COVID-19 resulted in the widespread shifting of hospital resources to handle surging COVID-19 cases resulting in the postponement of surgeries, including numerous spine procedures. This study aimed to quantify the impact that COVID-19 had on the number of treated spinal conditions and diagnoses during the pandemic.
Methods
Using CPT and ICD-10 codes, TriNetX, a national database, was utilized to quantify spine procedures and diagnoses in patients >18 years of age. The period of March 2020-May 2021 was compared to a reference pre-pandemic period of March 2018-May 2019. Each time period was then stratified into four seasons of the year, and the mean average number of procedures per healthcare organization was compared.
Results
In total, 524,394 patient encounters from 53 healthcare organizations were included in the analysis. There were significant decreases in spine procedures and diagnoses during March-May 2020 compared to pre-pandemic levels. Measurable differences were noted for spine procedures during the winter of 2020-2021, including a decrease in lumbar laminectomy and anterior cervical arthrodesis. Comparing the pandemic period to the pre-pandemic period showed significant reductions in most spine procedures and treated diagnoses; however, there was an increase in open repair of thoracic fractures during this period.
Conclusions
COVID-19 resulted in a widespread decrease in spinal diagnosis and treated conditions. An inverse relationship was observed between new COVID-19 cases and spine procedural volume. Recent increases in procedural volume from pre-pandemic levels are promising signs that the spine surgery community has narrowed the gap in unmet care produced by the pandemic.
The coronavirus disease 2019 (COVID-19) pandemic drastically affected the United States, directly impacting accessibility, quality, and delivery of medical services worldwide.1-3 After being declared a pandemic by the World Health Organization (WHO) in March of 2020,4 this global health crisis brought an unprecedented change to the field of spine surgery.5 While non-elective surgeries continued as needed with revised guidelines and protocols; elective surgeries were placed on hold with the intent of preserving medical resources and as part of efforts to reduce the spread of the virus during a period of high-volume hospital admissions.6,7 Specifically, in March of 2020, the American College of Surgeries (ACS) placed a guideline that recommended the discontinuation of elective, non-emergency procedures.8 Around the same time, the American Academy of Orthopaedic Surgeons (AAOS) released a four-tier system to classify conditions based on the priority for surgical intervention ranging from procedures that could be delayed without significant harm to the patient (Tier 1) to emergency surgeries (Tier 4).9 These recommendations allowed only essential orthopedic procedures to be performed, while other non-essential procedures were postponed.
Within the United States healthcare system, orthopedic and musculoskeletal surgery (MSK) accounts for approximately $65.6-71.1 billion in reimbursement and $15.6-$21.1 billion in annual net income.10 Moreover, orthopedic and MSK surgery accounts for a significant portion of hospital reimbursement compared to all hospital encounters.10 Therefore, given the substantial increase in spine surgery over the last 20 years11 it is critical to understand the degree to which spine surgery has been impacted during the pandemic. While current literature has focused mainly on perioperative and postoperative complications of patients during the COVID-19 pandemic12,13 little is known about the impact that the COVID-19 pandemic has had on the incidence of common spine procedures. Consequently, this study aimed to quantify the pandemic’s impact on the most common elective and non-elective spine procedures and diagnoses during the peak of COVID-19. With our current understanding of the complications that arise from delaying spine procedures,14 gaining insight into this area could serve as a foundation to understand the role the COVID-19 pandemic had on spine surgery and patient outcomes.
Methods
This is a retrospective analysis conducted using adult patient data (ages ≥18 years) from March 2018 to May 2021 using the TriNetX Research Network. TriNetX is a global federated private database consisting of electronic health records from 53 healthcare organizations (HCOs) and comprises over 68 million unique patient records. TriNetX contains real-time, de-identified, aggregate patient records, including but not limited to demographics, genomics, medications, procedures, and vitals. Given the de-identified nature of the information in the TrinetX database, ethical approval from the institutional review board (IRB) was not required. Most participating HCO’s provide patient records dating back to the last seven years, however the identity of the HCOs subscribed to the network is not provided. However, most patient information comes from academic medical centers and their affiliates. Importantly, TriNetX has been previously validated and utilized in published studies across multiple subspecialties.15-19
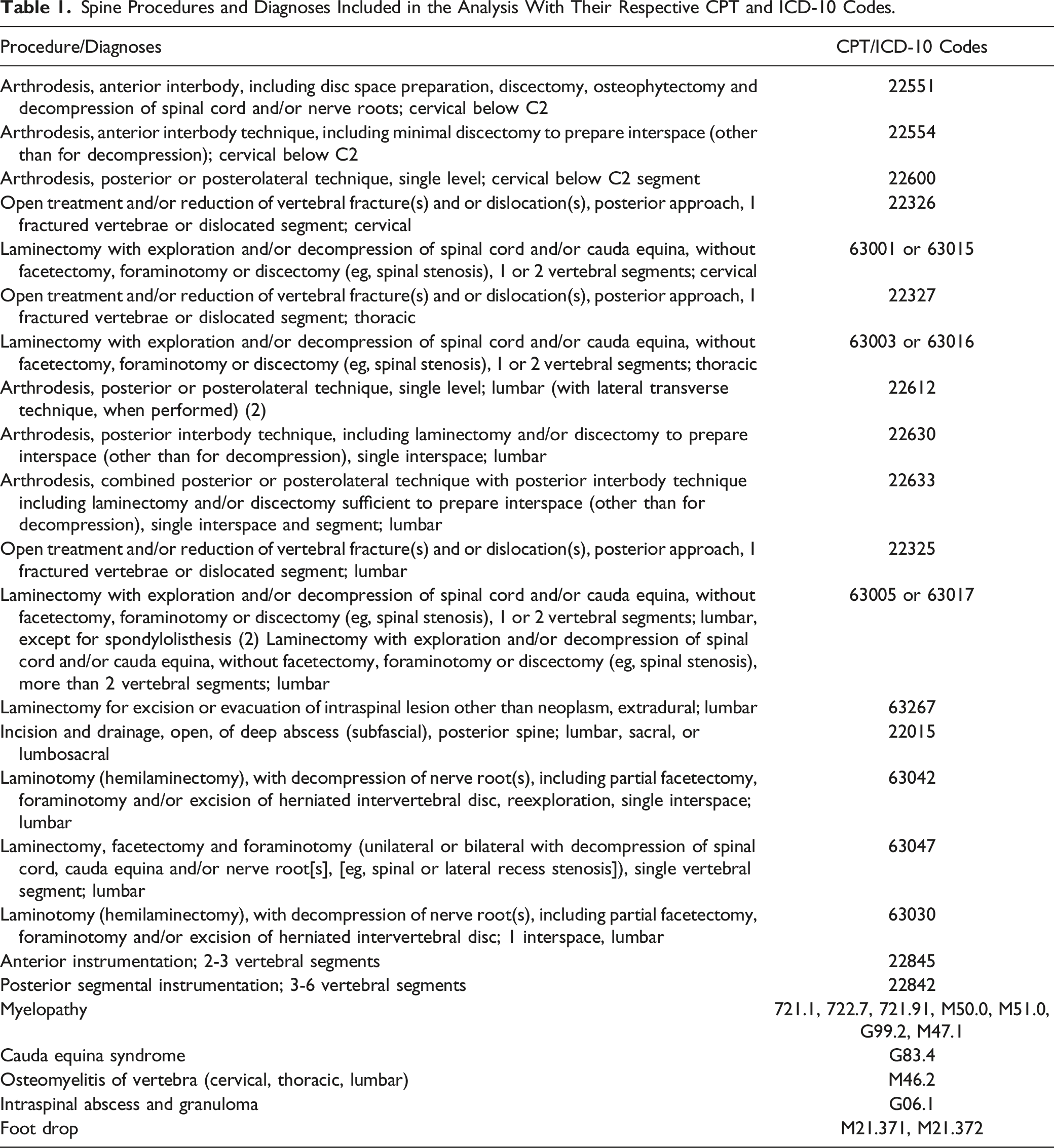
Using Current Procedural and Terminology codes (CPT) and International Classification of Disease 10 (ICD-10) codes (Table 1), TriNetX was queried for the most common spine procedures and diagnoses. In addition to input from the primary investigators, a literature search was conducted to obtain the aforementioned list of CPT and ICD-10 codes representing the most widely performed procedures and treated diagnoses.20-24 The data was then aggregated based on seasonal averages and compared to national monthly averages before the pandemic during the corresponding months of 2018-2020 to provide a baseline of pre-pandemic volume. The average number of procedures per HCO encounter was computed to account for procedure-specific changes in the number of reporting HCOs.
Spine Procedures and Diagnoses Included in the Analysis With Their Respective CPT and ICD-10 Codes.
Procedure/Diagnoses
CPT/ICD-10 Codes
Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy and decompression of spinal cord and/or nerve roots; cervical below C2
22551
Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); cervical below C2
22554
Arthrodesis, posterior or posterolateral technique, single level; cervical below C2 segment
22600
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; cervical
22326
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; cervical
63001 or 63015
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; thoracic
22327
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; thoracic
63003 or 63016
Arthrodesis, posterior or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) (2)
22612
Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar
22630
Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar
22633
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; lumbar
22325
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis (2) Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), more than 2 vertebral segments; lumbar
63005 or 63017
Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; lumbar
63267
Incision and drainage, open, of deep abscess (subfascial), posterior spine; lumbar, sacral, or lumbosacral
22015
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; lumbar
63042
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [eg, spinal or lateral recess stenosis]), single vertebral segment; lumbar
63047
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar
Osteomyelitis of vertebra (cervical, thoracic, lumbar)
M46.2
Intraspinal abscess and granuloma
G06.1
Foot drop
M21.371, M21.372
The seasons of the pandemic period included in the study were subsequently stratified as spring 2020 (March-May 2020), summer 2020 (June-August 2020), fall 2020 (September-November 2020), winter 2020 (December 2020-February 2021), and spring 2021 (March-May 2021). Additionally, the entire pandemic period included in the analysis (March 2020-May 2021) was compared to the corresponding months between March 2018 and February 2020. Descriptive analysis was performed, and comparisons were conducted utilizing a student’s t-test. All statistical analyses were performed using Microsoft Excel (Microsoft Inc, Washington, USA). Statistical significance was set at P < .05.
Results
In total, 524,394 patient encounters from 53 healthcare organizations between March 2018 - May 2021 were included in the analysis. Myelopathy, foot drop, and osteomyelitis of vertebra had the highest seasonal mean procedural/diagnosis volumes per HCO during the pre-pandemic and pandemic periods for all four seasons. There was a general decrease in the mean number of procedures/diagnoses over the spring of 2020, with 13 significant reductions and only one increase. The spring of 2021 had five significant increases and one reduction in laminotomy with decompression of nerve roots.
Spring 2020
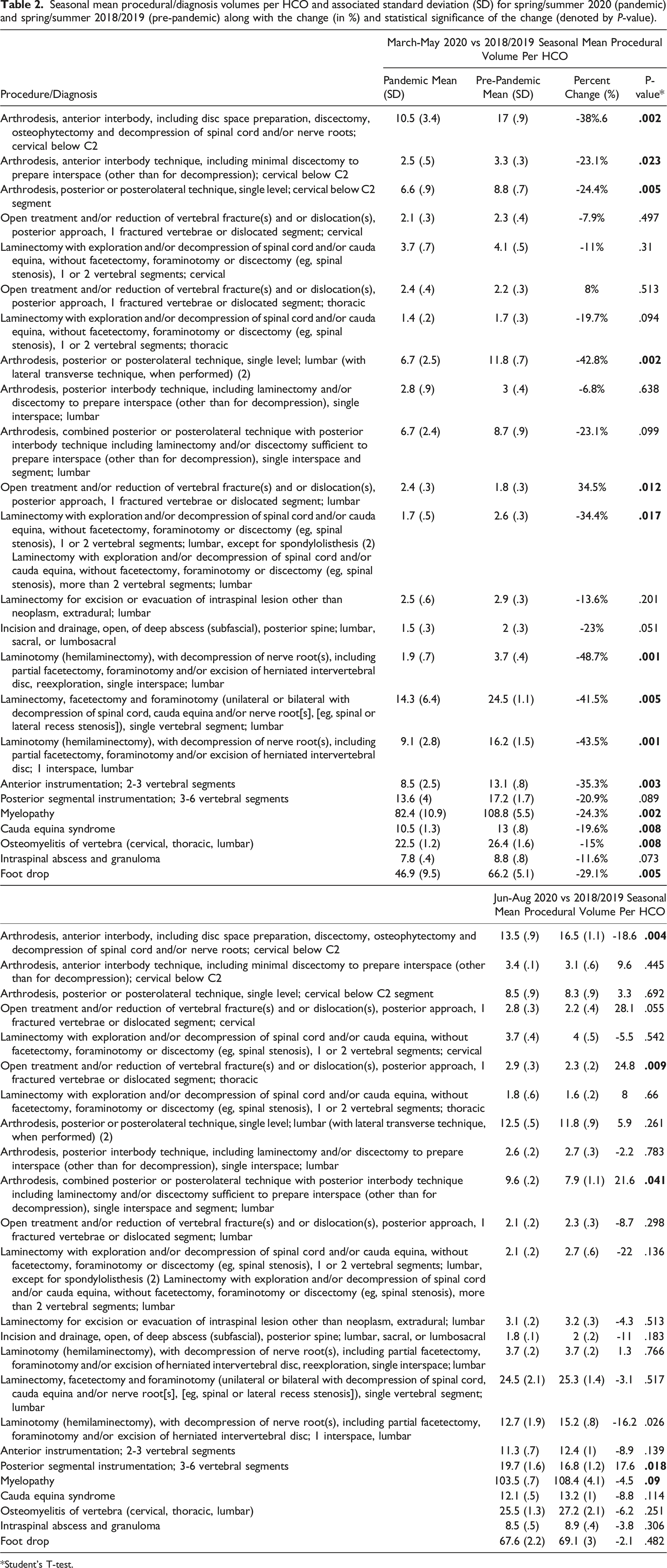
When compared to the pre-pandemic period, the spring of 2020 (March-May 2020) showed significant decreases in the following procedures: cervical arthrodesis anterior interbody technique with decompression (10.5 vs 17; P < .002), cervical arthrodesis anterior interbody technique without decompression (2.5 vs 3.3; P < .023), cervical arthrodesis posterior technique (6.6 vs 8.8; P < .005), lumbar arthrodesis posterior technique (6.7 vs 11.8; P < .002), lumbar laminectomy with exploration/decompression without facetectomy/foraminotomy/discectomy (1.7 vs 2.6; P < .017) and lumbar laminectomy with exploration/decompression with facetectomy/foraminotomy/discectomy (14.3 vs 24.5; P < .005), lumbar decompression laminotomy (9.1 vs 16.2; P = .001), lumbar decompression laminotomy re-exploration (1.9 vs 3.7; P < .001), and anterior lumbar instrumentation procedures (8.5 vs 13.1; P < .003) while lumbar open treatment of vertebral fracture/dislocation saw a significant increase (2.4 vs 1.8; P < .012). Additionally, when compared to the pre-pandemic period, diagnoses from March-May 2020 showed a significant decrease in the treatment of the following conditions: myelopathy (82.4 vs 108.8; P < .002), cauda equina syndrome (10.5 vs 13; P = .008), spinal osteomyelitis (22.5 vs 26.4; P < .008) and foot drop (46.9 vs 66.2; P < .005). (Table 2)
Seasonal mean procedural/diagnosis volumes per HCO and associated standard deviation (SD) for spring/summer 2020 (pandemic) and spring/summer 2018/2019 (pre-pandemic) along with the change (in %) and statistical significance of the change (denoted by P-value).
Procedure/Diagnosis
March-May 2020 vs 2018/2019 Seasonal Mean Procedural Volume Per HCO
Pandemic Mean (SD)
Pre-Pandemic Mean (SD)
Percent Change (%)
P-value*
Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy and decompression of spinal cord and/or nerve roots; cervical below C2
10.5 (3.4)
17 (.9)
-38%.6
.002
Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); cervical below C2
2.5 (.5)
3.3 (.3)
-23.1%
.023
Arthrodesis, posterior or posterolateral technique, single level; cervical below C2 segment
6.6 (.9)
8.8 (.7)
-24.4%
.005
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; cervical
2.1 (.3)
2.3 (.4)
-7.9%
.497
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; cervical
3.7 (.7)
4.1 (.5)
-11%
.31
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; thoracic
2.4 (.4)
2.2 (.3)
8%
.513
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; thoracic
1.4 (.2)
1.7 (.3)
-19.7%
.094
Arthrodesis, posterior or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) (2)
6.7 (2.5)
11.8 (.7)
-42.8%
.002
Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar
2.8 (.9)
3 (.4)
-6.8%
.638
Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar
6.7 (2.4)
8.7 (.9)
-23.1%
.099
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; lumbar
2.4 (.3)
1.8 (.3)
34.5%
.012
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis (2) Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), more than 2 vertebral segments; lumbar
1.7 (.5)
2.6 (.3)
-34.4%
.017
Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; lumbar
2.5 (.6)
2.9 (.3)
-13.6%
.201
Incision and drainage, open, of deep abscess (subfascial), posterior spine; lumbar, sacral, or lumbosacral
1.5 (.3)
2 (.3)
-23%
.051
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; lumbar
1.9 (.7)
3.7 (.4)
-48.7%
.001
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [eg, spinal or lateral recess stenosis]), single vertebral segment; lumbar
14.3 (6.4)
24.5 (1.1)
-41.5%
.005
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar
Osteomyelitis of vertebra (cervical, thoracic, lumbar)
22.5 (1.2)
26.4 (1.6)
-15%
.008
Intraspinal abscess and granuloma
7.8 (.4)
8.8 (.8)
-11.6%
.073
Foot drop
46.9 (9.5)
66.2 (5.1)
-29.1%
.005
Jun-Aug 2020 vs 2018/2019 Seasonal Mean Procedural Volume Per HCO
Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy and decompression of spinal cord and/or nerve roots; cervical below C2
13.5 (.9)
16.5 (1.1)
-18.6
.004
Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); cervical below C2
3.4 (.1)
3.1 (.6)
9.6
.445
Arthrodesis, posterior or posterolateral technique, single level; cervical below C2 segment
8.5 (.9)
8.3 (.9)
3.3
.692
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; cervical
2.8 (.3)
2.2 (.4)
28.1
.055
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; cervical
3.7 (.4)
4 (.5)
-5.5
.542
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; thoracic
2.9 (.3)
2.3 (.2)
24.8
.009
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; thoracic
1.8 (.6)
1.6 (.2)
8
.66
Arthrodesis, posterior or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) (2)
12.5 (.5)
11.8 (.9)
5.9
.261
Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar
2.6 (.2)
2.7 (.3)
-2.2
.783
Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar
9.6 (.2)
7.9 (1.1)
21.6
.041
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; lumbar
2.1 (.2)
2.3 (.3)
-8.7
.298
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis (2) Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), more than 2 vertebral segments; lumbar
2.1 (.2)
2.7 (.6)
-22
.136
Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; lumbar
3.1 (.2)
3.2 (.3)
-4.3
.513
Incision and drainage, open, of deep abscess (subfascial), posterior spine; lumbar, sacral, or lumbosacral
1.8 (.1)
2 (.2)
-11
.183
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; lumbar
3.7 (.2)
3.7 (.2)
1.3
.766
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [eg, spinal or lateral recess stenosis]), single vertebral segment; lumbar
24.5 (2.1)
25.3 (1.4)
-3.1
.517
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar
Osteomyelitis of vertebra (cervical, thoracic, lumbar)
25.5 (1.3)
27.2 (2.1)
-6.2
.251
Intraspinal abscess and granuloma
8.5 (.5)
8.9 (.4)
-3.8
.306
Foot drop
67.6 (2.2)
69.1 (3)
-2.1
.482
*Student’s T-test.
Summer 2020/Fall 2020
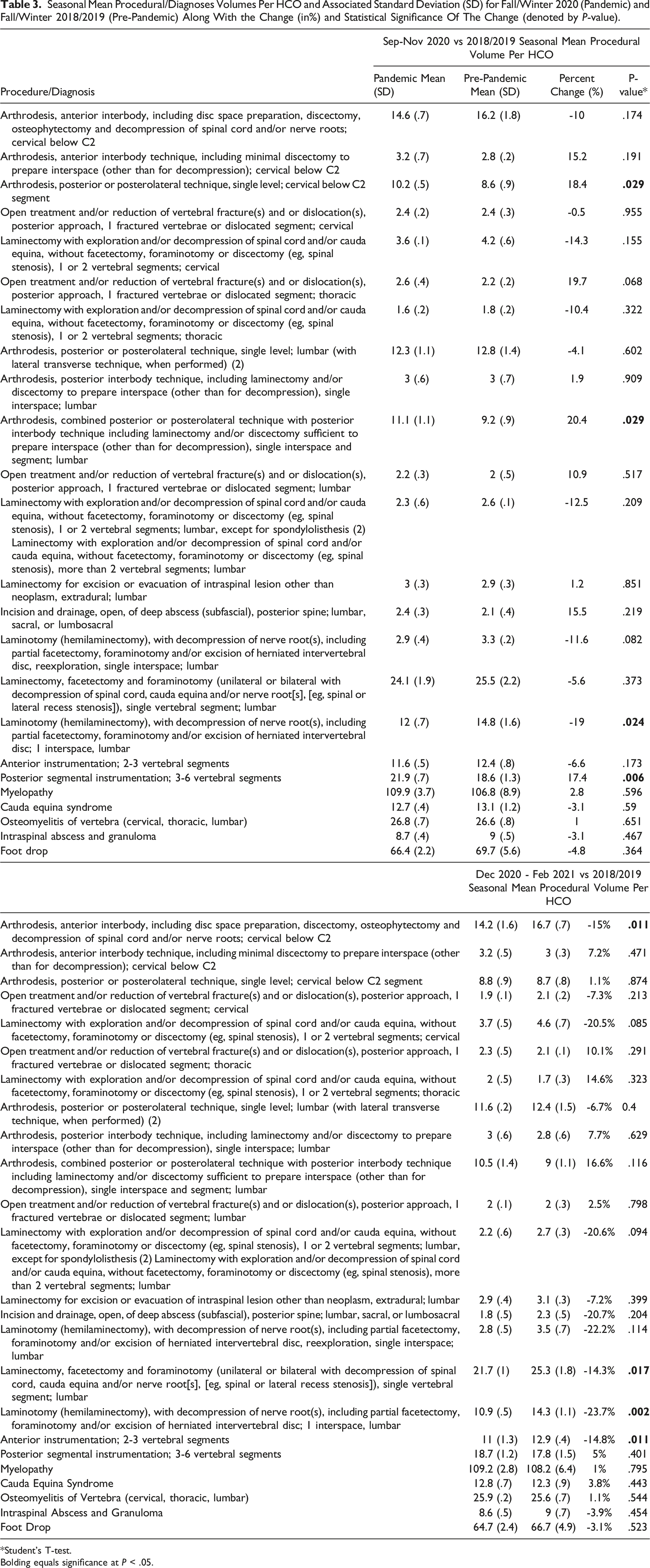
Several procedures (6/24) saw a statistically significant decrease in volume during the summer of 2020 (Table 2). Similarly, several procedures (4/24) in the fall of 2020 observed statistically significant reductions. On a procedure-specific level, multiple procedures (7/24) during the fall of 2020 increased in volume compared to the summer months. However, the majority maintained the declining trend in line with the preceding summer months. (Table 3)
Seasonal Mean Procedural/Diagnoses Volumes Per HCO and Associated Standard Deviation (SD) for Fall/Winter 2020 (Pandemic) and Fall/Winter 2018/2019 (Pre-Pandemic) Along With the Change (in%) and Statistical Significance Of The Change (denoted by P-value).
Procedure/Diagnosis
Sep-Nov 2020 vs 2018/2019 Seasonal Mean Procedural Volume Per HCO
Pandemic Mean (SD)
Pre-Pandemic Mean (SD)
Percent Change (%)
P-value*
Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy and decompression of spinal cord and/or nerve roots; cervical below C2
14.6 (.7)
16.2 (1.8)
-10
.174
Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); cervical below C2
3.2 (.7)
2.8 (.2)
15.2
.191
Arthrodesis, posterior or posterolateral technique, single level; cervical below C2 segment
10.2 (.5)
8.6 (.9)
18.4
.029
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; cervical
2.4 (.2)
2.4 (.3)
-0.5
.955
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; cervical
3.6 (.1)
4.2 (.6)
-14.3
.155
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; thoracic
2.6 (.4)
2.2 (.2)
19.7
.068
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; thoracic
1.6 (.2)
1.8 (.2)
-10.4
.322
Arthrodesis, posterior or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) (2)
12.3 (1.1)
12.8 (1.4)
-4.1
.602
Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar
3 (.6)
3 (.7)
1.9
.909
Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar
11.1 (1.1)
9.2 (.9)
20.4
.029
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; lumbar
2.2 (.3)
2 (.5)
10.9
.517
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis (2) Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), more than 2 vertebral segments; lumbar
2.3 (.6)
2.6 (.1)
-12.5
.209
Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; lumbar
3 (.3)
2.9 (.3)
1.2
.851
Incision and drainage, open, of deep abscess (subfascial), posterior spine; lumbar, sacral, or lumbosacral
2.4 (.3)
2.1 (.4)
15.5
.219
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; lumbar
2.9 (.4)
3.3 (.2)
-11.6
.082
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [eg, spinal or lateral recess stenosis]), single vertebral segment; lumbar
24.1 (1.9)
25.5 (2.2)
-5.6
.373
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar
Osteomyelitis of vertebra (cervical, thoracic, lumbar)
26.8 (.7)
26.6 (.8)
1
.651
Intraspinal abscess and granuloma
8.7 (.4)
9 (.5)
-3.1
.467
Foot drop
66.4 (2.2)
69.7 (5.6)
-4.8
.364
Dec 2020 - Feb 2021 vs 2018/2019 Seasonal Mean Procedural Volume Per HCO
Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy and decompression of spinal cord and/or nerve roots; cervical below C2
14.2 (1.6)
16.7 (.7)
-15%
.011
Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); cervical below C2
3.2 (.5)
3 (.3)
7.2%
.471
Arthrodesis, posterior or posterolateral technique, single level; cervical below C2 segment
8.8 (.9)
8.7 (.8)
1.1%
.874
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; cervical
1.9 (.1)
2.1 (.2)
-7.3%
.213
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; cervical
3.7 (.5)
4.6 (.7)
-20.5%
.085
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; thoracic
2.3 (.5)
2.1 (.1)
10.1%
.291
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; thoracic
2 (.5)
1.7 (.3)
14.6%
.323
Arthrodesis, posterior or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) (2)
11.6 (.2)
12.4 (1.5)
-6.7%
0.4
Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar
3 (.6)
2.8 (.6)
7.7%
.629
Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar
10.5 (1.4)
9 (1.1)
16.6%
.116
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; lumbar
2 (.1)
2 (.3)
2.5%
.798
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis (2) Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), more than 2 vertebral segments; lumbar
2.2 (.6)
2.7 (.3)
-20.6%
.094
Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; lumbar
2.9 (.4)
3.1 (.3)
-7.2%
.399
Incision and drainage, open, of deep abscess (subfascial), posterior spine; lumbar, sacral, or lumbosacral
1.8 (.5)
2.3 (.5)
-20.7%
.204
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; lumbar
2.8 (.5)
3.5 (.7)
-22.2%
.114
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [eg, spinal or lateral recess stenosis]), single vertebral segment; lumbar
21.7 (1)
25.3 (1.8)
-14.3%
.017
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar
Osteomyelitis of Vertebra (cervical, thoracic, lumbar)
25.9 (.2)
25.6 (.7)
1.1%
.544
Intraspinal Abscess and Granuloma
8.6 (.5)
9 (.7)
-3.9%
.454
Foot Drop
64.7 (2.4)
66.7 (4.9)
-3.1%
.523
*Student’s T-test.
Bolding equals significance at P < .05.
Winter 2020-2021
December 2020-February 2021 saw a significant decrease in cervical arthrodesis anterior interbody technique with decompression (14.2 vs 16.7; P < .011), lumbar laminectomy decompression with facetectomy/foraminotomy/discectomy (21.7 vs 25.3; P < .017), lumbar laminotomy with decompression (10.9 vs 14.3; P < .002), and anterior instrumentation (11 vs 12.9; P < .011) when compared to the pre-pandemic period(Table 3).
Spring 2021
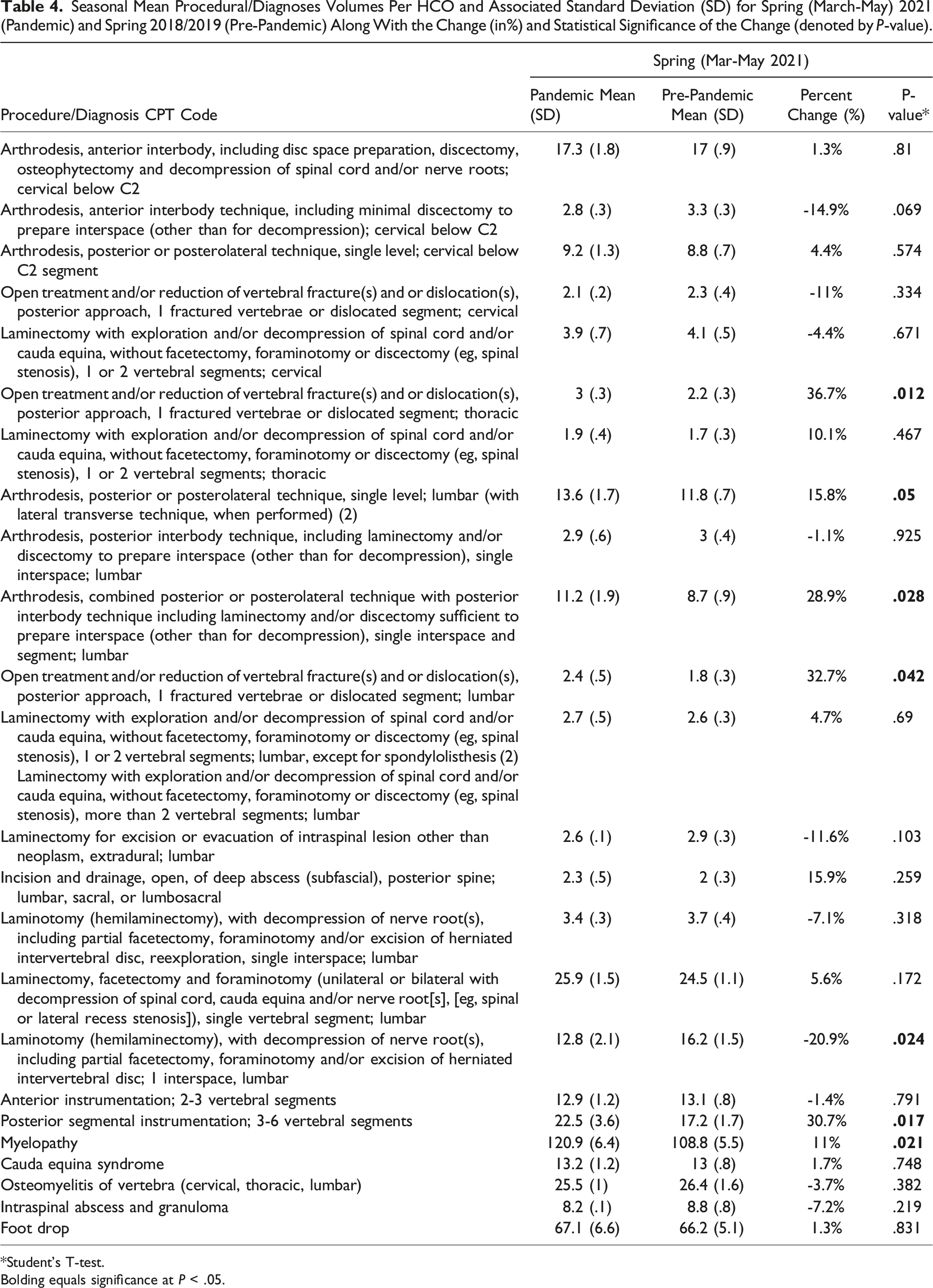
On the other hand, the spring of 2021 (March-May 2021) saw significant increases in thoracic open treatment/reduction of fracture/dislocation (3 vs 2.2; P < .012), lumbar arthrodesis posterior technique single level (13.6 vs 11.8; P < .05), lumbar arthrodesis posterolateral technique including laminectomy and discectomy (11.2 vs 8.7; P < .028), lumbar open treatment/reduction of fracture/dislocation (2.4 vs 1.8; P < .042), posterior segmental instrumentation (22.5 vs 17.2; P < .017), and in myelopathy diagnosis (120.9 vs 108.8; P < .021) while lumbar laminotomy with decompression and partial facetectomy/foraminotomy/excision of herniated disc saw a significant decrease during the same spring of 2021 period (12.8 vs 16.2; P < .024). (Table 4)
Seasonal Mean Procedural/Diagnoses Volumes Per HCO and Associated Standard Deviation (SD) for Spring (March-May) 2021 (Pandemic) and Spring 2018/2019 (Pre-Pandemic) Along With the Change (in%) and Statistical Significance of the Change (denoted by P-value).
Procedure/Diagnosis CPT Code
Spring (Mar-May 2021)
Pandemic Mean (SD)
Pre-Pandemic Mean (SD)
Percent Change (%)
P-value*
Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy and decompression of spinal cord and/or nerve roots; cervical below C2
17.3 (1.8)
17 (.9)
1.3%
.81
Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); cervical below C2
2.8 (.3)
3.3 (.3)
-14.9%
.069
Arthrodesis, posterior or posterolateral technique, single level; cervical below C2 segment
9.2 (1.3)
8.8 (.7)
4.4%
.574
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; cervical
2.1 (.2)
2.3 (.4)
-11%
.334
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; cervical
3.9 (.7)
4.1 (.5)
-4.4%
.671
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; thoracic
3 (.3)
2.2 (.3)
36.7%
.012
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; thoracic
1.9 (.4)
1.7 (.3)
10.1%
.467
Arthrodesis, posterior or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) (2)
13.6 (1.7)
11.8 (.7)
15.8%
.05
Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar
2.9 (.6)
3 (.4)
-1.1%
.925
Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar
11.2 (1.9)
8.7 (.9)
28.9%
.028
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; lumbar
2.4 (.5)
1.8 (.3)
32.7%
.042
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis (2) Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), more than 2 vertebral segments; lumbar
2.7 (.5)
2.6 (.3)
4.7%
.69
Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; lumbar
2.6 (.1)
2.9 (.3)
-11.6%
.103
Incision and drainage, open, of deep abscess (subfascial), posterior spine; lumbar, sacral, or lumbosacral
2.3 (.5)
2 (.3)
15.9%
.259
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; lumbar
3.4 (.3)
3.7 (.4)
-7.1%
.318
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [eg, spinal or lateral recess stenosis]), single vertebral segment; lumbar
25.9 (1.5)
24.5 (1.1)
5.6%
.172
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar
Osteomyelitis of vertebra (cervical, thoracic, lumbar)
25.5 (1)
26.4 (1.6)
-3.7%
.382
Intraspinal abscess and granuloma
8.2 (.1)
8.8 (.8)
-7.2%
.219
Foot drop
67.1 (6.6)
66.2 (5.1)
1.3%
.831
*Student’s T-test.
Bolding equals significance at P < .05.
Aggregate Pandemic Period vs Pre-pandemic Period
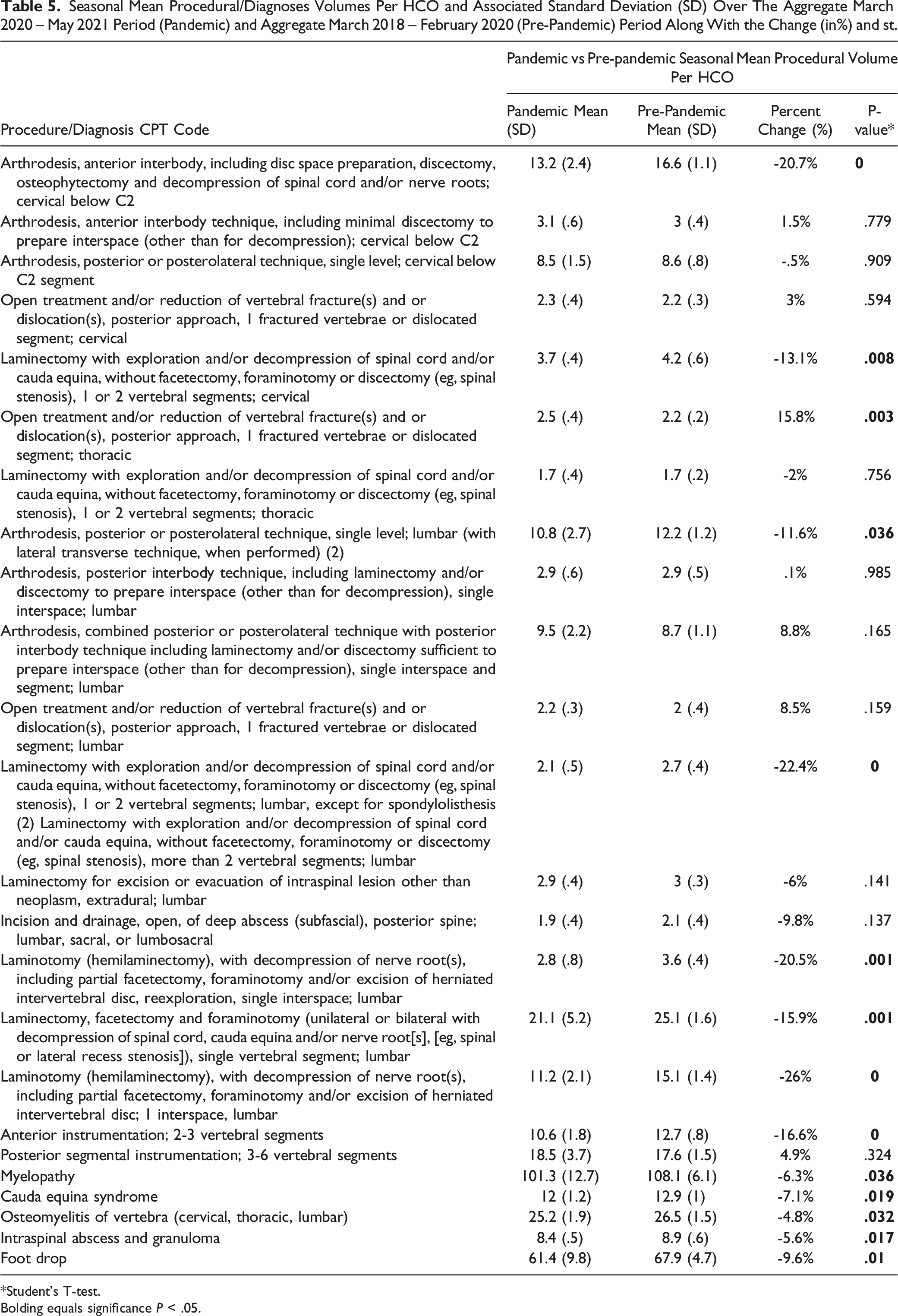
Comparing the entire pandemic period (March 2020-May 2021) assessed to the pre-pandemic (March 2018-February 2020) period, there was a significant decrease in spine procedures such as cervical arthrodesis anterior interbody (13.2 vs 16.6; P < .001), cervical laminectomy (3.7 vs 4.2; P < .008), lumbar arthrodesis posterior/posterolateral approach (10.8 vs 12.2; P < .036), lumbar laminectomy with decompression without facetectomy, foraminotomy or discectomy (2.1 vs 2.7; P < .001), decompression lumbar laminotomy (11.2 vs 15.1; P < .001), decompression lumbar laminotomy re-exploration (2.8 vs 3.6; P < .001), lumbar laminectomy with decompression single vertebral segment (21.1 vs 25.1; P < .001), and anterior lumbar instrumentation (10.6 vs 12.7; P < .001). Additionally, there was a significant decrease in the incidence of diagnoses such as myelopathy (101.3 vs 108.1; P < .036), cauda equina syndrome (12 vs 12.9; P < .019), osteomyelitis (25.2 vs 26.5; P < .032), intraspinal abscess and granuloma (8.4 vs 8.9; P < .017), and foot drop (61.4 vs 67.9; P < .01) during the pandemic when compared to pre-pandemic. A significant increase in incidence was only seen in thoracic open treatment/reduction of vertebral fracture/dislocation (2.5 vs 2.2; P < .003) during the pandemic period compared to pre-pandemic. (Table 5)
Seasonal Mean Procedural/Diagnoses Volumes Per HCO and Associated Standard Deviation (SD) Over The Aggregate March 2020 – May 2021 Period (Pandemic) and Aggregate March 2018 – February 2020 (Pre-Pandemic) Period Along With the Change (in%) and st.
Procedure/Diagnosis CPT Code
Pandemic vs Pre-pandemic Seasonal Mean Procedural Volume Per HCO
Pandemic Mean (SD)
Pre-Pandemic Mean (SD)
Percent Change (%)
P-value*
Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy and decompression of spinal cord and/or nerve roots; cervical below C2
13.2 (2.4)
16.6 (1.1)
-20.7%
0
Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); cervical below C2
3.1 (.6)
3 (.4)
1.5%
.779
Arthrodesis, posterior or posterolateral technique, single level; cervical below C2 segment
8.5 (1.5)
8.6 (.8)
-.5%
.909
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; cervical
2.3 (.4)
2.2 (.3)
3%
.594
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; cervical
3.7 (.4)
4.2 (.6)
-13.1%
.008
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; thoracic
2.5 (.4)
2.2 (.2)
15.8%
.003
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; thoracic
1.7 (.4)
1.7 (.2)
-2%
.756
Arthrodesis, posterior or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) (2)
10.8 (2.7)
12.2 (1.2)
-11.6%
.036
Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar
2.9 (.6)
2.9 (.5)
.1%
.985
Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar
9.5 (2.2)
8.7 (1.1)
8.8%
.165
Open treatment and/or reduction of vertebral fracture(s) and or dislocation(s), posterior approach, 1 fractured vertebrae or dislocated segment; lumbar
2.2 (.3)
2 (.4)
8.5%
.159
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis (2) Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), more than 2 vertebral segments; lumbar
2.1 (.5)
2.7 (.4)
-22.4%
0
Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; lumbar
2.9 (.4)
3 (.3)
-6%
.141
Incision and drainage, open, of deep abscess (subfascial), posterior spine; lumbar, sacral, or lumbosacral
1.9 (.4)
2.1 (.4)
-9.8%
.137
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; lumbar
2.8 (.8)
3.6 (.4)
-20.5%
.001
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [eg, spinal or lateral recess stenosis]), single vertebral segment; lumbar
21.1 (5.2)
25.1 (1.6)
-15.9%
.001
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar
Osteomyelitis of vertebra (cervical, thoracic, lumbar)
25.2 (1.9)
26.5 (1.5)
-4.8%
.032
Intraspinal abscess and granuloma
8.4 (.5)
8.9 (.6)
-5.6%
.017
Foot drop
61.4 (9.8)
67.9 (4.7)
-9.6%
.01
*Student’s T-test.
Bolding equals significance P < .05.
Total Procedural Volume vs New COVID-19 Cases
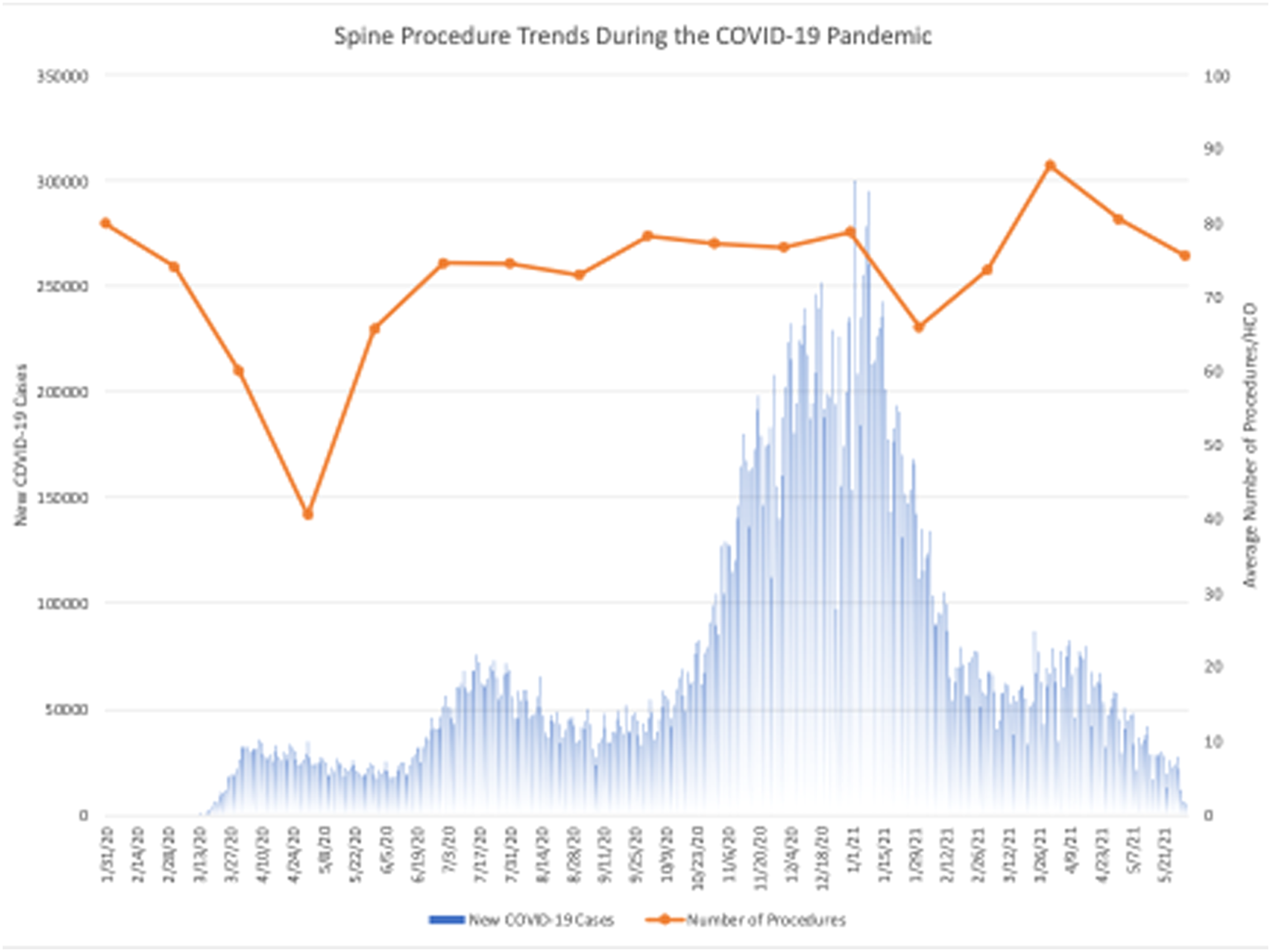
Figure 1 displays the monthly total number of spine procedures per HCO over time overlayed onto a temporal bar graph of new COVID cases, demonstrating the association between each wave of the pandemic and the incidence of spine procedures. The most significant number of COVID-19 cases and the largest reduction in the number of spine procedures occurred during spring of 2020, followed by a subsequent rebound in the number of cases during the early summer of 2020. The largest spike in COVID-19 cases was seen during the fall and winter of 2020 into the beginning of 2021, accompanied by a gradual reduction in spine procedures. As COVID-19 case numbers began to drop in the spring of 2021, a rebound in spine procedures to the highest number performed throughout the entire pandemic was observed. A subsequent decrease followed this in spine procedures despite a drop in COVID-19 cases.
Average number of procedures/HCO compared to the number of new COVID-19 cases between March 2020-May 2021.
Discussion
To the best of the authors’ knowledge, this study represents the first analysis of trends in spine procedures and diagnosis during the COVID-19 pandemic using a large national cohort. Multiple seasonal analyses were performed to quantify the fluctuations in spine surgery volume. TriNetX, a real-time, continuously updated national database, provided insight into the barriers encountered by patients seeking spine care during the pandemic. Retrospective analyses demonstrated a statistically significant decline in the total volume of spine procedures during the spring season immediately following the WHO’s declaration of the COVID-19 pandemic. For example, spring 2020 volumes for cervical arthrodesis anterior interbody technique with (10.5 vs 17; P < .005) and without decompression (2.5 vs 3.3; P < .05), cervical arthrodesis posterior technique (6.6 vs 8.8; P < .005), and lumbar arthrodesis posterior technique (6.7 vs 11.8; P < .005), all experienced significant decreases in procedural volume compared to pre-pandemic levels. The general decrease in mean procedural volumes in spring 2020 relative to pre-pandemic levels suggests an accumulated, unmet demand for spine surgeries. Considering, that spring 2018 and spring 2019 mean procedural volumes are not statistically different and presumably total demand for spine procedures remains relatively stable year-on-year basis, the observed spring 2020 seasonal decrease in mean procedural volumes quantifies the extent of national backlogs in spine procedures as a result of the pandemic. This decrease simultaneously reflects the spine surgery communities’ inability to meet patient demand due to patient safety concerns and diverted healthcare resources during the pandemic. It is not surprising that the creation of these backlogs on a local scale has been extensively documented as a significant source of financial losses not only in the spine community but also in various other elective-centric specialties.25-29
From an economic standpoint, the relative increases in various procedural volumes further represent efforts to manage backlog-associated medical demand and economic impacts. For instance, after the initial decline in mean procedural volume in spring 2020, subsequent seasonal analyses demonstrated a rebound increase in mean procedural volume in summer 2020, approaching more similar volumes to those seen in pre-pandemic summer seasons. Some procedures in spring 2021 even experienced increased mean procedural volumes compared to pre-pandemic levels, such as lumbar arthrodesis posterior technique single level (13.6 vs 11.8; P < .05). The rebound increase represents a return to more normal operating efficiencies and attempts to address months of backlogged cases.
Overlaying new COVID-19 cases on mean procedural volumes an initial inverse relationship between the number of new COVID-19 cases and spine procedures performed was observed. (Figure 1) The initial rise and peak in COVID-19 cases from March-May correspond with the initial spring 2020 decrease in mean procedural volumes. However, the winter season spanning the end of 2020 and the start of 2021 experienced extensive and steady COVID-19 caseloads but coincided with a rebound increase in total spine procedural volume. While this rebound is undoubtedly multifactorial it likely reflects a change in local, state, and federal regulations, and in particular relaxed hospital policies, and patient behavior. As we anticipate evolving variants of COVID-19 and surges during the winter months, it is imperative that healthcare organizations preemptively prepare for not only seasonal variations in procedural volume, but also procedural backlogs, subsequent surging demand, and potential pandemic-associated regulations. Ultimately, the lingering uncertainty surrounding COVID-19 and its impact on healthcare delivery demands that spine surgeons and their institutions remain flexible to changes in pre-, post-, and intra-operative protocol. Undoubtedly, the gradual return to normalcy was in part due to institutional flexibility such as increased implementation of telemedicine and various remote care options for pre-surgical evaluations and postoperative follow-up.
Despite these institutional adjustments, it is also important to consider our findings in the context of their influence on surgical delay, triaging, and patient outcomes. Multiple studies across a number of spine surgeries suggest that delaying care negatively affects outcomes specifically leading to increased intraoperative bleeding, prolonged hospitalization, increased postoperative complications, and higher treatment costs.14,30,31 Moreover, several studies have highlighted the prolonged pain and neurological debilitation patients experience as a result of treatment delay in addition to the reduced productivity and financial burden experienced on the part of the spine surgeon.32 Therefore, it is our belief that clinicians and surgical centers can utilize our findings as a foundation with which to make informed decisions when enacting pre-, post-, and intra-operative protocol changes that undoubtedly affect patient outcomes. Furthermore, a thorough understanding of pandemic spine trends can clarify which recommendations may have benefited spine patients and where there lies a need for additional triaging strategies to meet gaps in unmet care. When considering the unique sets of challenges and high acuity associated with spine surgery, spine surgeons must play a vital role in ensuring that rapidly evolving recommendations are optimized to preserve both health care resources and patient safety.33 Finally, our findings quantify which spine cases are most at risk of experiencing unexpected delay and allows clinicians to adjust their practices moving forward to address demand-specific changes.
The analyses presented in this study represent only a snapshot of the wide-ranging implications of the COVID-19 pandemic. Increases in spring 2021 procedural volume show that it is possible to operate at efficiency levels above those observed in pre-pandemic seasons. As we continue to move past the pandemic, future studies should evaluate the impact of increased procedural volumes on patient outcomes both prior to and following the widespread distribution of the COVID-19 vaccine and boosters. Specific emphasis should be placed on investigating potential associations between increased procedural volume and patient-reported outcomes and satisfaction measures. Individualized procedural analysis could highlight improvements in safety and guidelines to best maintain and improve patient care in the spine setting, both during COVID-19 and future pandemics. Lastly, a strong understanding of procedural backlogs associated with COVID-19 allows for the perceptive clinician and medical director to adjust their practices to better address procedure-specific changes in demand.
Limitations
Use of the TrinetX database posed several limitations to the current study. By nature of the de-identified electronic health record, specific information regarding case complexity, and emergence, was not provided. Given that procedures were identified by CPT codes, we also cannot directly discern the indications for surgery. Moreover, because the majority of institutions contributing data to TrinetX are large tertiary institutions, the presented data may vary from the experiences encountered within community hospitals. In addition, we stratified the COVID-19 pandemic by season as a surrogate for periods of waxing and waning caseloads; however, there was extensive geographic variation in pandemic waves. Therefore, in describing surgical volume as the mean number of procedures per HCO, we are unable to accurately describe regional variation in procedure volume which is noteworthy considering the varying COVID-19 precautions implemented across the United States.
Conclusion
A thorough understanding of spine procedural trends during the COVID-19 pandemic highlights the preparedness and response within the spine surgery community and can serve as an integral foundation for future pandemic responses. Overall, the COVID-19 pandemic resulted in a widespread decrease in spine procedures. We observed statistically significant reductions in common spine procedures and diagnoses, potentially indicating that patients less frequently sought care for their symptoms during the pandemic or faced limited access to spine care providers. However, increases in procedural volume from pre-pandemic levels during the post-peak stages of the pandemic are encouraging signs that operative volume has improved, and the spine community has aptly adjusted to close the gap in unmet patient care.
Footnotes
Acknowledgments
The authors acknowledge the TriNetX (Cambridge, MA) health care network for their assistance in data analysis for this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iD
Syed Faraz Kazim
References
1.
KhullarDBondAMSchperoWL. COVID-19 and the financial health of U.S. hospitals. JAMA. 2020;323:2127-2128.
2.
AlfaroMMuñoz-GodoyDVargasM, et al.National health systems and COVID-19 death toll doubling time. Front Public Health. 2021;9:669038.
3.
WinkelmannJWebbEWilliamsGAHernandez-QuevedoCMaierCBPanteliD. European countries’ responses in ensuring sufficient physical infrastructure and workforce capacity during the first COVID-19 wave. Health Pol;126:362-372. doi:10.1016/j.healthpol.2021.06.015
4.
CucinottaDVanelliM. WHO declares COVID-19 a Pandemic. Acta Biomed. 2020;91:157-160.
5.
NolteMTHaradaGKLouiePK, et al.COVID-19: Current and future challenges in spine care and education-a worldwide study. JOR Spine. 2020;3:e1122.
6.
MasseyPAMcClaryKZhangASSavoieFHBartonRS. Orthopaedic surgical selection and inpatient paradigms during the coronavirus (COVID-19) pandemic. J Am Acad Orthop Surg. 2020;28:436-450.
7.
MattinglyASRoseLEddingtonHS, et al.Trends in U.S.US surgical procedures and health care system response to policies curtailing elective surgical operations during the COVID-19 pandemic. JAMA Netw Open. 2021;4:e2138038.
BestMJAzizKTMcFarlandEGAndersonGFSrikumaranU. Economic implications of decreased elective orthopaedic and musculoskeletal surgery volume during the coronavirus disease 2019 pandemic. Int Orthop. 2020;44:2221-2228.
11.
GrotleMSmåstuenMCFjeldO, et al.Lumbar spine surgery across 15 years: Trends, complications and reoperations in a longitudinal observational study from Norway. BMJ Open. 2019;9:e028743.
12.
SeretisCArcherLLalouL, et al.Minimal impact of COVID-19 outbreak on the postoperative morbidity and mortality following emergency general surgery procedures: Results from a 3-month observational period. Med Glas. 2020;17:275-278.
13.
KayaniBOnochieEPatilV, et al.The effects of COVID-19 on perioperative morbidity and mortality in patients with hip fractures. Bone Joint J. 2020;102-B:1136-1145.
14.
WagnerSCButlerJSKayeIDSebastianASMorrisseyPBKeplerCK. Risk factors for and complications after surgical delay in elective single-level lumbar fusion. Spine. 2018;43:228-233.
15.
MehrabianDLiuIZPakhchanianHHTarawnehOHRaikerRBoydCJ. Nationwide analysis of plastic and reconstructive procedural volume in the United States during the COVID-19 pandemic. J Plast Reconstr Aesthet Surg;75:1483-1496. doi:10.1016/j.bjps.2021.11.100
16.
SinghDSlavinBRHoltonT. Comparing surgical site occurrences in 1 versus 2-stage breast reconstruction via federated EMR network. Plast Reconstr Surg Glob Open. 2021;9:e3385.
17.
TaquetMLucianoSGeddesJRHarrisonPJ. Bidirectional associations between COVID-19 and psychiatric disorder: Retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatr. 2021;8:130-140.
18.
NiaAMSrinivasanVMLallRRKanP. Middle meningeal artery embolization for chronic subdural hematoma: A national database study of 191 patients in the United States. World Neurosurg. 2021;153:e300-e307.
19.
ChuKYNackeeranSHorodyskiLMastersonTARamasamyR. COVID-19 infection is associated with new onset erectile dysfunction: Insights from a National Registry. Sex Med. Feb 2022;10(1):100478.
20.
WeissHKYamaguchiJTGarciaRMHsuWKSmithZADahdalehNS. Trends in national use of anterior cervical discectomy and fusion from 2006 to 2016. World Neurosurg. 2020;138:e42-e51.
21.
SanfordZTaylorHFiorentinoA, et al.Racial disparities in surgical outcomes after spine surgery: An ACS-NSQIP analysis. Global Spine J. 2019;9:583-590.
22.
AliRSchwalbJMNerenzDRAntoineHJRubinfeldI. Use of the modified frailty index to predict 30-day morbidity and mortality from spine surgery. J Neurosurg Spine. 2016;25:537-541.
23.
HaglinJMRichterKRPatelNP. Trends in Medicare reimbursement for neurosurgical procedures: 2000 to 2018. J Neurosurg. 2019;132:649-655.
24.
MeyersJEWangJKhanADaviesJMPollinaJ. Trends in physician reimbursement for spinal procedures since 2010. Spine. 2018;43:1074-1079.
25.
InglesbyDCBoydCJ. Economic implications of the COVID-19 pandemic on the plastic surgery community. J Plast Reconstr Aesthet Surg. 2020;73:1357-1404.
26.
WisemanSMCrumpRTSutherlandJM. Surgical wait list management in Canada during a pandemic: Many challenges ahead. Can J Surg. 2020;63:E226-E228.
27.
JainAJainPAggarwalS. SARS-CoV-2 impact on elective orthopaedic surgery: Implications for post-pandemic recovery. J Bone Joint Surg Am. 2020;102:e68.
28.
BoseSKDasaniSRobertsSE, et al.The cost of quarantine: Projecting the financial impact of canceled elective surgery on the nation’s hospitals. Ann Surg. 2021;273:844-849.
29.
LouiePKHaradaGKMcCarthyMH, et al.The Impact of COVID-19 pandemic on spine surgeons worldwide [published correction appears in Global Spine J. 2021 Jul;11(6):1012]. Global Spine J. 2020;10(5):534-552.
30.
WadeSMFredericksDRJrMorrisseyPB, et al.Risk factors, and complications associated with surgical delay in multilevel fusion for adult spinal deformity. Global Spine J. 2022;12(3):441-446.
31.
van TolFRMassierJRAFrederixGWJOnerFCVerkooijenHMVerlaanJJ. Costs associated with timely and delayed surgical treatment of spinal metastases. Global Spine J. 2022;12(8):1661-1666.
32.
WeinerJASwiatekPRJohnsonDJ, et al.Spine surgery and COVID-19: The influence of practice type on preparedness, response, and economic impact. Global Spine J. 2022;12(2):249-262.
33.
JainNSAlluriRKSchoplerSSHahRWangJC. COVID-19 and spine surgery: A review and evolving recommendations. Global Spine J. 2020;10(5):528-533.