
Abstract
Study Design
Randomized controlled animal experiment.
Objectives
To determine and compare the efficacy of riluzole, MPS and the combination of two drugs in a rat model with acute spinal trauma, electrophysiologically and histopathologically.
Methods
59 rats were divided into 4 groups as control, riluzole (6 mg/kg, every 12 hours for 7 days), MPS (30 mg/kg, 2nd and 4th hours after injury) and riluzole + MPS. Spinal trauma was created and the subjects were followed for 7 days. Electrophysiological recordings were made via neuromonitoring. The subjects were sacrificed and histopathological examination was made.
Results
For the amplitude values, mean alteration in the period from the spinal cord injury to the end of the 7th day is 15.89 ± 20.00%, 210.93 ± 199.44%, 24.75% ± 10.13% increase and 18.91 ± 30.01% decrease for the control, riluzole, riluzole + MPS and MPS groups, respectively. Although the riluzole treatment group produced the greatest increase in amplitude, it was observed that no treatment provided a significant improvement compared to the control group, in terms of latency and amplitude. It was observed that there was significantly less cavitation area in the riluzole treatment group compared to the control group (P = .020). (P < .05).
Conclusions
Electrophysiologically, no treatment was found to provide significant improvement. Histopathologically, it was observed that riluzole provided significant neural tissue protection.
Introduction
Acute spinal injury is a process with a global incidence known to be approximately 10.5 per 100 000 1 and that is diffucult to treat due to the effects that ocur after trauma. Acute spinal injury consists of secondary injury that develops over time after the mechanical cause disappears after the primary injury, which occurs as a result of mechanical effects at the time of injury, and continues at the cellular level. 2 The medical literature, on the other hand, has focused on preventing this ongoing injury at the cellular level, and methylprednisolone (MPS, Steroid) has been the most popular among the most frequently applied medical (drug) treatments among the treatment options with this target. MPS stabilizes cell membranes by inhibiting lipid peroxidation and neurofilament degradation, and protects the blood-brain barrier. Theoretically, it is thought that due to these anti-inflammatory properties, it reduces vasoactive metabolites released from arachidonic acid metabolism, thus reducing cord edema and increasing cord perfusion.3-5 However, scientific data on the usefulness of this drug are controversial and it is mentioned that it has side effects.6-8
Research continues on the use of the drug riluzole, which is used in some neurological diseases (Amyotrophic Lateral Sclerosis, ALS), in patients with acute spinal trauma. 9 These studies were accelerated by the discovery of some biochemical activities during spinal trauma, such as extracellular accumulation of glutamate, increased intracellular calcium, overproduction of reactive oxygen radicals, and lipid peroxidation.10-19 Riluzole is in the benzothiazole derivative anticonvulsant group, which is a sodium channel blocker, and was approved for use in the treatment of ALS by the FDA in 1995 for its neuroprotective effects. 9 A harmful amount of sodium accumulation occurs in neurons after acute spinal trauma. 20 The inability to remove sodium cellularly causes membrane depolarization and increases the entry of sodium into the cell. Sodium channel blockers exert their neuroprotective effect by preventing the increase in intracellular sodium and reversing the operation of axonal sodium/calcium pumps. The aim of this study has been to investigate the combined effects of riluzole, MPS and these two drugs electrophysiologically and histopathologically on a rat model with acute spinal cord injury. Previous studies show a lack of electrophysiological examination of damage or are insufficient in drug combination comparisons. With the numeric data which will be collected as a result of this research, it will be possible to make a more objective observation compared to the previous experimental researches, that included more subjective measurements.
Materials and Methods
Experimental Procedure
The study started with the ethics approval of Bursa Uludag University Animal Experiments Local Ethics Committee decision no 2021-02/05. 59 adult female Wistar-Albino type rats weighing 250-300 g obtained from Bursa Uludağ University Faculty of Medicine Experimental Animal Breeding and Research Unit. The subjects were randomized to control (n = 13), riluzole (n = 13), MPS (n = 19).) and riluzole + MPS (n = 14) treatment groups. All subjects were kept on a 12-12Phour light-dark cycle and the room temperature was kept stable throughout the experiment (20°C ± 2°C). No subject’s access to food and water was restricted. After paraplegia, manual bladder emptying was performed 3 times a day.
Anesthesia was induced by inhalation of 2% dose of sevoflurane (Sevorane 100%, AbbVie, Illinois, USA) and was completed by using 60 mg/kg intramuscular (IM) ketamine,
21
Ketax (VEM, Istanbul, Turkey) in 500 mg/10 mL ampoule form. The reason ketamine was used as an anesthetic agent is because it is known to have little effect on Motor Evoked Potentials (MEP) values.
22
Ventilation was provided with oxygen. The depth of anesthesia was determined by pedal reflex control, and the color of the reflective eye and mucous membrane colors were followed at regular intervals for vital monitoring purposes. For the neuromonitoring process, 3 electrodes with 2 probes each were connected to the subjects. One of them is connected to the vertex region, one to the left quadriceps muscle, and one to the right quadriceps muscle for grounding purposes (Figure 1A). A: Placement of neuromonitoring electrodes. B: Laminectomy. C: Advancing embolectomy catheter through epidural space.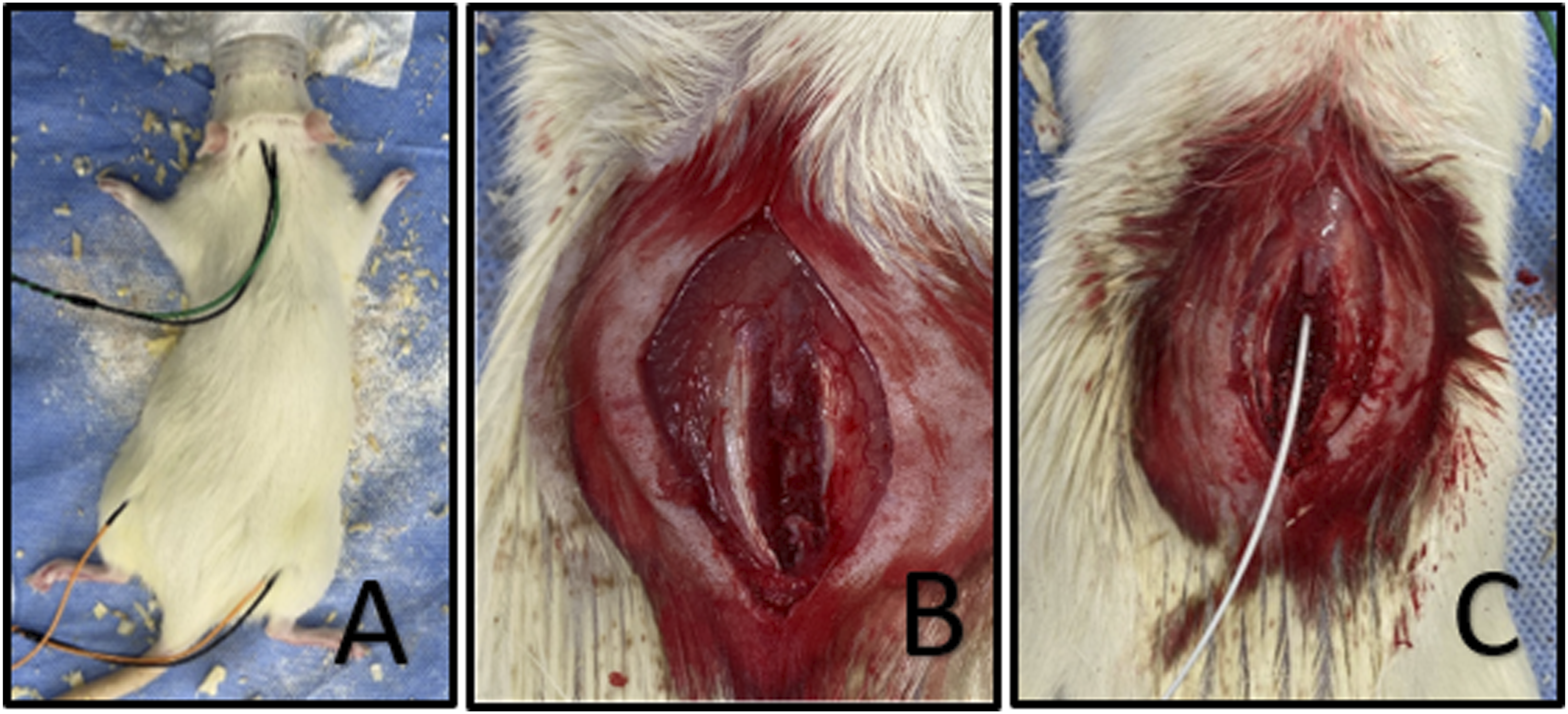
The subject was stabilized in the prone position and the back hair was shaved. The surgical field was sterilized with povidine iodine. A dorsal incision was made at the thoracic vertebral level, and the posterior vertebral elements were reached by dissecting the paraspinal muscles. Laminectomy was performed using a high-speed drill (Figure 1B). The MEP value was recorded again with neuromonitoring. After making sure that spinal cord damage did not develop during laminectomy with the MEP values obtained, Fogarty (Edwards, California, USA) embolectomy catheter (french 2 size) of appropriate size was advanced to the T10-12 level (13th rib was palpated and the desired vertebra was reached by counting the spinous processes towards the cranium) and repeated MEP values taken (Figure 1C). After making sure once again that spinal cord damage did not develop, compression damage was performed on the spinal cord by inflating it (at the same pressure for all subjects and for 8 minutes). MEP values were obtained with neuromonitoring and spinal cord damage development was observed. After the incision site was irrigated with saline, the skin was sutured with a stapler and dressed with povidin-iodine. Our experimental model was designed in a similar way to Stutzmann et al's previous experimental model, 23 as we think that a trauma that compresses the spinal cord due to fragments retropulsed into the medullary canal with the resulting hematoma secondary to unstable vertebral fractures such as AO type B or type C can be best imitated by this model.
Administration of Treatment Agents
The MPS dosing used in our experiment was determined as 30 mg/kg, to be administered at the 2nd and 4th hours of the injury on the 1st day, as milligrams per kilogram prescribed by the Bracken protocol.8,24,25 MPS was administered Intraperitoneally (IP). It is known that the safe treatment dose of riluzole for ALS in humans is 2 × 1 50 mg. 26 Using the human equivalent dose (HED) formula based on animal experiments in the 2005 FDA (Food and Drug Administration) industrial guideline, the average dose of riluzole to be used in our experiment was found to be 2 × 1 6 mg/kg.9,27 For administration of Riluzole, Rilutek (Sanofi-Aventis, Paris, France) 50 mg tablet form is crushed into powder and fixated in Tween 80 solution (ZAG chemistry, Istanbul, Turkey) which is used as an emulsifier in the food industry and known as polyoxyethylenesorbitan monooleate (polysorbate), as similar to the experimental procedure described by Zgrajka et al and Rejdak et al.28,29 This gavage form administered to subjects in desired dosage perorally (PO) once in 12 hours for 7 days starting from the injury.
Neuromonitoring
MEP (Motor Evoked Potentials) values were measured with the Medtronic - Xomed NIM-ECLIPSE SD neuromonitoring device (Medtronic Sofamor Danek, USA). In our study, 3 electrodes, each of which has 2 probes (needles), were connected to the subjects for the neuromonitoring process. One of them was connected to the vertex region, one to the left quadriceps muscle, and one to the right quadriceps muscle for grounding purposes. Stimulation was given with an average of 5-10 mA until obtaining a proper wave form, and latency (msec) and amplitude (mV) values were recorded. 30 The bandwidth was determined as 15-3000 Hz, and the record interval was determined as 10 msec. It was aimed to be reproducible in order to understand whether the values were meaningful or not, and it was seen that similar waves were obtained by giving multiple stimulation. Due to the known depressive effect of inhaled anesthesia on MEP values, MEP measurement was discontinued for 8 minutes 31 before measurement. 32
MEP values were measured at the beginning of the experiment (pre-experiment) (Figure 2A), after laminectomy (Figure 2B), after catheter advancement (Figure 2C), after baloon inflation (Figure 2D), on the 4th and 7th days. It was aimed to understand that the spinal injury model was created homogeneously for all subjects by obtaining MEP values during the phases of experiment. Neuromonitoring of a subject at first day of experiment (Vertical arrows shows amplitude measurement while horizontal arrows shows latency measurement of MEP values.) A: Pre-experimental B: After laminectomy C: After embolectomy catheter advancement through epidural space D: After inflation of catheter. (Note the amplitude decrease and latency increase).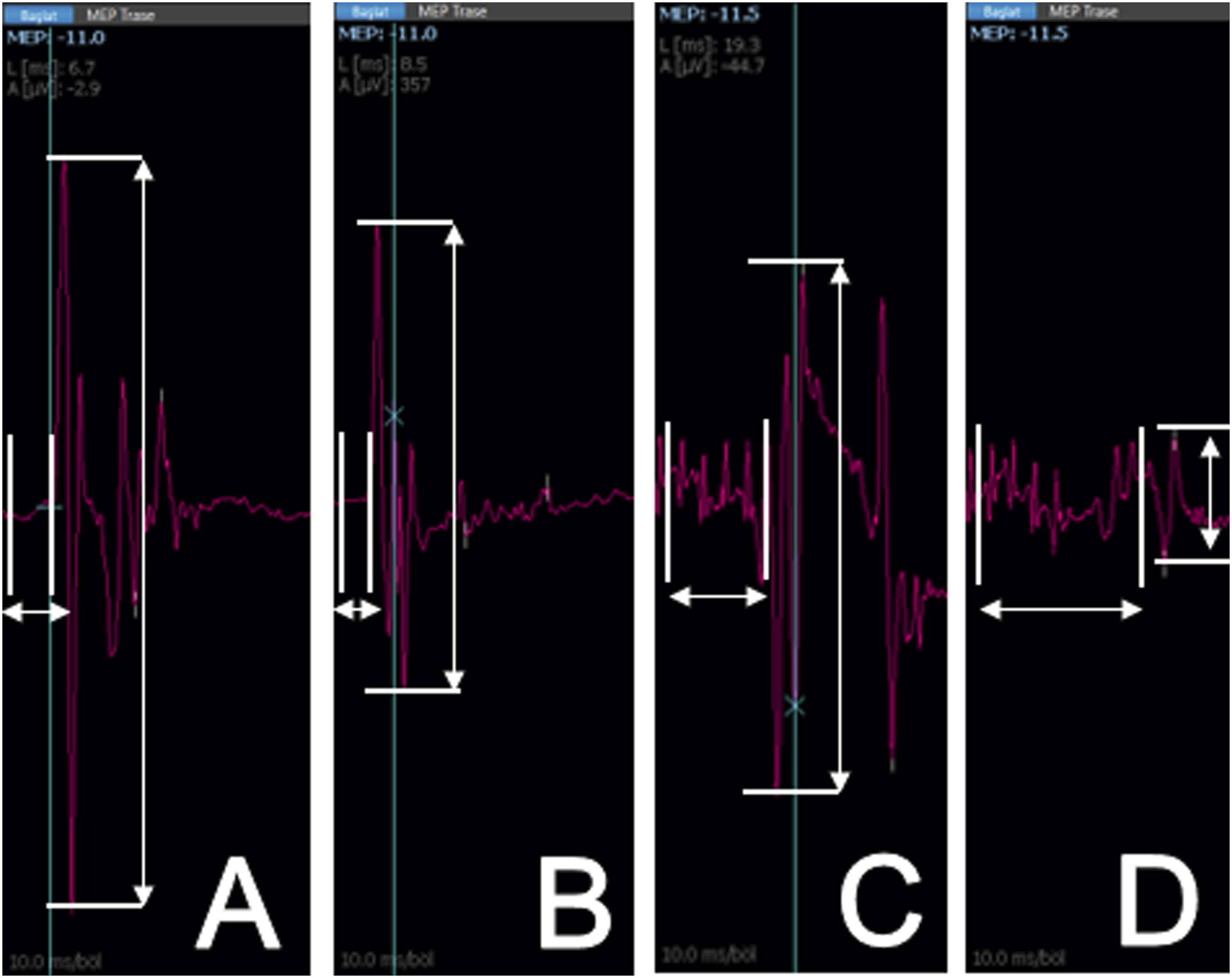
Histopathological Examination
The spinal injury area of the subjects was excised together with the surrounding muscle tissues after sacrification. After the decalcification process, the columna vertebralis was sliced horizontally at right angles to the coronal plane and taken into cassettes. Then, they were embedded in paraffin and 4 μm thick sections were taken from the paraffin blocks. Sections were stained with Hematoxylin and Eosin (H&E) and examined under a light microscope, and photographs were taken from each slide with a ×4 magnified lens. With ImageJ© (a Java-based image processing program developed in the National Institutes of Health and Optics and Computational Instrumentation Laboratory) program, the total medulla spinalis (Figure 3B) and cavitation areas (Figure 3A) in each subject’s samples were calculated separately as pixels per inch (PPI). For each subject, all samples were averaged and the mean lesion area was proportioned to the mean total spinal cord area. This ratio was used as a percentage for comparison between groups. Histopathological examination with ImageJ software A: Calculation of cross-sectional cavitation area B: Calculation of total medulla spinalis cross-sectional area.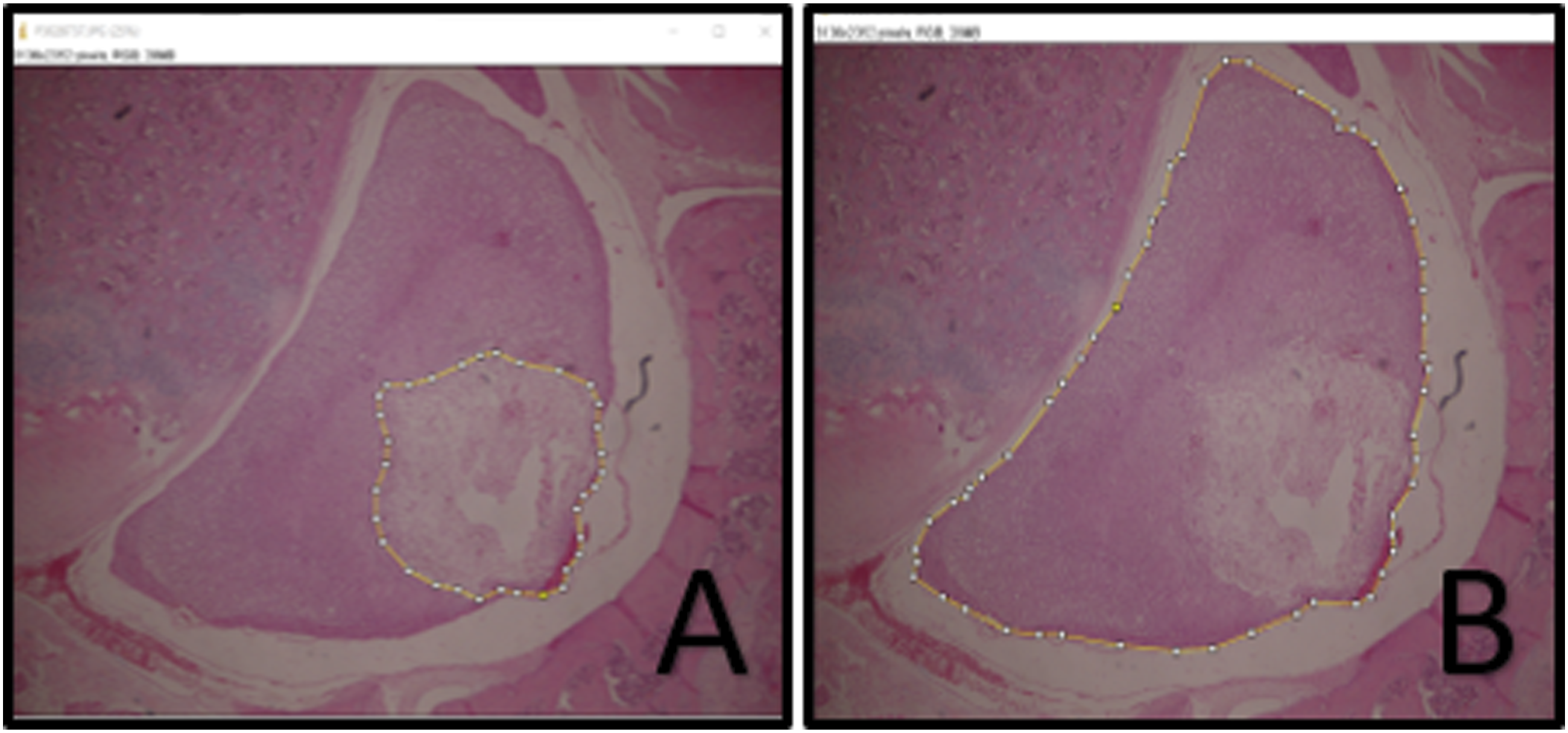
Statistical Analysis
After completing the power analysis by examining similar articles, it was found that the required number of subjects was 8 for each group, with 5% significance, 80% power and .6 effect size. Statistical analysis of the data was performed in the statistical package program IBM SPSS 23.0 (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.). The Shapiro-Wilk test was used to examine whether the data showed a normal distribution or not. Descriptive statistics are expressed as mean and standard deviation or median (minimum-maximum) for quantitative data, and frequency and percentage for qualitative data. For normally distributed data, Kruskal Wallis test was used when one-way analysis of variance did not show normal distribution in more than two group comparisons. In case of significance, Bonferroni-Dunn test, one of the multiple comparison tests, was used. Comparison of repeated measurements between groups was made by calculating the percent change value from the initial measurement (percentage of change= (last measurement – first measurement) ÷ first measurement). It was analysed with the Spearman correlation coefficient. The significance level was determined as P = .05.
Results
Neuromonitoring
Demographic of Subjects and P Values for Interindividual Homogenity Comparison.
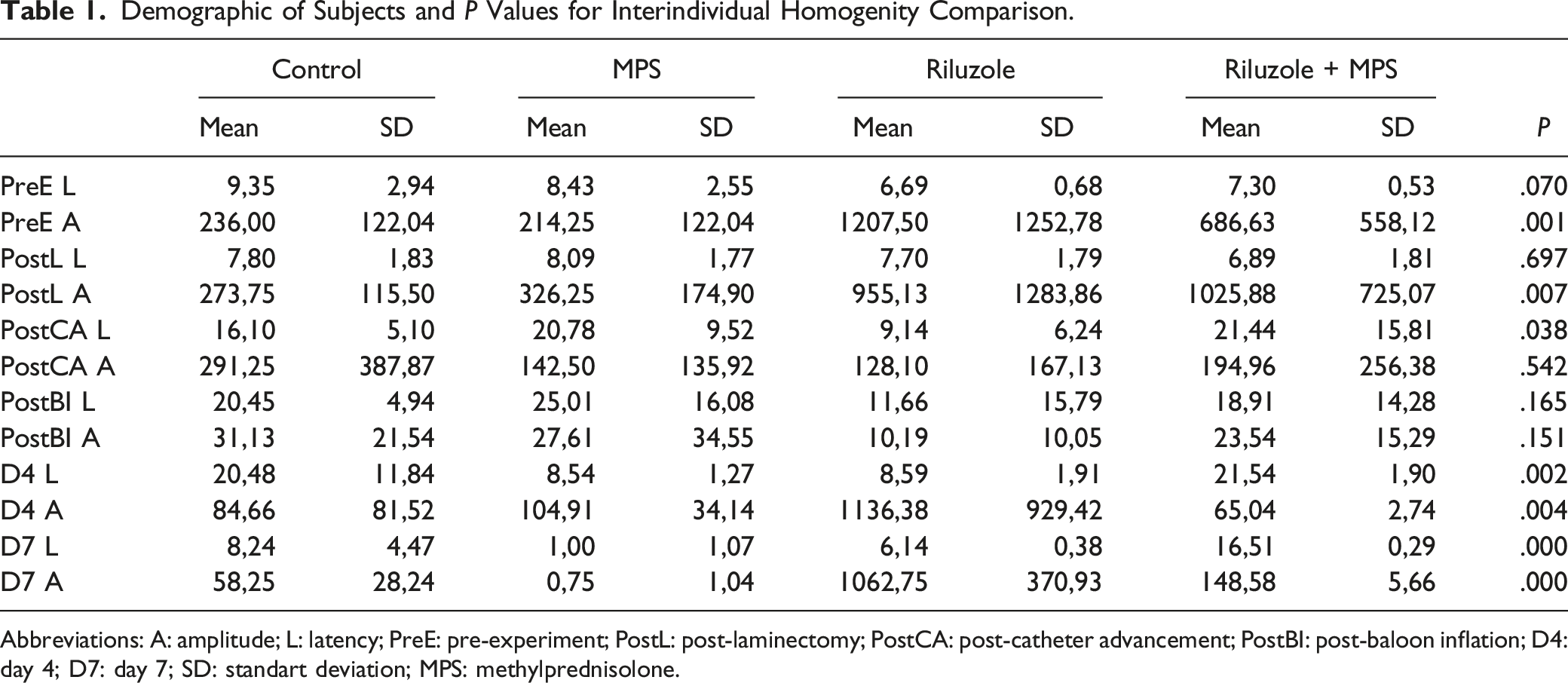
Abbreviations: A: amplitude; L: latency; PreE: pre-experiment; PostL: post-laminectomy; PostCA: post-catheter advancement; PostBI: post-baloon inflation; D4: day 4; D7: day 7; SD: standart deviation; MPS: methylprednisolone.
Demographic of Percentage Alterations and P Values for Homogenity of Experimental Procedure.
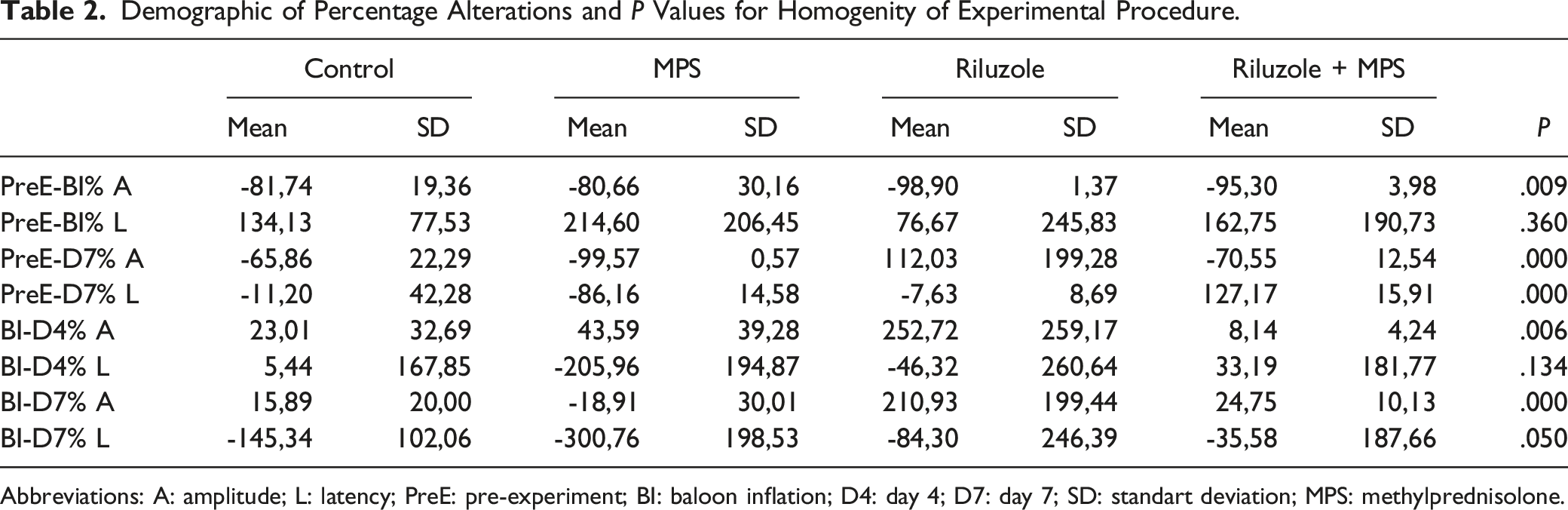
Abbreviations: A: amplitude; L: latency; PreE: pre-experiment; BI: baloon inflation; D4: day 4; D7: day 7; SD: standart deviation; MPS: methylprednisolone.
Pairwise Comparison of Groups for Treatment Superiority in Parameters of Baloon Inflation to End of Day 7 amplitude/latency % Alteration and Histopathological % Cavitation Area.
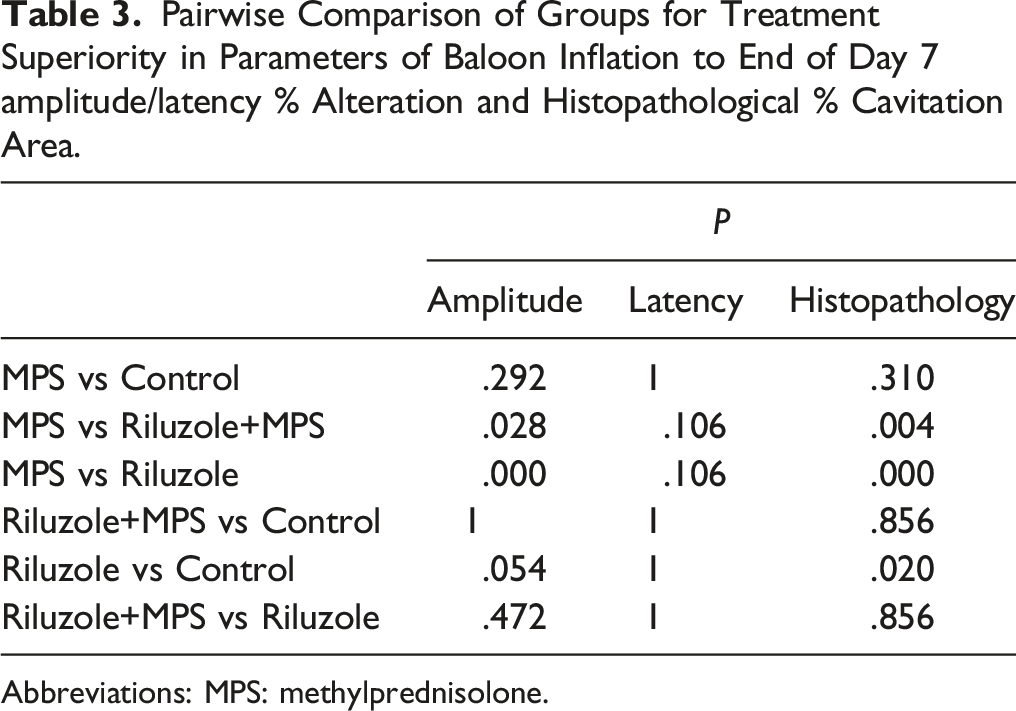
Abbreviations: MPS: methylprednisolone.
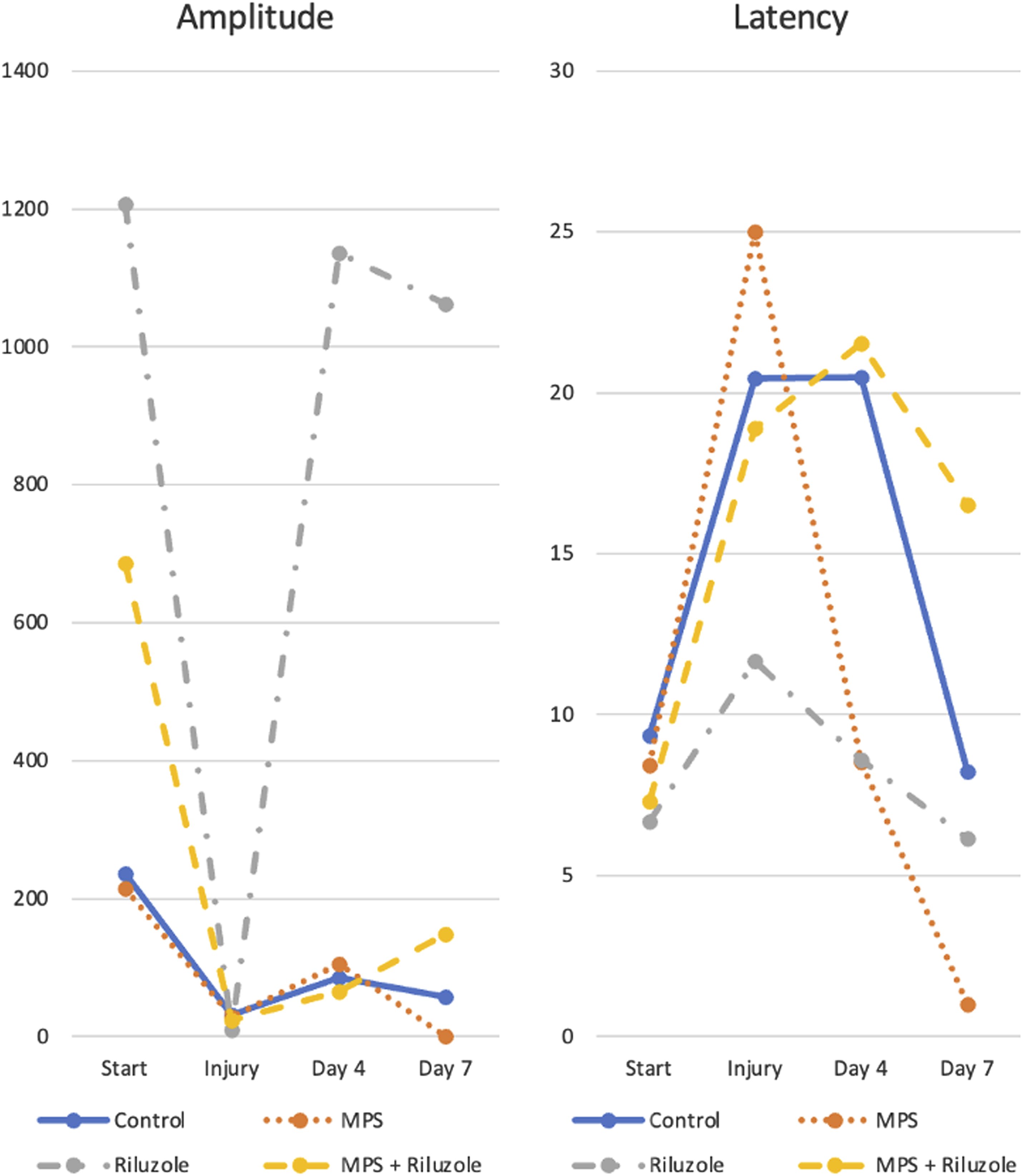
Alterations of amplitude and latency parameters for all groups.
Histopathology
Histopathological Demographics of Subjects and P Values for Homogenity Comparison of Cross-sectional Areas.
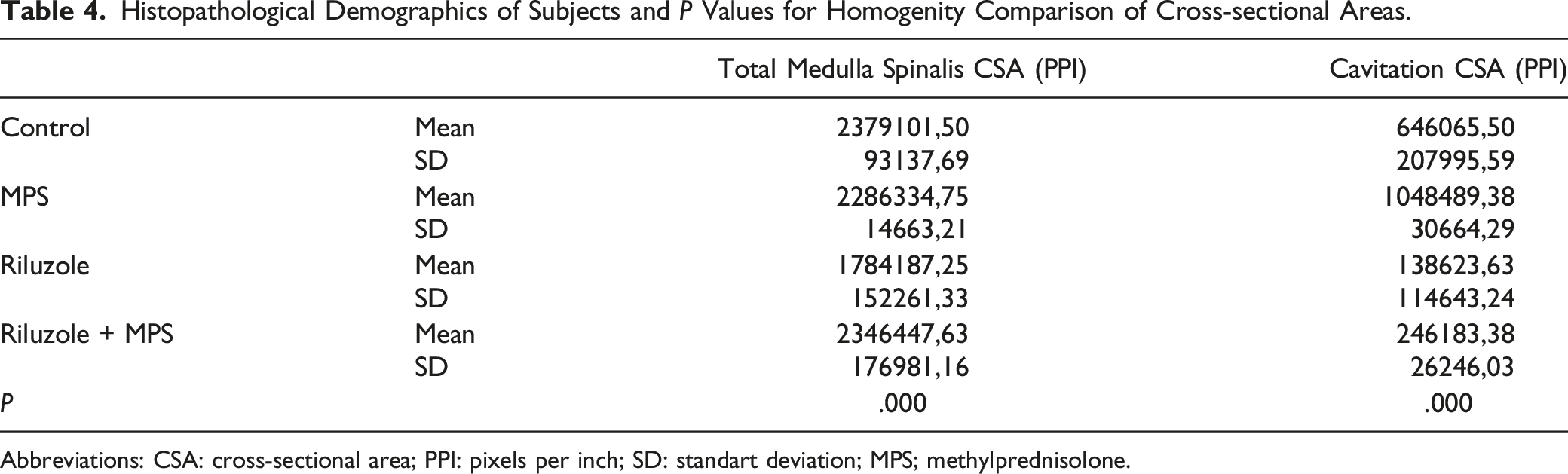
Abbreviations: CSA: cross-sectional area; PPI: pixels per inch; SD: standart deviation; MPS; methylprednisolone.
Discussion
In our study, it was observed that riluzole treatment was generally successful. Riluzole’s sodium channel blockage can reduce the amount of intracellular sodium by reversing the sodium/calcium exchange pump, and at the same time, protects the action potentials by preventing the deterioration of the sodium/hydrogen antiport pump 33 and inhibits presynaptic calcium-dependent glutamate excretion. 34 The inability to regulate calcium ion concentration is seen as a common feature of cell death mechanisms. 35 Excitotoxicity occurs by the diffusion of glutamate from the cells directly damaged during trauma to the extracellular space by disruption of the Na+-K+ ATPase membrane transporter. The increased level of glutamate causes sodium and calcium to enter the cell through NMDA and alpha-amino-3-hydroxy-5-methyl-isoxalopropionate/kainate receptors (AMPA) and cause excitotoxicity. 36 The neuroprotective property of sodium channel blockers is thought to be effective in this phase of injury, which is called the early acute phase. 9 It is thought that these neuroprotective effects lead to positive results on spinal cord injury, as supported in the literature,23,27,37-42 and it was observed in our study that they were correlated. Riluzole’s failure to provide significant electrophysiological improvement can be explained by the limited number of subjects, the sensitivity of MEP values to the dose of inhaler anesthesia, 32 and the difficulty of controlling the dose.
It has been found that MPS treatment, which is the most popular treatment agent in the indication of acute spinal injury in most clinics, is the most unsuccessful treatment. Although a few published article has considered that MPS inhibits lipid peroxidation and neurofilament destruction and protects the blood-brain barrier, reduces vasoactive metabolites, thereby reducing cord edema and increasing cord perfusion,3-5 in the approach to spinal injury guideline updates 2013 and 2017, the recommendation for MPS to be used in the treatment of acute spinal injury has been removed and stated that these beneficial cellular-based effects are controversial, clinicians should consider that this drug is not FDA approved for this indication, there is no level 1 and 2 evidence, and level 3 evidence emerged by coincidence. Also it has been seen in the guides that there are level 1-2-3 evidences about harmful side effects.6,43 In our study, it has been shown that MPS has negative effects on cord healing. It was observed that the highest number of deaths have occurred in the MPS treatment group throughout the experimental period. This is thought to be the result of the known immunosuppressive effects of MPS predisposing the subject to infection (such as pneumonia, surgical site infections, sepsis)44,45 and is thought to be a cause of failure in cord healing. Despite not being statistically evaluated as it is not our primary target, myositis at the surrounding muscle tissue and coagualition necrosis is slightly more dominant at the MPS group, which may supports the surgical site healing failure. In fact, in our study, it was seen that MPS had a more damaging effect on the cord than a healing feature in terms of MEP values (a decrease was observed in the MPS group despite a percent increase in amplitude over time in each group) and the feasible reasons for this depressive effect, although not amongst the parameters that were evaluated in our study, are wound infection due to immunosuppression and possible secondary spinal infections. On the contrary, MPS caused a decrease in latency values. It was considered to have no scientific value since there was no statistical significance in terms of percentage changes in latency values between any of the groups. It was thought that the use of riluzole in combination with MPS did not achieve as much success as riluzole, due to the negative effect of MPS on recovery, which prevented the success of treatment with riluzole.
In the literature, it is seen that BBB (Basso, Beattie, Bresnahan) motor scale and inclined plane tests are used in other studies where MPS and riluzole are evaluated with similar experimental procedures, which are based on observation and provided subjective data.27,39,40,46 In our study, it was preferred to make an evaluation on numerical data with neuromonitoring in order to avoid observational errors. The reason why MEP is preferred over SEP in our experimental procedure can be explained by the fact that it is an electrophysiological indicator of motor force. 47 In other similar studies using neuromonitoring, it was observed that MPS, which is still used in some clinics and is a popular treatment agent, was not evaluated.23,38,42
The major drawback of our study is that the experimental procedure-although this was difficult to create-was not fully homogeneous. (Table 2; amplitude value alteration percentages between spinal injury and pre-experimental values - mentioned as PreE-BI% - were significantly different between groups, P = .009) It was thought that the equal damage to the spinal cord for all subjects was due to the irregularity of the pressure distribution created by the balloon of the embolectomy catheter while inflating in the epidural space mentioned in the experimental procedure (a manually inflated balloon) and possible differences in the epidural space distance between the subjects. At the same time, the fact that MEP values are affected by the dose of inhaler anesthesia 32 and the difficulties in controlling the dose may be the reason for the statistical result indicating that the damage is not created homogeneously. Last but not least, pre-experimental MEP values dissimilarities (pre-experimental amplitudes, post-laminectomy amplitudes, post-catheter advancement latencies) (Table 1; P = .001, .007, .038 respectively). Could be a result of possible interindividual biological disparities as mentioned in studies conducted by Fujiki et al and Maeda et al.48,49 Lastly, significant number of subject exitus occured for all groups during experiment. It was estimated that this was due to excessive damage created. It was observed that after being paraplegic, access to food and water and self care of subjects gradually decreased.
Conclusion
It seems that classical MPS treatment does not show any benefit in acute spinal injury, even increasing spinal cord damage, and current guidelines also support this information. While it’s not certain, Riluzole, one of the new and promising treatment agents, may be used in the near future with this indication. Although it does not affect the electrophysiological results significantly, it is thought that riluzole has proven itself in histopathological improvement. We think that the neuroprotective effect of riluzole by regulating the cellular sodium circulation prevents the damaging effects of secondary injury mechanisms that develop after trauma to the spinal cord, thus providing hope to thousands of patients every year. In order for Riluzole to be approved for routine use, it needs to be supported by clinical studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.