
Abstract
Study Design
Retrospective database analysis.
Objectives
To study postoperative complication rates following anterior cervical discectomy and fusion (ACDF) in patients with Ehlers-Danlos syndrome (EDS) compared with patients without EDS.
Methods
The Mariner database was utilized to identify patients with EDS undergoing one or two level anterior cervical discectomy and fusion (ACDF). Postoperative short-term outcomes assessed included medical complications, readmissions, and ED-visits within 90 days of surgery. Additionally, surgical complications including wound complications, surgical site infection, one- and two-year anterior revision along with posterior revision, pseudarthrosis, and hardware failure within 2 years were assessed. Multivariate logistic regression was used to adjust for demographic variables, comorbidities and number of levels operated on.
Results
The present study identified 533 patients in the EDS group and 2634 patients in the matched control group. EDS patients undergoing ACDF are at an increased risk for 90-day major medical complications (OR 3.31; P < .001). EDS patients were also found to be associated with surgical complications including wound complications (OR 2.94; P < .001), surgical site infection (OR 8.60; P < .001) within 90 days, pseudarthrosis (OR 2.33; P < .001), instrument failure (OR 4.03; P < .001), anterior revision (OR 22.87; P < .001), and posterior revision (OR 3.17; P < .001) within 2 years.
Conclusions
EDS is associated with higher rates of both medical and surgical complications following ACDF. Spine surgeons should be cognizant of the increased risks in this population to provide appropriate preoperative counseling and enhanced perioperative medical management.
Introduction
Ehlers-Danlos syndrome (EDS) is a collective term for a series of genetic connective tissue disorders with variable expressivity that is characterized by skin hyperextensibility, tissue fragility, and joint hypermobility.1,2 13 types of EDS have been identified by the new international EDS Consortium. 3 Incidence of Ehlers-Danlos syndromes is 1 in 5000, with hypermobile EDS being the most prevalent, 4 followed by classical and vascular types. 5 Of particular interest to spine surgeons, cervical segmental instability is more frequently observed in patients with EDS however its prevalence has not been well established. This cervical instability results in a progressive loss of cervical lordosis with subsequent narrowing of the spinal canal, predisposing EDS patients to progressive myelopathy. 6
Many studies have documented surgical outcomes for EDS patients with thoracolumbar kyphoscoliosis, however, there is a paucity of literature involving cervical pathologies. Kobets described a case where anterior corpectomy and fusion (ACCF) with posterior fusion was employed to treat an infant with EDS type VI for symptomatic cervical kyphoscoliosis. 7 Fang et al reported a similar case where ACCF was used to treat an adolescent EDS patient with cervical kyphosis. 8
While isolated case reports have been published, large retrospective studies regarding the outcomes of EDS patients undergoing anterior cervical discectomy and fusion (ACDF) procedures have not been assessed given the paucity of patients with this condition. The main objective of this study is to assess the outcomes of patients with EDS undergoing ACDF procedures. We hypothesize that patients with EDS will have higher rates of post-operative 90-day complications, including readmission and revision.
Methods
Data Source
The PearlDiver database (www.pearldiverinc.com, Colorado Springs, CO), a fee-based patient records database, was utilized in this study. It is an insurance-based database that contains a combination of patient demographics, charge data, and procedural records for patients with International Classification of Diseases, 9th Revision (ICD-9-CM), 10th revision (ICD-10-CM) diagnoses and procedures or Current Procedural Terminology (CPT) codes from multiple different insurers, including both Medicare and Humana (private insurer). The PearlDiver database houses records of over 100 million patients from either the Mariner claims or the Medicare Standard Analytical Files. Access to this database, which was stored on a password-protected server, was obtained from PearlDiver Technologies for the purpose of academic research. Patient data was de-identified and therefore exempt from institutional review board approval.
Study Population
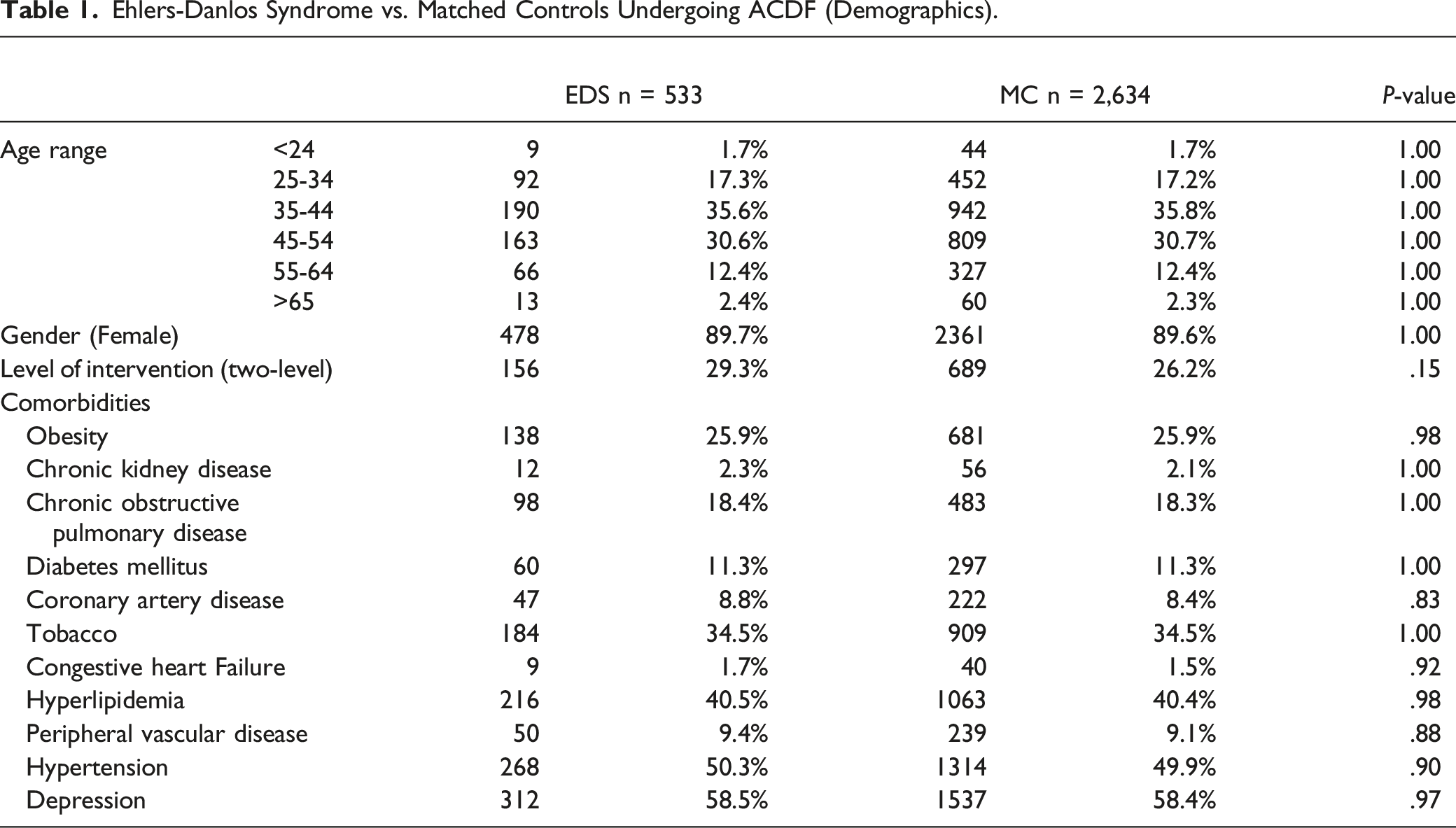
Ehlers-Danlos Syndrome vs. Matched Controls Undergoing ACDF (Demographics).
Outcomes
Patients with EDS were compared to controls for 90-day major and minor medical complications, 90-day emergency department (ED) visits, 90-day readmissions, one-year and two-year anterior revisions as well as posterior revisions, and pseudarthrosis and instrument failure within 2 years. 90-day major medical complications included pulmonary embolism, pneumonia, cerebrovascular accident, myocardial infarction, and sepsis. Other 90-day complications included deep vein thrombosis, acute kidney injury, urinary tract infection, and transfusion. Patients were also queried for wound complications and surgical site infections at 90 days following surgery.
Statistical Analysis
Pearson χ2 test was used to assess differences in demographics and preexisting comorbidities (including smoking status). A multivariate logistic regression comparing patients with EDS and those without was used to determine the independent effect of EDS on the postoperative outcomes after adjusting for demographic factors and comorbidities as well as levels operated on. R software embedded within the PearlDiver database (R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analysis. Factors were considered significant at P < .05.
Results
Patient Demographics and Comorbidities
Ehlers-Danlos Syndrome vs Matched Controls Undergoing ACDF (Outcomes)
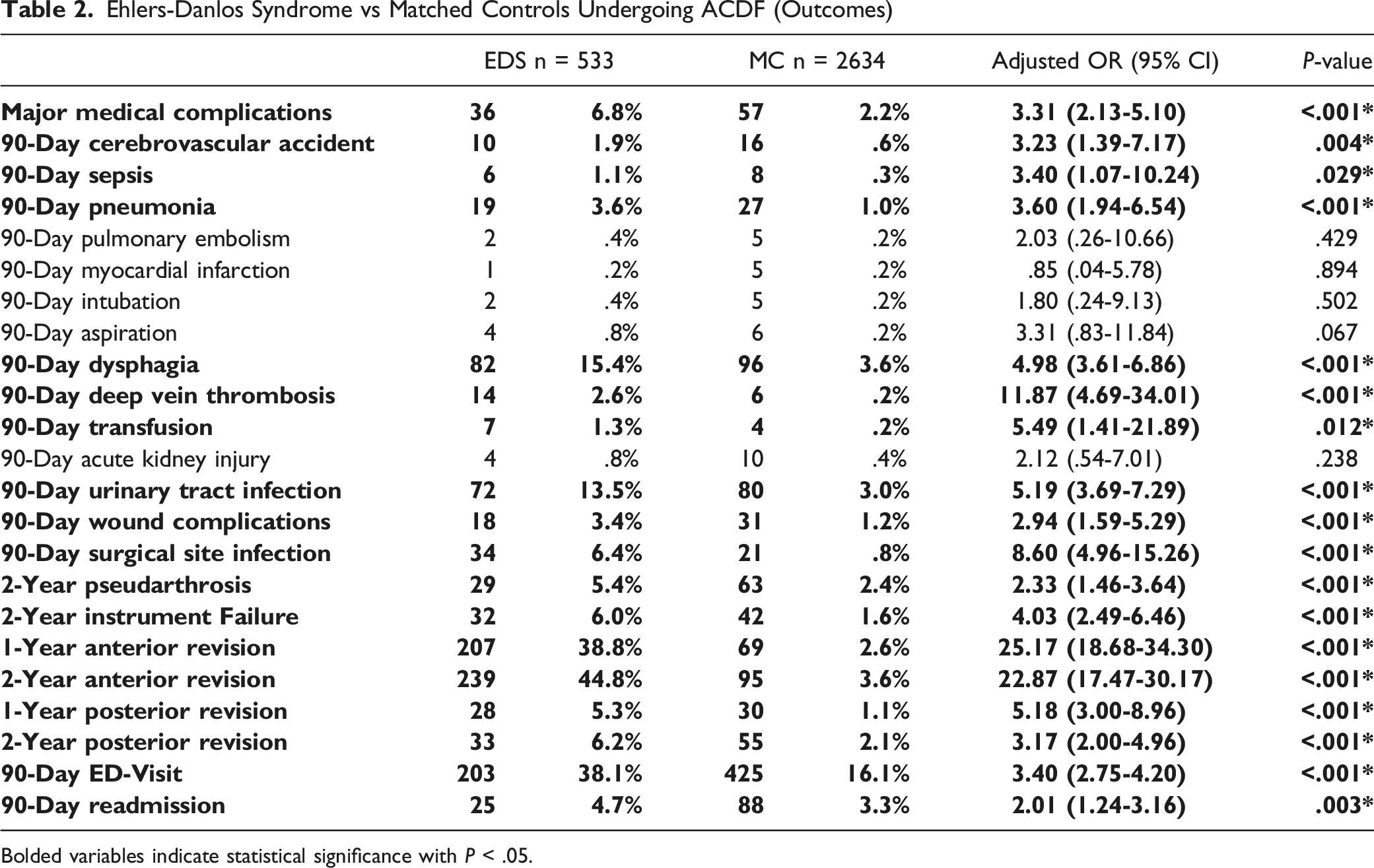
Bolded variables indicate statistical significance with P < .05.
Postoperative Complications
Multivariate analysis showed that patients with EDS undergoing ACDF were found to have increased incidence of 90-day major medical complications including: cerebrovascular accident (1.9% vs .6%; OR 3.23, 95% CI 1.39-7.17; P = .004), sepsis (1.1% vs .3%; OR 3.40, 95% CI 1.07-10.24; P = .029), pneumonia (3.6% vs 1.0%; OR 3.60, 95% CI 1.94-6.54; P < .001). Other medical complications within 90 days include dysphagia (15.4% vs 3.6%; OR 4.98, 95% CI 3.61-6.86; P < .001), deep vein thrombosis (2.6% vs .2%; OR 11.87, 95% CI 4.69-34.01; P < .001), transfusion (1.3% vs .2%; OR 5.49, 95% CI 1.41-21.89; P = .012), urinary tract infection (13.5% vs 3.0%; OR 5.19, 95% CI 3.69-7.29; P < .001). EDS was also associated with higher incidences of 90-day ED-visit (38.1% vs 16.1%; OR 3.40, 95% CI 2.75-4.20; P < .001), and 90-day readmission (4.7% vs 3.3%; OR 2.01, 95% CI 1.24-3.16; P = .003). In addition, EDS patients had increased rates of surgical complications: 90-day wound complications (3.4% vs 1.2%; OR 2.94, 95% CI 1.59-5.29; P < .001), 90-day surgical site infection (6.4% vs .8%; OR 8.60, 95% CI 4.96-15.26; P < .001), 2-year pseudarthrosis (5.4% vs 2.4%; OR 2.33, 95% CI 1.46-3.64; P < .001), 2-year instrument failure (6.0% vs 1.6%; OR 4.03, 95% CI 2.49-6.46; P < .001), 1-year anterior revision (38.8% vs 2.6%; OR 25.17, 95% CI 18.68-34.30; P < .001), 2-year anterior revision (44.8% vs 3.6%; OR 22.87, 95% CI 17.47-30.17; P < .001), 1-year posterior revision (5.3% vs 1.1%; OR 5.18, 95% CI 3.00-8.98; P < .001), 2-year posterior revision (6.2% vs 2.1%; OR 3.17, 95% CI 2.00-4.96;P < .001) (Table 2).
Discussion
EDS is a group of rare connective tissue disorders that are mainly caused by the abnormality of the gene encoding collagen fibers. 2 Ligamentous laxity, which is present in varying degrees in all forms of EDS, can result in cervical instability and kyphoscoliosis, manifesting clinically as motor delay, myelopathy and radiculopathy, dyspraxia, paresthesia, spasticity, and gait instability. 6
Previous literature has established that EDS is associated with dysphagia.9-13 The present study further confirms prior research, as EDS was found to be associated with increased occurrence of dysphagia postoperatively. The high prevalence of swallowing difficulties may be contributed by the underlying connective tissue defect, which causes failure of the larynx to move upward and forward at the right time. This causes hold-up of solids/liquids and epiglottis not closing properly. And as food particles descend into the larynx, choking might occur. This can happen in EDS patients when competing muscle groups and ligaments that coordinate free-floating movements fall out of sync.9,12 Furthermore, previous literature has demonstrated that pneumonia is one of the most common complications in EDS patients, and the present study confirms that.14-18
Surgical complications such as wound healing complications and surgical site infection were more prevalent in the EDS cohort with 6.4% developing surgical site infection. Other studies support this increase in infection rates with one retrospective review consisted of 120 patients identifying 8.6% in the average infection rates among EDS patients undergoing orthopaedic surgery. 19 Furthermore, Weinberg et al reported that wound complications and surgical site infections occurred in 11% and 6% of orthopaedic procedures in EDS patients respectively, which is significantly greater than that of the average population. 20 In many instances, EDS is attributed to mutations that produce abnormal collagen with specific molecular defects in types I, III, and V collagen, manifesting in collagen-rich tissues such as skin, ligaments, and joints.21,22 DeNigris et al demonstrated in a mouse modal that collagen V deficiency decreases dermal fibroblast proliferation and attachment of fibroblasts to wound matrix components, which ultimately decreases wound healing response in classical type EDS. 23 Porter et al reported 2 cases of deep surgical site infection in pediatric patients with connective tissue disorder with 1 being EDS out of 112 following cervical spine surgery. 24 A retrospective study by Matur et al compared pediatric EDS patients undergoing spine surgery to those without EDS. After evaluating 56 EDS patients following lumbar spine surgery, they found no differences in reoperations, wound infections or disruptions, total blood transfused, hospital length of stay, or overall complication rate. However, since the data for this study came from the Pediatric National Surgery Quality Improvement Program Database, long-term outcomes could not be recorded, and the sample size is small, severely restricting the study’s findings. 25
Additional long term surgical complications were also more prevalent in EDS patients, collectively pseudarthrosis, implant failure and revision rates within 1 and 2 years with EDS patients presenting with a 15-fold increase in anterior revision rate in 1 year relative to their age matched controls and 44.8% of EDS patients requiring anterior revision within 2 years of their index procedure. Though rates of posterior revision for additional stabilization within 1 and 2 years were considerably lower compared to anterior revision in the EDS cohort, at 5.3% and 6.2% respectively, speculating that anterior adjacent level fusion was sufficient in achieving fusion and restoring normal lordotic configuration. 26 Gouzoulis et al found no significant differences in 5-year reoperation rates in EDS patients undergoing single-level posterior lumbar fusion. 27 The discrepancy could be due to that the amount of axial rotation tolerated in the cervical spine can be 10 times that of the lumbar spine, 28 particularly in hypermobile EDS population with global pathology likely consisted of cervical kyphosis and segmental instability. Immobilization of a cervical motion segment transfers increased loading and biomechanical stress to the adjacent motion segments than lumbar motion segment, potentially leading to increased adjacent segment disease and rates of revision. 29
Rabenhorst et al recorded 1 pediatric patient with EDS experiencing multiple implant failures after posterior spinal fusion, however, those failures were in a growing child who was operated on with different equipment in a different era of spine surgery. 30 Jasiewicz et al reported 4 EDS patients out of 11 undergoing reoperations following spinal deformity surgery due to instrumentation failure and pseudarthrosis. 31 The proposed etiology behind this could be associated with poor bone mineralization which along with fractures appear to be common in certain rare types of EDS (kyphoscoliotic, arthrochalasia, spondylodysplastic, and classical-like EDS). For the more prevalent hypermobile and classic EDS types, there seems to be a slight reduction in bone mineral density. 32 Coussens et al also found lower cortical bone mineral content and cortices in individuals with hypermobile EDS. 33 Poor bone health commonly manifests as osteoporosis, which is a risk factor for pseudarthrosis and instrument failure as a result of displaying diminished pullout strength and insertional torque.34,35 This phenomenon is clinically warranted as pseudarthrosis has been shown to impede neck pain relief and is one of the most common indications for additional intervention after ACDF, accounting for up to 56% of revision cases. 36 Though it is unclear whether increased rates of reoperation are due to adjacent level or index level pathologies due to the nature of CPT code definition. EDS patients should be consulted and informed for the additional risks of reoperation before undergoing ACDF.
Decompression of neural elements, correction of deformity, and stabilization constitute the overall surgical goals for EDS patients. Decompression and fusion can be accomplished via anterior, posterior, and combined anterior-posterior approaches. Anterior approaches may be preferred in the presence of anterior pathologies, cervical kyphosis, or one-to two-level pathologies. 37 Posterior approaches may be favored for wider decompressions, pathologies involving more than three levels, and ossification of the posterior longitudinal ligament. 38 The anterior-posterior combined approach provides a better fusion rate and a lower instrumentation failure rate in the osteoporotic population, 39 which is not rare in patients with EDS. Kim et al noted that for patients with kyphotic deformity or in need of multi-level surgery, combined approach is preferred for stability. 40 Song et al reported higher rates of pseudarthrosis and hardware-related complications in patients with cervical kyphosis treated with anterior-only approach than combined approach. 41 Despite these distinctions, the anatomy in many cases renders anterior, combined anterior-posterior, and posterior approaches clinically equipoise, leaving the choice to surgeon preference. Consequently, a patient-specific surgical strategy should be employed to achieve optimal surgical outcomes in EDS patients.
This study benefits from the inherent advantages that come with the use of large national databases, namely the ability to examine rare diseases on a large scale that would be difficult to do at a single institution. Likewise, the inclusion of 533 patients in this study ensured that it was adequately powered and did not suffer from the limitations of a small sample size and regional biases that can result from underpowered, single-center observational studies. Moreover, the PearlDiver database is unique in its capacity to longitudinally track postoperative patient data. In comparison to databases such as the National Inpatient Sample (NIS) database and the National Surgical Quality Improvement Program (NSQIP) database, which can only track complications that occur in-hospital or within 30 days after surgery, outcomes can be recorded at any time during enrollment, providing a reliable source of short- and intermediate-term data. In addition, the scarcity of literature on EDS patients undergoing ACDF renders the results of this study unique.
Unfortunately, the use of a large retrospective database is not with its inherent limitations. The reliability of our findings depends on the accuracy of the database’s coding. Human error can result in inaccurate coding; however, this error is estimated to account for only 1.1% of all entries. 42 In addition, a comprehensive multivariate regression analysis corrects any potential confounding due to code. However, multivariate regression analysis cannot control for variables that exist outside of the coding database (operative time, blood loss, surgical technique) because of the limited granularity of the database and that may potentially skew outcomes. Further, certain complications such as adjacent segment disease, C5 palsy, recurrent laryngeal nerve palsy cannot be assessed due to inexistence of ICD9/10 diagnostic codes.
Conclusion
The results of this study indicate that patients with EDS are at an increased risk for medical complications as well as surgical complications following ACDF. EDS presents a challenge to cervical spine fusion patients who are undergoing a relatively safe procedure. Prior to surgical intervention, a proper understanding of potential postoperative risks of EDS diagnosis and evaluation for cervical spine instability could give insight into resulting complications postoperatively.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.