
Abstract
Study Design
Retrospective comparative study.
Objectives
This study compares supine vs bending flexibility radiographs and evaluates their ability to predict residual postoperative lumbar curvature after selective thoracic fusion for Lenke 1 and 2 curves across different lumbar modifiers (A, B, and C) in adolescent idiopathic scoliosis (AIS).
Methods
This was a retrospective review of AIS Lenke 1 and 2 patients who underwent posterior fusion. All patients had preoperative flexibility radiographs including side-bending and supine posteroanterior (PA) films, in addition to pre- and post-operative standing PA and lateral radiographs. We used SurgiMap 2.0 software for all radiographic measurements. Pearson correlations and linear regression models were developed in SAS.
Results
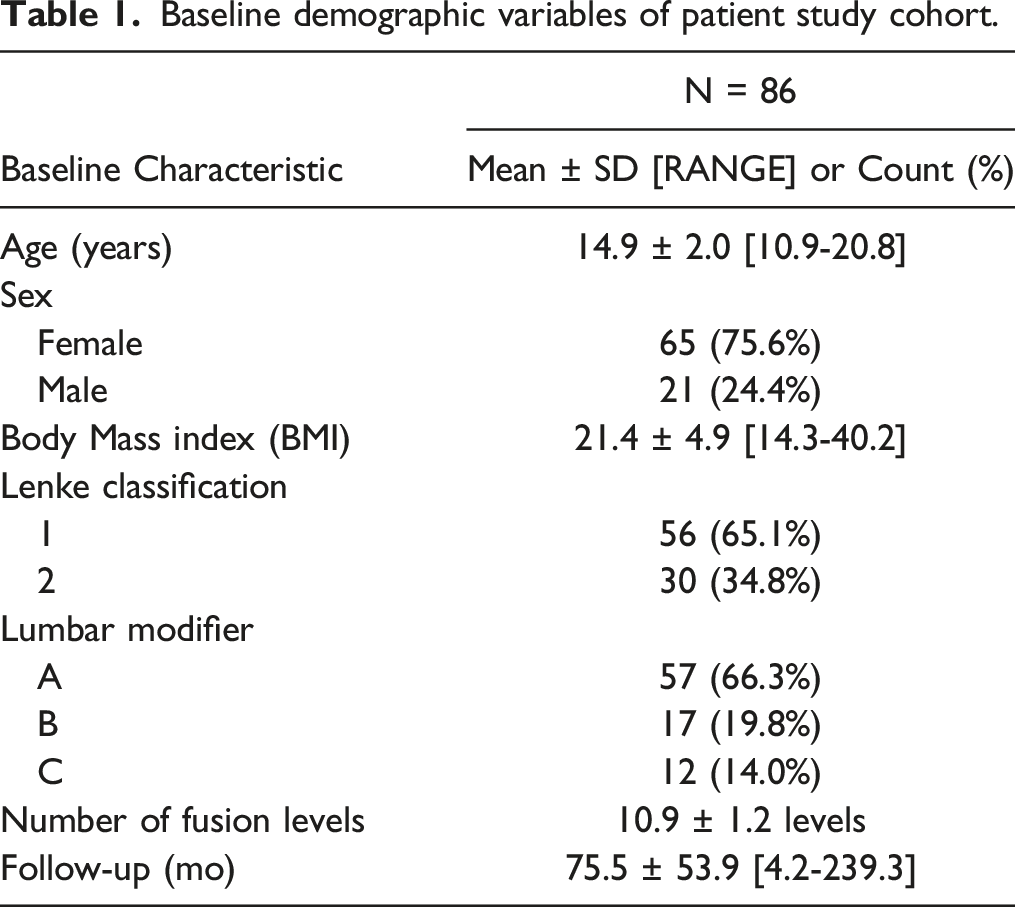
A total of 86 patients were included mean age 14.9 years and follow-up 72.3 months
Conclusion
Either supine or side-bending radiographs alone may be used to estimate mean residual postoperative lumbar curvature after selective posterior thoracic fusion, but little is to be gained by taking both supine and side-bending radiographs.
Introduction
Juvenile and adolescent idiopathic scoliosis is primarily treated with posterior instrumented spinal fusion to halt curvature progression and optimize spinal balance in large magnitude curves. Main thoracic curves typically generate compensatory curves in the lumbar and proximal thoracic spines to maintain coronal balance. Per the Lenke classification, these compensatory lumbar curves are either deemed structural and are typically included in the fusion construct, or non-structural and left unfused (“selective thoracic fusion”). In selective thoracic fusions, some residual curvature is usually observed in the lumbar spine. In order to determine the structural nature of compensatory curves-and therefore the appropriate Lenke classification and levels of instrumented fusion-preoperative flexibility radiographs can be used. 1
A variety of radiographs have historically been utilized to assess flexibility, including side-bending, push-prone, traction, or a supine anteroposterior (AP) spine radiograph. The side-bending view-often referenced to be the gold standard-uses a forced lateral bend from the patient’s hips in both left and right directions to study and measure coronal curve correction. 2 The push-prone view requires a manual three-point correction of the major coronal curve at the time of imaging. It has shown similarity to side-bending in assessing curve flexibility with small advantages in evaluating the residual curve above and below an instrumented fusion. 3 The traction view requires manually pulling on the patient’s head/neck with countertraction provided by an assistant by grabbing the lower extremities. Given the particular level of discomfort and difficulty with this method, it is typically performed under general anesthesia and has demonstrated some usefulness in assessing flexibility in larger curves >65°.4 Although variably utilized, the supine AP radiograph eliminates gravity and allows nonstructural components of spinal curvature to relax to baseline for evaluation. 2
Our institution regularly obtains both supine AP and side-bending radiographs preoperatively for assessment of curvature flexibility. While it is well established in prior reports that the supine AP radiograph can detect spinal flexibility,2,5-9 it is unknown whether pre-operative supine radiographs can reliably predict the postoperative residual Cobb angle in the unfused lumbar curve in selective thoracic fusions. This study compares supine vs bending flexibility radiographs and evaluates the ability to predict residual postoperative lumbar curvature after selective thoracic fusion for Lenke 1 and 2 curves across the different lumbar modifiers (A, B, and C).
Materials and Methods
This was a retrospective cohort of patients aged 10 to 21 with juvenile or adolescent idiopathic scoliosis with Lenke 1 or 2 classification who underwent posterior-only instrumented selective thoracic spinal fusion from January 2012 through December 2019 by a single fellowship-trained pediatric orthopaedic surgeon. Patients were identified via electronic medical record search of current procedural terminology (CPT) codes. We excluded any patients with concomitant anterior spinal surgery, history of prior spinal surgery (eg, growing rods), pre-operative halo gravity traction, three-column osteotomies, and non-idiopathic scoliosis diagnoses. We also excluded any patient who required revision surgery or did not have a full series of pre-operative standing posteroanterior (PA), lateral, side-bending, and supine AP radiographs and post-operative standing PA and lateral radiographs. Altogether, we excluded a total of 4 patients per the above exclusion criteria following our initial query. Side-bending films were performed in the supine position. Institutional Review Board approval was obtained and exempted from individual informed consent processes for this retrospective study (No. 1578049-4).
We reviewed electronic medical records to extract clinical variables, and radiographs were reviewed for Lenke classification and coronal curve magnitude (Cobb angle). Lenke modifiers were dichotomized into two groups, “A” and “B or C”, as Lenke B and C curves were noted to behave similarly from a statistical perspective. Flexibility indices were calculated for both side-bending and supine films [(1-flexibility Cobb/standing Cobb)*100], as were correction indices [(1−post Cobb/preop Cobb)*100]. All radiographic measurements were conducted by two co-investigators using computer assistance SurgiMap 2.0 software (Nemaris, Inc, Methuen, Massachusetts, USA).
Spearman correlations were performed using SAS v. 9.4 and JMP Pro v. 16 (SAS Institute Inc, Cary, NC, USA) to analyze correlation between pre-operative standing, supine, and side-bending lumbar curve measurements and flexibility indices, with post-operative lumbar Cobb angles and lumbar correction index. Regression models were built to predict postoperative lumbar Cobb angles from preoperative variables, including the dichotomized Lenke modifier (“A” and “B or C”). Regression models were also constructed to relate supine and side-bending preoperative lumbar flexibility indices, along with Lenke modifier, to lumbar correction index. Significance was established at P < .05. With regards to power analyses, the P-values for the regression models and the Spearman’s correlations (except one) were all ≤ .001, which led to rejecting the null hypothesis of no linear relationship. When the null hypothesis is rejected, it is impossible to make a Type 2 error. With regards to the one Spearman correlation study, the power for detecting a correlation of at least .30 with n = 86 at the 5% level of significance is .80 which was deemed adequate.
Results
Baseline demographic variables of patient study cohort.
Preoperative curve characteristics of patient study cohort.

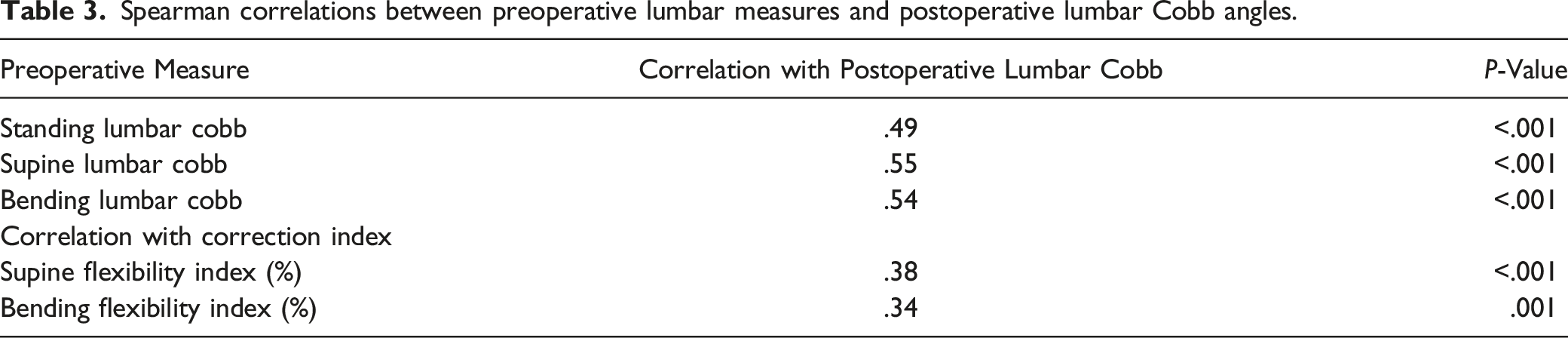
Spearman correlations between preoperative lumbar measures and postoperative lumbar Cobb angles.
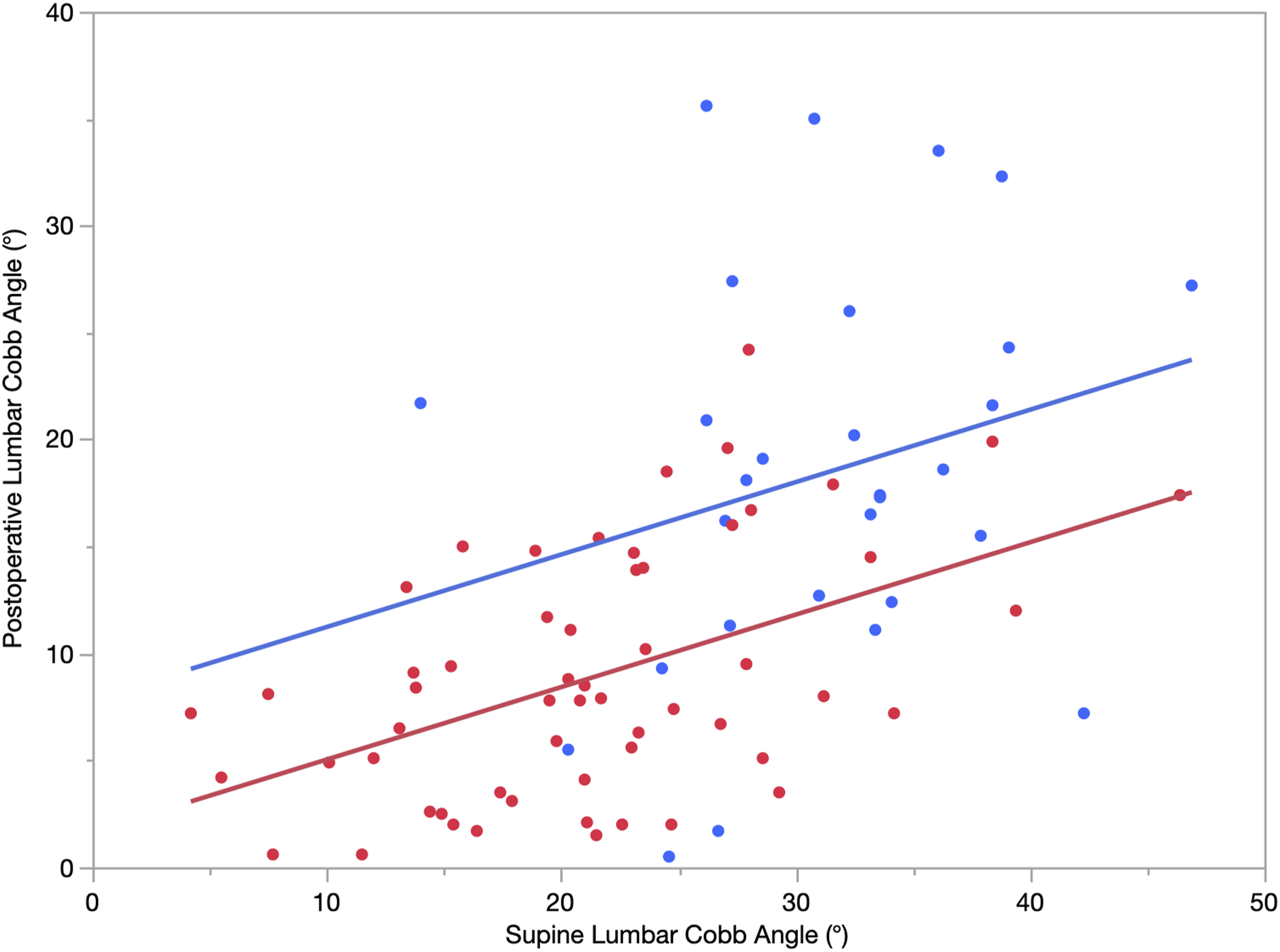
Three regression models were built to predict postoperative lumbar Cobb angles from preoperative information (Table 4). All three models included the Lenke modifier (“A”, “B or C”). The first model (Model S, R2 = .39) uses the preoperative supine lumbar curve as the explanatory variable (Figure 1): Predicted Y = 7.85 – 6.20 X1 + .34 X2 Y = postoperative lumbar Cobb X1 = Lenke modifier (1 = A, 0 = B or C) X2 = supine lumbar Cobb Comparison of regression models of the relationship between preoperative radiographs and postoperative lumbar Cobb angles. The joint model contains both supine and bending radiographs. Smaller values of model standard deviation and median absolute error indicate a better model, however larger values of R2 indicate a better model with more explained data variation. Scatterplot of postoperative Lumbar Cobb angle vs preoperative supine lumbar Cobb angle with the regression Model S overlaid. (Red is Lenke A; Blue is Lenke B or C). 39% of the variation from patient-to-patient in postoperative lumbar Cobb angles can be explained by this regression model (R2 = .39, P < .001).

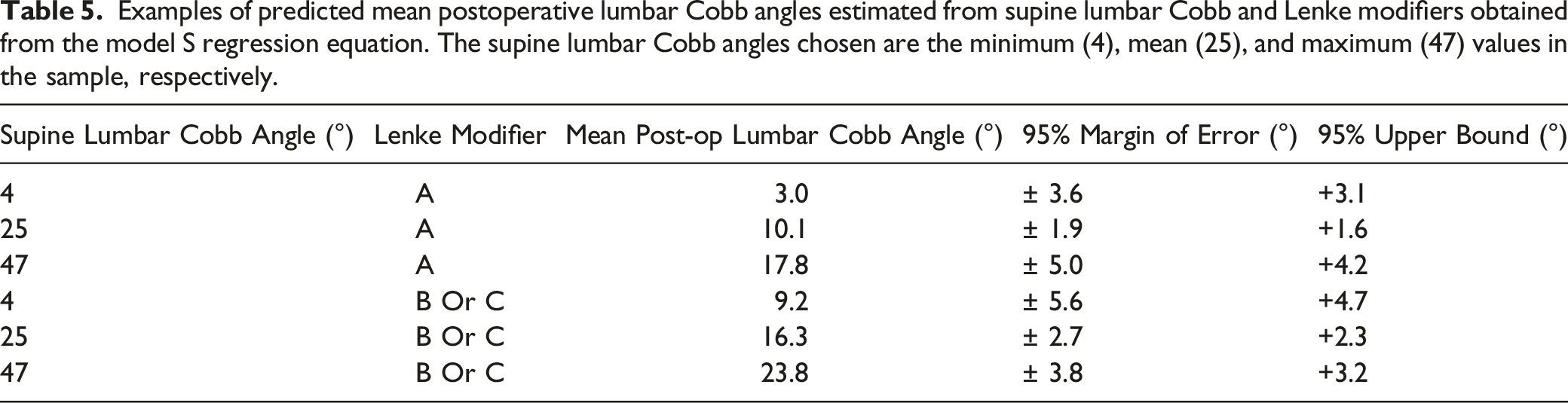
Examples of predicted mean postoperative lumbar Cobb angles estimated from supine lumbar Cobb and Lenke modifiers obtained from the model S regression equation. The supine lumbar Cobb angles chosen are the minimum (4), mean (25), and maximum (47) values in the sample, respectively.
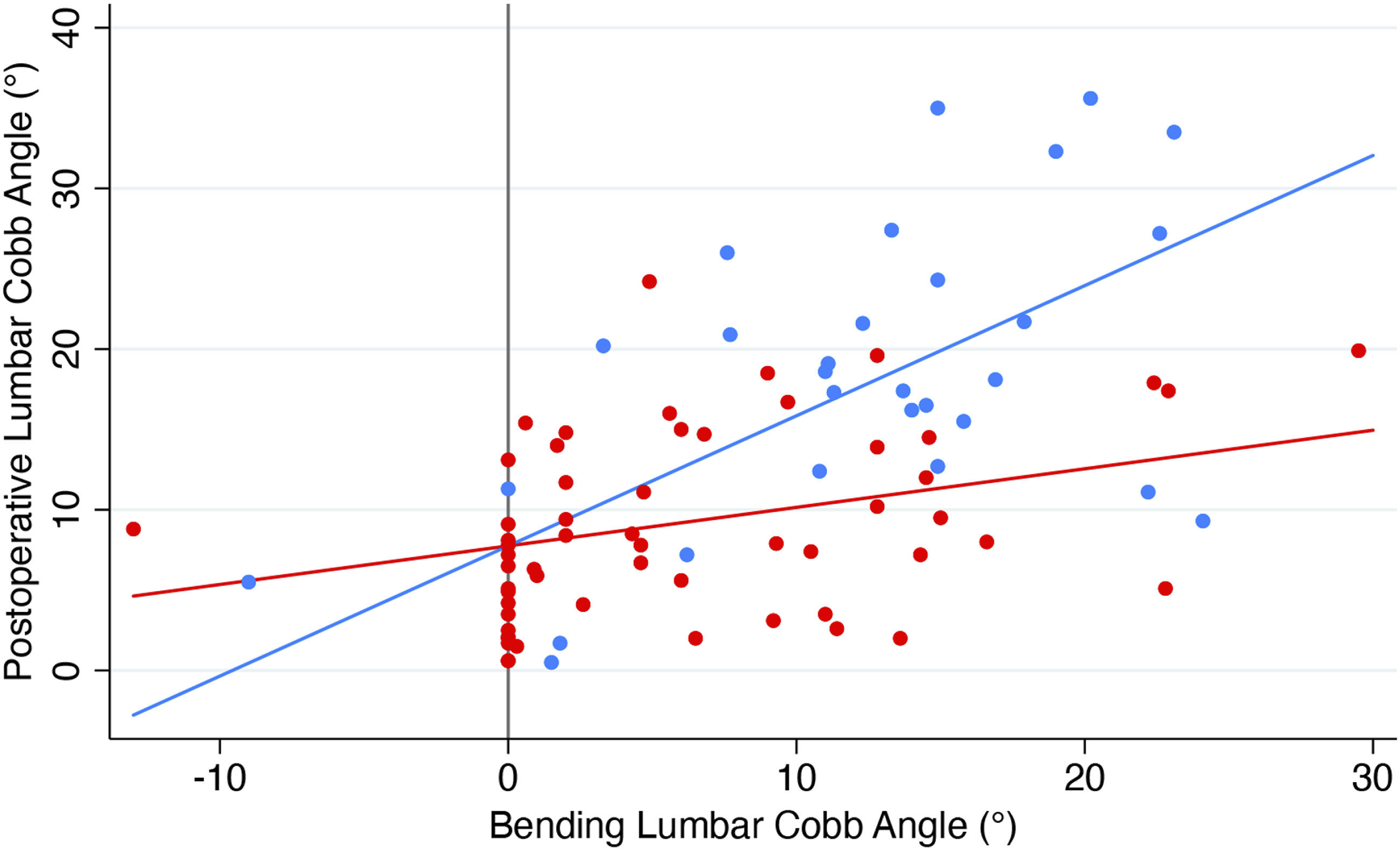
The second model (Model B, R2 = .44) uses the preoperative side-bending lumbar curve as the explanatory variable (Figure 2): Predicted Y = 7.75 + .81X1 - .57 X2 Y = postoperative lumbar Cobb X1 = preoperative bending lumbar Cobb angle X2 = preoperative bending lumbar Cobb angle x Lenke modifier (1 = A, 0 = B or C) Scatterplot of postoperative Lumbar Cobb angle vs preoperative bending lumbar Cobb angle with the regression Model B overlaid. (Red is Lenke A; Blue is Lenke B or C). The larger the preoperative Cobb angle, the larger the difference between the Lenke modifier groups postoperatively. 44% of the variation from patient-to-patient in postoperative lumbar Cobb angles can be explained by this regression model (R2 = .44, P < .001).
The third model (Model SB, R2 = .49) is a joint model that uses both supine and bending lumbar Cobb angles: Predicted Y = 3.05 + .25X1 + .61 X2 – .53 X3 Y = postoperative lumbar Cobb X1 = preoperative supine lumbar Cobb angle X2 = preoperative bending lumbar Cobb angle X2 = preoperative bending lumbar Cobb angle x Lenke modifier (1 = A, 0 = B or C)
The joint model SB was found to have the highest explained variation (R2 = .49). Model B performed slightly better than model S and performs nearly as well as model SB with similar margins of error.
Discussion
The role of side-bending radiographs to evaluate curve flexibility and structurality in adolescent idiopathic scoliosis has been well-established in literature and practice. 1 The supine radiograph has been proposed as a potential tool to evaluate pre-operative curve flexibility, with studies having correlated its curve measurements to those of in-brace correction10,11 and side-bending films.2,12 Given the difficulty in standardizing the extent of effort and force in side-bending radiographs-as well as the possibility of discomfort in association with their underlying spinal pathology-the supine radiograph has several potential advantages in assessing pre-operative flexibility and structurality, including ease and standardization. 2 This study demonstrated similar ability of the supine and side-bending radiographs as measures of curve flexibility for prediction of postoperative residual lumbar curvature following selective thoracic fusion. Therefore, our institution has discontinued use of supine radiographs preoperatively for Lenke 1 and 2 curves, which will provide important cost-savings and limit radiation exposure to our patients from unnecessary radiographs.
Undoubtedly, many preoperative and intraoperative factors influence residual lumbar curvatures. Some such factors include preoperative lumbar Cobb angle, flexibility, and Lenke classification modifier. We found that preoperative supine lumbar Cobb angle and preoperative side-bending Cobb angles had similar, positive correlations with postoperative lumbar Cobb angle, r = .55 (P < .001) and r = .54 (P < .001), respectively.
Three regression models were built to predict postoperative lumbar Cobb angles from preoperative variables, using supine lumbar Cobb (Model S), bending lumbar Cobb (Model B), and both supine and bending lumbar Cobbs (Model SB). All three models included the dichotomized Lenke modifier, and as anticipated, we found that larger preoperative Cobb angles tended to result in larger postoperative Cobb angles. The three models were similar in their ability to estimate the mean postoperative lumbar Cobb angle. Model SB (R2 = .49, P < .001) performed slightly better than the other two models, as might be expected, but not substantially better. Model S (R2 = .39, P < .001) and Model B (R2 = .44, P < .001) performed similarly to each other and nearly as well as Model SB. Therefore, either supine or side-bending radiographs alone may be used to estimate mean residual postoperative lumbar curvature to within 5.6° or less after selective posterior thoracic fusion, but little is to be gained by taking both supine and side-bending radiographs.
From a biomechanistic standpoint, supine radiographs eliminate gravity and allow the nonstructural spinal elements to relax and return to baseline. 2 The supine position also likely imparts a small derotational force on the thoracic and lumbar curvatures. The similarity of side-bending and supine radiographs in assessing flexibility likely emanates from different inherent limitations in both modalities. Side-bending radiographs result in greater lateral correctional forces but are effort-dependent and can be mechanically limited (eg costo-pelvic impingement in lower apex curves). Supine radiographs have lesser lateral correctional forces but are independent of effort and technique and can be less mechanically limited.
Studies have similarly attempted to construct complex mathematical models to predict post-operative lumbar curves, utilizing a number of pre-operative standing and flexibility measurements.13-15 This prediction is an important tool to guide deformity correction, as iatrogenic overcorrection of the thoracic curve relative to the residual lumbar curve has been associated with lumbar curve decompensation.13,16,17 Only one prior study has specifically evaluated the ability of pre-operative flexibility radiographs to predict post-operative residual lumbar curve magnitude following selective thoracic fusions in Lenke 1 and 2 curves. Dobbs et al
13
published a retrospective review of 100-patients with selective thoracic spinal fusions, and similar to our results, found that pre-operative supine lumbar Cobb angles have moderate correlation with final lumbar Cobb angles (r = .55, P < .0001). This study also utilized multiple linear regression analysis to develop a formula to help predict lumbar response in patients undergoing selective thoracic fusion with R2 = .72: Predicted Y = 14.4 + 3.06X1 + .30 X2 – .18 X3 + .81 X4 −.15 X5 – .16X6 Y = postoperative lumbar Cobb X1 = Lenke lumbar modifier (0 = B, 1 = C) X2 = preoperative standing lumbar Cobb angle X3 = preoperative supine lumbar Cobb angle X4 = preoperative push-prone lumbar Cobb X5 = preoperative standing thoracic Cobb X6 = % thoracic Cobb change from preoperative to immediate postoperative
While this model has a higher R2 than our model, it requires use of multiple preoperative flexibility images, including supine and push-prone views, with additional bending views required for Lenke classification. Additionally, their model incorporates a postoperative measurement, and therefore cannot be used preoperatively with the same R2 predictive capability for surgical planning purposes. When this prediction model by Dobbs et al is fit to our study dataset using Lenke B and C curves only (n = 29) and again using Lenke A, B, and C curves (n = 86), the R2 explained variation was only 40% and 53% respectively, which did not approach the 72% reported Dobbs et al (Appendix). This somewhat poorer performance is likely due to the absence of the pre-operative push-prone lumbar Cobb angle, which was the largest contributor in the Dobbs et al model (partial R2 = .58). Further prospective study would be helpful in comparing the relative predictive capabilities of flexibility films.
Building upon this prior study, we present the largest series of selective posterior thoracic fusions in assessing the prediction capabilities of the pre-operative flexibility radiographs, finding that either supine or side-bending radiographs alone may be used to estimate mean residual postoperative lumbar curvature to within 5.6°, which can be used to guide deformity correction and avoid overcorrection of the thoracic fusion. With the data from our study, one could conceivably make an argument for either supine or side-bending films as the pre-operative measure of choice-just not both. Given that bending radiographs are necessary for Lenke classification, and that Model B performs slightly better than Model S and nearly as well as Model SB, our institution has discontinued routine use of the supine film for Lenke 1 and 2 curves, and we now limit routine pre-operative flexibility evaluation to only side-bending films. This will provide important cost-savings and limit radiation exposure from unnecessary radiographs.
This study has important limitations. This is a retrospective study and is thus limited by the availability, quality, and reporting of the source data and radiographs. We attempted to standardize radiographic measurements with two reviewers using computer-assisted SurgiMap software; however, there is still some measurement error or bias that could have been introduced during the radiograph measurement process that could limit the generalizability of the results. Given the retrospective nature of this study, we were unable to control each individual radiographic encounter, including the appropriate amount of side-bending effort offered by each patient. We acknowledge this could introduce some error or bias in the correlations presented in this study. This study is limited to predicting compensatory lumbar curves after selective thoracic fusions for Lenke 1 and 2 curves; it cannot comment on the stiffer, main lumbar or thoracolumbar curves. Given the variable availability of retrospective data, we were unable to comprehensively study other preoperative and intraoperative variables, such as additional pre-operative flexibility measures (eg push-pull, traction), which may have provided further insight into post-operative lumbar predictability. Traction radiography has been a promising technique which has been shown in some studies to be superior to supine side-bending radiographs in assessing curve flexibility 18 and to be possibly predictive of actual curve correction after posterior fusion. 19 Future studies should evaluate incorporating these important techniques to reliably predict post-operative lumbar curvature.
This study represents the largest series of posterior selective thoracic fusions in assessing the prediction capabilities of pre-operative flexibility radiographs, finding that either supine or side-bending radiographs alone may be used to estimate mean residual postoperative lumbar curvature following selective thoracic fusion for Lenke 1 and 2 curves, but that both modalities are not needed. Since bending radiographs are important adjuncts in the determination of pre-operative curve flexibility and structurality for classification of AIS, we recommend against obtaining routine supine radiographs due to similar predictive value to side-bending radiographs, unnecessary cost, and increased radiation exposure.
Supplemental Material
Supplemental Material - Do Preoperative Supine Radiographs Predict Postoperative Residual Lumbar Curvatures in Adolescent Idiopathic Scoliosis? A Retrospective Cohort Study
Supplemental Material for Do Preoperative Supine Radiographs Predict Postoperative Residual Lumbar Curvatures in Adolescent Idiopathic Scoliosis? A Retrospective Cohort Study Prashant V. Rajan, MD, Richard Steiner, PhD, Todd F. Ritzman, MD, Trey Moberly, MD, and Lorena V. Floccari, MD in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PVR serves as a committee member of the North American Spine Society. RS reports no disclosures or conflicts of interest. TFR or an immediate family member is a member of a speakers’ bureau or has made paid presentations on behalf of Stryker; serves as an unpaid consultant to Apto Orthopaedics/Austin Bioinnovation Institute of Akron; serves as a paid consultant to Medtronic; has stock or stock options held in Apto Orthopaedics; serves as a board member, owner, officer, or committee member of AAOS, Foundation for the Advancement of Pediatric Orthopedics, and Pediatric Orthopaedic Society of North America; and on the Editorial or governing board of Journal of Bone and Joint Surgery-American and Journal of Pediatric Orthopedics. TM reports no disclosures or conflicts of interest. LVF or an immediate family member is an employee of Xellia pharmaceuticals; serves as a board member, owner, officer, or committee member of Pediatric Orthopaedic Society of North America; Pediatric Deputy Editor of European Journal of Orthopaedic Surgery and Traumatology
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
- Dr. Rajan serves as a committee member of the North American Spine Society
- Dr Steiner reports no disclosures or conflicts of interest
- Dr. Ritzman or an immediate family member is a member of a speakers’ bureau or has made paid presentations on behalf of Stryker; serves as an unpaid consultant to Apto Orthopaedics/Austin Bioinnovation Institute of Akron; serves as a paid consultant to Medtronic; has stock or stock options held in Apto Orthopaedics; serves as a board member, owner, officer, or committee member of AAOS, Foundation for the Advancement of Pediatric Orthopedics, and Pediatric Orthopaedic Society of North America; and on the Editorial or governing board of Journal of Bone and Joint Surgery-American and Journal of Pediatric Orthopedics
- Dr Moberly reports no disclosures or conflicts of interest
- Dr. Floccari or an immediate family member is an employee of Xellia pharmaceuticals; serves as a board member, owner, officer, or committee member of Pediatric Orthopaedic Society of North America; Pediatric Deputy Editor of European Journal of Orthopaedic Surgery and Traumatology
Supplemental Material
Supplement material for this article is available in online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.