
Abstract
Study Design
Retrospective cohort study.
Objective
Magnetic Resonance Imaging (MRI) is often regarded as the gold standard for spinal pathology, as it provides good structural visualisation. SPECT-CT, however, provides combined structural and functional information. There is a paucity of literature comparing SPECT-CT with MRI in the spine. Our aim was to determine whether SPECT-CT provides additional information to MRI in individuals with complex spinal pathology, including deformity, which altered management.
Methods
We conducted a retrospective review of all individuals seen at our tertiary spinal unit that were investigated with both MRI and SPECT-CT of the spine between 2007-2020. We reviewed imaging reports, and collated diagnoses, surgical treatment and the relative contributions of MRI and SPECT-CT to management decisions.
Results
104 individuals identified, with a mean age of 30 years (89 females and 15 males). Diagnostic categories were adolescent, adult, and congenital deformity, degenerative pathology, and miscellaneous pathology. MRI returned positive findings in 58 (55.8%), and SPECT-CT in 41 (39.4%) cases. SPECT-CT identified 10 cases of facet joint degeneration, 5 of increased uptake around metalwork suggestive of loosening, 1 pseudoarthrosis, 1 partial failure of fusion and 1 osteoid osteoma which were not reported on MRI, all in individuals who had previously undergone spinal instrumentation. Despite this, SPECT-CT only altered management for 6 individuals (5.8%).
Conclusion
MRI is less useful in the setting of previous instrumentation due to metal artefact. Where MRI is inconclusive, particularly in individuals with previous spinal instrumentation, SPECT-CT may provide a diagnosis, but is not recommended as primary imaging.
Introduction
Single-Photon Emission Computed Tomography (SPECT) demonstrates increased osteoblastic activity much earlier in the pathologic process than most static imaging modalities. 1 Historically, SPECT was often used in combination with planar scintigraphy and, whilst this gives important functional information with good sensitivity, the specificity is low due to poor anatomical localisation. 2 Combining SPECT with standard Computed Tomography (CT) into SPECT-CT solves this as it combines the benefits of functional and structural information with an improved anatomical accuracy. 3 There are instances in clinical practice where the generally accepted ‘Gold Standard’ for spinal imaging, Magnetic Resonance Imaging (MRI), may show pathology, but does not necessarily help us identify pain generators. In these cases, the functional component of SPECT-CT provides a theoretical advantage, as it highlights areas of increased metabolic activity, with blood flow as the surrogate marker. The caveat to this is the risk of additional exposure to ionising radiation from CT, which is compounded by the radioactive contrast exposure from the SPECT element of the scan. 4
SPECT-CT has been demonstrated to improve diagnostic confidence in differentiating benign from malignant lesions when investigating known or suspected cancer.5,6 It has a good specificity for excluding infection and in confirming a lack of cellular activity at the fracture site in non-unions of long bone fractures. 7 There have been several small clinical series over the previous decade focusing on the utilisation of SPECT-CT for the imaging of the painful post-operative spine. The consensus from these studies is that SPECT-CT can help in identifying pain generating pathologic lesions such as pseudoarthroses, metalwork loosening and facet joint degeneration.2,8–14 SPECT-CT has also been used to identify primary pain generators in degenerative spinal disease, helping to instigate appropriate treatment and avoiding the unnecessary use of invasive spinal fusion surgery.15,16 SPECT-CT has also been shown to have utility in predicting pain relief following vertebroplasty. 17
There are numerous studies that report a higher sensitivity and specificity of SPECT-CT in detecting pathology than either planar scintigraphy or plain CT alone.5,6,9,14 SPECT-CT has been noted as being highly valuable when other imaging modalities are inconclusive or contraindicated.6,13,17,18 Compared with MRI, SPECT-CT has been found to provide additional diagnostic information and guide treatment in complex foot and ankle pathology 19 and to be superior in detecting implant loosening in painful hip arthroplasty. 20
The comparative roles of MRI and SPECT-CT in complex spinal pathology has not been reported. The aim of this study was to evaluate whether SPECT-CT provided any additional diagnostic information compared with MRI when dealing with complex spinal pathology.
Methods
From a prospectively maintained radiology database, we performed a retrospective service evaluation of all individuals who underwent SPECT-CT between November 2007 and July 2020. The project was registered locally at our institution and all appropriate guidelines were adhered to (local Project Number:20-022). All data were strictly anonymised and no informed consent was required. From this cohort, we excluded all individuals that were not investigated with MRI of the spine within six months of SPECT-CT. The predominant symptom and indication for MRI was pain. Indication for SPECT-CT was failure to identify a definitive cause for pain on MRI. In cases where there were multiple spinal MRI scans on the system, we identified the scan performed closest in time to the SPECT-CT as the MRI reviewed for this study. MRI and SPECT-CT reports were reviewed on Picture Archiving and Communication System (PACS). Where no report was available, the imaging was reviewed and reported on by a specialist musculoskeletal radiologist. All MRI (3 Tesla Magnetom Skyra, Siemens) consisted of T1 and T2 axial sequences, and T1 and T2 sagittal Short Tau Inversion Recovery (STIR) sequences, with metal artefact reduction. SPECT-CT was carried out by administration of a radionuclide tracer and initial imaging with a gamma camera, immediately followed by CT scan (Spectrum Dynamics Veriton 64, and Siemens Symbia Pro.specta). CT slice thickness was 0.625 mm. The two modalities were then co-registered to provide the hybrid SPECT-CT images.
Paper and electronic clinical notes were reviewed to collect data on demographics, diagnoses, and prior surgical treatment. We reviewed the reports to document whether the MRI and SPECT-CT findings were positive or negative. MRI scans that failed to identify any new pathology which could account for patient symptoms, or had degraded images due to metal artefact were documented as negative. Similarly, SPECT-CT scans which did not identify any pathology which could explain symptoms were classed as ‘negative’. Note was made on whether the SPECT-CT provided any additional information over the MRI scans.
Results
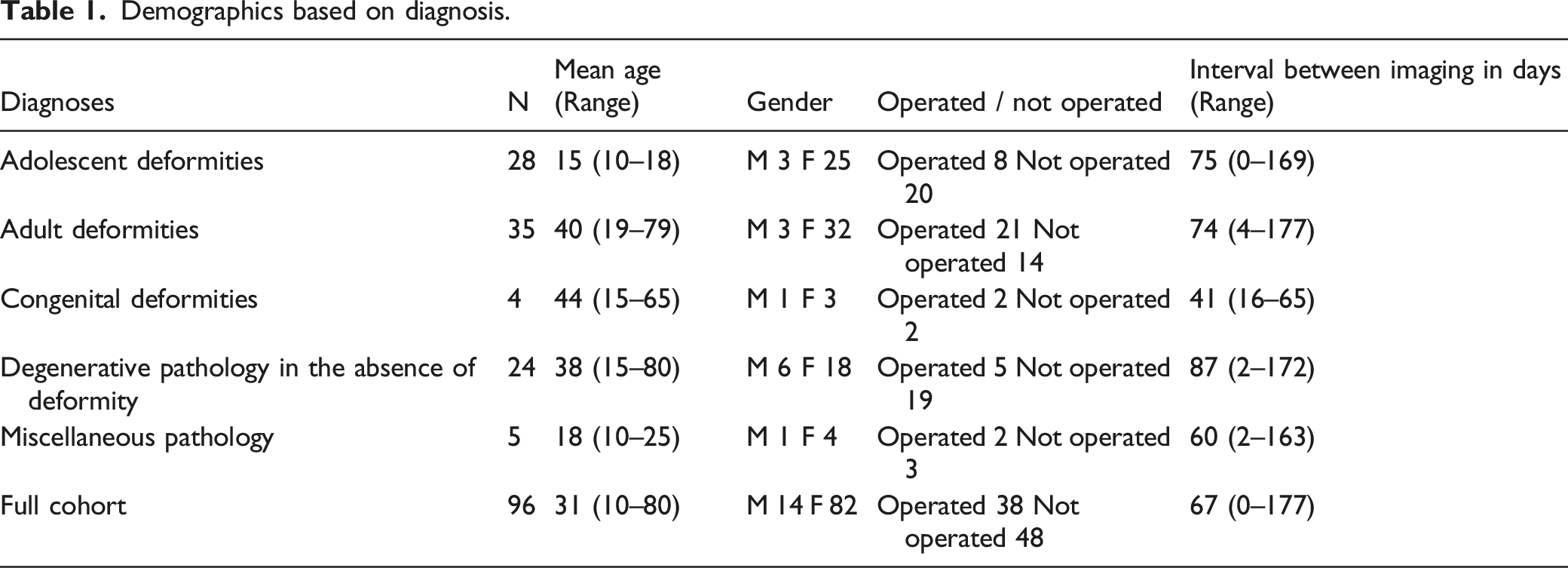
Demographics based on diagnosis.
Adolescent Deformities
This sub-group comprised of 25 female and 3 male (28/96, 29.2%) individuals with a mean age of 15 years (range: 10-18). 2/28 (7.1%) had a diagnosis of Scheuermann’s disease and the remainder (92.9%) had adolescent idiopathic scoliosis (AIS). The majority of the individuals (20/28, 71.4%) were treated non-surgically; of the eight individuals who were operated upon, there were two combined anterior and posterior instrumented fusions, and six posterior instrumented fusions. Predominant symptom and reason for imaging was pain in 28 patients, and altered neurology in 2 patients. Average time from MRI to SPECT-CT was 75 days (0 — 169). There were 26 MRI whole spine and 2 lumbar-sacral only.
MRI was classed as negative in 22 cases (78.6%). Abnormal findings included degenerative changes (n = 2), neural axis abnormality (n = 2), non-specific or post surgical changes (n = 1) and spondylolisthesis (n = 1).
3/28 individuals (10.7%) had a positive SPECT-CT result, only one of whom had previously undergone spinal instrumentation (posterior fusion). This individual had facet joint changes in a non-instrumented segment (Figure 1), as well as some increased uptake around the implants. The facet joint degeneration was not reported on the initial MRI scan. Despite this, SPECT-CT did not lead to any significant change in management for any patient in this cohort. (A) Coronal SPECT-CT image demonstrating increased uptake around facet joints. (B) Coronal SPECT-CT image demonstrating increased uptake around facet joints. (C) Sagittal SPECT-CT image demonstrating increased uptake around facet joints.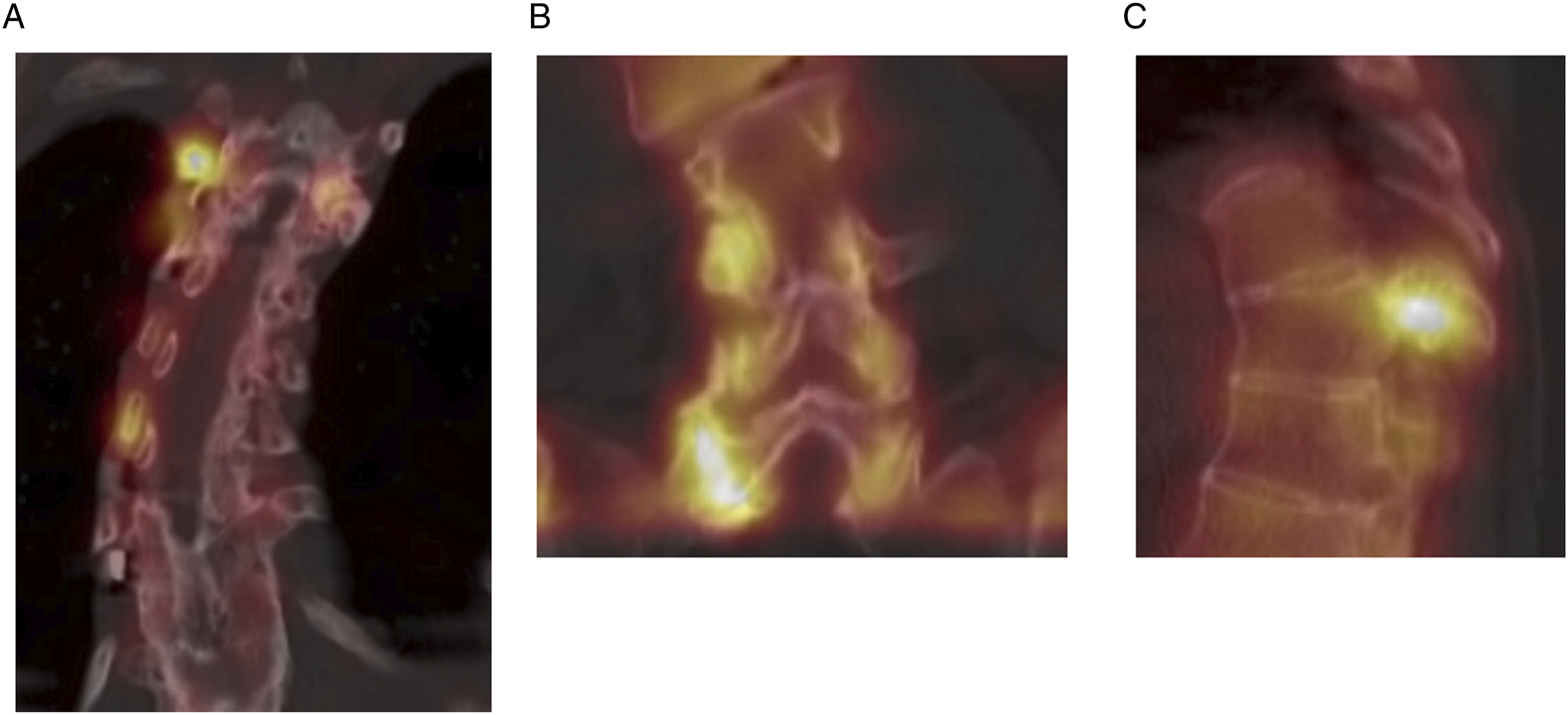
Adult Deformities
This cohort comprised 35/96 (36.5%) individuals and was sub-analysed as de novo adult deformity secondary to degeneration (mean age 67 years, range: 44-79), comprising 11/35 (31.4%) individuals, and adults previously diagnosed with AIS presenting with new symptoms (mean age 27 years, range: 19-49), comprising 24/35 (68.6%) individuals. Average time from MRI to SPECT-CT was 74 days (4 — 177). There were 21 MRI whole spine, nine lumbar-sacral, three thoracolumbar, one thoracic only, and one cervicothoracic only. Predominant symptom and reason for imaging in all patients in this cohort was pain.
In the de novo group, five individuals (45.5%) had previously received spinal surgery (all posterior instrumented fusions), four of whom had a positive SPECT-CT scan. 16/24 (66.7%) of the adult AIS group were previously operated upon (12 posterior instrumented fusions, three combined anterior and posterior instrumented fusions, and one anterior only fusion. Four individuals also underwent revision posterior procedures). 11 of the operated individuals had a positive SPECT-CT scan.
MRI was negative in 15 cases (42.9%). Abnormal findings included degenerative changes (n = 17), facet degeneration (n = 5), non-specific or post surgical changes (n = 3), and neural axis abnormality (n = 1).
The positive SPECT-CT results included spondylotic changes in the un-instrumented segments (n = 11), facet degeneration (n = 6), non-specific uptake (n = 3), and an increased uptake around the implants (n = 3), including one partial failure of fusion. SPECT-CT led to a change in management in three individuals (8.6%) who demonstrated facet joint degeneration not reported on initial MRI (two of whom had previous spinal instrumentation). All three underwent successful CT-guided facet joint injections.
Congenital Deformities
The four individuals in this group had a mean age of 44 years (Range: 15-65), and consisted of three females and one male. Two individuals had previously undergone spinal instrumentation (both posterior instrumented fusions). Predominant symptom and reason for imaging was pain in 3 patients, and altered neurology in 1 patient. Average time from MRI to SPECT-CT was 41 days (16 — 65). All four underwent MRI whole spine.
MRI was negative in in only one case. All three positive scans demonstrated degenerative changes, with one individual also exhibiting facet degeneration.
SPECT-CT was positive in three cases (75%) including one operated patient; one pseudoarthrosis in a patient with previous instrumentation (Figure 2), and two cases of facet degeneration. None of these pathologies were reported on the respective initial MRI scans. Despite this, however, SPECT-CT did not alter management in any of the individuals in this sub-group. Sagittal T2 MRI (A) and SPECT-CT (B) imaging; SPECT-CT demonstrates increased uptake confirming pseudoarthrosis proximally (P) as well as facet joint degeneration (F) distal to construct.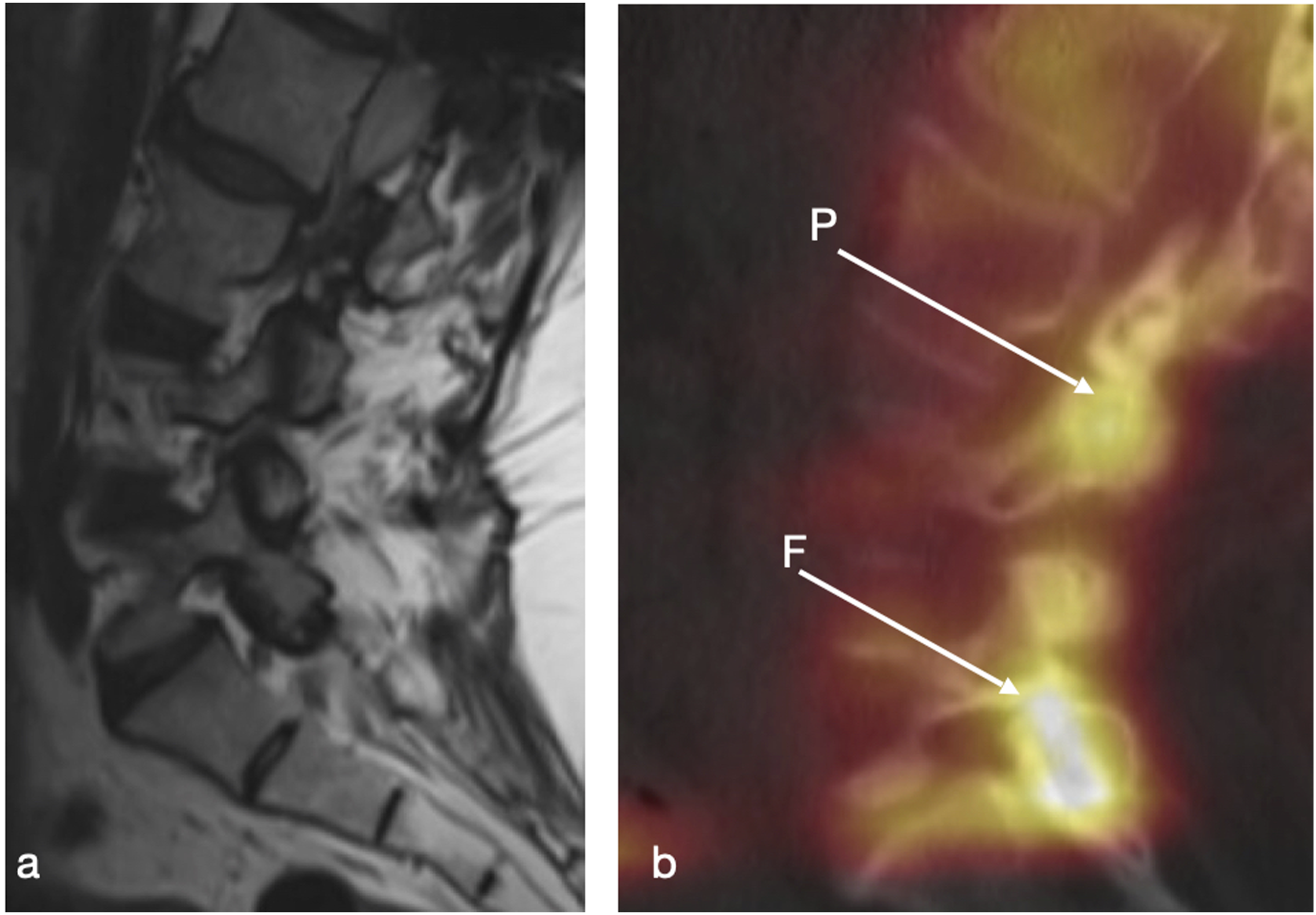
Degenerative Pathology in the Absence of Spinal Deformity
This subgroup comprised 24/96 individuals (25%) with a mean age of 38 years (range: 15-80), comprising 18 females and 6 males. Predominant symptom and reason for imaging in all patients in this cohort was pain. Average time from MRI to SPECT-CT was 87 days (2 — 172). There were 14 MRI whole spine, 6 lumbar-sacral, 3 thoracolumbar, and 1 cervical only. Five individuals had previously undergone spinal surgery (three laminectomies and two posterior instrumented fusions). Five of these had increasing degenerative changes, whilst one patient demonstrated insufficiency fractures.
MRI was negative in 7 (29.2%); positive findings included degenerative changes (n = 14), facet degeneration (n = 2), non-specific/post-surgical changes (n = 2), wedge compression fracture (n = 2), and pars defect (n = 1).
SPECT-CT was positive in 12 (50%): findings included non-specific uptake (n = 6), widespread degenerative changes (n = 5) and a pars defect (n = 1). SPECT-CT did not detect any pathology that was not already evident on MRI and led to no alteration in management for any in this cohort.
Miscellaneous Pathology
In addition to the above sub-groups, there were five individuals with independent diagnoses - Ewing sarcoma, Neurofibromatosis type 1 (with associated dystrophic scoliosis), arthrogryposis, osteoid osteoma, and Marfan’s syndrome (with associated scoliosis). The mean age was 18 years (range: 10-25), consisting of 4 females and 1 male. Predominant symptom and reason for imaging was pain in 4 patients, and altered neurology in 1 patient. Average time between scans was 60 days (2 — 163). There were 4 MRI whole spine and 1 lumbar-sacral only.
Two individuals had previously undergone spinal surgery (posterior instrumented fusions).
Miscellaneous group individual diagnoses and respective imaging findings.

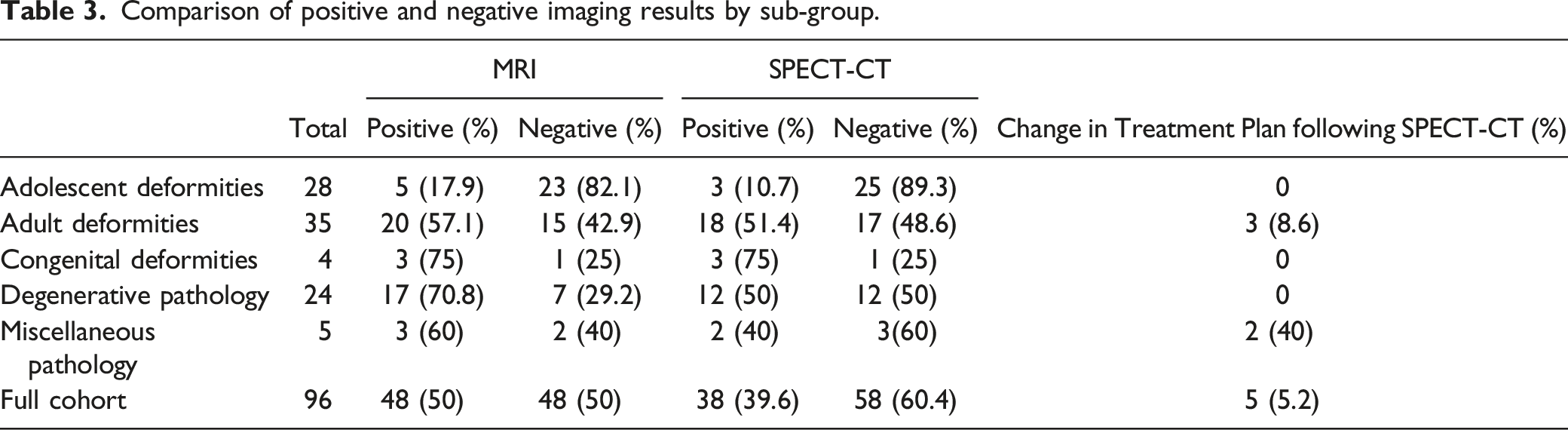
Comparison of positive and negative imaging results by sub-group.
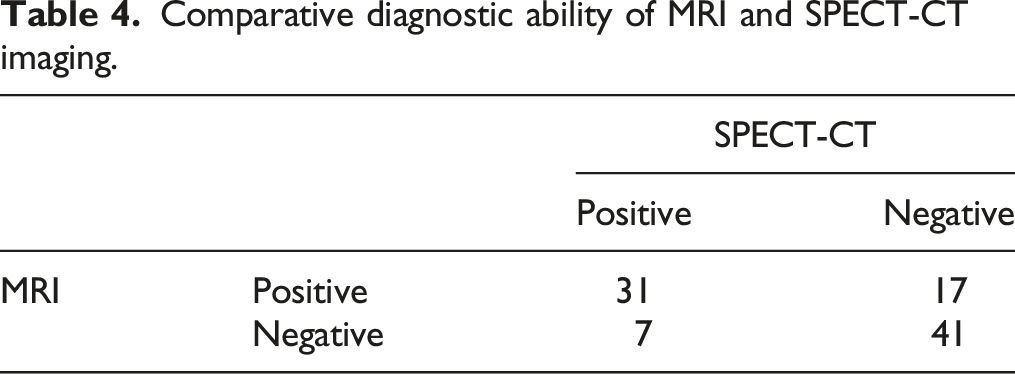
Comparative diagnostic ability of MRI and SPECT-CT imaging.
Discussion
SPECT-CT has the theoretical advantage over MRI of providing functional, as well as structural information. The nuclear medicine component of the scan detects pathological increases in blood flow, resulting in ‘hot spots’ where there is increased uptake of radioisotope tracer. When combined with standard CT, this can lead to improved localisation of focal pathologies such as infection and malignant lesions.5–7
The majority of literature regarding the utilisation of SPECT-CT in imaging the spine has focused on investigating persistent pain following lumbar spine surgery. MRI in this setting is often less useful due to artefact from instrumentation.6,17,21 Several groups have used the focal bone uptake seen in SPECT-CT to successfully diagnose loosening of pedicle screws8,11,14 or failure of fusion.2,12 In our cohort of 104 individuals, SPECT-CT demonstrated increased focal uptake around metalwork in 5 individuals; 2 of these were focussed around pedicle screws, suggestive of loosening. We also found two cases where fusion had not been adequately achieved, leading to one pseudoarthrosis in the congenital deformity group and one partial failure of fusion in the adult group. In all of these individuals, MRI had been inconclusive. Campbell et al 22 made a comparison of SPECT-CT and MRI in investigating juvenile spondylolysis and concluded that MRI was able to detect some abnormality in almost 98% of cases where SPECT-CT had correctly identified a pars defect and so MRI could replace SPECT-CT as a first line investigation in juvenile spondylolysis. When using SPECT/CT to predict positive response to vertebroplasty for osteoporotic vertebral compression fracture, Sola et al 17 found agreement of 80% between MRI and SPECT/CT, suggesting that MRI and SPECT/CT are almost equally matched in terms of detecting pathology in the spine, and similar findings were reported by Li et al. 18 To our knowledge, however, no other studies have directly compared MRI and SPECT-CT at detecting implant loosening and failure of fusion. Al-Riyami et al 13 have recommended routine use of SPECT-CT in assessing individuals with persistent pain post-spinal surgery. Heimberger et al 10 found SPECT-CT to have reasonable sensitivity and specificity for guiding diagnosis in the painful post-operative spine where other imaging modalities were inconclusive. In this setting, we found SPECT-CT to be most useful for detecting facet pathology and metalwork loosening or pseudoarthrosis.
SPECT-CT has also been used to investigate pain in the setting of degenerative spinal disease, and is often noted to successfully identify primary pain generators, and may help avoid unnecessary spinal fusion surgery.15–18 Many groups have also reported SPECT-CT to be advantageous at highlighting alternate pathology that may be a primary pain generator.11–14,23 MRI may become less diagnostically useful in these situations when clouded by widespread degenerative changes, which may be incidental and potentially masking the true cause of symptoms. We found this to be the case in our study, with MRI returning more apparent pathology than SPECT-CT (72% of MRI had some positive finding, compared with 48% of SPECT-CT scans), often of non-specific or degenerative changes, making it difficult to be certain of a diagnosis. The functional element of SPECT-CT theoretically provides a clear advantage here but in our cohort of degenerative pathology, SPECT-CT was not able to identify any clear pathology that was not already evident on MRI.
SPECT-CT was able to identify degenerative changes in the non-instrumented levels in three individuals in the adolescent deformity cohort. Again, this was typically in the facet joints, which were perceived to show the earliest changes secondary to abnormal loading below the instrumented levels (Figure 1). Additionally, degenerative changes were noted in eight of the operated individuals in the adult deformity cohort, six of which were focused around facet joints. In our cohort, SPECT-CT reported nine cases in total of facet joint degeneration which were not evident on initial MRI scan, seven of which were in the setting of previous spinal instrumentation. Lehman et al 24 compared signal change around lumbar facets on MRI and SPECT-CT in individuals with lumbar spine pain and found that, whilst there was some inter-modality agreement, it was not consistent. It is of note however that even with both imaging modalities, there is a false positive and negative rate for the identification of pathology in the spine. MRI and SPECT-CT form part of the diagnostic armamentarium for clinicians, both of which have some utility as part of the holistic investigative options that should form the basis of each individual’s care.
We acknowledge that there are certain limitations to the present study, particularly with respect to the timeframe between imaging modalities; interval between MRI and SPECT-CT ranged from same day to over 5months. We acknowledge that pathology may have progressed in this time, or new pathology emerged which could impact the interpretation of the data presented here. There is also considerable heterogeneity in our cohort, by the nature of the complex case mix referred to our centre, which may affect what can be inferred from the utility of SPECT-CT overall.
It is also worth noting that, in an effort to reduce confirmation bias, we have used only the information from the initial radiology reports of the images for this study, rather than all images being re-reviewed retrospectively by spinal surgeons. The only exception to this being images with no available report which were reviewed by a specialist musculoskeletal radiologist who was not aware of the final diagnosis. All imaging studies were reviewed contemporaneously by the treating surgeon. We acknowledge that this means the surgeon may have identified some pathology on the images that was not mentioned in the report and which could have influenced that patients’ clinical course, which we were unable to control for in this study.
Conclusion
The quality of the MRI images can be compromised by the presence of spinal implants. The situation may be further clouded by varying degrees of degenerative changes at the non-instrumented levels that may or may not be clinically relevant. In such a situation, SPECT-CT may assist in identification and guide treatment of the likely pain generators. From our review, we do not believe that SPECT-CT has any place in the routine primary imaging of the spine. Rather, it may have some use as a second-line imaging modality which provides a ‘metabolic angle’ to the assessment of pain generators when MRI is inconclusive as a static imaging modality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.