
Abstract
Study Design
Retrospective cohort study.
Objectives
The coronavirus disease (COVID-19), caused by the severe respiratory syndrome coronavirus 2 (SARS-CoV-2), has created an unprecedented global public health emergency. The aim of the current study was to report on COVID-19 rates in an asymptomatic population prior to undergoing spine procedures or surgeries at two large Los Angeles healthcare systems.
Methods
Elective spine procedures and surgeries from May 1, 2020 to January 31, 2021 were included. Results from SARS-CoV-2 virus RT-PCR nasopharyngeal testing within 72 hours prior to elective spine procedures were recorded. Los Angeles County COVID-19 rates were calculated using data sets from Los Angeles County Department of Public Health. Chi-squared test and Stata/IC were used for statistical analysis.
Results
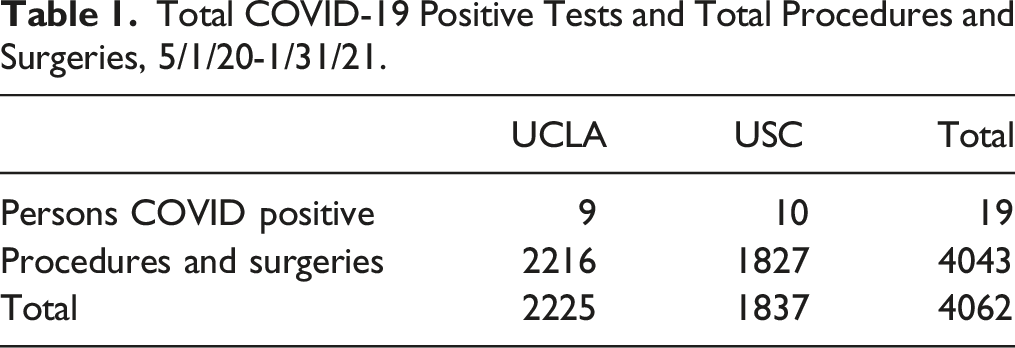
A total of 4,062 spine procedures and surgeries were scheduled during this time period. Of these, 4,043 procedures and surgeries were performed, with a total of 19 patients testing positive. Nine positive patients were from UCLA, and 10 from USC. The overall rate of positive tests was low at .47% and reflected similarities with Los Angeles County COVID-19 rates over time.
Conclusions
The current study shows that pre-procedure COVID-19 testing rates remains very low, and follows similar patterns of community rates. While pre-procedure testing increases the safety of elective procedures, universal COVID-19 pre-screening adds an additional barrier to receiving care for patients and increases cost of delivering care. A combination of pre-screening, pre-procedure self-quarantine, and consideration of overall community COVID-19 positivity rates should be further studied.
Introduction
COVID-19, caused by the SARS-CoV-2 virus, has created an unprecedented global public health emergency with wide-ranging health, economic, and public policy implications. Originally described in Wuhan, China, in December 2019, COVID-19 quickly spread around the world and disrupted health systems. The disease usually causes cold symptoms, fever, and cough, but can progress to cause pneumonia, acute respiratory distress syndrome, and death. The World Health Organization (WHO) reported that there have been 119,220,681 confirmed cases of COVID-19, including 2,642,826 deaths worldwide as of March 14, 2021. 1 The United States has been particularly impacted, with 29,229,162 cases and 531,766 deaths recorded by March 14, 2021. 2 As the virus spread, many non-essential healthcare services were reduced or stopped altogether in order to prevent infections of healthcare workers and to preserve resources, such as personal protective equipment (PPE) and hospital beds, in preparation for continued surges in COVID-19 cases.
As these reduced services have been restored, new guidelines have been established to continue to deliver healthcare widely while reducing risk of COVID-19 transmission. In “OPENING UP AMERICA AGAIN, Centers for Medicare & Medicaid Services (CMS) Recommendations Re-opening Facilities to Provide Non-emergent Non-COVID-19 Healthcare: Phase I,” published April 19, 2020, CMS recommends screening for COVID-19 symptoms prior to patients entering healthcare facilities and screening with laboratory testing once adequate testing can be established. 3 The American College of Surgeons (ACS) recommends consideration of laboratory testing policy that provides useful pre-operative information as to COVID-19 status of surgical patients, particularly in areas of residual community transmission. 4 The American Academy of Orthopedic Surgeons (AAOS) recommends that all patients undergoing surgery receive reverse transcription polymerase chain reaction (RT-PCR) testing within 72 hours of scheduled surgery. 5 This laboratory testing has been suggested to be superior to symptomatic screening as patients can shed virus prior to symptom onset. RT-PCR testing is the gold standard for detecting COVID-19.
The goal of the current study was to describe the rates of COVID-19 positivity in an asymptomatic population of patients prior to undergoing spine procedures and surgeries at two large Los Angeles healthcare systems, Keck Medicine of University of Southern California and the University of California, Los Angeles Healthcare System. Both of these healthcare systems have adopted protocols based on the guidelines above and, prior to restarting procedures and surgeries, had required universal COVID-19 RT-PCR testing of patients within 72 hours of their procedures or surgeries. The current study provides instrumental information over a 9-month time period, including two periods of COVID-19 surges with regard to geographic variances, continued screenings, patient and healthcare worker safety, and infection control as institutions around the world enter re-opening phases.
Methods
This was a retrospective observational study using internal institutional data as well as public data from Los Angeles County Department of Public Health and Center for Disease Control (CDC) data. All elective spine procedures and surgeries over 9 months, from May 1, 2020 to January 31, 2021 following an initial shutdown in spring 2020 were included. During this time, although Los Angeles County initially had relatively low numbers, it quickly became a hotspot for COVID-19 with two significant surges—first in summer of 2020, and again in late fall and early winter 2020–2021. In addition, the geographic distribution of positive COVID-19 cases in Los Angeles County was unique, with significant surges coming from the central and eastern communities of the county. 6
Institutional Review Board (IRB) approval was obtained via USC IRB. Both UCLA and USC used routine universal SARS-CoV-2 virus RT-PCR nasopharyngeal testing within 72 hours prior to elective spine surgeries and procedures. These included spine surgeries, from minimally invasive spine surgery to fusions, as well as spinal procedures and injections, including epidural injections, facet blocks, spinal cord stimulators, and radiofrequency ablations. Each institution has a multidisciplinary spine center which has providers from Neurosurgery, Orthopaedics, and Physical Medicine and Rehabilitation (PM&R). Spine surgeries were performed by both Neurosurgery and Orthopaedics, and procedures were performed primarily by PM&R interventionalists, in both Neurosurgery and Orthopaedics departments.
Los Angeles County COVID-19 rates were calculated using data sets from Los Angeles County Department of Public Health. 7 Rates were determined by dividing positive COVID-19 patients with total number of patients tested each month. These rates mirrored the 7-day average rate trend published by the Los Angeles Times COVID-19 tracking project. 8
Descriptive summary statistics were generated and presented in the results as graphs and a table. Proportion of patients who tested positive was calculated by dividing the number of patients testing positive over the total number of patients who were tested for each month. These proportions were plotted by each month from May 2020 to January 2021 for each institution to examine any possible trends. Since both UCLA and USC had very few positive cases, we were only able to perform a standard Chi-squared test at α = .05 significance level for the total number of positive cases to compare if there was any difference in the proportion of positive cases between the two institutions over the entire study period. P-value of ≥.05 was considered to be not significant. All analyses were performed using Stata/IC (version 15.1, StataCorp LP).
Results
Total COVID-19 Positive Tests and Total Procedures and Surgeries, 5/1/20-1/31/21.
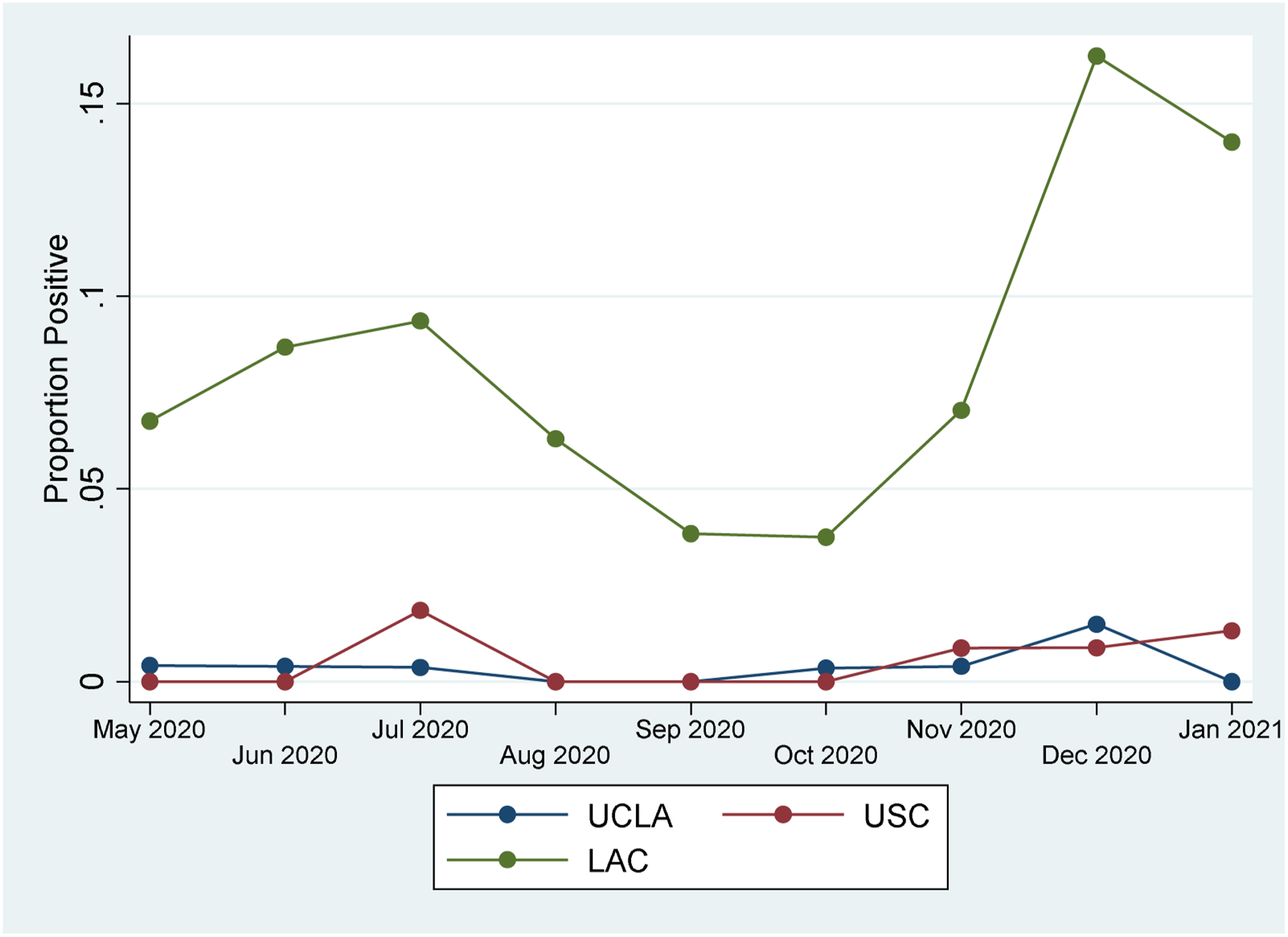
USC had a distinct spike in July 2020, and both USC and UCLA showed increased rates in November 2020, December 2020, and January 2021 (Figure 1). The overall rate of COVID-19 positive screening patients was far lower than the rate COVID-19 positive tests in Los Angeles County, however, it followed the same overall trend, with positive spikes in summer 2020 and winter 2020-2021 (Figure 2). UCLA, USC spine elective cases proportion positive. UCLA, USC, and Los Angeles County (LAC) proportion positive.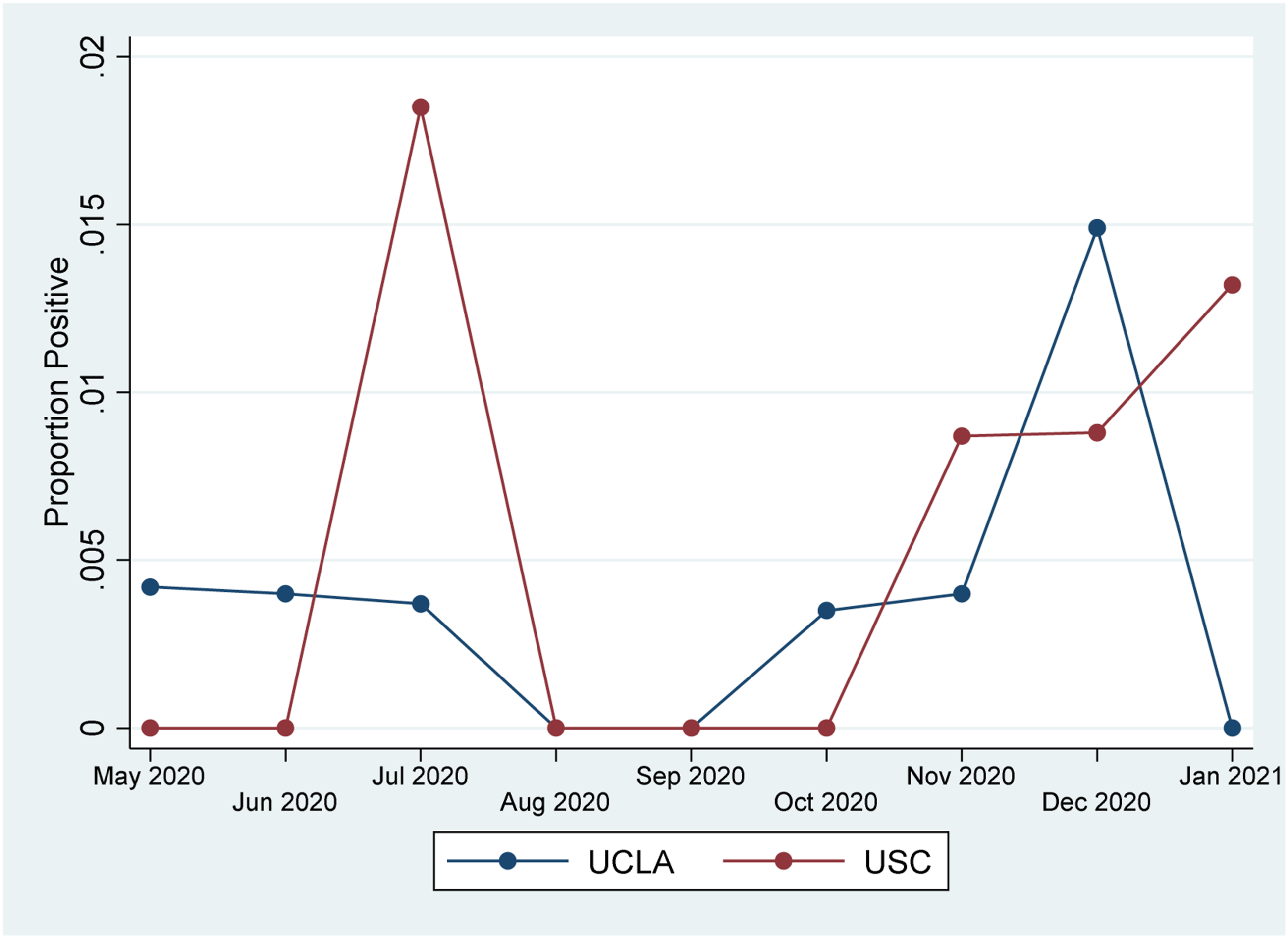
The mean age of COVID-19 positive patients was 59 years old, with a wide geographic distribution which did not correspond with the geography of the institutions, including 4/10 from USC associated with zip codes outside of Los Angeles County.
Discussion
Using routine universal SARS-CoV-2 virus RT-PCR nasopharyngeal testing on asymptomatic patients prior to elective spine procedures and surgeries in two large Los Angeles academic health systems from May 2020 through January 2021, the overall rate of positive COVID-19 tests was .47%. As of March 14, 2020, Los Angeles County reported 1,210,265 cases of COVID-19 (estimated 12-13% of the population), and deaths from COVID-19 are documented at 22,474 (1.85% of those infected). 7 The lower rate seen in the current study is likely due to an asymptomatic screening population, prior to an elective procedure or surgery. The population of Los Angeles County who may have had testing done were more likely due to exposure, symptoms, or both. As such, this population may have been inherently at higher risk for COVID-19 infection. In addition, our study population likely had a lower overall percentage of higher risk individuals, such as those residing in nursing homes. Patients exhibiting COVID-19 symptoms or testing positive would be less likely to be seen in spine clinic and/or schedule elective procedures or surgeries given robust screening questionnaires and protocols.
The current study evaluating elective spine procedures and surgeries complements other recently published data, which have described rates of COVID-19 positivity among asymptomatic screening populations between .13% and 12.1%. Zangrilli et al. 9 described a low rate of COVID-19 in elective hip and knee replacements between May 1 and July 21, 2020; out of 2329 patients only 5 (.21%) were COVID-19 positive. Singer et al. 10 examined asymptomatic pre-operative COVID-19 rates for all pre-operative screening at UCLA from April 7 to May 12, 2020, during a non-peak COVID-19 period in Southern California and reported a rate of .13% out of 4,751 patients.
From April 5 to April 24, 2020, at the height of the first surge in COVID-19 in New York City, Gruskay et al. 11 described a COVID-19 positive rate of 12 out of 99 patients (12.1%) for planned orthopedic surgery. Villa et al. 12 reported COVID-19 rates during pre-operative screening in Florida from April 13 through August 27, 2020; they found a total rate of 1.2% positive out of 7213 patients, and noted that changes in their rates mirrored the trend seen in the general Florida population. The published New York City rates in April 2020 and Florida rates from April to August 2020 were higher than other published data and higher than our findings, possibly reflecting the high prevalence of the time period and locations where the data was collected.
All of these prior studies reported data for shorter time periods, from 3 weeks to 4 months, while we report data for 9 months, inclusive of two community COVID-19 surges. By measuring COVID-19 positivity in our study population over a longer period of time at two large and geographically diverse academic institutions, we demonstrate how our elective spine screening data mirrored the monthly trend in the Los Angeles County population, with two distinct COVID-19 surges.
California appeared to be spared from the initial surge in COVID-19 in March–April 2020 seen in places like New York City. However, soon thereafter, Los Angeles become a COVID-19 hotspot. There were two distinct surges in COVID-19 rates in Los Angeles County: the first in June–July 2020 and the second in December 2020–January 2021. This study encompasses both non-surge and surge periods. While we were not able to perform statistical correlations by time given our low overall numbers, we do observe similarities in the rates of COVID-19 positive patients in the study population with the surges in cases from June–July 2020 and in December 2020–January 2021 (Figure 2).
Although UCLA and USC are located in two distinct geographic regions within Los Angeles, no difference was noted in COVID-19 rates. On January 29th, 2021, Jill Cowan and Matthew Bloch of the New York Times published an article and map showing that East Los Angeles, where USC is located, had much higher rates of COVID-19 than West Los Angeles, where UCLA is located. 13 Vijayan et al. showed that geographic clusters of highest quintile positivity were found in Central and East Los Angeles, while areas of lowest quintile positivity were found in West Los Angeles, with higher COVID-19 rates correlating with higher Latino/a population, more dense housing, and lower socioeconomic status. 14
Our study data showed similar rates at each institution, with rates of COVID-19 positivity of .40% at UCLA and .54% at USC. There are several reasons the two institutions did not have significantly different rates despite distinct geographic locations. Mainly, both USC and UCLA are academic spine centers which draw patients from a wide geographic range. In fact, four of the ten positive patients from USC were from outside of Los Angeles County entirely, and two of the nine UCLA positive patients were from zip codes immediately adjacent to USC. As such, despite unique geographic positions within Los Angeles County, pre-procedure COVID-19 testing in these two institutions showed no statistical differences. The population of patients being seen for spine procedures and surgery were likely similar between institutions, with health literacy, insurance status, or socioeconomic status of the population not necessarily reflective of the geographic area of the academic spine center.
Applications to Current Practice
Population prevalence data can help inform screening protocols prior to elective procedures and surgeries. As seen in our data, pre-screening COVID-19 rates are much lower than actual county rates, however, do seem to follow similar trends. While pre-procedure testing can increase safety of elective procedures and give peace of mind to staff and patients, universal COVID-19 pre-screening adds an additional barrier to receiving care for patients and increases cost of delivering care. If pre-procedure COVID-19 testing rates follow similar patterns of community rates, at what point does it no longer make sense to require universal RT-PCR testing for every patient pre-procedure? A study by Nishitani et al 15 of asymptomatic orthopedic patients required to self-quarantine for 14 days prior to receiving elective surgery in Kyoto, Japan, found that none of the 304 patients had positive COVID-19 RT-PCR testing, suggesting that self-quarantine reduces rates of COVID-19 before procedures. Currently, given increasing rates of COVID-19 vaccinations amongst the general population, health care providers, hospitals, and systems must consider the time and cost associated with COVID-19 pre-screening for all patients for elective procedures and surgeries. While we certainly do not have an answer, perhaps a combination of pre-screening, pre-procedure self-quarantine, and consideration of overall community COVID-19 positivity rates should be further studied.
Conclusion
This study describes the rates of COVID-19 positive RT-PCR testing from May 2020–January 2021 in a population of asymptomatic patients prior to receiving spine surgery or procedures from two large academic centers in Los Angeles, an epicenter of COVID-19. The current data shows a low overall rate of COVID-19 positivity of .47%. There was no difference in COVID-19 positivity between USC and UCLA, despite differences in geographic location. The observed COVID-19 rates were much lower than published Los Angeles County rates overall, and the current study observed a similar increase in rates of COVID-19 positive test results in the study population during the COVID-19 surges in summer 2020 and winter 2020–2021. This study suggests that county or regional COVID-19 data could be used as an additional measure to augment our decision-making process with regard to universal pre-procedure testing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosures outside of submitted work: AC- Fellowship support: Medtronic, Abbott (paid to institution); Spine Intervention Society (Non-financial - travel stipend); JCL – Board: North American Spine Society; JCW- Royalties – Biomet, Seaspine, Synthes; Investments/Options – Bone Biologics, Pearldiver, Electrocore, Surgitech; Board of Directors - AO Foundation; Fellowship Funding (paid to institution): AO Foundation; ZB- consultancy: Cerapedics (past), The Scripps Research Institute (past), Xenco Medical (past), AO Spine (past); Research Support: SeaSpine (past, paid to the institution), Next Science (paid directly to institution), Medical Metrics (past, paid directly to institution); North American Spine Society: committee member; Lumbar Spine Society: Co-chair Educational Committee, AO Spine Knowledge Forum Degenerative: Associate member; AOSNA Research committee- committee member.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.