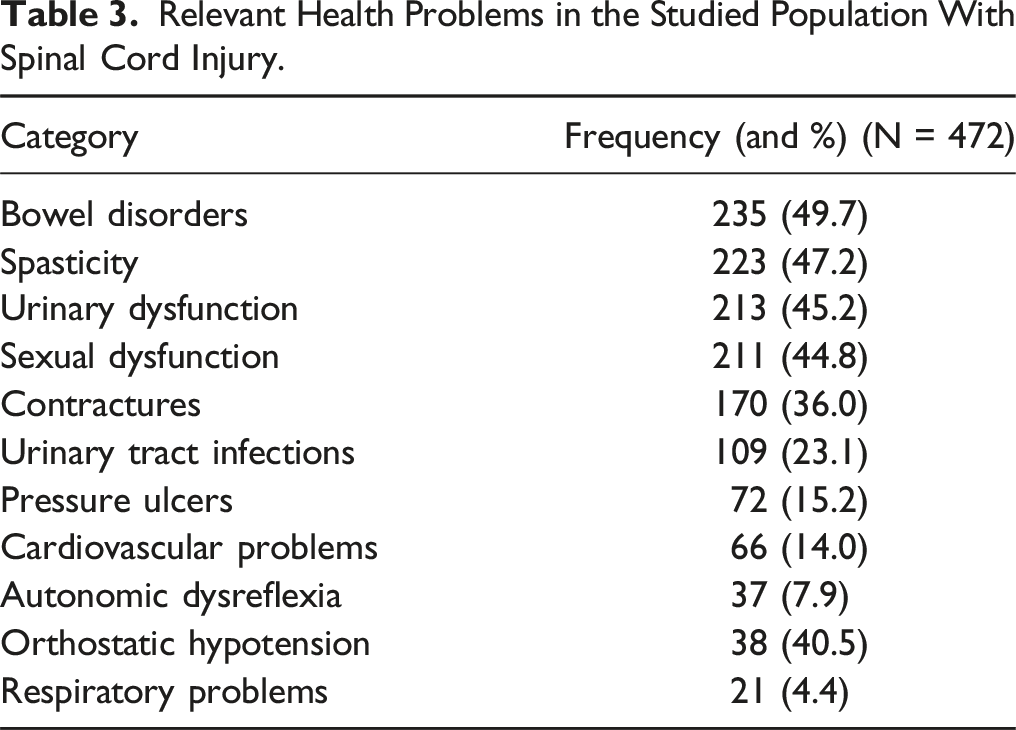
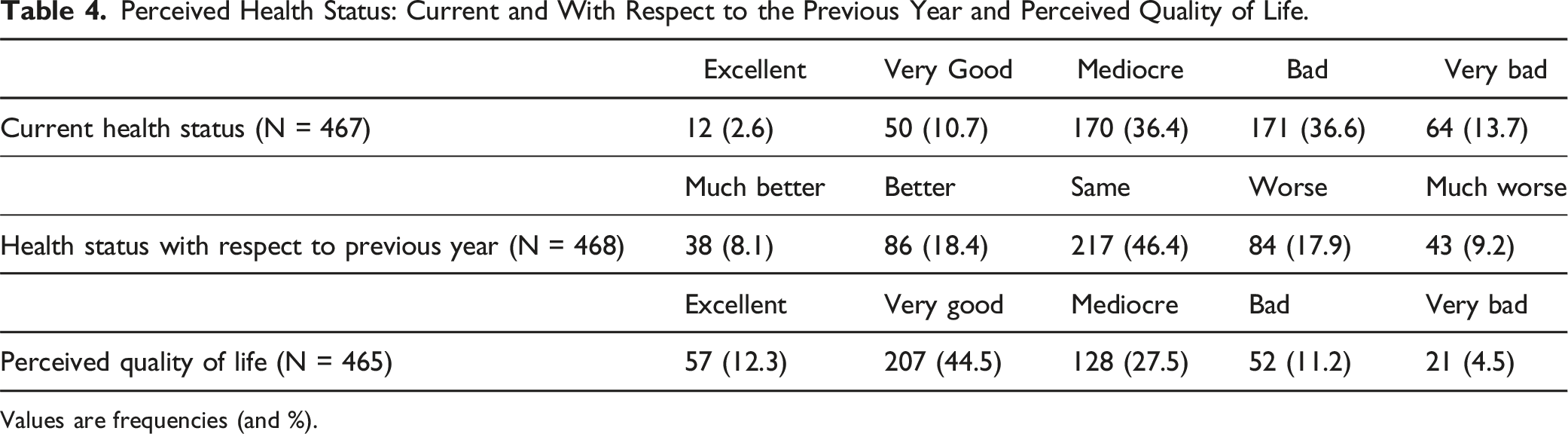
The monthly average income was between 1641 and 1750 € and its distribution can be seen in Figure 1. The vast majority were unemployed (382, 89.2%) and received a disability pension (364, 77.1%). The most relevant health problems included: bowel disorders, urinary and sexual dysfunction, and spasticity and pain (Table 3). Half of the respondents (235, 50.3%) considered their perceived state of health as bad or very bad and most (217, 46.4%) felt the same 1 year later (Table 4). On the other hand, the perceived quality of life was mostly good or very good (264, 56.8%) (Table 4). Gross monthly income of the studied population. Absolute frequencies and % are represented in the graph. Relevant Health Problems in the Studied Population With Spinal Cord Injury. Perceived Health Status: Current and With Respect to the Previous Year and Perceived Quality of Life. Values are frequencies (and %).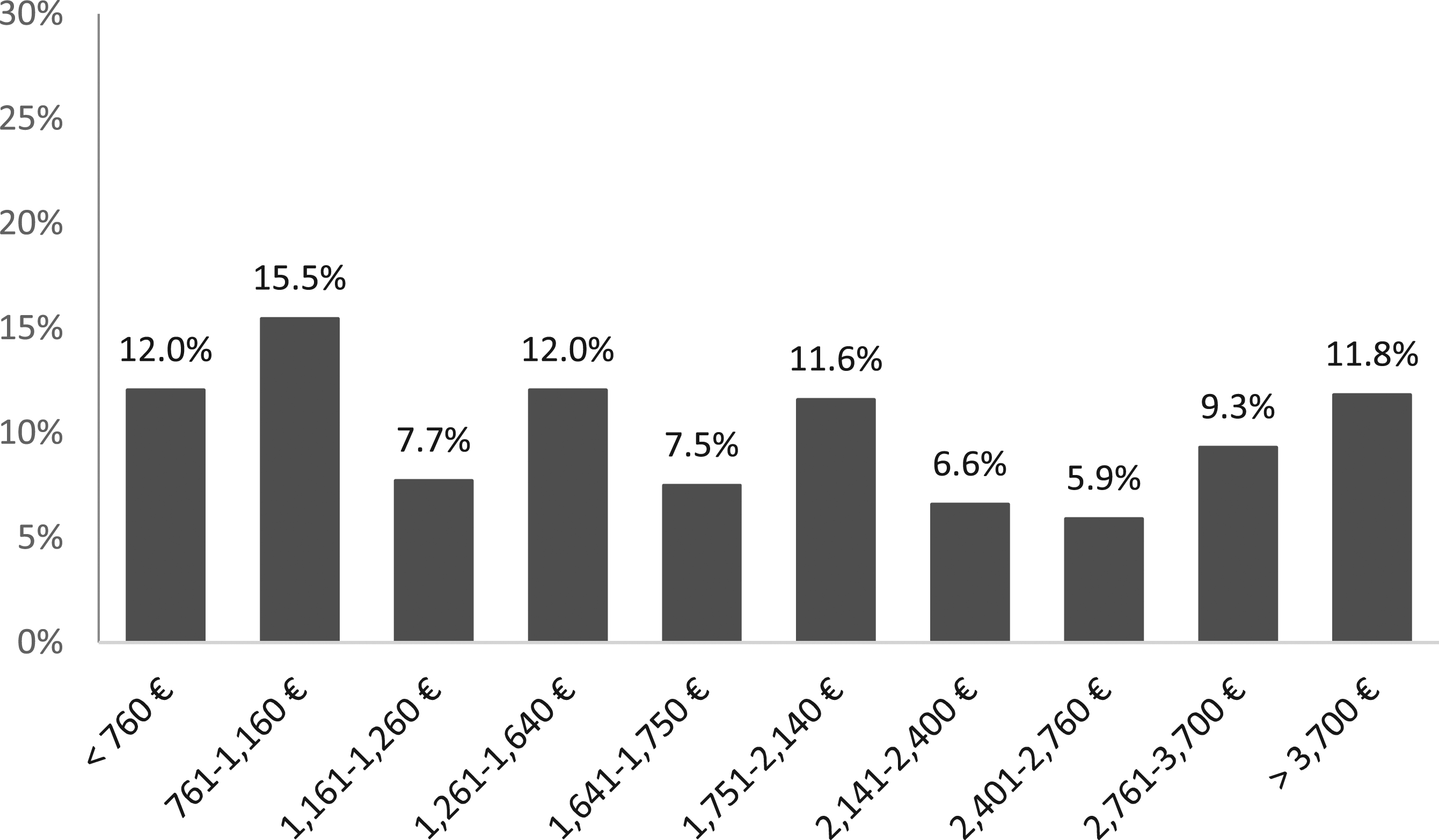
Notably, most of the respondents considered that neither the relationship between the environment and their personal conditions (377, 83.5%), the negative social attitudes (385, 85.5%), nor family or friends' attitudes (439, 97.5%) had an impact on them. Similarly, the lack of technical aids to move around did not influence them (294, 65.1%), and the majority (341, 75.7%) considered that state services regarding their disability were sufficient and had no effect on their status.
Figure 2 summarizes the healthcare visits of the subjects with SCI during the previous year. In total, they visited 1 152 health professionals, with an annual average of 2.3 visits to medical professionals per year. The most visited were primary care physicians (320, 68%) and rehabilitation physicians (270, 57.4%). In the same period, there were 158 hospital admissions and 94 patients (19.8%) required at least 1 admission. Furthermore, 434 (94.8%) patients acknowledged that the healthcare in their area or hospital had been very good or good (Table 5). Regarding treatment, 423 (92.4%) indicated that the explanation had been very good or good, and 374 (82.7%) considered that they were able to discuss and share decisions (Table 5). Finally, for the most part (84.5%), the respondents deemed that the medical supplies were provided with the desired frequency. Visits to healthcare professionals by patients with SCI in the last 12 months. Perceived Experience With Healthcare, Treatment Explanations, And Shared Decision-Making. Values are absolute frequencies (and %).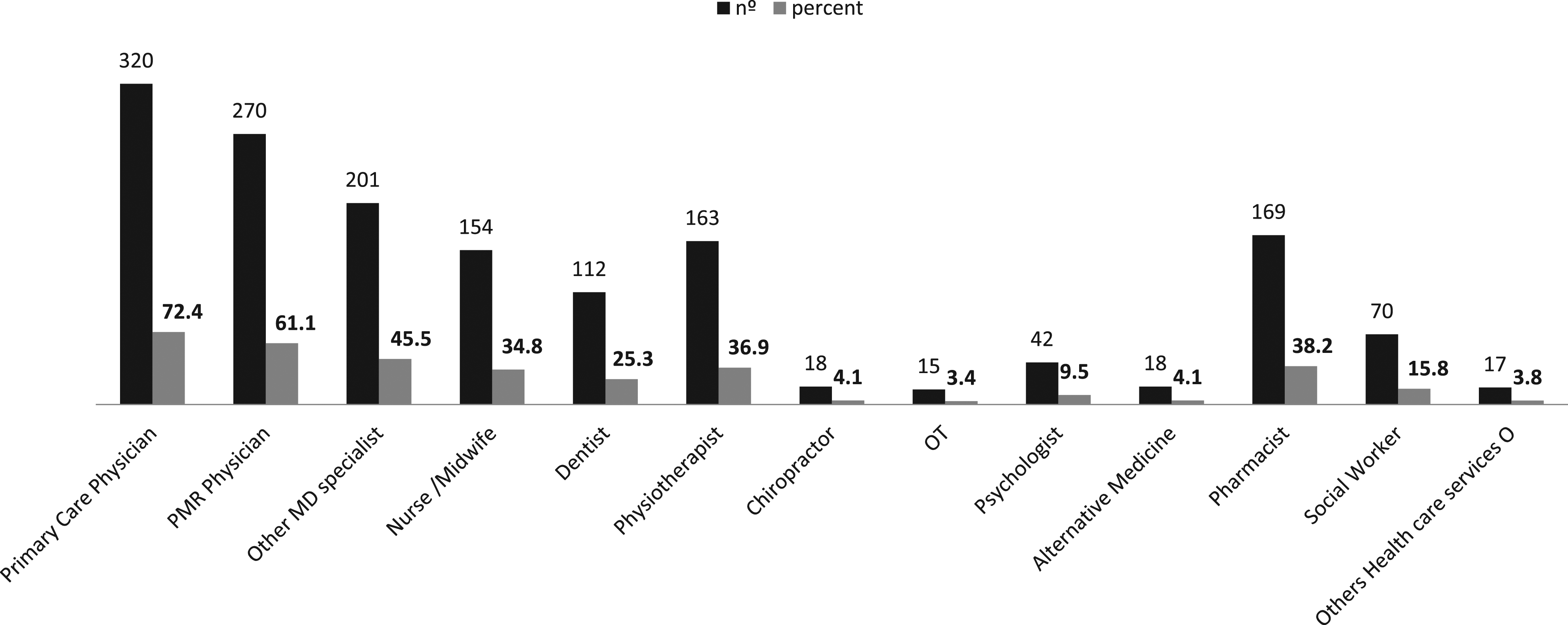

Discussion
Through the InSCIsurvey, this study assessed the socioeconomic characteristics of patients with SCI in Spain and their level of use and satisfaction with the public health system. The results showed that the majority had paraplegia, were unemployed but received a disability pension, considered their health status perceived as bad or very bad and without progression after 1 year, were not affected by external relationships, and felt that state services regarding disability were enough. In addition, the health professionals most visited were primary care and physical medicine and rehabilitation doctors, and satisfaction with the health system and with explanations about treatments was extremely high.
Reports covering various population groups with SCI worldwide have demonstrated that epidemiological characteristics have changed in recent decades.25,37-41 There is a growing body of evidence on the increase in the average age of patients with traumatic SCI, a circumstance that can have a great impact on rehabilitation programs and the healthcare continuum. 42 In our study, the mean age and follow-up time were higher than in similar studies, implying our patients had several health comorbidities beyond those of SCI.14,15,22 Within the international InSCI study, Spain was the eighth country with the largest sample of the 22 participating countries. 43 Although the median income was high among our respondents (compared to Spanish interprofessional minimum wage of 2019, valued at 900€/month), 44 our results showed that most were unemployed and lived on a disability pension. Previous studies have shown that the poor financial situation of these patients is a barrier 45 and that it can affect their access to medical care. 46 In addition, in studies undertaken in the EU and Canada, the rate of employed persons with SCI was much lower than that of persons without disabilities, which could be explained by the executive limitations in vocational rehabilitation.47,48 It is worth to mention that in Spain, according to the Social Security Law, total permanent or severe disability pension is incompatible with holding a position in the same category or professional group. In consequence, different and acurated work inclusion policies are needed to improve economic conditions of SCI population in Spain.
As expected, a high incidence of health problems was observed in this group of patients, mainly related to intestinal dysfunction, urinary dysfunction, and spasticity and pain, besides other problems (eg, contractures, pressure ulcers) that limit their function and social participation and socio-occupational integration. Several studies have reported that individuals with SCI are treated for around 8–14 secondary conditions per year,49-51 which can complicate their health status and impact productivity/employment, dignity, mobility, independence, and quality of life. 52 Furthermore, these conditions can worsen if not managed properly and lead to hospitalizations.2,53
Our findings indicated that the structure and availability of services to manage these patients were appropriate and had little influence on the personal and social life of individuals with SCI. On the other hand, the results obtained showed a Spanish society well-developed regarding its perceptions and actions in relation to disability: negative social and family attitudeswere very scarce.
The economic impact of SCI on healthcare providers and the system has become an increasingly important topic of concern. 54 For example, the economic burden associated with the life of a person with SCI in Canada has been described to range from 1.47 million CA$ for a person with incomplete paraplegia to 3 million CA$ for a person with complete tetraplegia. 55 In this regard, the rate of annual visits to health professionals in our study was higher than that described in previous studies.19,24 2.3 visits to medical professionals per year is a reasonable rate for people with SCI. Therefore, healthcare in Spain for this population is suitable and correctly dimensioned.
On the contrary, the rate of hospitalizations observed in our sample was lower than that reported by other authors.16,18 This can be explained by the model of care for SCI in Spain, carried out by healthcare specialist familiar with the condition and its complications and who establish systematized standards of care. In this sense, patients with SCI have been previously reported to prefer specialized care and feel happier when receiving follow-up care from rehabilitation specialists.15,56,57 The organization of SCI specialized care in Spain address this issue, given that systematic and systematized approaches are carried out by applying the guidelines promoted by the Spanish Society of Paraplegia (Sociedad Española de Paraplegia). 58
Of note, our results indicated that the availability of means for socialization could be improved, given the number of respondents who reported insufficient technical aids that impacted importantly or very importantly on their life. We consider that this could be 1 of the elements to be improved for SCI patients. Similarly, state services related to disability could be upgraded since almost a quarter of the respondents indicated that the insufficiency of these services made their lives more difficult. 59 Although it is a noticeable problem, the solution is not easy. Since 2 ministeries, Health Ministry and Equality and Social Servicies Ministry, are coresponsible for this subject, an agreement on the policies concerning SCI population is difficult to achieve.
Our study has the intrinsic limitations of descriptive studies, especially compared to systematic reviews. However, the former provides an accurate image and sufficient information that allows continuing with specific and valid research questions through a study with a careful process of scrutinizing evidence from different methodologies and designs. 60
Although the size of our sample was important, it could also be considered limited since only 1.2% of people with SCI in Spain were represented, although this percentage is probably higher given the inclusion criteria (eg, people who live in the community, adults). Further studies with an extended sample are required to better know SCI population in Spain. Importantly, the number of respondents varied slightly for each module, which precluded a constant denominator for our percentages. In addition, albeit the theoretical frameworks that have guided the analysis of the information have been carefully chosen and weighted against other competitive models, alternative analytical, valid frameworks could have been used.
Conclusions
Through the InSCIsurvey, we observed in this study that SCI patients in Spain showed a high incidence of health problems but had good access to primary and specialized care. However, the annual average number of visits to medical professionals during the year prior to the survey was high, although the number of hospitalizations was low. Our survey highlighted the good acceptance and assessment of the healthcare system, which showed an appropriate structure and availability of services. Our results could be used to (i) modify the services provided to cover unmet needs, (ii) conceive new studies and develop new interventions, and (iii) adapt and adjust existing programs according to the needs of SCI patients.
Footnotes
Acknowledgments
The authors would like to thank Karla Rojas Cuotto, Xurxo Segura Navarro, Carolina Alemán Sánchez, María José Zarco Periñan, Arrate Orueta Olabarria, Montserrat Cuadrado Rebollares, and Inés Lodeiro Mendieta for their contribution to the study. The authors also thank Matías Rey-Carrizo at BCN Medical Writing for providing medical writing support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.