
Abstract
Study Design
Retrospective Cohort Study.
Objectives
To determine the ability of early vital sign abnormalities to predict functional independence in patients with SCI that required surgery.
Methods
A retrospective analysis of data extracted from the Pennsylvania Trauma Outcome Study database. Inclusion criteria were patients >18 years with a diagnosis of SCI who required urgent spine surgery in Pennsylvania from 1/1/2010-12/31/2020 and had complete records available.
Results
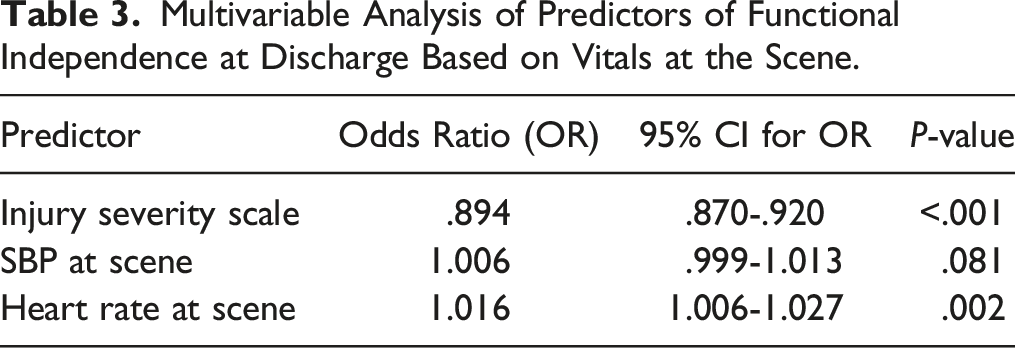
A total of 644 patients met the inclusion criteria. The mean age was 47.1 ± 14.9 years old and the mean injury severity score (ISS) was 22.3 ± 12.7 with the SCI occurring in the cervical, thoracic, and lumbar spine in 61.8%, 19.6% and 18.0%, respectively. Multivariable logistic regression analyses for predictors of functional independence at discharge showed that higher HR at the scene (OR 1.016, 95% CI 1.006-1.027, P = .002) and lower ISS score (OR .894, 95% CI .870-.920, P < .001) were significant predictors of functional independence. Similarly, higher admission HR (OR 1.015, 95% CI 1.004-1.027, P = .008) and lower ISS score (OR .880, 95% CI 0.864-.914, P < .001) were significant predictors of functional independence. Peak Youden indices showed that patients with HR at scene >70 and admission HR ≥83 were more likely to achieve functional independence.
Conclusions
Early heart rate is a strong predictor of functional independence in patients with SCI. HR at scene >70 and admission HR ≥83 is associated with improved outcomes, suggesting lack of neurogenic shock.
Introduction
Spinal cord injury (SCI) is a devastating disorder that leads to significant short- and long-term morbidity with regard to both physical and mental health for patients.1,2 The annual incidence of spinal cord injuries in the US is estimated at 54 cases per million with vehicular accidents and falls remaining the leading cause. 3 Previous studies have identified numerous variables to reliably predict functional outcome after spinal cord injury, some of which are grade of injury by the ASIA Impairment Scale (AIS), injury location or level of injury, severity of neurological injury, age, and blood pressure.4-8 Given the high incidence of SCI and its complex management, a clear prognosis for patients following SCI is imperative for counseling and rehabilitation, which ultimately affects quality of life and performance status. 9
Early fluid resuscitation and inpatient blood pressure (BP) management to maintain a mean arterial pressure (MAP) above 85 mmHg is a critical component of early SCI management to prevent neurogenic shock and aid tissue perfusion.10-12 Maintaining a MAP >85 mmHg has been shown to improve neurological recovery and decrease mortality in the SCI population.13-16 A study by Dakson et al demonstrated that even just 2 consecutive hours with MAPs less than 85 mmHg decreased a patient’s likelihood of neurological improvement 11-fold when compared to a patient with MAPs maintained above 85 mmHg for the first 5 days post-injury. 17 Additionally, the spinal cord plays an immense role in hemodynamic and cardiovascular homeostasis, which is why vital sign abnormalities may be a valuable surrogate to predict outcomes after SCI. A few studies have indicated that severity of injury is inversely related to heart rate with those with the highest degree of injury exhibiting lower heart rates.18,19 Bradycardia in the setting of SCI suggests neurogenic shock, which is clinically defined as a systolic blood pressure (SBP) of <100 mmHg and a pulse of <80 beats per minutes. Neurogenic shock typically occurs in approximately 20% of cervical SCI patients, while in 7% and 3% of thoracic and lumbar injury, due to injury to sympathetic outflow seen in lesions higher on the spinal cord.20,21 The resultant autonomic dysreflexia also predisposes SCI patients to other complications, such as venous thromboembolic events (VTE), respiratory dysfunction, pressure ulcers, and more that can worsen prognosis. 22
Despite the importance of spinal cord perfusion and its effect on SCI, there is a paucity of literature on the predictive capability of early vital signs on functional outcome after SCI. In this study, we use the Pennsylvania Trauma Systems Foundation (PTSF) registry to determine the impact of blood pressure and heart rate at the scene and on admission on the functional recovery of patients with SCI who required surgery.
Methods
Patient Selection and Variables
The study protocol was approved by the University Institutional Review Board (#20D.1092). We conducted a retrospective analysis of 272,174 patients admitted at a hospital in Pennsylvania from January 2010 to December 2020 after sustaining a trauma from the Pennsylvania Trauma Systems Foundation (PTSF) patient registry. The registry was queried using the ICD-9 806 and 952 codes and ICD-10 S14, S24, and S34 codes to identify patients with spinal cord injury who underwent surgery. Patients who did not require surgery were excluded to decrease the heterogeneity of the study population and improve the generalizability of the study findings to neurosurgical patients. Patient age, gender, race, ethnicity, cause of spinal cord injury (SCI), insurance, GCS at the scene, Injury Severity Score (ISS), level of SCI, vital signs at the scene and on admission, patient comorbidities, surgery status, functional status at discharge (FSD) (locomotion, transfer mobility, feeding, expression and social interaction) were provided for these patients. The severity of injuries on admission is provided using the injury severity scale that ranges from 0 (no injury) to 75 (unsurvivable injury). 23 The primary endpoint is functional independence as determined by the locomotion and transfer mobility components of the FSD scale that is graded by a physiatrist. Each of them is scored from 1 to 4 (1 = complete dependence, 2 = modified dependence, 3 = independent with device, 4 = complete independence). 24 Functional independence included scores 3 and 4 from both the locomotion and transfer mobility variables. Patients scoring less than 3 for either locomotion or transfer mobility were therefore designated as functionally dependent. Patients who were missing locomotion or transfer mobility scores were excluded. Data collection was conducted securely without sharing of identifiable personal health information. Individual patient consent was not obtained given the retrospective, noninterventional design of the study that was based on query of an existing database.
Statistical Analysis
Data is presented as mean and standard deviation (SD) for continuous variables that are normally distributed and median and interquartile range (IQR) for non-normally distributed variables. Normality was assessed using the Shapiro-Wilks test. Categorical variables are presented with count and frequency. Associations were determined by χ2, χ2-trend, Fisher’s Exact, as appropriate. Univariable analysis was carried out using unpaired t-test, Chi-square, and Fisher’s exact tests, Mann-Whitney U, Spearman Rank, as appropriate. If identified as predictive (defined herein as P < .20) of the endpoint on univariate analysis, the variable was included in a multivariable backward conditional logistic regression model. Results from multivariable logistic regression are reported as odds ratios (ORs), 95% confidence intervals (CI), and significance. Statistical significance was achieved when P-value was <.05. Statistical analysis was carried out with IBM SPSS (Version 26.0. Armonk, NY: IBM Corp.).
Results
A total of 644 patients were identified from the PTSF registry that were admitted at a Pennsylvania trauma center from 2010-2020 with the diagnosis of spinal cord injury and required spine surgery (Figure 1). The mean age was 47.1 ± 14.9 years and males comprising 76.7% of the patients. The most common causes of SCI were falls (51.2%), motor vehicle accidents (36.8%), and violence (3.7%). The mean injury severity score (ISS) of this cohort was 22.3 ± 12.7 with the SCI occurring in the cervical, thoracic and lumbar spine in 61.8%, 19.6% and 18.0%, respectively. Patient characteristics and comorbidities in the two cohorts are displayed in Table 1. Patient selection flow chart. Characteristics and Comorbidities for All Patients, Surgical and Nonsurgical Cohorts.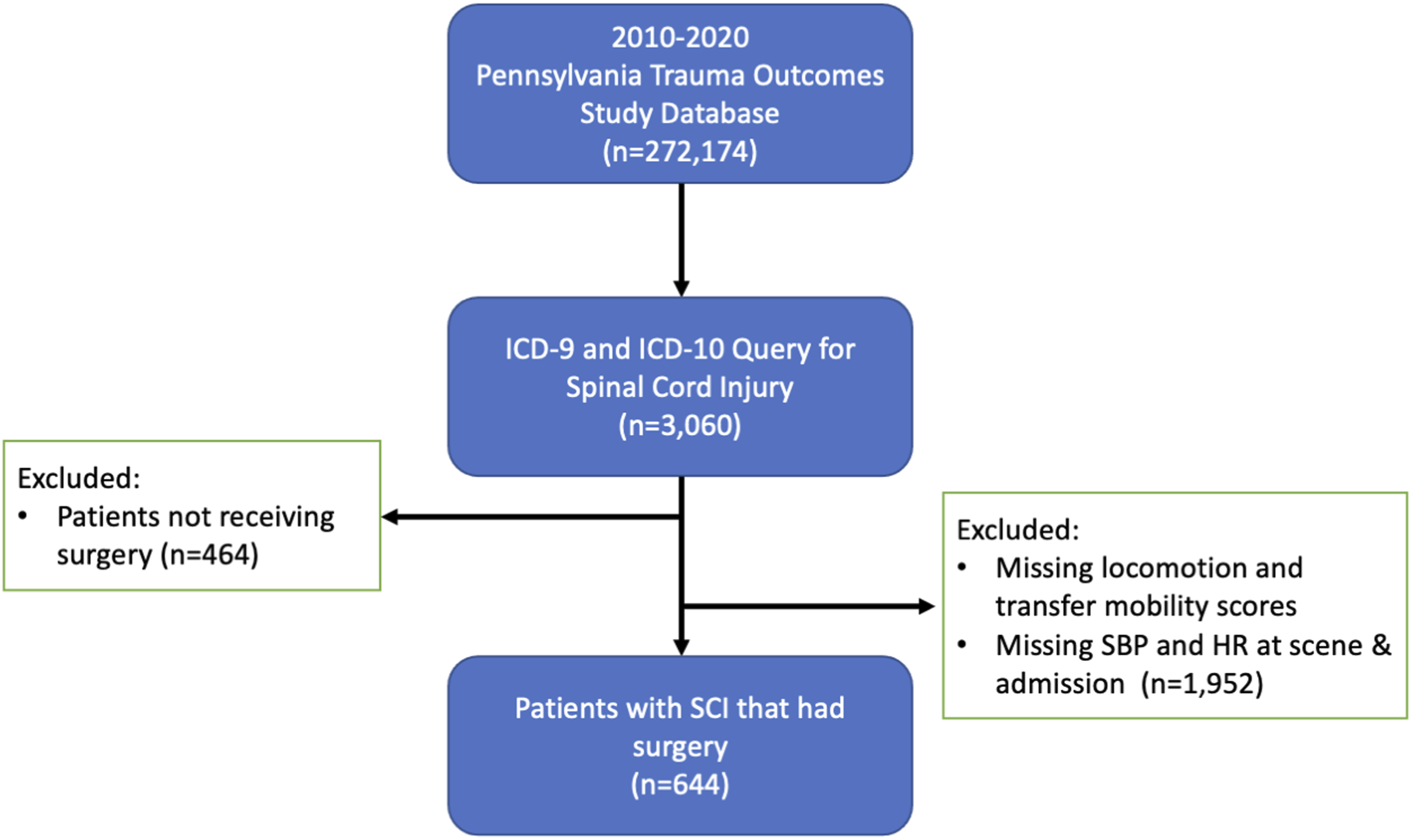
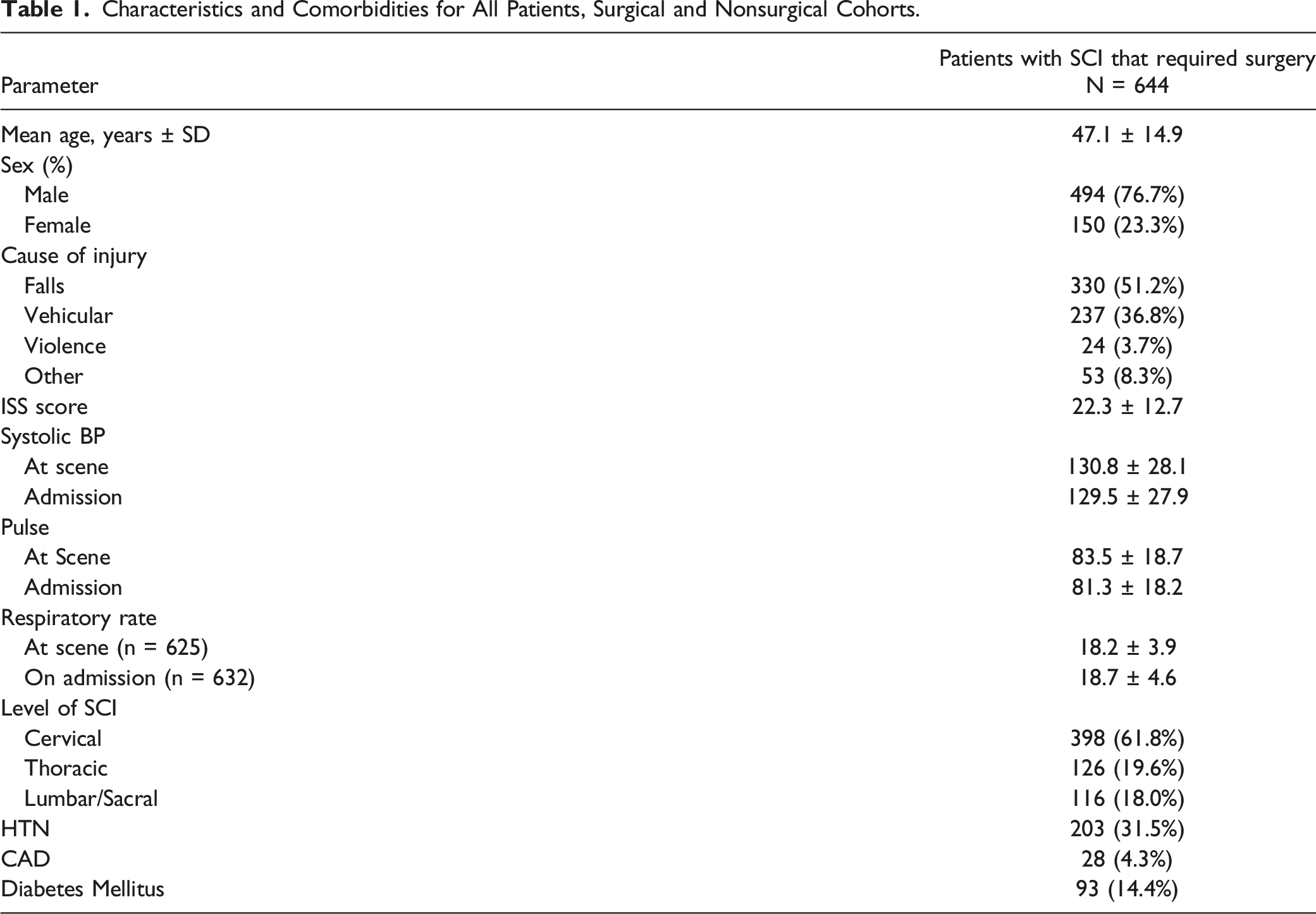
In the 644 patients that required surgery for their SCI, the mean systolic blood pressure was 130.8 ± 28.1 at the scene and 129.5 ± 27.9 on admission. The heart rate (HR) at the scene and on admission was 83.5 ± 18.7 and 81.3 ± 18.1 respectively. The respiratory rate (RR) at the scene was 18.3 ± 3.9 (n = 625) and 18.7 ± 4.6 (n = 632) on admission. The mean locomotion score at discharge was 2.1 ± 1.1. In terms of locomotion, 14.9% of patients were completely independent, 19.7% were independent with a device, 21.3% were partially dependent, and 44.1% were completely dependent. The mean transfer mobility score at discharge was 2.1 ± 1.1. In terms of transfer mobility, 15.7% were completely independent, 19.3% were independent with a device, 21.0% were partially dependent, and 44.1% completely dependent.
Impact of Blood Pressure and Heart Rate on Functional Outcomes
Characteristics and Comorbidities for Patients Based on Functional Outcome.
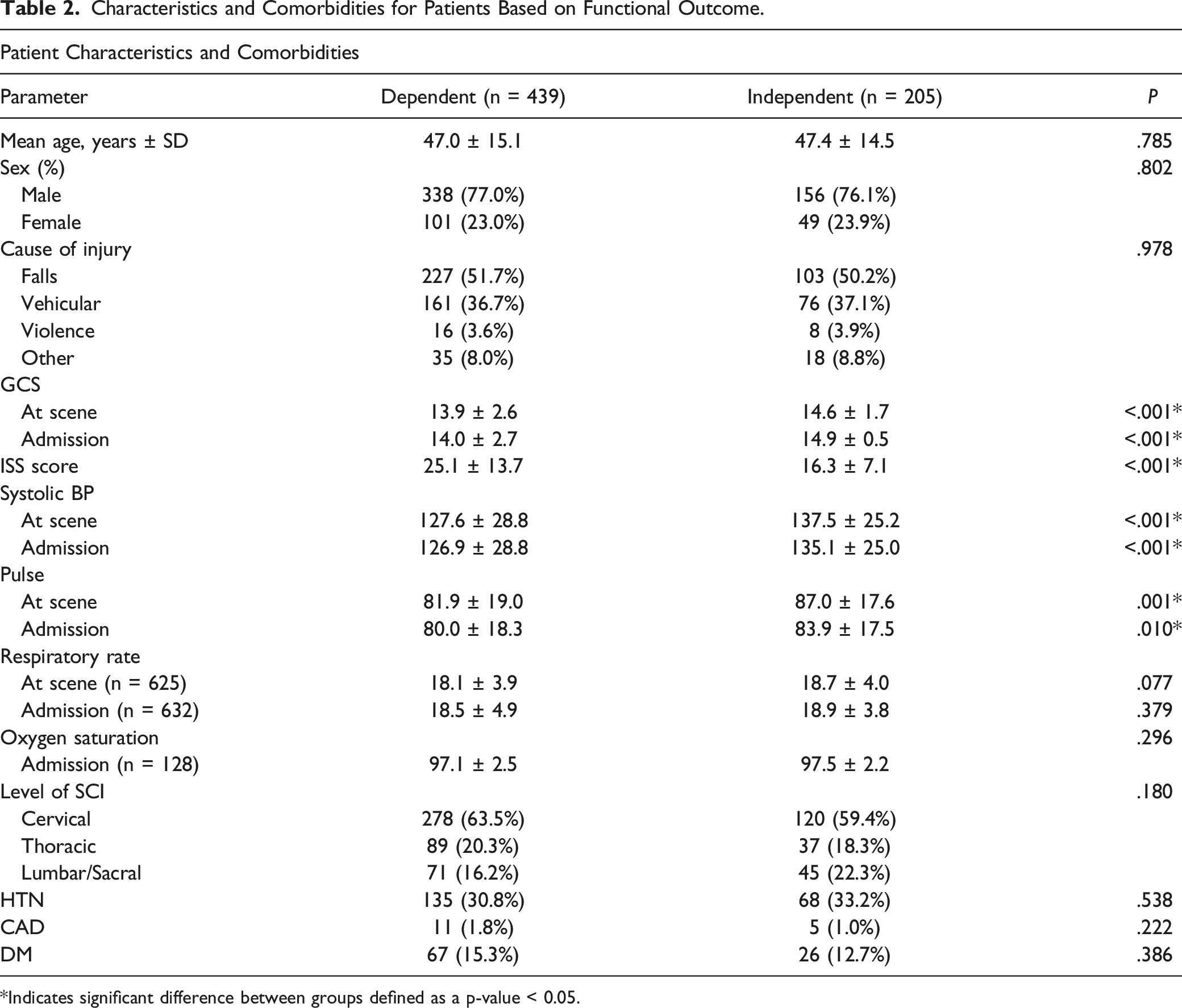
*Indicates significant difference between groups defined as a p-value < 0.05.
Level of neurological injury played a significant role on favorable locomotion and transfer mobility. Functional independence was seen in 30.2% of patients with cervical SCI (OR .681, 95% CI .443-1.047, P = .080), 29.4% in those with thoracic (OR .656, 95% CI .384-1.120, P = .123), and 38.8% of those with lumbar SCI (P = .180).
Multivariable Analysis of Predictors of Functional Independence at Discharge Based on Vitals at the Scene.
Multivariable Analysis of Predictors of Functional Independence at Discharge Based on Vitals on Admission.

Optimal Cutoff Heart Rate Values Predictive of Functional Independence
Peak Youden indices showed that the optimal cut-off values for HR at the scene and on admission above which patients with SCI were more likely to achieve functional independence are 69.5 beats per minute (BPM) (sensitivity of .883, specificity .268, max Youden index .151) and 82.5 BPM (sensitivity of .522, specificity .605, max Youden index .126), respectively (Figure 2). ROC curves for HR at scene (A) and on admission (B) predicting functional independence at discharge.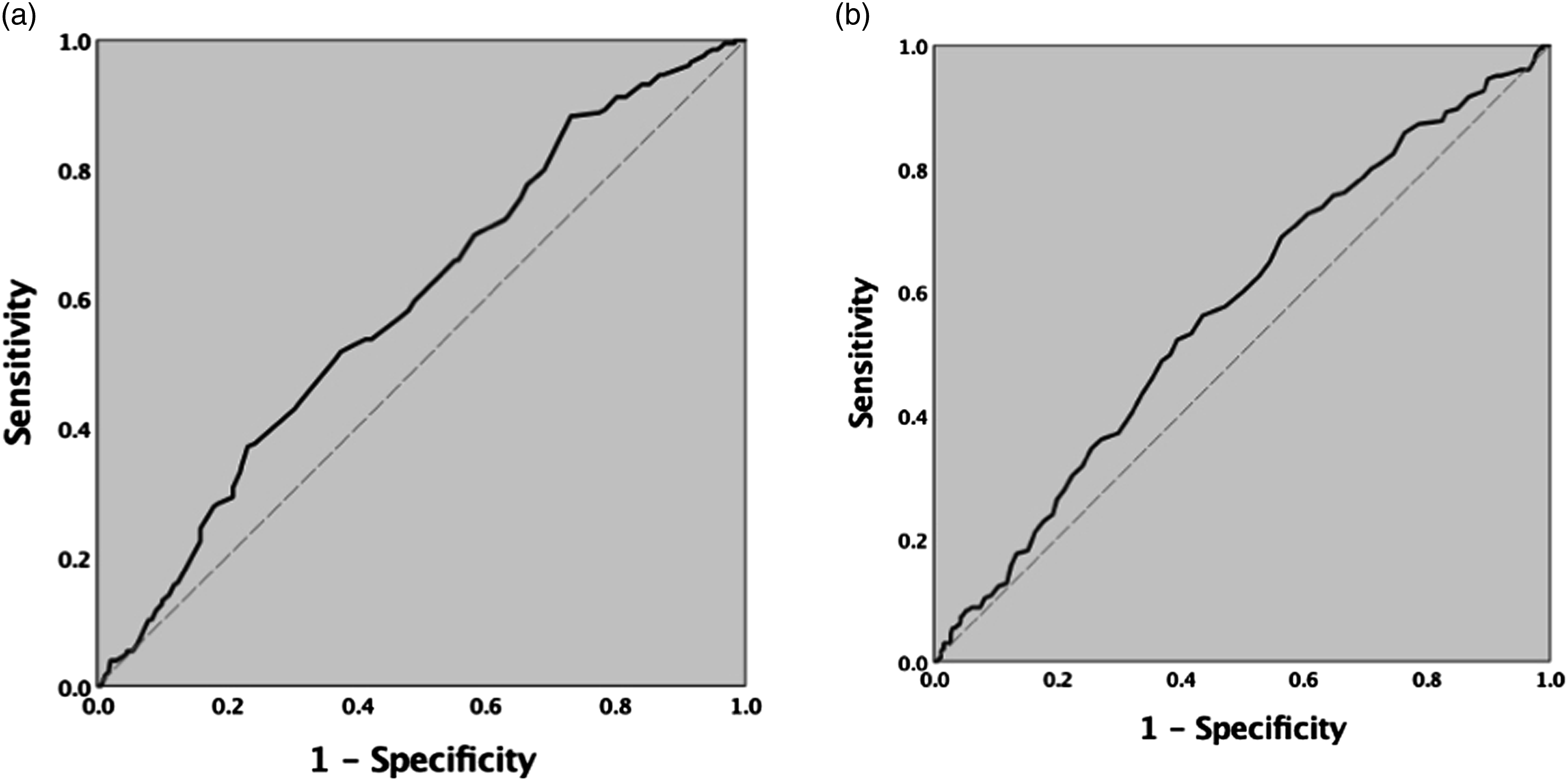
Discussion
While early resuscitation and BP management are essential in the management of acute spinal cord injury, there is not clear evidence on the predictive ability of initial blood pressure and heart rate on the functional outcomes in this patient population. Most studies to date have focused on the impact of the level and severity of neurological injury, operative and postoperative management on the functional outcomes. The aim of our study was to use a large patient registry from a mature trauma state to determine the relationship between early vital sign abnormalities and functional independence in hopes of laying the foundation for further studies on early SCI management as well as prognostication.
Our findings demonstrate a clear relationship between HR at the scene and on admission and functional independence as determined by the locomotion and transfer mobility grading among patients that required surgery. Initial systolic blood pressure was not correlated with functional independence. The Youden index analysis identified the HR at the scene of >70 and a HR of >83 on admission as the threshold values, above which patients are likely to achieve functional independence. As bradycardia is seen in patients with neurogenic shock, this cutoff value helps stratify the severity of neurogenic shock and correlate HR on presentation to functional outcomes at discharge. Furthermore, our study demonstrates that systolic blood pressure alone cannot be used to predict functional outcomes, likely due to the confounding effects of acute blood loss, early fluid resuscitation, and vasopressor infusion, however the exact relationship remains unclear. Given the complexity of acute SCI management, heart rate appears to be the vital sign with a more reliable predictive ability.
The existing literature shows equivocal evidence on the predictive ability of initial vital signs on functional independence. Despite the key role of BP management in recovery after SCI, Shea et al in 2021 studied 319 SCI patients and showed that initial emergency room blood pressure did not predict functional outcome. 25 This study was limited by the use of the single timepoint in the emergency room and suggested that prehospital vital signs closer to the onset of injury or the trajectory of physiologic parameters could be more predictive. Furthermore, persistent bradycardia has also been associated with severe SCI, while patients with mild SCI were less likely to exhibit bradycardia.26-28 The relationship between HR and functional independence at discharge shown in our study strengthens the current literature by not only corroborating the association of HR with SCI severity, but also demonstrating its predictivity of functional independence based on both HR at the scene and on admission. While our univariate analysis demonstrated a significant relationship between SBP and functional independence, significance was lost in our multivariable analysis after adjustment which is more in agreement with current literature such as Shea et al. 25
Our study entails limitations that need to be taken into consideration. As a retrospective large registry-based study, data on vasopressors and dosing to maintain the blood pressure were not available. Similarly, it is unknown whether patients were on beta-blocking medications prior to the SCI and their dosing. The preferential impact of any of these medications on HR and SBP is unclear. Further, it is unclear whether patients had surgery for decompression or stabilization of a traumatic fracture. The indication for surgery, timing, and exact surgical treatment were not provided in the PTSF database. This is a known limitation of large registry-based studies as we are unable to capture specific details regarding intervention. Additionally, patients were not analyzed based on need for surgery. We only assessed patients who underwent surgery which therefore excludes surgical influence on patient outcomes but is important to our study to reduce heterogeneity of subjects and improve generalizability to the neurosurgical patient. Including patients who did not require surgery adds complexity as it may select for patients who are either less severe injury and do not require intervention or are too impaired to require surgery. Therefore, ISS and level of SCI are used as surrogates to reflect patient presentation. Additionally, the PTOS registry uses the Functional Status at Discharge scale as evaluated by a physiatrist to assess functional outcomes as an equivalent to the Functional Independence Measure (FIM) scale. Blood pressure management would be very important in those with a compressive lesion, but less so in those with an unstable fracture alone. Despite these limitations, this study achieved our goal of identifying a relationship between bradycardia and functional status at discharge and lay the groundwork for further, well-powered studies to determine the optimal resuscitation strategy.
Conclusion
The presence of neurogenic shock drastically impacts functional outcomes in patients with spinal cord injury who require surgery. Our study demonstrates that bradycardia at the scene and on admission is a significant predictor of functional dependence in terms of locomotion and transfer mobility. HR ≥70 at the scene and HR ≥83 on admission were shown to be cutoff values above which patients are significantly more likely to achieve functional independence at discharge.
Footnotes
Author Contributions
NM, TL, and JJ designed the study. NM, TL were involved with data collection and analysis. NM, TL, CY, KH, DF, FA, ST, OK were involved with data collection, manuscript preparation, critical revision, and data interpretation. SP, JH, JSH, JJ were responsible for manuscript preparation, and critical revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
These data were provided by the Pennsylvania Trauma Systems Foundation, Mechanicsburg, PA. The foundation specifically disclaims responsibility for any analyses, interpretations, or conclusions.