
Abstract
Study Design
Retrospective cohort study.
Objective
Odontoid synchondrosis fracture is rare, and there is a paucity of literature on its surgical treatments. This case series study analyzed patients treated with C1 to C2 internal fixation with or without anterior atlantoaxial release and discussed the clinical effectiveness of the procedure.
Methods
Data were retrospectively collected from a single-center cohort of patients who had undergone surgical treatments for displaced odontoid synchondrosis fracture. The operation time and blood loss volume were recorded. Neurological function was assessed and classified using the Frankel grades. The odontoid process tilting angle (OPTA) was used to evaluate fracture reduction. Fusion duration and complications were also analyzed.
Results
Seven patients (1 boy and 6 girls) were included in the analysis. Three patients underwent anterior release and posterior fixation surgery, and the other 4 underwent posterior-only surgery. The fixation segment was C1 to C2. The average follow-up period was 34.7 ± 8.5 months. The average operation time was 145.7 ± 45.3 min, with an average blood loss volume of 95.7 ± 33.3 mL. The OPTA was corrected from 41.9° ± 11.1° preoperative to 2.4° ± 3.2° at the final follow-up (P < .05). The preoperative Frankel grade of 1 patient was grade C, of 2 patients was grade D, and of 4 patients was grade E. The neurological function of the patients in grade C and grade D recovered to grade E at the final follow-up. None of the patients developed a complication. All the patients achieved odontoid fracture healing.
Conclusion
Posterior C1 to C2 internal fixation with or without anterior atlantoaxial release is a safe and effective method for treating young children with displaced odontoid synchondrosis fracture.
Introduction
Cervical spine injuries, which infrequently occur in young children, accounting for 1.5% of overall pediatric traumas. 1 The majority of pediatric cervical spine injuries occur in the upper cervical spine, and C2 vertebra is the most frequently affected. It has been reported that 75% of cervical spine injuries are seen in children aged below 7 years, as the synchondrosis of the axis remains open at this age. 2 Despite the low incidence of these injuries, their management requires special deliberations due to the associated morbidity and mortality.3,4
In young children, the axis is separated by synchondroses. The odontoid basilar synchondrosis, where the odontoid process connects to the C2 vertebra, is particularly susceptible to trauma-induced fracture.5,6 Fracture through the odontoid synchondrosis is also known as odontoid epiphysiolysis or odontoid synchondritic slip. Hosalkar et al 7 proposed a classification system for these fractures. Type I injury is a fracture through the odontoid synchondrosis and type II injury is a fracture above the level of the synchondrosis. Type I injuries are further divided into subtype IA (0-10%), subtype IB (11%–100%), and subtype IC (>100%).
The management and treatment strategies for odontoid synchondrosis fractures are notably complex because of the distinctive spinal anatomy in pediatric patients. The treatment goals are to restore functional ability, prevent neurological deficits, and achieve fracture union, thus avoiding long-term disability. The initial treatment for such fractures is predominantly conservative therapy with external stabilization, which has shown a high fusion rate and is extensively recommended by spine surgeons. However, the possibility of surgical reduction and fixation still exists in cases with significant displacement, angulation, and accompanying neurological lesions, as the joint capsules and ligaments may be disrupted, and forcible closed reduction with traction may worsen such injuries. 8
Level 1 trauma centers encounter only a few children with odontoid synchondrosis fractures per year. 9 Hence, recommendations of surgical treatments for such injuries are mainly based on case reports. This study was designed to evaluate the functional outcomes of posterior C1 to C2 internal fixation with or without anterior release for patients with displaced odontoid synchondrosis fractures.
Materials and Methods
Study Population
We retrospectively analyzed young pediatric patients with displaced odontoid synchondrosis fractures that had undergone surgical treatment from January 2012 to June 2020. This study was approved by the Ethics Committee of our institution (No. K201805-11). Written informed consent was obtained from the parents of all participants. Patients who satisfied the following inclusion criteria were included (i) confirmed diagnosis with displaced odontoid synchondrosis fracture, (ii) delayed presentation (the duration from injury to admission was more than 2 weeks), (iii) non-reduction after skull traction or occipital-maxillary band traction, (iv) patients younger than 7 years, and (v) patients with a minimum follow-up period of 2 years. Exclusion criteria included (i) patients with fractures other than synchondrosis and (ii) patients with insufficient follow-up data.
Selection of Surgical Methods
After general anesthesia, the patient was positioned supine, and the neck was maintained in a neutral position. Under close neuromonitoring, skull traction was performed. The traction weight was gradually increased from 1/10 body weight, while monitoring the position of the fracture with serial radiographs. The maximum traction weight was 1/5 body weight. Traction was maintained for 15 to 20 min. If more than 1/3 reduction of the displacement was achieved, the displaced fracture was considered reducible, and the posterior-only surgery was selected. Otherwise, anterior release and reduction followed by posterior fixation were used.
Posterior-Only Surgery
The patient was positioned prone with a Mayfield head holder. Through a midline incision, the periosteum of C1 to C2 was exposed. The C2 nerve root ganglia were protected using a nerve stripper. A C1 lateral mass screw and C2 pedicle screw (or lateral mass screw) that were 18-24 mm in length and 3.5 mm in diameter were inserted under fluoroscopy. Thereafter, the articular capsules were exposed and the cartilage endplates were removed with a curette to release the joints. Through the loosen facets, abnormal calluses and fibrous scar tissues were scraped and released. C2 was pressed forward and the screws were locked to achieve reduction. After rinsing and placement of a drainage tube, the wound was closed in layers.
Anterior Release and Posterior Fixation
A right-sided submandibular retropharyngeal approach was employed to expose the prevertebral fascia of C1 to C2, the muscles and ligaments were dissected from the anterior surface of the atlantoaxial complex, and the abnormal calluses and fibrous scar tissues were cleared and removed from the fractured bone ends. The joint capsules were incised to release intra-articular adhesions. After meticulous hemostasis and wound closure, the patient was immediately turned prone for posterior fixation.
Postoperative Treatment
The patients were transferred to the intensive care units, where their respiratory and neurological conditions were closely monitored over a 24-hour period after the operations. The drainage tube was removed when the drainage volume was less than 10 mL/24 h. Radiography, computed tomography (CT), and magnetic resonance imaging (MRI) were conducted within 1 week after surgery. Patients were discharged after the incision healed.
Follow-Up
Follow-up examinations were performed at 1, 3, and 6 months and one year after discharge. Subsequent follow-ups occurred at one-year intervals. The neurological function of the patient was evaluated. Radiographs were reviewed at each follow-up to assess the reduction and healing of the odontoid fracture. If necessary, CT and MRI scans were further performed to confirm the healing of the odontoid fracture and spinal cord compression status.
Evaluation Standard
The surgical data including operation time, estimated bleeding volume, and complications were recorded. Neurological function was evaluated using the Frankel grade classification. The odontoid process tilting angle (OPTA), which was defined as the angle between the perpendicular line to the base of the vertebral body of the axis and the tangent line to the posterior surface of the odontoid process, was used to evaluate fracture reduction. 10 Odontoid fracture healing was determined by the formation of bridging bone.
Statistical Analysis
All data were presented as mean ± SD. Statistical significance was determined by unpaired t-test using the SPSS17.0 software (SPSS Chicago, IL, USA). P < .05 was considered statistically significant.
Results
Participant Demographics
Clinical Characteristics of the 7 Patients with Displaced Odontoid Synchondrosis Fracture.
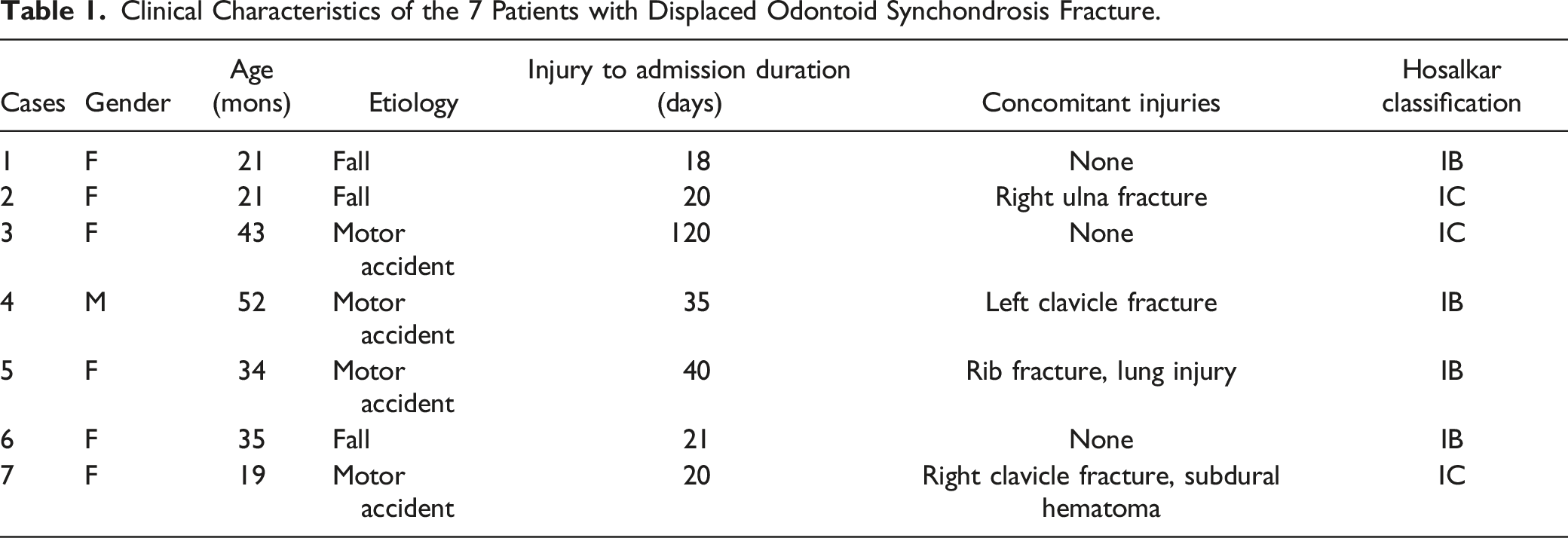
The most common clinical manifestations were neck-shoulder pain (7/7), restricted neck mobility (5/7), torticollis (4/7), and paralysis (3/7). According to Hosalkar et al’s classification, 7 4 patients had Type IB injury and 3 patients had Type IC injury.
Surgical Data
Details of Treatment and Outcome in the 7 Patients with Odontoid Synchondrosis Fracture.
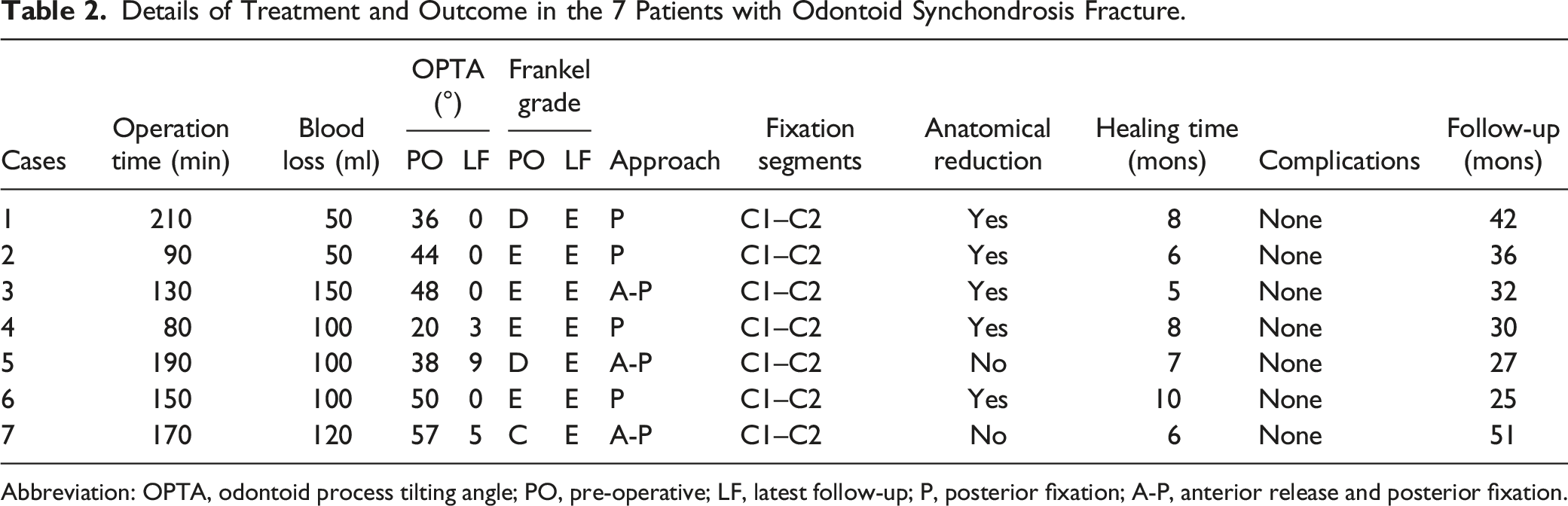
Abbreviation: OPTA, odontoid process tilting angle; PO, pre-operative; LF, latest follow-up; P, posterior fixation; A-P, anterior release and posterior fixation.
Recovery of Neurological Function
Preoperative Frankel grade classification indicated that the neurological function of 4 patients was grade E, of 2 patients was grade D, and of 1 patient was grade C. At 6 months follow-up, the neurological function of 1 case recovered from grade C to grade D, and 2 patients recovered from grade D to grade E. At the last follow-up, the neurological function of all the patients had recovered to grade E (Table 2).
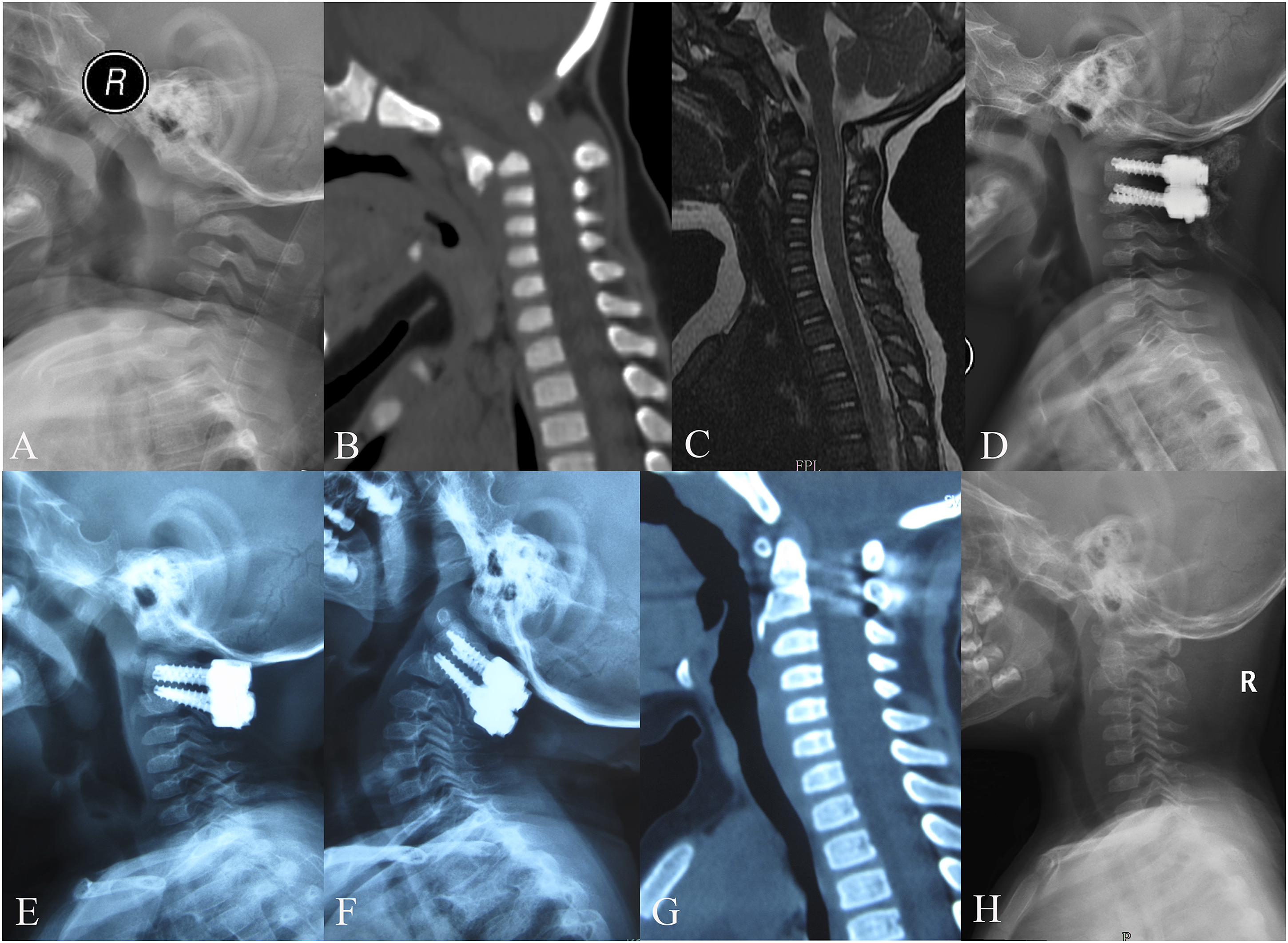
Reduction of Fracture
Of the 7 patients, 5 achieved anatomical reduction (Figures 1 and 2). The preoperative OPTA was 41.9° ± 11.1°, which was corrected to 6.9° ± 3.4° postoperatively (P < .05). At the final follow-up, the OPTA was 2.4° ± 3.2° (Table 2). A 21-month-old girl with displaced odontoid synchondrosis fracture. (A-B) Pre-operative lateral radiography and sagittal CT scan images show a fracture line through the odontoid synchondrosis with angulation and a 5-mm anterior displacement. (C) MR image shows an intact spinal cord. (D) The patient underwent posterior fixation, and post-operative lateral radiography shows that anatomical reduction was obtained. (E-F) At the 15-month follow-up, lateral radiographic and sagittal CT scan images show that odontoid fracture healing was achieved. (G-H) At the 34-month follow-up, the instruments were removed. A 21-month-old girl with displaced odontoid synchondrosis fracture. (A-B) Pre-operative lateral radiographic and sagittal CT scan images show a fracture line through the odontoid synchondrosis with severe anterior angulation and displacement. (C) MR image shows spinal stenosis. (D) The patient underwent anterior release and posterior fixation, and the post-operative lateral radiograph shows that anatomical reduction was obtained. (E) At the 6-month follow-up, lateral radiograph shows a favorable cervical alignment. (F-G) At the 12-month follow-up, lateral radiographic and sagittal CT scan images show that odontoid fracture healing was achieved. (H) The instruments were removed 25 months after the initial surgery.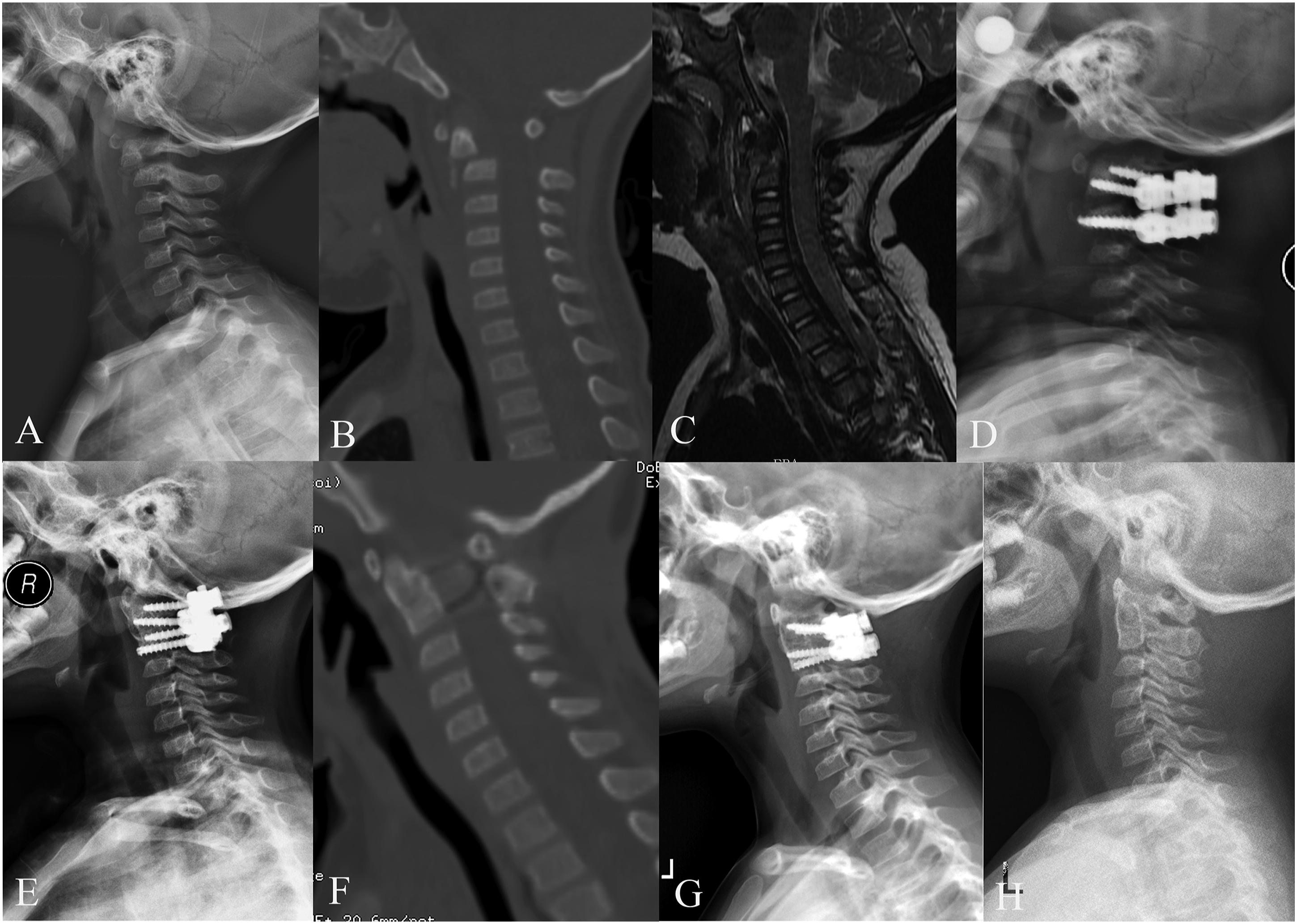
Complications and Healing of Odontoid Fracture
None of the patients developed a complication. All the patients achieved odontoid fracture healing, and the fracture healing duration was 7.1 ± 1.6 months (range, 5-10 months). At the final follow-up, none of the cases had developed fixation failure (Table 2).
Discussion
C2 is the most frequently injured vertebra in young children. This may be attributed to the unique biomechanics and anatomy of the pediatric vertebrae, including incomplete ossification of synchondroses, hypermobility due to ligamentous laxity, large cranium body ratio, and immature upper cervical musculature.11,12 Such structural characteristics make the odontoid synchondrosis prone to injuries even with minor trauma. 6 The common injury mechanisms include motor vehicle accident, sports-related injury, and falls. 9 Similar to previous reports, 4 patients experienced motor accident and 3 experienced a fall in this case series.
An understanding of odontoid synchondrosis fractures in young children is facilitated by an adequate awareness of the development of the axis. The axis is comprised of 5 primary ossification centers, which form the body, lateral masses, and dens axis. 13 The cartilage endplate between the odontoid and C2 body does not ossify until a child is aged 5 to 7 years old. Therefore, odontoid fractures in children usually occur through synchondrosis between the C2 body and the odontoid peg.
Detrimental consequences may be prevented if the fractures are identified early and managed appropriately. However, there are certain challenges regarding accurate and timely diagnosis of these fractures in pediatric patients. First, it is difficult to achieve accurate physical examination results in young children, and such patients often lack communicative competence and cannot respond to neurological examinations. In addition, concomitant injuries can conceal a patient’s odontoid synchondrosis fracture. Besides, because of the wide range of anatomical variants, plain radiographs are often misread. Under such circumstances, CT reconstructions may help to identify such fractures, and MRI can contribute to the evaluation of spinal cord and ligamentous injuries. For young children who present with neck-shoulder pain, restrained neck mobility, torticollis, and neurological symptoms, this type of fracture is suspected.
Fracture classification is typically employed to instruct treatment. The first classification system for odontoid fractures was designed by Anderson and D’Alonzo, 14 who divided the fractures into 3 types without distinguishing the skeletally mature adults from immature children. This classification is more suitable for patients with a closed synchondrosis. Pediatric injuries to the cartilaginous plates of the axis prior to bony fusion, despite their similarity to type II odontoid fracture in adults, are more accurately termed as “synchondrotic slips”.15,16 Hosalkar et al proposed the concept of “open basilar synchondrosis” for C2 synchondrosis fractures, and devised a new classification system according to the degree of displacement of the odontoid, the site of fracture, and the presence or absence of atlantoaxial dislocation. More recently, based upon Hosalkar et al.’s classification of displacement and Gore et al.’s 17 description of synchondroses, Rusin et al 18 reported a spectrum of C2 synchondrosis fractures involving 5 synchondroses in different combinations. However, Rusin et al.’s classification is complicated and incomprehensible for successfully classifying patients into each subtype. In the present study, Hosalkar et al.’s classification was employed to evaluate the odontoid synchondroses fractures.
There is still no consensus on the treatment for odontoid synchondrosis fractures. Conservative treatment using closed reduction and external stabilization is recommended by most authors.6,19-21 Fassett et al 6 reviewed 45 children treated with external stabilization, and reported that the fusion rate was 93%. Odent et al 22 reported that patients who had undergone external fixation had a better overall recovery compared with those who undergone surgery. However, conservative treatment carries a high rate of complication. A 68% complication rate was observed among 24 patients who received halo-vest immobilization. 23 Fulkerson et al 16 reported 2 cases who demonstrated progressive angulation despite being immobilized with external orthoses. By analyzing patients treated with halo fixation, it was noted that the complication rate was 43.3% and the nonunion rate was 11.4%. 16
For patients with severe dislocation, complete displacement, delayed presentation, spinal cord compression, and progressive deformity, surgical interventions with fixation are recommended.1,24,25 Some studies have documented a high complication rate following surgical treatments. However, those studies were published 2 decade ago, the outcomes were limited by the poor technology and improper internal fixation instrumentations. 22 Recently, improved spinal hardware has allowed for robust fixation and guaranteed favorable postoperative outcomes.8,16,26-29 Surgical fixation has significant advantages over conservative treatment. On the other hand, immediate and robust internal fixation provides more stability, thus enabling an early return to daily life activities. On the other hand, associated complications and discomforts caused by external immobilization can be avoided by internal fixation. 16
The significant angulation and/or neurological damage, and the delayed admission (range, 18-120 days) in our cases may have placed the patients at risk of nonunion with conservative therapy. Therefore, surgical reduction and stabilization for the patients were recommended and performed. The OPTA, which was a critical indicator of reduction, was corrected from 41.9° ± 11.1° preoperatively to 2.4° ± 3.2° postoperatively. All the patients in this study achieved odontoid fracture healing, and none developed fixation failure. Two patients did not achieve anatomical reduction. However, excellent remodeling was observed at the last follow-up. Based on previous literature, indications for surgery are summarized as (i) an OPTA of more than 30°, (ii) odontoid displacement of more than 10%, (iii) evidence of spinal cord injury, (iv) progressive deformity, and (v) failure of conservative management. 16
The soft and small vertebrae of young children with limited pull-out strengths make manipulation of the vertebrae difficult. However, the technological progress in preoperative and intraoperative imaging techniques has assisted surgeons in discerning anatomical variations in this population, thus guiding operative manipulations. 30 The application of preoperative CT remains the most reliable roadmap to identifying anatomical differences in each patient. In our cases, screws with lengths of 18 to 24 mm and diameters of 3.5 mm were successfully inserted.
This study has limitations. First, because odontoid synchondrosis fractures in children are rare, the present study included a small sample size. Therefore, the results obtained may be biased. Second, the participants were young children with poor communicative competence, and few functional assessment scales could be used to evaluate clinical outcomes. Third, although short-term follow-up showed favorable outcomes, long-term follow-up until skeletal maturity is encouraged to further investigate the clinical effectiveness of the surgical intervention.
Conclusions
In summary, posterior C1 to C2 internal fixation with or without anterior release is a safe and effective alternative treatment for young children with displaced odontoid synchondrosis fracture. As odontoid synchondrosis fractures are rare, multicenter prospective studies with a large sample size are encouraged to increase the current knowledge of this subject.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.