
Abstract
Study Design
Systematic review
Objectives
It remains unknown whether general anesthesia (GA) or local ± epidural anesthesia (LA) results in superior outcomes with percutaneous endoscopic lumbar discectomy (PELD). The present study sought to examine the impact of anesthesia type on patient-reported outcomes (PROs) and complications with PELD.
Methods
Systematic review and meta-analysis examining PELD performed under GA or LA was conducted. Patient-reported outcomes including Visual Analog Scale (VAS)-leg/back, and Oswestry Disability Index (ODI) scores were collected. Complication, recurrent disc herniation, durotomy, and reoperation rates as well as surgical data were recorded. All outcomes were compared between pooled studies examining GA or LA.
Results
Sixty-eight studies consisting of 5269 patients (724 GA, 4465 LA) were included in the meta-analysis. Overall complication rate was significantly higher in the GA group (9% vs 4%, P = .003). Durotomy rates, length of stay, recurrent disc herniation and reoperation rates were similar between groups. At the first follow-up timepoint, the LA group demonstrated significant improvements in VAS back and ODI scores (P < .05) while the GA group did not (P > .05). At the final follow-up (> 6 months), the percent of patients achieving an excellent McNab score was significantly higher in the GA vs LA group (P < .001).
Conclusions
Percutaneous endoscopic lumbar discectomy with LA may be associated with greater short-term improvement in VAS back pain and ODI scores. General anesthesia may be associated with more durable pain relief but a higher complication rate. Further systematic investigation is necessary to determine what short and long term benefits are associated with PELD performed under LA and GA.
Keywords
Introduction
Symptomatic lumbar disc herniation is one of the most common causes of lower back and leg pain. 1 When aggressive nonoperative management fails to provide symptomatic relief, surgical intervention is necessary. While open laminectomy and discectomy has traditionally shown acceptable outcomes for lumbar disc pathology, surgeons have developed minimally invasive techniques including percutaneous endoscopic lumbar discectomy (PELD). 2
The percutaneous endoscopic approach for lumbar discectomy has gained popularity amongst some spine surgeons due to the shorter recovery times, hospital stays, and less muscular trauma encountered by the patient during the approach.3-5 Percutaneous endoscopic lumbar discectomy can be performed under both general anesthesia (GA) or local ± epidural anesthesia (LA). 6 Local ± epidural anesthesia is now being recommended by some spine surgeons due to its rapid analgesic onset, shorter operative times, decreased systemic complications, and adequate intraoperative and postoperative pain control.7,8 Downsides to LA include patient discomfort potentially necessitating shorter operative times, in addition to a diminished ability to maintain strict hemodynamic and anesthetic parameters and risk of insufficient discectomy.3,9-11 Controversy surrounds the feasibility, efficacy, and safety of LA compared to GA when it comes to PELD. 12 Therefore, the aim of this study was to conduct a systematic review and meta-analysis examining complication rates and patient-reported outcomes (PROs) after PELD performed under LA vs GA.
Methods
This study was conducted with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 13 and was exempt from institutional review board approval.
Search Strategy
The PubMed, EMBASE and SCOPUS databases were used to identify relevant studies. A search was conducted on August 16, 2021, of these 3 databases and included all studies published between 1990 and the date of the search. The search strategy consisted of combinations of key words and commonly used synonyms and abbreviations. Two authors (AS, JM) performed separate literature searches. The advanced search for articles in each database included the terms (((conscious sedation [Title/Abstract]) OR (awake [Title/Abstract]) OR (without GA [Title/Abstract]) OR (local [Title/Abstract])) AND (PELD [Title/Abstract]))) to identify relevant articles for the LA group. Articles for the GA group were identified with the following terms: ((PELD [Title/Abstract])). References cited in the eligible studies were also evaluated to identify any additional studies.
Records were screened by several reviewers working independently including JM and either AS, NE, AM, BM and NL. Reviewers JM, AS, NE, AM, BM and NL independently collected the data from the final list of included studies and this data was reviewed by JM. Any discrepancies were adjudicated by a third reviewer.
Inclusion and Exclusion Criteria
Study inclusion criteria were: (1) first-time single or two-level PELD between L1-S1; (2) patient age ≥ 18; (3) > 10 patients; (4) study published in the English language; (5) patients with at least 6 months of reported follow-up with (6) documented pre and post-operative PROs in one or more of the categories including visual analog scale (VAS) leg, VAS back, Oswestry Disability Index (ODI), Japanese Orthopedic Association (JOA) score, McNab Score or 36-item short form physical component score (SF-36 PCS) (7) inclusion of standard deviation values for included PROs and any other continuous variables.
Percutaneous endoscopic lumbar discectomy was defined as any purely endoscopic approach performed percutaneously and included both transforaminal and interlaminar approaches. Studies involving cases performed with an open approach as well as those involving a tubular retractor or operating microscope were excluded.
For the LA group, studies were required to have a patient cohort with >90% of patients undergoing surgery with local ± LA with or without conscious sedation. For the GA group, studies were required to have a patient cohort with >90% of patients undergoing GA prior to surgery.
Meta-analyses, review articles, case reports, and studies involving pathologies other than disc herniation, studies involving revision surgeries, non-English language, open surgical procedures and lumbar fusion procedures were excluded. Studies involving patients <18 years old were excluded in addition to studies with a lack of adequate follow-up (6 months) or lack of PRO data categories.
Data Collection and Analysis
Studies were grouped as having patient cohorts undergoing either GA or LA. If a study was comparative between GA and LA, the cohorts were analyzed separately in their respective groups for the purpose of meta-analysis. Information on patient demographics and follow-up time in addition to PROs including VAS general, VAS back/leg, JOA score, McNab Score (Percent Excellent), ODI and SF-36 PCS were extracted from the studies. Additional information including mean surgery time, blood loss, complication rate, durotomy rate, length of stay, disc recurrence rate and reoperation rates were extracted from each study when available, pooled and compared between the LA and GA groups. Only studies that reported data with standard deviation values for a given category were included in the final analyses. Additionally, subgroup analysis was performed comparing outcomes with LA and GA for PELD using data from only the prospective and randomized control trials (RCTs).
Outcomes
Primary outcomes were complication rate, durotomy rate, recurrent disc herniation rate, reoperation rate, and length of surgery, as these were the most consistently reported values across all studies and found to be the most objective. Complications included transient paresthesias, nerve root injuries, infection, wound dehiscence, sexual dysfunction, urinary retention, durotomy, discitis and post-operative hematoma. Complications attributed specifically to anesthesia and not related to the surgical intervention were not included.
Secondary outcome data including the PROs VAS general, VAS back/leg, JOA score, McNab Score (Percent Excellent), ODI score and SF-36 PCS score were recorded when available pre-operatively, at the first post-operative follow-up (within 1 month) and at the 3, 6, 12 and 24 months follow-up timepoints. Given the range in follow-up between studies, only the first post-operative follow-up and last follow-up time-points were pooled for comparison. Changes in PROs from pre-op to the first and last post-op follow-up appointment were also calculated and compared between LA and GA groups.
Statistical Analysis
Descriptive statistics were calculated for baseline, surgical, and outcomes data using R (R Foundation for Statistical Computing, Vienna, Austria). For categorical variables, absolute counts were extracted to calculate proportions. For continuous variables, means and associated standard deviations were extracted. After Freeman-Tukey double arcsine transformation for count variables, weighted pooled means and associated 95% confidence intervals (CI) were computed using the DerSimonian-Laird method. A random effects model was used due to the assumptions of clinical diversity and differences in methodology among the included studies. The LA and GA cohorts were compared using a subgroup meta-analysis. Forest plots and the I2 statistic were used to investigate heterogeneity. Heterogenity between different studies were evaluated by χ2 and I2, and P < .05 was considered statistically significant. I2 values of <25%, 25% to 75%, and > 75% represent mild, moderate and severe heterogeneity respectively. All statistical tests were two-tailed, and P < .05 was considered statistically significant.
Risk of Bias of Individual Studies
The Newcastle-Ottowa Scale 6 was used to assess the quality of the included studies. Several reviewers reviewed each study working independently and discrepancies were adjudicated by a third author.
Results
Search Results
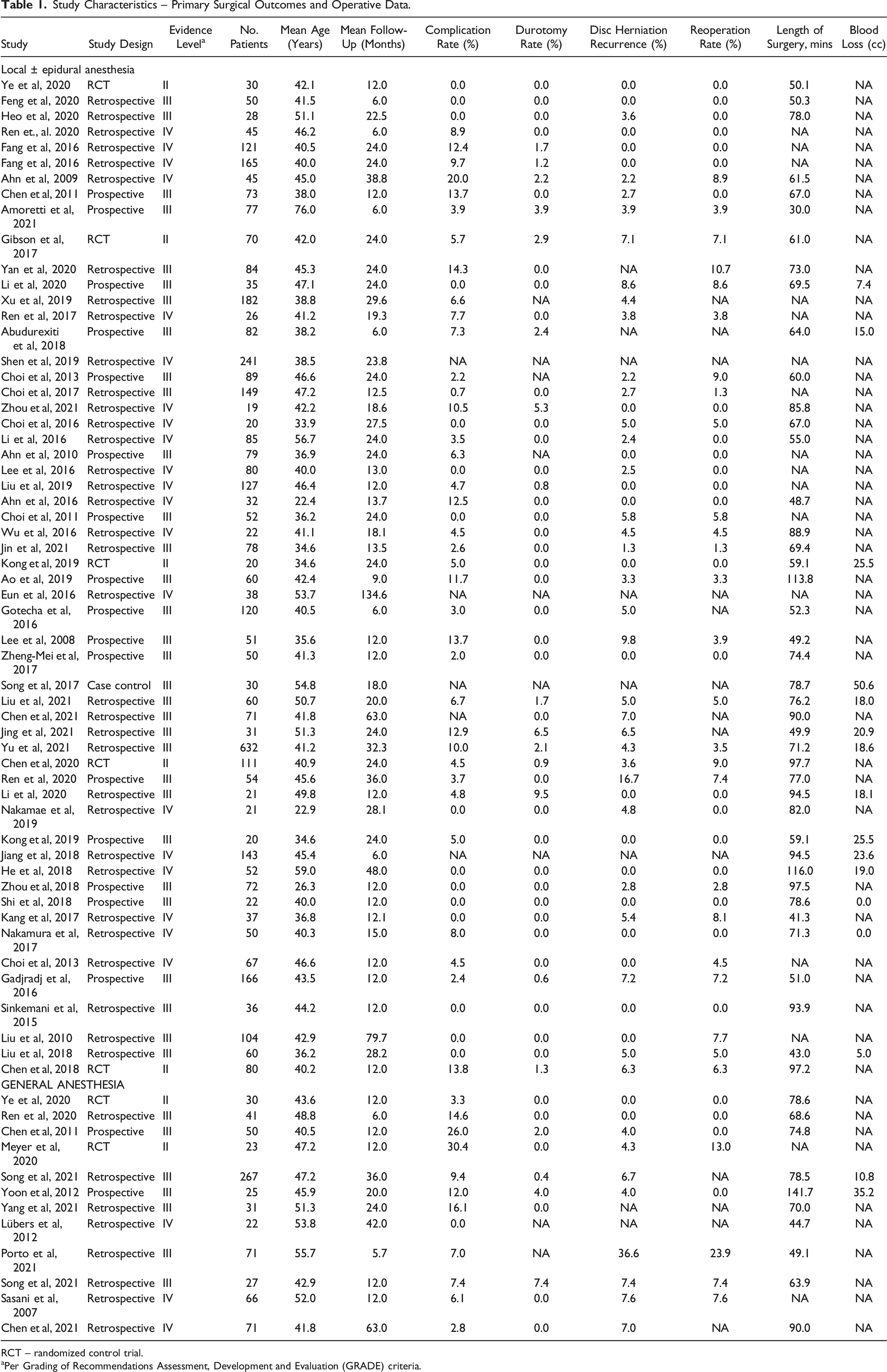
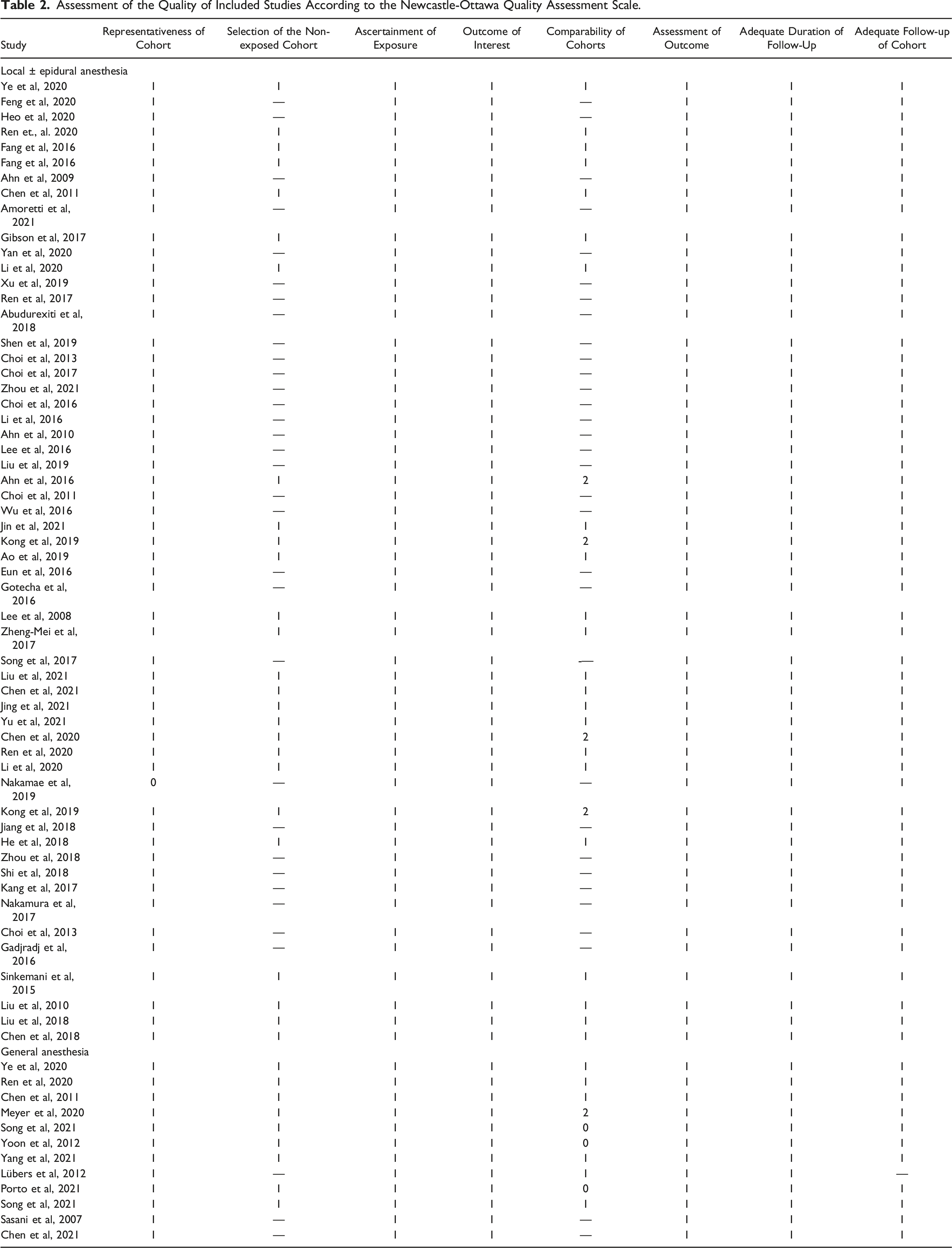
After the initial search of the electronic databases, a total of 806 articles were identified. Articles were further screened by titles, abstracts and full texts according to the specific inclusion and exclusion criteria. Ultimately, 687 articles were excluded and 119 were considered eligible for inclusion in this meta-analysis. The final articles included consisted of 68 articles (12 in the GA group, 56 in the LA group) (Figure 1). These 68 articles included a total of 5189 patients (724 GA, 4465 LA). Descriptive data related to the included articles is presented in Table 1. The risk of bias as assessed with the Newcastle-Ottawa Scale is summarized in Table 2. Flow diagram depicting the literature review, search strategy and selection process. Study Characteristics – Primary Surgical Outcomes and Operative Data. RCT – randomized control trial. aPer Grading of Recommendations Assessment, Development and Evaluation (GRADE) criteria. Assessment of the Quality of Included Studies According to the Newcastle-Ottawa Quality Assessment Scale.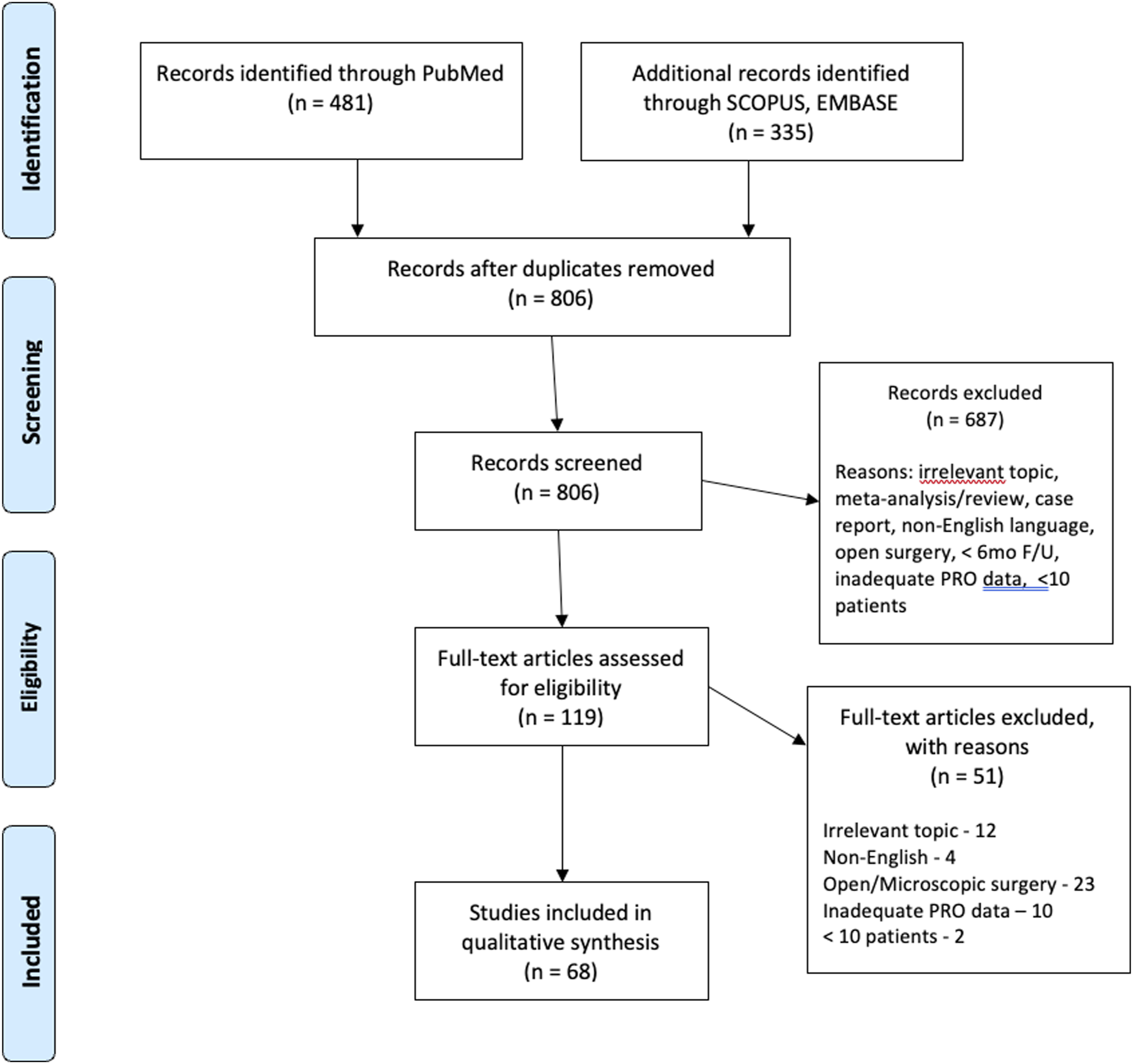
Baseline Data
Baseline Age and Patient-Reported Outcomes.
Overall Complications
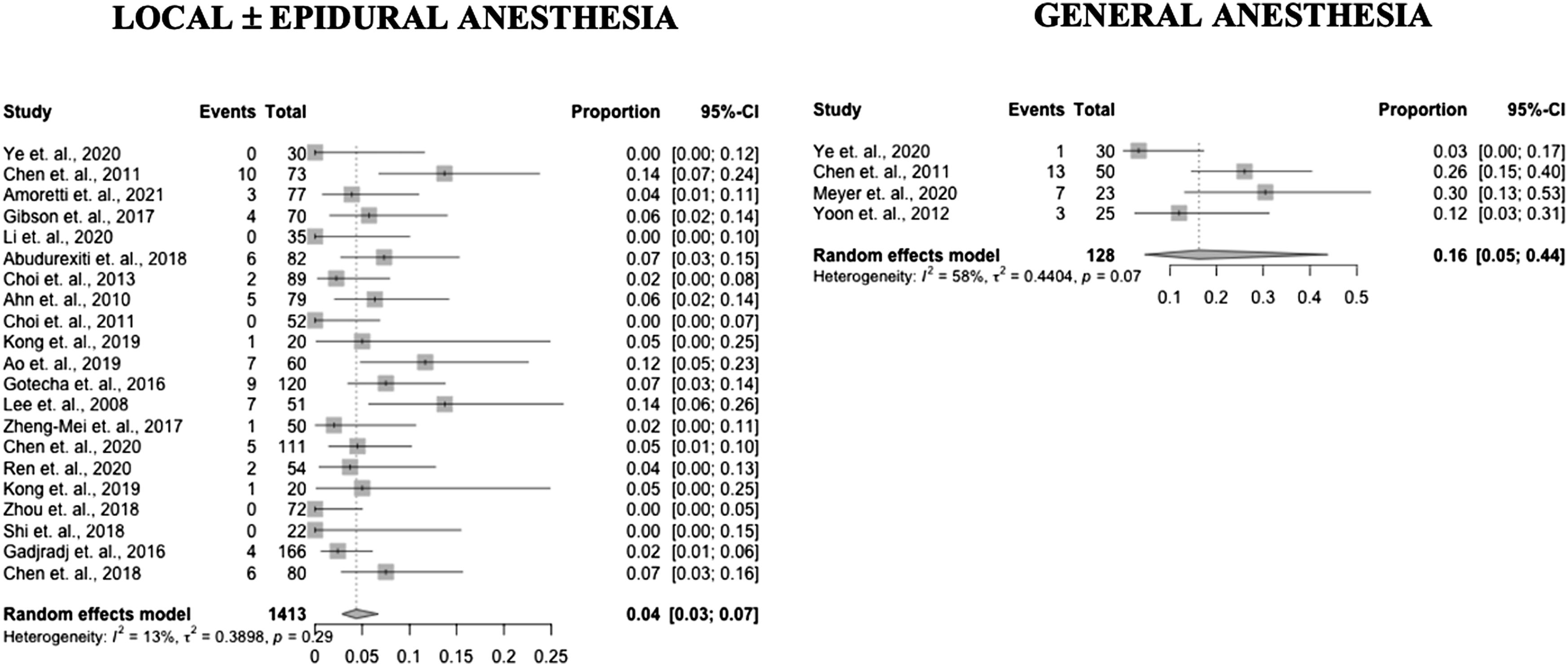
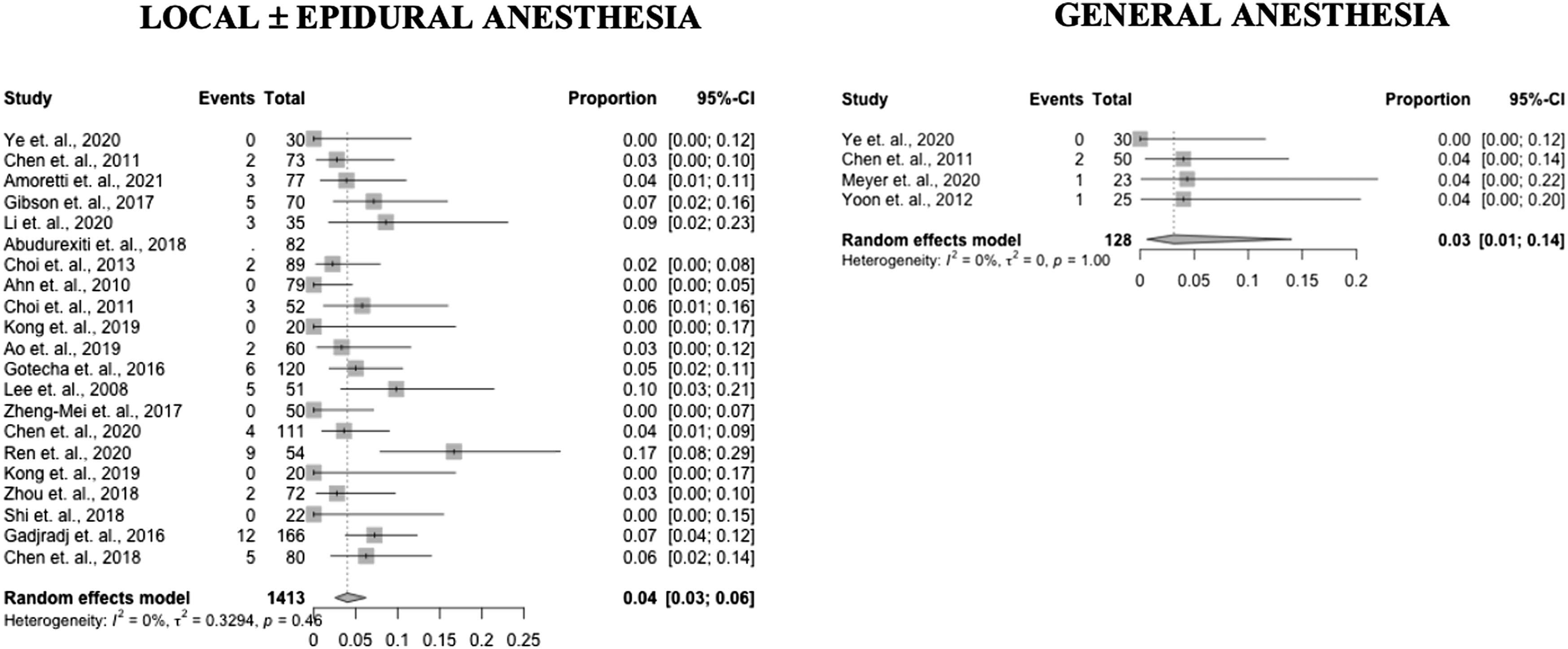
Sixty-three studies reported data on complications (12 GA – 100%, 51 LA – 91%). The complication incidence was .09 (95% confidence interval [CI] .06 – .15) in the GA group and .04 (95% CI .03 – .06) in the LA group (P = .003). These results are presented in Figure 2 as forest plots. Forest plots of complication incidence in PELD with GA and LA.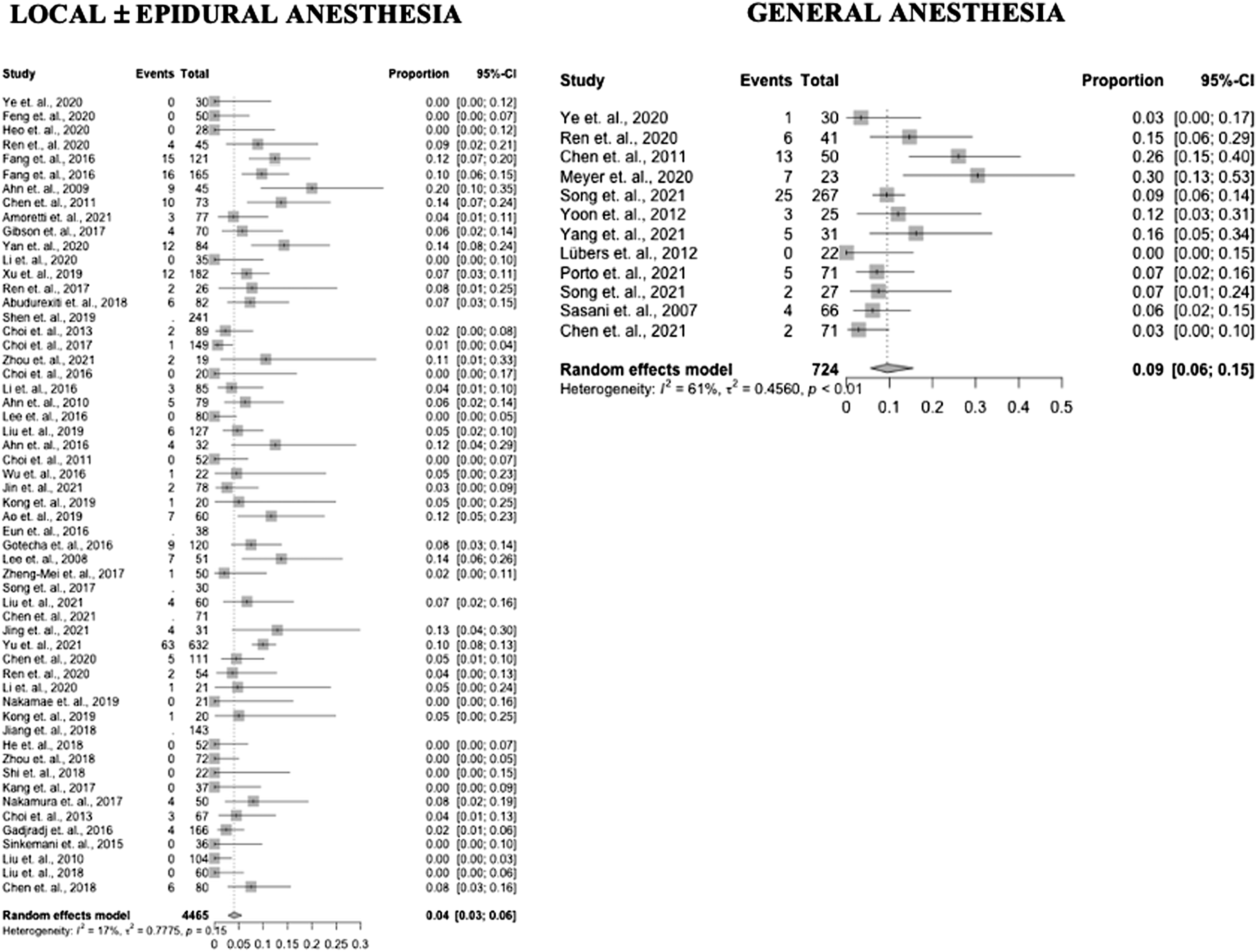
Durotomy
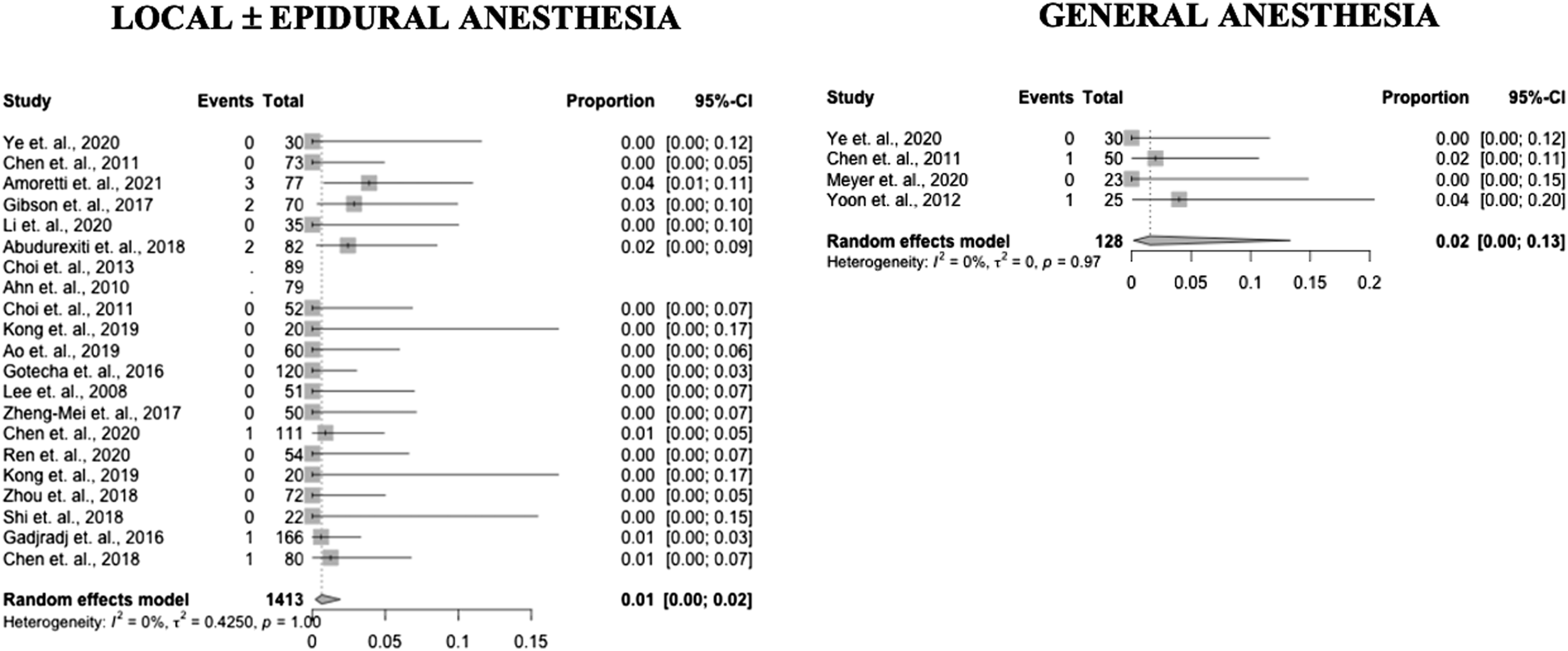
Fifty-nine studies reported data on durotomy incidence (10 GA – 83%, 49 LA – 88%). Durotomy incidence in the GA group was .007 (95% CI .001 – .03) and .006 (95% CI .003 – .01) in the LA group (P = .86). Results by study are presented in Figure 3 as forest plots. Forest plots of durotomy incidence in PELD with GA and LA.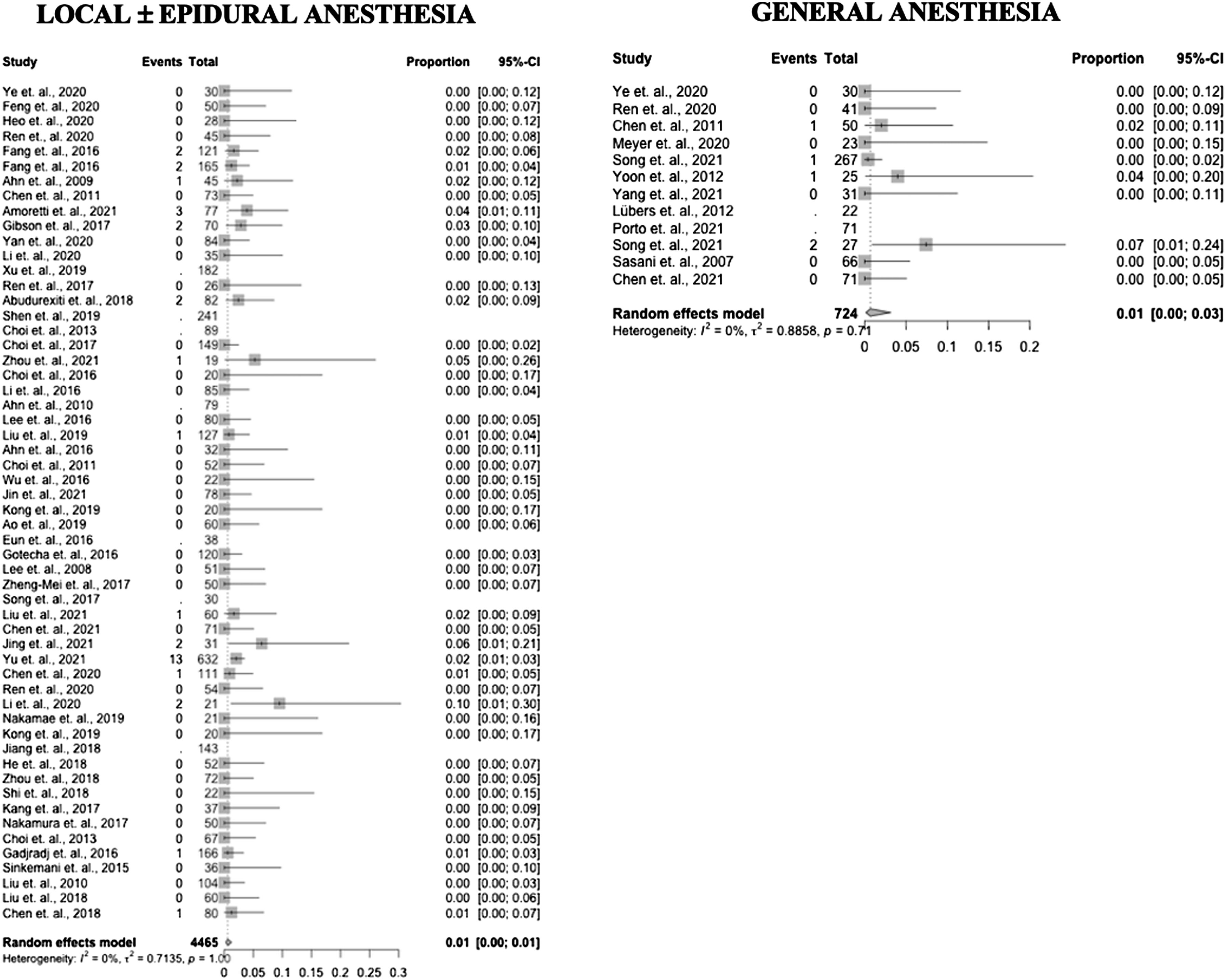
Recurrent Disc Herniation
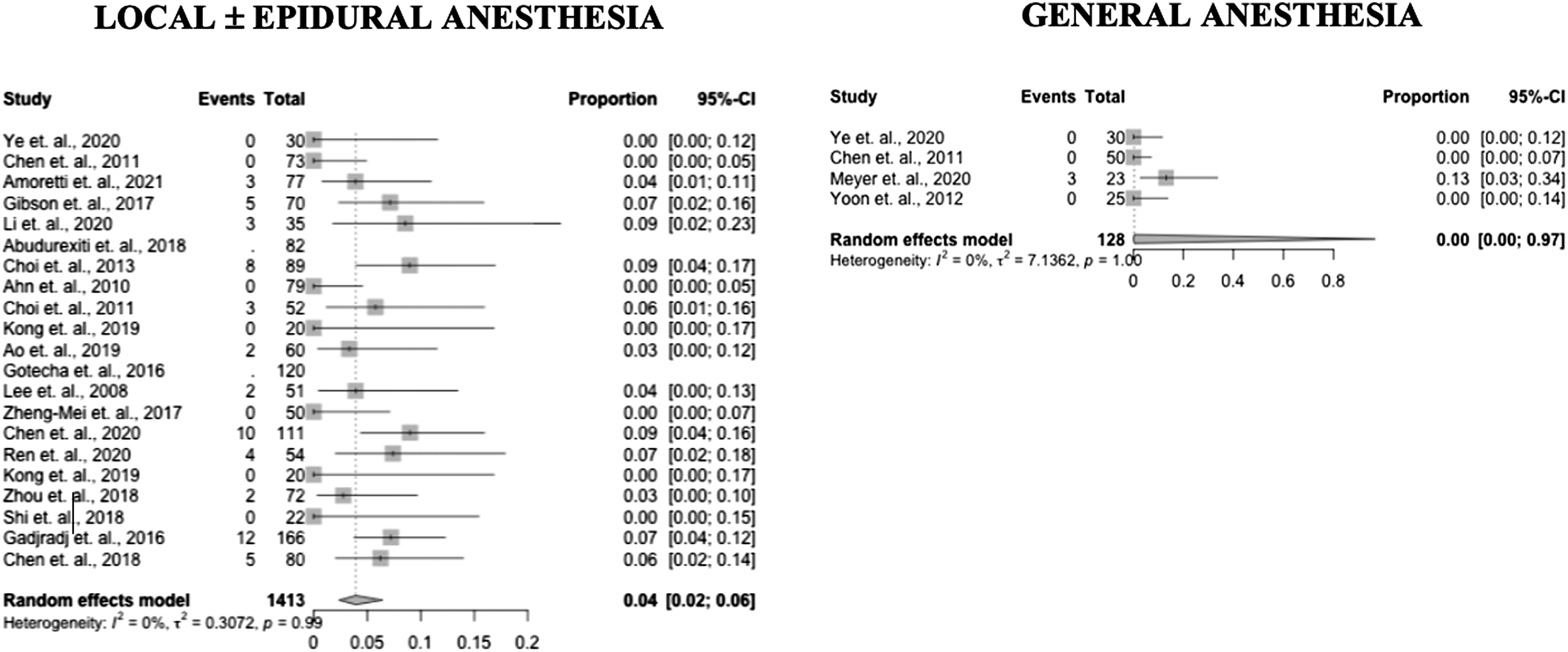
Sixty studies reported data on recurrent disc herniation incidence (10 GA – 83%, 50 LA – 89%). Recurrent disc herniation incidence in the GA group was .06 (95% CI .02 – .13) and .02 (95% CI .02 – .04) in the LA group (P = .06). Results by study are presented in Figure 4 as forest plots. Forest plots of recurrent disc herniation incidence in PELD with GA and LA.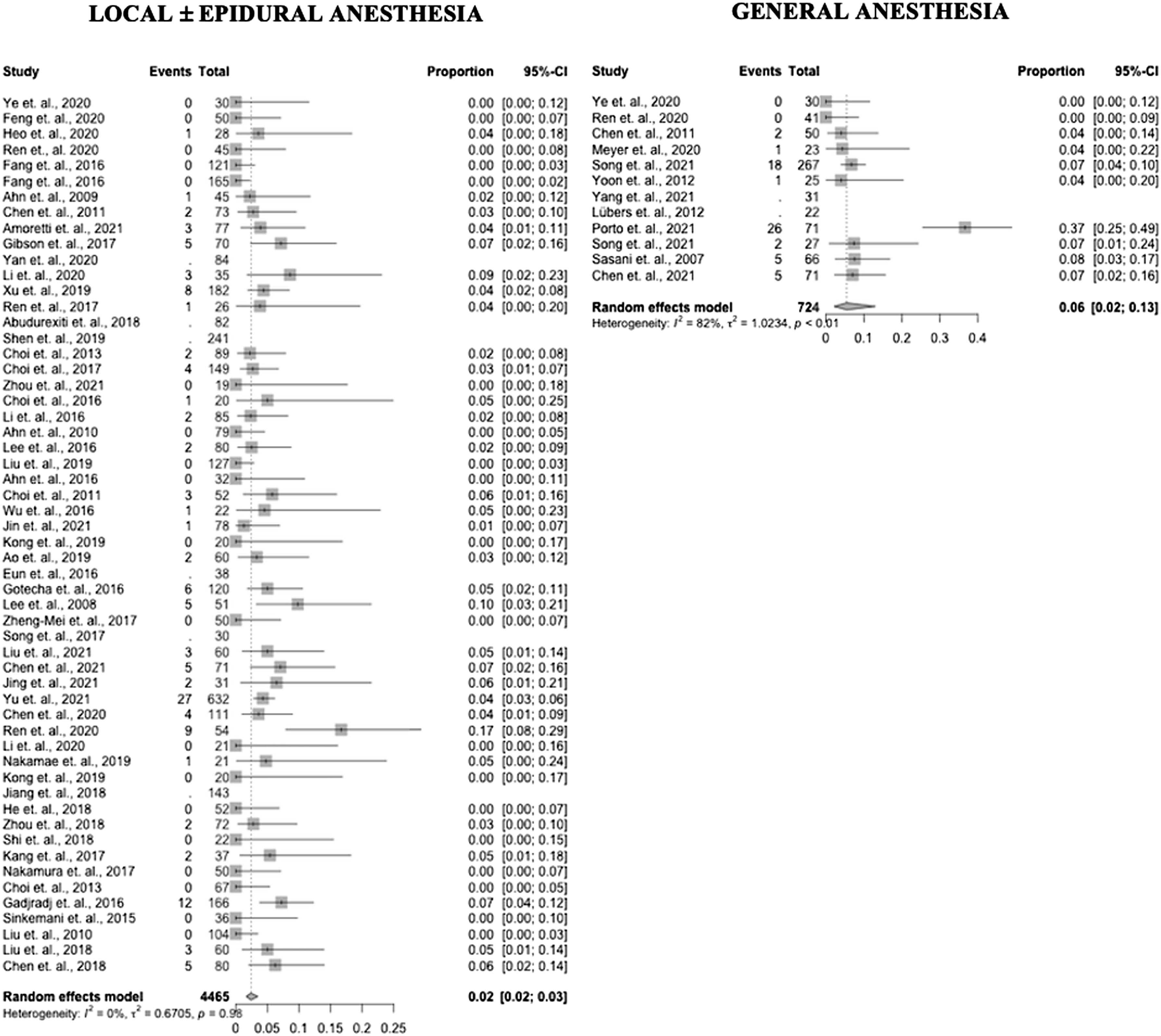
Reoperations
Fifty-five studies reported data on reoperation incidence (8 GA – 67%, 47 LA – 84%). Reoperation incidence in the GA group was .03 (95% CI .004 – .18) and .02 (95% CI .01 – .03) in the LA group (P = .74). Results by study are presented in Figure 5 as forest plots. Forest plots of reoperation incidence in PELD with GA and LA.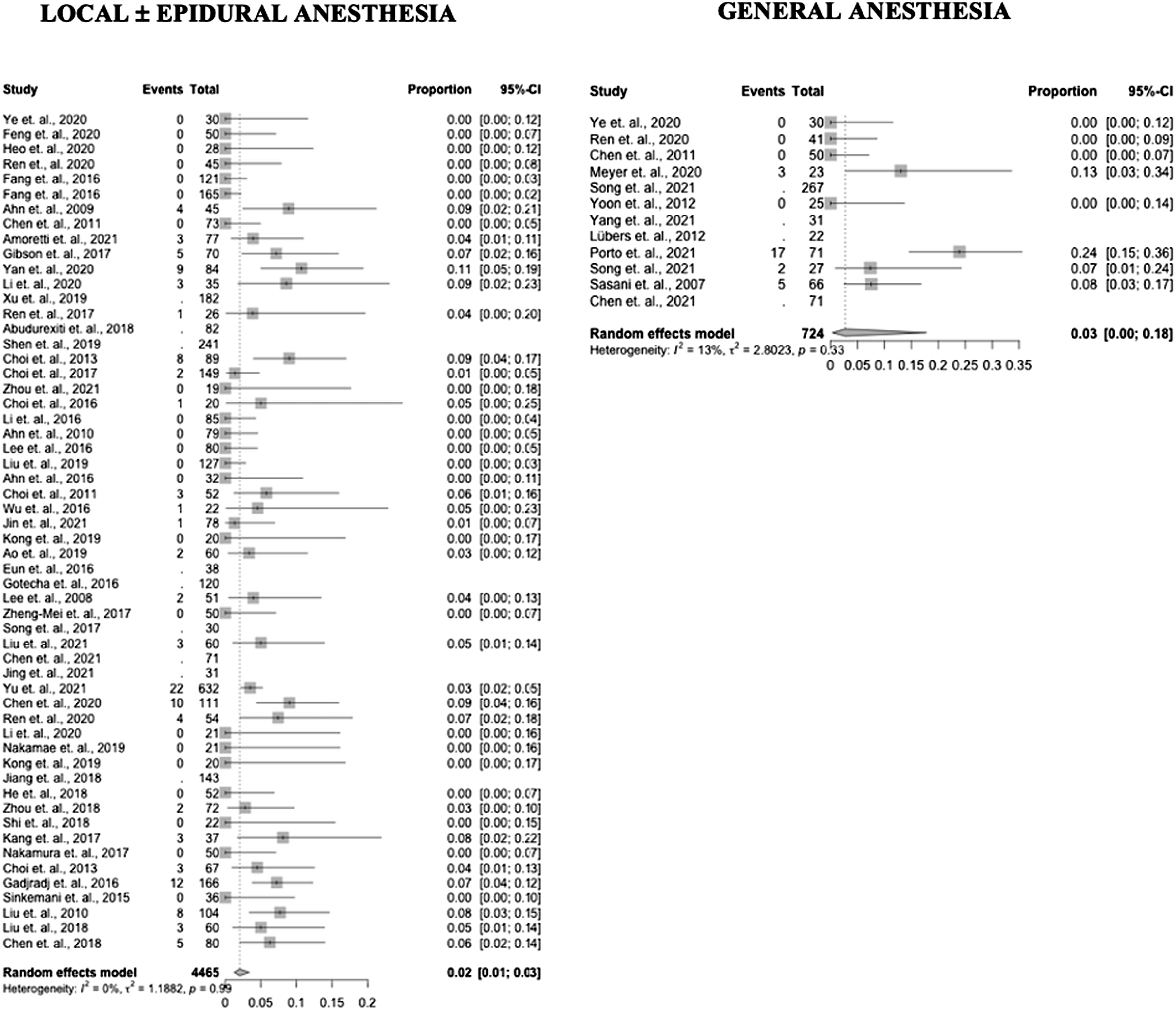
Operative Data
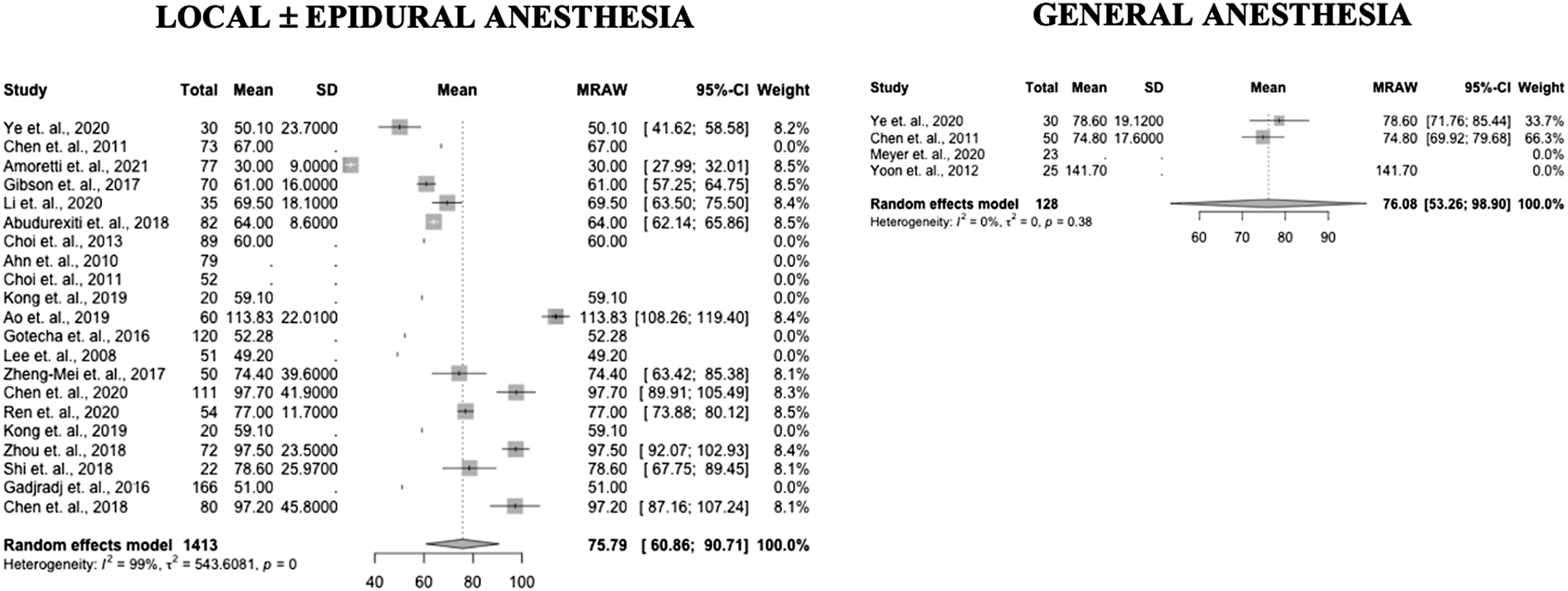
Thirty-eight studies reported data on length of surgery (7 GA – 58%, 31 LA – 55%). Length of surgery in the GA group was 65 minutes (95% CI 53 - 78) and 75 minutes (95% CI 67 - 82) in the LA group (P = .14). Results by study are presented in Figure 6 as forest plots. Eleven studies (1 GA – .5%, 10 LA – 18%) reported data on blood loss. Blood loss in the GA group was 11cc (95% CI 10 - 12) and 19cc (95% CI 11 - 28) in the LA group (P = .03). Forest plots of length of surgery in PELD with GA and LA.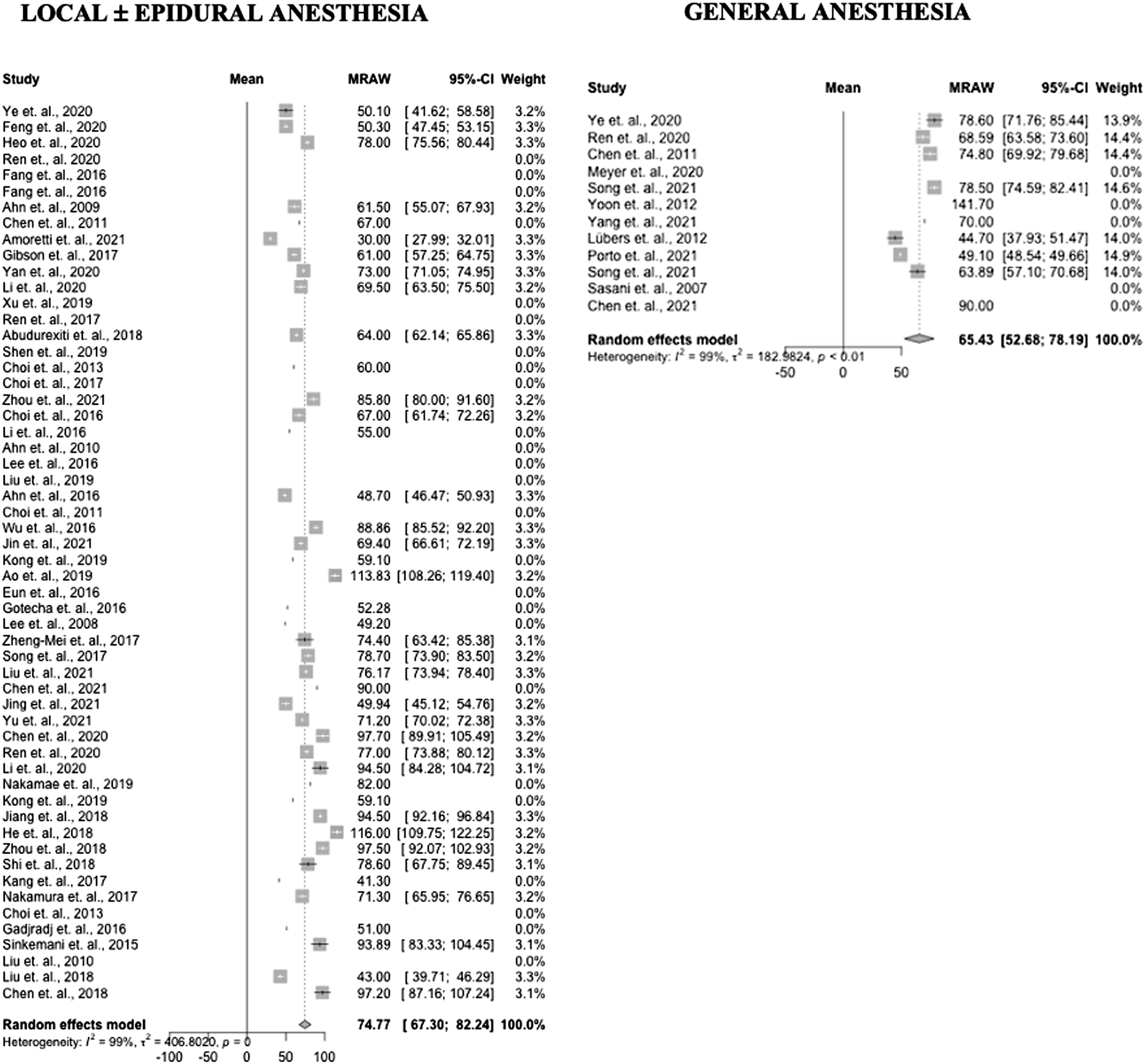
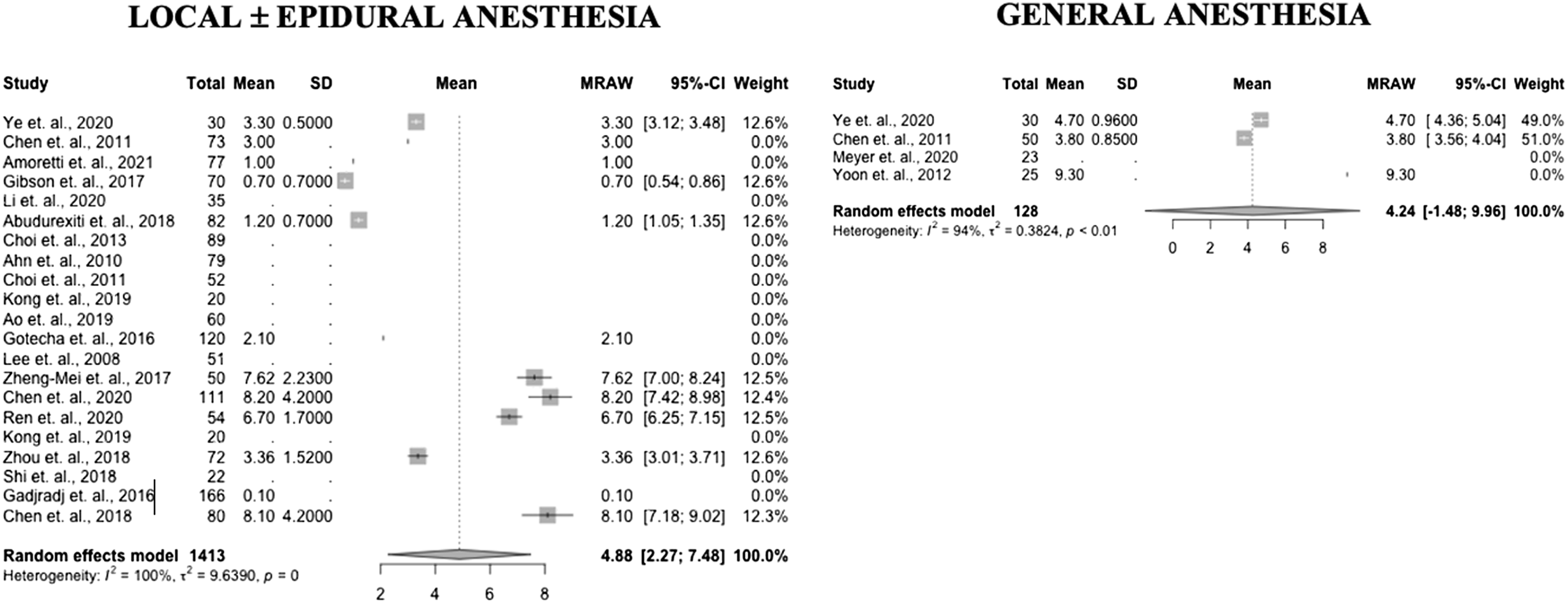
Patient Reported Outcomes
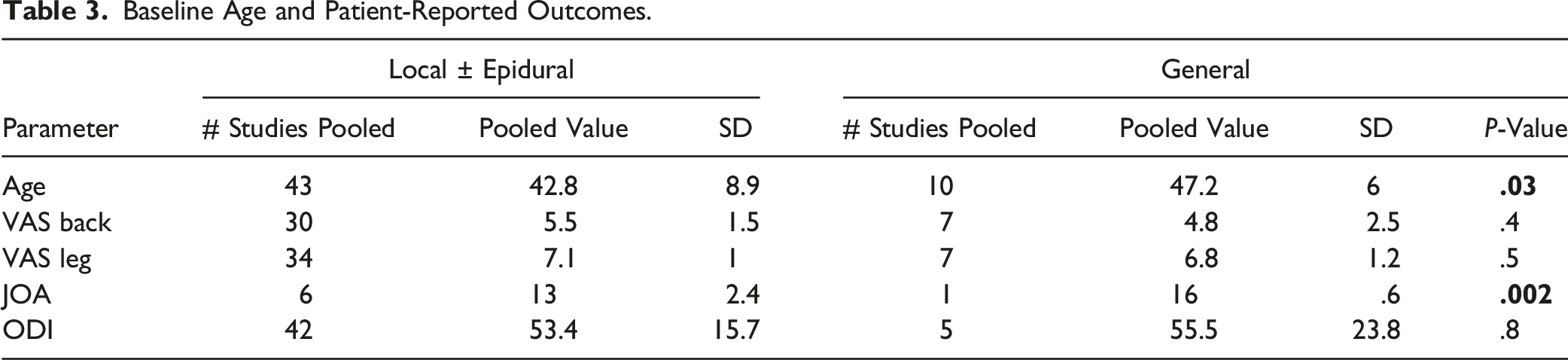
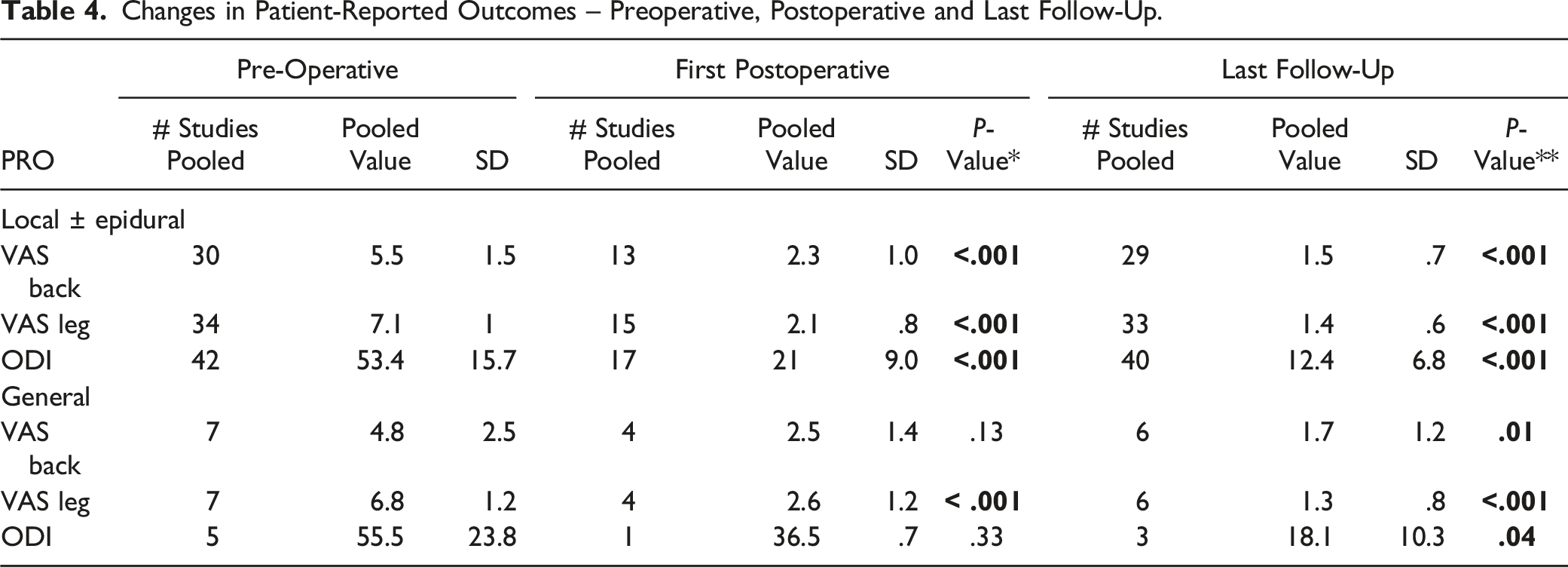
The greatest number of studies presented data on VAS back (37 studies: 7 GA – 58%, 30 LA – 54%) VAS leg (41 studies: 7 GA – 58%, 34 LA – 61%) and ODI scores (47 studies: 5 GA – 42%, 42 LA – 81%). Pre-operative VAS back, leg, and ODI scores were similar between the GA and LA groups. Seven studies (1 GA – 8%, 6 LA – 11%) reported JOA scores which overall were higher in the GA group pre-operatively (16 vs 13, P = .002) (Table 3).
Changes in Patient-Reported Outcomes – Preoperative, Postoperative and Last Follow-Up.
Twenty-three studies reported McNab scores at follow-up > 6 months (19 LA – 34%, 4 GA – 33%). At the final post-operative follow-up, the percent of patients achieving an excellent McNab score was significantly higher in the GA vs LA group (62% vs 20%, P < .001).
Subgroup Analysis (Prospective and RCT Studies)
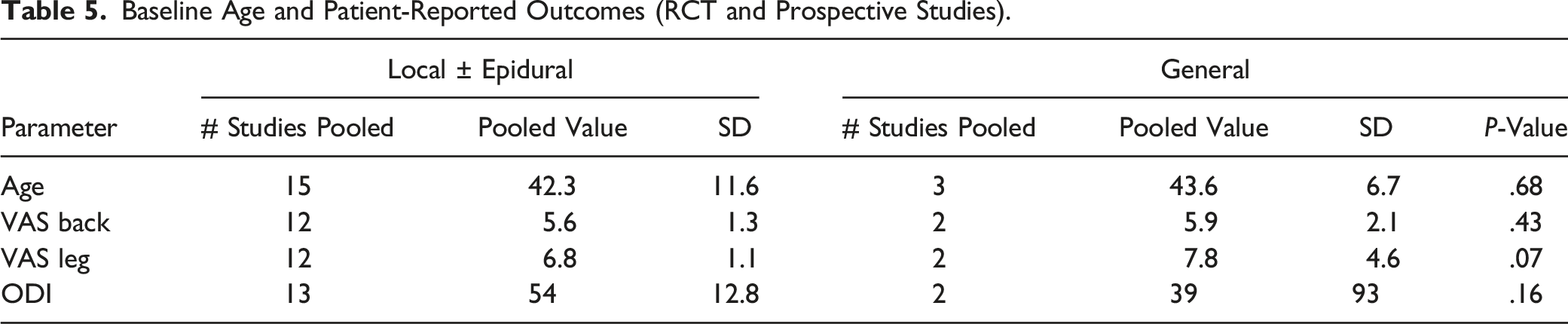
Baseline Age and Patient-Reported Outcomes (RCT and Prospective Studies).
Forest plots of complication incidence in PELD with GA and LA (Prospective and RCT studies).
Forest plots of durotomy incidence in PELD with GA and LA (Prospective and RCT studies).
Forest plots of recurrent disc herniation incidence in PELD with GA and LA (Prospective and RCT studies).
Forest plots of reoperation incidence in PELD with GA and LA (Prospective and RCT studies).
Forest plots of length of surgery in PELD with GA and LA (Prospective and RCT studies).
Forest plots of length of surgery in PELD with GA and LA (Prospective and RCT studies).
Discussion
Percutaneous endoscopic lumbar discectomy is commonly performed under LA which has been reported to reduce the risk of nerve injury.14,15 Pain experienced by the patient during PELD under LA; however, can pose various challenges to successfully completing the operation. Percutaneous endoscopic lumbar discectomy under GA has thus been reported as an alternative to keep patient’s more comfortable; however, may pose an increased risk of neurologic injury as patients are unable to provide feedback during the surgery.16,17
The present study demonstrated that the use of GA was associated with a higher percentage of patients achieving an excellent McNab score at final follow-up. Both GA and LA groups demonstrated significant improvement in VAS and ODI scores at the final follow-up. At the first post-operative follow-up, however, the GA group only demonstrated improvement in VAS leg score while the LA group demonstrated improvements in all PROs. Prior study has demonstrated that PELD under GA results in greater post-operative dysesthesias, possibly due to greater nerve root manipulation with lack of patient feedback compared to LA. 18 This could partially explain the non-significant improvement in ODI scores seen at the first follow-up timepoint in the GA group. Lower post-operative cognitive function resulting from GA use as noted by Ye et al may also contribute to ODI scores. 19 The higher percent of patients achieving an Excellent McNab score in the GA group may indicate that PELD performed under GA confers a more sustained benefit for the treatment of radiculopathy through providing the surgeon with increased ability to adequately mobilize nerve roots for inspection of residual disc material. The ability to achieve optimal decompression may be limited due to patient discomfort with the use of LA.
Overall complication rate of PELD under GA was significantly higher than PELD under LA in our analysis. This remained true when examining higher quality prospective and RCTs in subgroup analysis. Prior literature has demonstrated conflicting evidence regarding the effects of GA and LA on post-operative complications including nerve injury and dysesthesias. Exiting nerve root injury for PELD under LA are variably reported between 1-6.7%.20-24 However, one study by Choi et al in 2013 noted a slightly higher rate of 8.9% in a retrospective study of 233 patients. 25 These findings highlight the value of patient cooperation/feedback during PELD with LA.
There is a paucity of literature assessing the use of GA with PELD. The first report comparing PELD under GA vs LA was published in 2011 by Chen et al nothing that both techniques achieve good outcomes and high patient satisfaction. 18 However, the authors concluded that the use of LA was more favorable given the ability for patient feedback, less post-operative dysesthesia and shorter hospital stay. Ye et al in a randomized controlled trial comparing the effects of GA and LA in lumbar interlaminar endoscopic surgery also found shorter hospital stays and operative times with LA and no differences in ODI or VAS scores between groups. 26 These authors concluded that GA makes a positive intraoperative surgical experience more likely. Supporting our finding of a higher complication rate with PELD under GA, Ren et al demonstrated a complication rate of 14.6% for PELD patients undergoing GA vs 8.9% for those undergoing EA. 12 Similarly, Chen et al reported a 24% rate of post-operative transient paresthesias in patients undergoing PELD under GA compared to 14% of those with LA, while Ye et al report no differences in neurologic complications between GA and LA groups.27,28
Overall, the present analysis is consistent with several other reports in that both anesthetic methods achieve good patient outcomes long term. The risk of short-term complications resulting from the use of GA must be balanced against the risk of patient discomfort with the use of LA. The decision to pursue either anesthetic technique should be made on a case by case basis taking into account patient preferences.
Limitations
The limitations of this study are primarily related to the limited body of literature directly examining the topic. Cohorts of patients undergoing LA and GA for PELD were combined in attempt to overcome this, resulting in 68 total studies meeting the inclusion criteria. Additionally, while transforaminal and interlaminar PELD have distinct differences based on their approaches, these were combined due to the failure of many studies to distinguish between the approaches in their cohorts. Next, outcomes assessed were not present uniformly across all studies leading to underpowered metrics in several categories. While several RCTs were included, the majority of included studies were retrospective or case-control designs of poor quality. Subgroup analysis using only the higher quality prospective and RCT studies was performed to attempt to overcome this limitation. Significant heterogeneity within and between groups limits the strength of our conclusions. Additionally, studies of varying design were combined to generate the greatest amount of data for analysis, potentially limiting the strength of conclusions. Included studies constituted a wide-range of international locations, resulting in significant variation in patient assessment and outcome measurements. Primary outcomes were thus chosen based on those reported in the greatest number of studies and felt to be the most objective. The present study design is also limited by the inability to control for biases inherent to the use of GA vs LA for PELD. It is possible GA patients may have had more complex conditions warranting the use of GA that may have affected their outcomes. Despite these limitations, this is the first systematic review and meta-analysis on the topic of anesthetic use in PELD and generates several novel hypotheses that are worthy of further investigation.
Conclusions
The use of GA may carry a slightly higher rate of short-term (resolving within 1 month) complications including nerve root injuries and post-operative dysesthesias but may result in more sustained benefits with a greater percentage of patients achieving an Excellent McNab score at final follow-up. Both groups demonstrated significant improvements in all PROs at the final follow-up; however, LA may be associated with greater short-term improvement in disability scores. These conclusions are limited by a high level of study bias and heterogeneity and further systematic investigation is necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.