
Abstract
Study Design:
Narrative review with commentary.
Objectives:
The growing use of magnetic resonance imaging (MRI) often leaves clinicians faced with scenarios where imaging findings are inconsistent with the clinical picture. This is particularly relevant for degenerative cervical spinal cord compression (CSCC). In this article, we provide a focused narrative literature review to address whether (1) surgery should be offered to asymptomatic patients with CSCC and (2) should MRI spinal cord signal changes influence clinical decisions for a patient with mild myelopathy from CSCC?
Methods:
Illustrative cases are presented with expert commentary which is supplemented by a focused literature review.
Results:
The literature suggests that CSCC from degenerative pathology is a common incidental radiographic finding. For those without symptoms of myelopathy, the short-term risk of progression is low. There is a lack of evidence to support surgery for asymptomatic individuals with CSCC who have no risk factors for progression. For these patients, the authors suggest non-operative management that includes education on the symptoms of myelopathy, clinical follow-up within 6 to 12 months, and avoidance of high-risk activities. Conversely, symptomatic patients have a notable risk of progression. Surgical intervention improves neurological function and quality of life regardless of severity. The authors support surgery as an option for all patients with mild myelopathy who are appropriate operative candidates. Intramedullary signal change on MRI has not been shown to reliably predict progression.
Conclusions:
While MRI technologies are under evolution, we advise that surgical decisions for patients with CSCC should rely on clinical assessment and not imaging findings.
Keywords
Introduction
With the growing use of cross-sectional radiography such as magnetic resonance (MR) imaging and computed tomography imaging, spinal surgeons are increasingly faced with scenarios in which radiographic findings are inconsistent with a patient’s clinical picture. The most appropriate course of management in these scenarios is often perplexing and this is of particular relevance in the context of degenerative cervical spinal stenosis. Herein, patients often have imaging that demonstrates degenerative cervical spinal cord compression (CSCC). However, in many instances the patient is either asymptomatic or has only mild symptoms of myelopathy. The indications for treatment remain controversial and the surgeon is left with many factors to consider.
Through 2 illustrative cases and a focused narrative review of the recent literature, we provide an expert commentary to address 2 common questions: (1) should surgery be offered to asymptomatic patients with degenerative CSCC and (2) should intramedullary spinal cord signal change on conventional MR imaging influence surgical decision making for a patient with mild myelopathy? This commentary reflects the authors’ approach to management of these 2 challenging yet common scenarios and represents expert opinion on an area of clinical practice where high-quality evidence is lacking. We intend this to serve as a concise review of the current evidence surrounding these 2 challenging scenarios that will facilitate decision making.
Asymptomatic Cervical Spinal Cord Compression
Radiographic evidence of degenerative pathology of the cervical spinal column is common and becomes increasingly prevalent with age. 1,2 Changes include disc degeneration, vertebral body remodeling, spondylolisthesis, enlargement of intraspinal ligamentous tissue, and increased bulging of the ligamentum flavum partially due to increased laxity of the fibrous tissue. 2,3 These degenerative changes are often associated with cervical spinal canal stenosis, which, depending on the degree of degeneration, may lead to compression of the spinal cord. However, these patients may present without clinical evidence of neurological impairment. This section will focus on the role of surgical intervention for those with asymptomatic CSCC.
Prevalence
A number of studies have shown that the prevalence of CSCC increases with age. Matsumoto et al conducted an MR imaging-based cross-sectional population study of 497 asymptomatic volunteers and found that 7.6% of subjects (mostly over 50 years of age) had evidence of spinal cord compression from degenerative changes. 1 Another study of 1211 asymptomatic volunteers, with a similar methodological design, found evidence of spinal cord compression in 5.3%. 4 A smaller cross-sectional MR imaging-based series of 30 asymptomatic volunteers demonstrated a 13% prevalence of radiographic CSCC from degenerative pathology. 5 Lee et al conducted a postmortem assessment of the cervical spinal canal diameter of 469 adult cadaveric specimens. 6 They used a spinal canal anteroposterior diameter of <12 mm as their criterion and found that the overall prevalence of cervical spinal canal stenosis was 4.9% of the adult population with an age-related association. 6 The prevalence was observed to be 6.8% for those between the ages of 50 and 69 and 9% for those 70 years of age or older. 6 It is therefore clear that imaging assessment of patients with advanced age will demonstrate evidence of stenosis with increasing probability, though many will be asymptomatic.
Natural History of Asymptomatic Cervical Cord Compression
Some of the best evidence pertaining to the natural history of asymptomatic CSCC without symptoms of myelopathy may be found in a prospective observational cohort study published by Bednarik et al in 2008. 7 A cohort of 199 patients with CSCC from discogenic or osteoligamentous spondylotic changes were prospectively assessed at 6-month intervals for 2 years and then yearly thereafter. 7 Each subject had a baseline clinical neurological assessment along with MR imaging and electrophysiological testing. Over an average follow-up period of 44 months, 22.6% of subjects began to show clinical evidence of myelopathy, with 8% of subjects developing symptoms within 1 year. Risk factors for the development of myelopathy included prolonged somatosensory-evoked potentials and motor-evoked potentials, MR imaging with intramedullary T2-weighted imaging (T2WI) signal changes, and clinically symptomatic radiculopathy. 7
Natural history data pertaining specifically to asymptomatic patients with cervical spinal stenosis secondary to OPLL (ossification of the posterior longitudinal ligament) has been reported by Fujiyoshi et al based on the data from a small prospective study of 27 patients with a spinal canal that measured <12 mm on MR imaging. 8 They reported that no subject developed myelopathy, defined by a comparison of their baseline and follow-up Japanese Orthopaedic Association (JOA) scores over a mean follow-up period of 59 months (range 12-95 months). Further evidence is contributed by Matsunaga et al, who conducted a multicenter retrospective cohort study of 156 patients with a minimum 5-year follow-up. 9 They dichotomized risk for myelopathy development into groups with <60% stenosis and those with ≥60% cervical spinal stenosis. Myelopathy developed in 61.5% of subjects (96/156) and was observed in 100% of subjects (39/39) with ≥60% cervical spinal canal stenosis. A subgroup analysis of the cohort with <60% stenosis suggested that a larger cervical range of motion (total angle of C2-C7 angles at maximum anterior and posterior position) and lateral-deviated type OPLL are associated with a greater likelihood of developing myelopathy. However, these findings should be interpreted with caution. The authors did not provide a definition for myelopathy and did not appear to have used a quantifiable assessment metric. Moreover, time to event data was not used and risk ratios were not compared between groups.
Overall the literature suggests that the risk of development of myelopathy for patients with asymptomatic degenerative CSCC is low over the short term; however, those with abnormal electrophysiological studies, T2WI hyperintensity, or symptoms of radiculopathy may be at an elevated risk for progression. Higher quality data is needed to further assess the risk of progression to myelopathy in patients with asymptomatic OPLL. 10
Risk of Traumatic Injury
It is not uncommon for asymptomatic patients with radiographic cervical spinal stenosis to receive a recommendation for surgical intervention to mitigate a perceived elevation in the risk of neurological injury resulting from a traumatic event. 11 However, the present literature aimed to address this concern is controversial.
Bednařík et al reviewed their prospective cohort of 199 patients to specifically assess whether trauma is a risk factor for the development of neurological impairment. 12 They identified 14 traumatic episodes over the mean follow-up period of 44 months and reported one case where myelopathy manifested after the trauma. They concluded that the risk of spinal cord injury is probably low in individuals with asymptomatic cervical compression, especially if a restriction in risky activities is implemented. This finding was corroborated by Chang et al, who found that in a cohort of 55 prospectively followed asymptomatic, or mildly symptomatic, patients with CSCC, 18% experienced a traumatic event but none of these had evidence of a spinal cord injury. 11
In another study, Ruegg et al utilized a retrospective case-control methodology to address the question. 13 A consecutive cohort of 52 patients presenting to a single center with traumatic quadriplegia or quadraparesis from a minor event over a 10-year period were compared with controls who had retained a similar minor injury but with no associated neurological compromise. They found that the cord-canal-area ratio (>0.8) or the space available for the cord (<1.2 mm) measured on MR imaging can be used to reliably identify patients at risk for acute spinal cord injury after a minor trauma. 13 However, caution should be taken before applying these finding to all individuals with asymptomatic CSCC. The authors suggest that they excluded those with preexisting neurological symptoms; however, no specific details are provided. Given the retrospective nature of this study, it is possible that some patients with neurological injury after the trauma may have had preceding symptoms of myelopathy that were not identified. Of note, falls were the inciting mechanism in nearly twice the proportion of cases with neurological injury compared with controls (48% cases vs 27% controls), which may suggest preexisting yet unidentified symptoms of myelopathy. It has also been suggested that a Torg-Pavlov ratio (Figure 2) of ≤0.82 is a risk factor for spinal cord injury and neurapraxia in athletes. 14,15 Unfortunately, the degenerative changes in the vertebral column over time result in changes to this ratio, and therefore this cutoff may not be applicable for use in elderly patients, and furthermore was developed in the pre-MR imaging era and has fallen out of favor when compared with other MR imaging-based measures such as maximum spinal cord compression (Figure 2B) on midsagittal MR sections. 16,17
Fengbin et al specifically looked at whether this risk of trauma-induced spinal cord injury would be influenced by the presence of dynamic instability on lateral flexion-extension radiographs as measured by the White-Panjabi standard. According to their retrospective study of 72 patients with cervical stenosis who suffered low-energy trauma, patients with dynamic instability on X-ray were more likely to experience new or aggravated myelopathy posttrauma (81.3% vs 53.6%, P < .05). 18 Again this finding should be interpreted with caution because the authors did not report the subjects’ baseline neurological status pretrauma.
Overall these studies are helpful, but contradictory findings and low-quality evidence pertaining to the risk to the asymptomatic patient population makes it difficult to draw any definitive conclusions. Moreover, there have been no prospective, controlled studies to lend further insight into the role that surgery has on mitigating the risk of neurological injury from a low-energy trauma mechanism in those with asymptomatic CSCC.
Recommended Treatment
Clinical suspicion for myelopathy should precede MR imaging examination; thus, the underlying reason for obtaining images should be sought out and considered. While the significance of CSCC should not be discounted, if the MR imaging was performed for an indication other than neurological dysfunction, then a careful history and physical examination should be performed to determine if the imaging findings do in fact correlate with any clinical manifestations. In instances where an asymptomatic patient is found to have CSCC, such as the scenario summarized in Box 1, we do not recommend surgical intervention. The natural history data suggests a low probability of short-term progression and surgery does present a risk for adverse events. We hold the same recommendation for patients with asymptomatic CSCC compression specifically related to OPLL, where there is a lack of high-quality evidence to suggest a benefit from surgical therapy.
Illustrative Case 1.
A 56-year-old women presents for a surgical consultation because of a finding of degenerative CSCC on MR imaging performed as part of a series of investigations for intermittent axial neck pain of 1-year duration. MR imaging reveals spinal stenosis with CSCC at C5/6 and C6/7 (Figure 1). Comprehensive history and neurological examination revealed no evidence of upper motor neuron dysfunction such as unsteady gait, clumsy hands, or brisk reflexes. The patient wishes to know what is the risk of her developing symptoms and if she should have surgery to mitigate this risk.

T2-weighted magnetic resonance images. (A) Midsagittal, (B) Axial through the C3/4 intervertebral disc space; (C) Axial through the C4/5 intervertebral disc space; (D) Axial through the C5/6 intervertebral disc space. The axial images at C4/5 and C5/6 demonstrate spinal canal stenosis with cervical spinal cord compression.
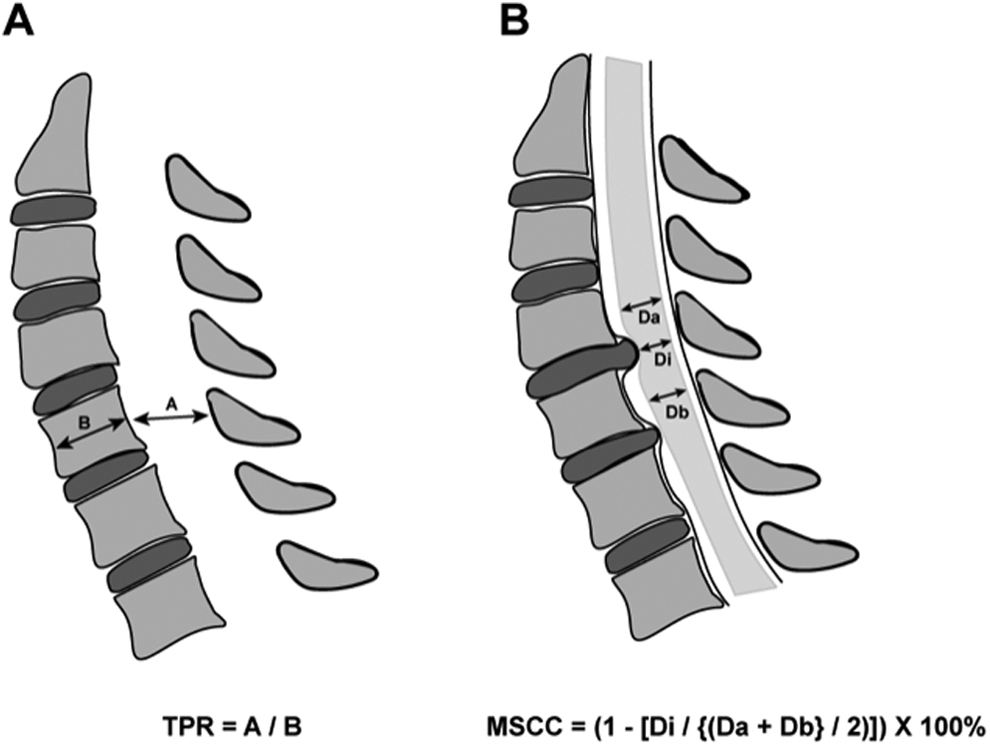
(A) Torg-Pavlov ratio (TPR). 14 Determined using sagittal X-ray plain film. A ratio of the distance from the posterior aspect of the vertebral body to the nearest point on the spinal laminar line (A) and the distance from the anterior aspect to the posterior aspect of the vertebral body (B). The normal A/B ratio is approximately 1.00. (B) Maximum spinal cord compression (MSCC). 16,17 Determined using midsagittal T2-weighted magnetic resonance imaging. Di is the anteroposterior spinal cord diameter at the level of MSCC, Da is the anteroposterior spinal canal diameter at the first normal vertebral segment above, and Db is the same measurement at the first normal vertebral segment below the level of injury. The measurements for Da and Db should be taken at the mid-vertebral body level.
Asymptomatic patients with CSCC who are managed conservatively should be educated on the symptoms associated with myelopathy so that they can seek clinical evaluation on the development of any early symptoms of myelopathy. We also suggest that these patients are seen again in the clinical setting within 6 months to 1 year of initial evaluation for a clinical reassessment, and we counsel them to avoid high-risk activities such as downhill skiing or snowboarding, mountain biking, or contact sports. We do not believe there is a role for serial MR imaging or for serial electrophysiological testing in patients with quiescent pathology, as there is no data in the literature to support this resource expenditure. However, we believe that the onset of myelopathy symptoms should prompt repeat imaging and consideration of surgical intervention.
We do present surgery as an option for one subgroup of asymptomatic patients with CSCC; those who present with risk factors for the development of myelopathy (abnormalities on electrophysiological testing, symptoms of cervical radiculopathy, or T2WI hyperintensity of the spinal cord). 7 As mentioned, we do not routinely obtain electrophysiological testing on patients with asymptomatic CSCC; however, we do take this finding into consideration in those who do present with these investigations (largely performed in the context of symptomatic cervical radiculopathy). If a patient in this subgroup opts for conservative management, we initiate a more frequent clinical follow-up regime and believe they should be seen in clinic within at least 6 months of their initial presentation for reassessment.
Cervical Spinal Cord Compression With Minimal Symptoms of Myelopathy
The role of surgery is controversial for patients with CSCC and minimal symptoms of myelopathy. To assist with clinical decision making, some have advocated for the use of conventional MR imaging to assess for intramedullary spinal cord signal change. This may be either T2WI hyperintensity (Figure 3A) or T1-weighted imaging (T1WI) hypointensity (Figure 3B). Intramedullary signal changes relate to water content, and it is believed that increased water content is associated with increased severity of injury. 2 However, the role of MR imaging in surgical decision making for patients with degenerative cervical myelopathy (DCM) who have minimal neurological symptoms is controversial and will be the focus of this section.
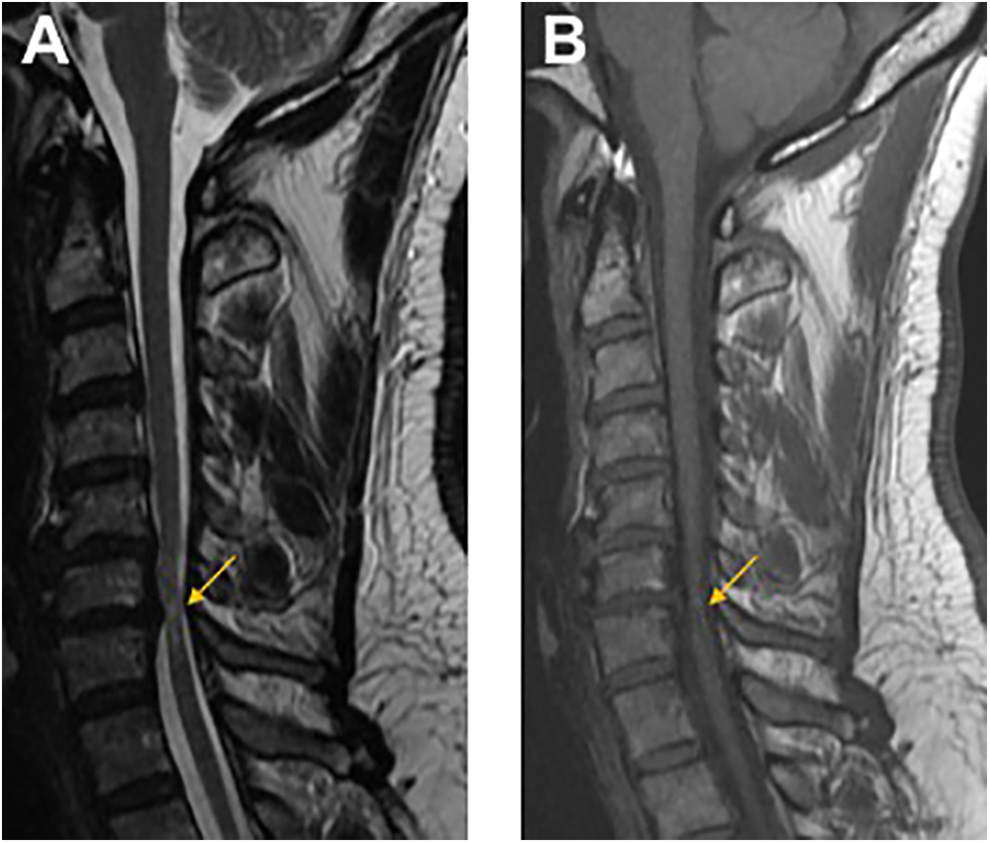
Midsagittal magnetic resonance images of a C6/7 intervertebral disc herniation with cervical spinal cord compression. (A) T2-weighted image demonstrating signal hyperintensity; (B) T1-weighted image demonstrating signal hypointensity.
Natural History of Symptomatic Cervical Spine Cord Compression and Surgical Outcomes
On manifestation of the signs and symptoms of cervical myelopathy, the risk of progression becomes substantial. A recent systematic review of the literature suggests that the risk of neurological worsening falls in the range of 20% to 60% of patients over a period of 3 to 6 years. 19 Furthermore, 2 prospective, multicenter, international cohort studies have shown significant improvements in neurological function, quality of life, and disability after surgical decompression for patients with mild to severe DCM, with relatively low rates of postoperative complications. 20,21 The primary results of the safety and efficacy of these 2 AOSpine studies have, in part, resulted in a paradigm shift in the way surgical intervention is viewed. 20,21 Previously, surgery was thought of as a means to halt neurological deterioration. Now surgery is regarded as a means to improve neurological function and quality of life, and it is now strongly recommended for those with moderate to severe impairment. 22
Evidence specifically in support of surgery for patients with mild symptoms has been recently provided by a multivariate clinical prediction model derived from the combined data set of the CSM North America and International trials. Herein, Tetreault et al used multivariate Poisson regression modeling and found that milder symptoms of myelopathy, shorter symptom duration, and an absence of impaired gait function independently predicted a significantly greater likelihood of achieving a good modified JOA (mJOA) score (≥16) at 1-year follow-up. 23 However, elements of equipoise still remain in the management of those with mild impairment. In response, a number of investigators have studied if intramedullary signal change on conventional MR imaging sequences could help define a subgroup of patients that would benefit from surgery in this scenario.
Prevalence and Prognostic Value of Spinal Cord Signal Change
Intramedullary signal changes of the spinal cord are frequently observed in the setting of degenerative CSCC, and the prevalence of T2WI hyperintensity has been reported to range from 58 to 85% in those with symptoms of myelopathy. 2 The likelihood of myelopathy being present on clinical examination significantly increases with the presence of T2WI cord signal hyperintensity, and there appears to be a stepwise increase in neurological impairment as well as an increased prevalence of signs when comparing patients with no signal change, T2 hyperintensity, and both T2 hyperintensity and T1 hypointensity. 24,25 In addition, the number of signs and symptoms and impairment are more prevalent in patients with a greater number of T2 hyperintensity levels. 24,25 Similarly, a significant association between a T2WI hyperintensity at the level of maximal spinal cord compression and a lower mJOA has been found. 26 However, similar hyperintensity may also be an incidental finding. It was observed that 2.3% of 1211 asymptomatic volunteers had evidence of compressive cervical spinal pathology with an associated T2WI hyperintensity. 4 It has also been recently shown that males present with significantly greater MR imaging evidence of degenerative cervical changes and a higher prevalence of T2WI hyperintensity than woman despite comparable baseline neurological impairment. 27 It is unclear why this is the case, but these findings do contribute to the challenge in matching MR imaging appearance with the clinical presentation.
A few studies have looked at the predictive value of intramedullary signal changes on MR imaging in the context of conservative management of CSCC. Shimomura et al found that T2WI hyperintensity was not predictive of clinical progression as measured by a deterioration in JOA score in patients with mild myelopathy. 28 Yoshimatsu et al looked for factors that predicted failure of conservative treatment in a similar cohort of patients with early myelopathy and found that the presence of T2WI hyperintensity failed to reliably predict functional deterioration. 29
There have been several reports that have sought to assess the utility of intramedullary signal changes on MR imaging to predict surgical outcome. A number of reviews have been undertaken to unify the evidence. 30 –32 Collectively, these have not been able to collate consistent or strong evidence to support the prognostic value of signal changes. There is weak evidence to suggest that T2WI hyperintensity may portend a worse outcome, particularly when present at multiple sites, when the signal intensity is substantially different than the normal segments of the spinal cord, or when the T2WI hyperintensity is accompanied by a corresponding T1WI hypointensity. 30 –32 The nonspecific nature of T2WI hyperintensity, which represents a number of pathophysiological correlations, accompanied by the high prevalence of these changes among patients with DCM, makes this a challenging criterion from which to differentiate outcome. In fact, the recent combined analysis of the AOSpine North America and International studies have provided the strongest evidence to date that there is no significant difference in surgical outcomes between subjects who had no signal change identified with conventional MR imaging and those with T2WI hyperintensity. 25 However, some stronger evidence specific to T1WI has been gained from the AOSpine studies, which supports that T1WI hypointensity may be a negative prognosticator for surgical outcome, but because it is present in about only 20% of patients it is of lesser clinical utility. 25,33 Overall, intramedullary signal changes observed on conventional MR imaging sequences may provide some additional information pertaining to surgical outcomes, but the evidence that is presently available does not support its routine use for surgical decision making.
Emerging imaging sequences, which have now reached the stage of clinical study, do hold promise to serve as eventual adjuncts to the clinical decision-making process. These include the use of diffusion tensor imaging (DTI), T2*WI and functional MR imaging. 34 –36 In a meta-analysis of 14 studies involving 479 patients with DCM, Guan et al concluded that DTI indices at stenotic levels are more sensitive markers of clinical myelopathy than conventional MR signal change, especially in the early stages of the disease. 37 That said, its prognostic value as it relates to progression of the symptoms of myelopathy and prediction of postoperative outcomes remains to be elucidated, limiting its clinical utility at this time. Although some small cohort studies suggest that higher fractional anisotropy coefficients predict better postoperative outcomes, these results remain to be validated in larger controlled studies. 38,39
Recommended Treatment
Considering the beneficial effects of surgery on function, quality of life, and disability, we recommend surgical decompression for all symptomatic forms of DCM and for patients who have signs of myelopathy based on comprehensive neurological examination. We would suggest surgical intervention as an option for the patient (as summarized in Box 2). There is no high-quality data to support the use of intramedullary signal change on conventional MR imaging in the surgical decision-making process for patients with DCM, and as such we provide surgery as an option for patients with symptoms of myelopathy regardless of severity as long as they are fit to undergo surgical intervention.
Illustrative Case 2.
A 62-year-old male presents with a 6-month history of progressive worsening in his ability to use his hands for fine motor skilled activities such as retrieving his house keys from his pocket or buttoning his shirt. Comprehensive neurological examination reveals the presence of a Hoffman sign in both upper extremities along with brisk patellar and Achilles deep tendon reflexes. All other aspects of the neurological examination are normal. The MR imaging (Figure 4) demonstrates spondylotic changes at C4/5 and C5/6 with resultant CSCC. The patient wishes to know if he should have surgery to improve his symptoms.
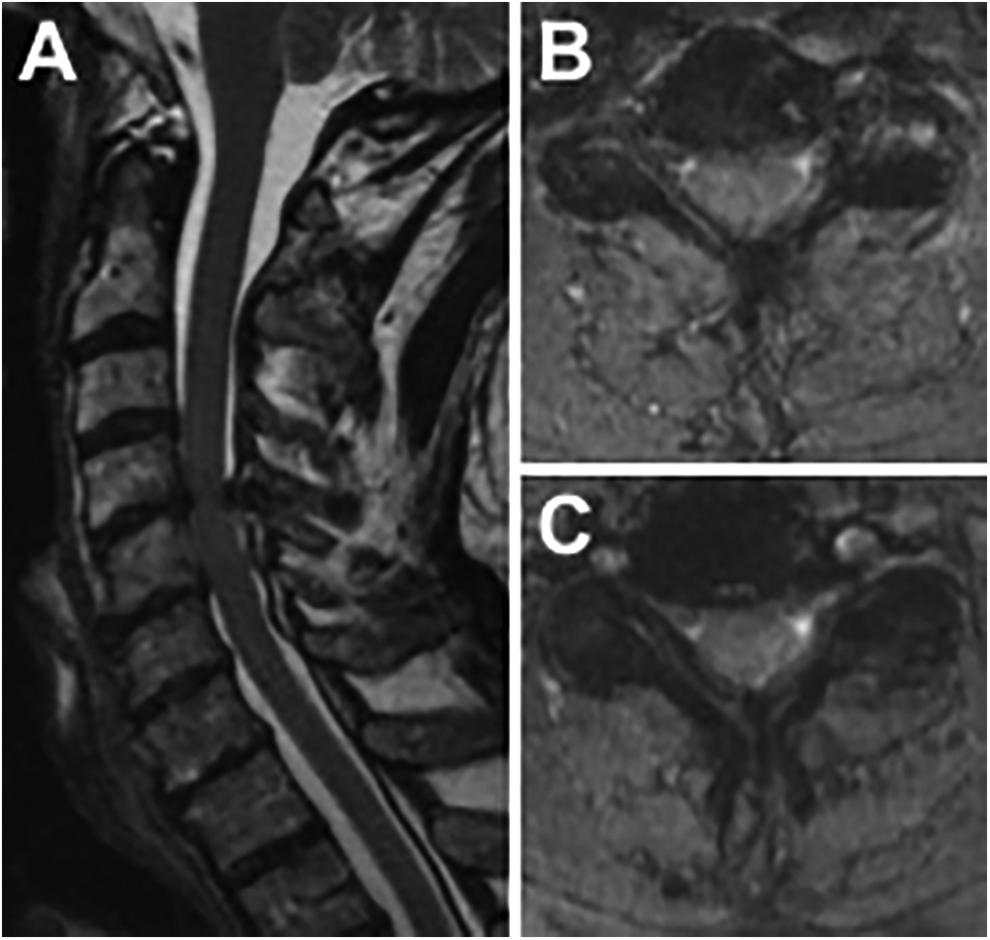
T2-weighted magnetic resonance images. (A) Midsagittal; (B) Axial through the C4/5 intervertebral disc space; (C) Axial through the C5/6 intervertebral disc space. The axial images at C4/5 and C5/6 demonstrate spinal canal stenosis with cervical spinal cord compression from spondylotic changes at these 2 levels.
Intramedullary signal changes may help predict outcome and may help in the management of patient expectations for neurological recovery. Preliminary evidence suggests that the absence of T2WI hyperintensity predicts better recovery after surgery, whereas the presence of T1W1 hypointensity may be associated with a lower likelihood of obtaining an optimal surgical outcome. Further research is required to reliably incorporate these conventional MR imaging features in surgical decision making.
Conclusions
As population demographics shift and the utilization of cross-sectional diagnostic imaging increases, it is likely that spinal surgeons will increasingly face scenarios of clinico-radiographic discordance when managing degenerative CSCC. Multiple promising inroads are being made to improve the predictive ability of MR imaging for cervical spinal cord dysfunction. However, at present we advocate that the decision to operate on a patient with degenerative CSCC should be anchored in the clinical history and examination.
It is our opinion that asymptomatic patients can be managed conservatively after a detailed discussion of the symptoms of myelopathy, counselling to avoid high-risk activities and advice to return for assessment if any symptoms of myelopathy should occur. However, those asymptomatic individuals who have one or more of the recognized risk factors for the onset of myelopathy (abnormalities on electrophysiological testing, symptoms of cervical radiculopathy, or T2WI hyperintensity of the spinal cord) 7 should be presented the option of surgical intervention. This is in keeping with recently published clinical practice guidelines. 40 We believe that those with symptoms and/or signs of myelopathy should be considered for surgical intervention regardless of the presence or absence of MR imaging signal changes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MGF is supported by the Halbert Chair in Neural Repair and Regeneration and the DeZwirek Foundation.