
Abstract
Study Design
A retrospective matched case–control study.
Objective
This study aims to investigate the value of Subcutaneous Lumbar Spine Index (SLSI) as a predictor of early surgical site infection (SSI) after lumbar intervertebral fusion surgery.
Methods
A retrospective case–control study was performed on patients who underwent transforaminal lumbar interbody fusion (TLIF) from January 1, 2014 to December 31, 2019 in a single institution. Cases were defined as those who developed early SSI according to the US Center for Disease Control and Prevention criteria, and controls were matched from those patients without early SSI using the following matched criteria: gender, age, time of surgery and diabetes. Subcutaneous fat thickness (SFT) and SLSI were measured on preoperative MRI mid-sagittal T2 weighted images.
Results
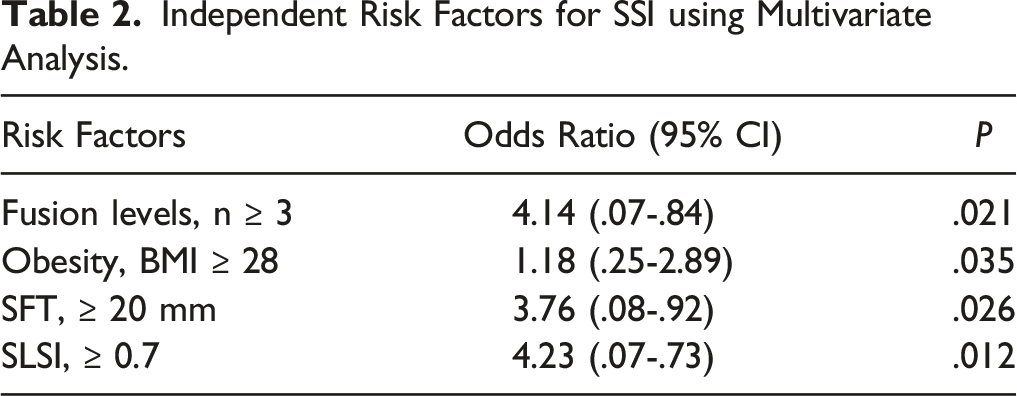
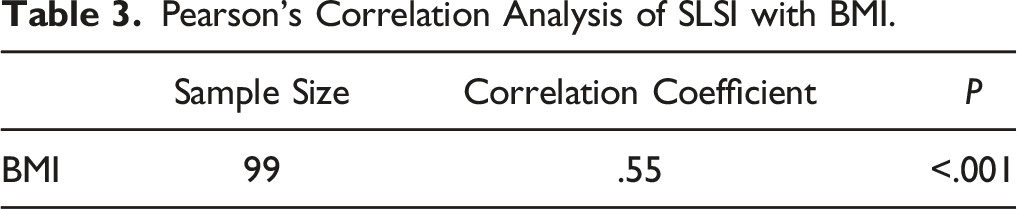
A total of 3615 patients who underwent TLIF were enrolled in this study. Thirty-three patients were included in early SSI, and sixty-six patients were selected as matched controls. Univariate analysis indicated that fusion levels (P = .007), operation time (P = .022), obesity (P = .013), SFT (P = .002) and SLSI (P = .001) were significantly associated with early SSI. Multiple logistic regression analysis revealed that multilevel fusion levels (P = .021), obesity (P = .035), a large SFT (P = .026) and a high SLSI (P = .012) were independent risk factors. Body mass index (BMI) and SLSI were moderately correlated (r2 = .55). ROC curve demonstrated that SLSI was more sensitive than SFT to predict the early SSI.
Conclusion
SLSI is a novel radiological risk factor for early SSI development and is a better indicator than SFT to predict early SSI risk after lumbar intervertebral fusion.
Introduction
Surgical site infection (SSI) is a common complication in lumbar intervertebral fusion. 1 Although most patients were given prophylactic antibiotics and aggressive wound care within perioperative period, early SSI still occurred frequently and influenced patient prognosis, such as prolonged the time of hospitalization and increased medical cost.2-4 Some researchers had found some risk factors were associated with early SSI development, such as obesity, poor nutritional status, multilevel segment surgery, smoker, diabetes, longer operative time, and high lumbar subcutaneous fat thickness (SFT).5-8
BMI is always described a risk factor for SSI in TLIF.9,10 However, it neither takes into account body mass distribution nor distinguishes fat from muscle. 11 Afterwards some researchers proposed that lumbar subcutaneous fat thickness was associated with early SSI in lumbar spine surgery.12,13 Lee et al 12 reported that every 1-mm thickness of subcutaneous fat there was a 6% increase in the odds of surgical site infection. This measurement ignored the effect of spinous process and some patients with normal fat thickness, but shorter spinous process also had a high infection rate at the surgical site. Shaw et al 14 considered BMI and subcutaneous fat thickness were unable to epitomize the variability of adipose distribution and proposed subcutaneous lumbar spine index (SLSI) which quantified the relationship between lumbar SFT and spinous process height (SPH).
In this study, we performed a retrospective, matched case-control study to investigate that SLSI is a better predictor than lumbar SFT for developing early SSI after lumbar fusion surgery.
Materials and Methods
Demographic Data
A retrospective review retrieved all patients who underwent TLIF in our hospital from January 1, 2014 to December 31, 2019. The criteria for exclusion: patients less than 18 years of age; patients diagnosed with spinal tuberculosis, tumors, infection, a gross deformity of the spine or revision surgery. Finally, 3615 patients were enrolled in this study and 33 patients were identified as having early SSI within 30 days. All patients in this study obtained informed consent before surgical procedures.
Identification of SSI
SSI was identified as microbiology, operative and hospital records, laboratory reports, and infection symptoms (such as fever, increased pain, incision erythema, swelling or purulent secretion) according to the Centers of Disease Control (CDC) and Prevention definition. 15 we defined early SSI as infection developing within 30 days after surgery in this study.
Matching
A matched case-control design was conducted due to the low incidence of SSI. Infection groups were defined as patients who occurred early SSI, and controls were matched from people without early SSI according to the following criteria: age (±3 y), gender (male or female), diabetes (yes or no), timing of surgery (morning or afternoon).
Data Collection and Evaluated
General demographic data including age, gender, diabetes and time of surgery were collected. After successfully matching controls, body mass index (BMI), number of fusion levels, operative time and volume of drainage were recorded, lumbar SFT and spinous process height (SPH) at the operated levels were measured using preoperative MRI mid-sagittal T2 weighted images. The average value represented SFT and SPH in surgery levels. The SLSI was defined as the SFT:SPH ratio according to the method Shaw used (Figure 1). The measurements of lumbar subcutaneous fat thickness (SFT) and spinous process height (SPH) at the operated levels (excluding S1) on T2 midsagittal MRI. A: 3 fusion levels. B: 1 fusion level. SFT= (SFT1+SFT2…+ SFT n)/n. SLSI= (SFT1/SPH1+ SFT2/SPH2…+ SFT n / SPH n)/n.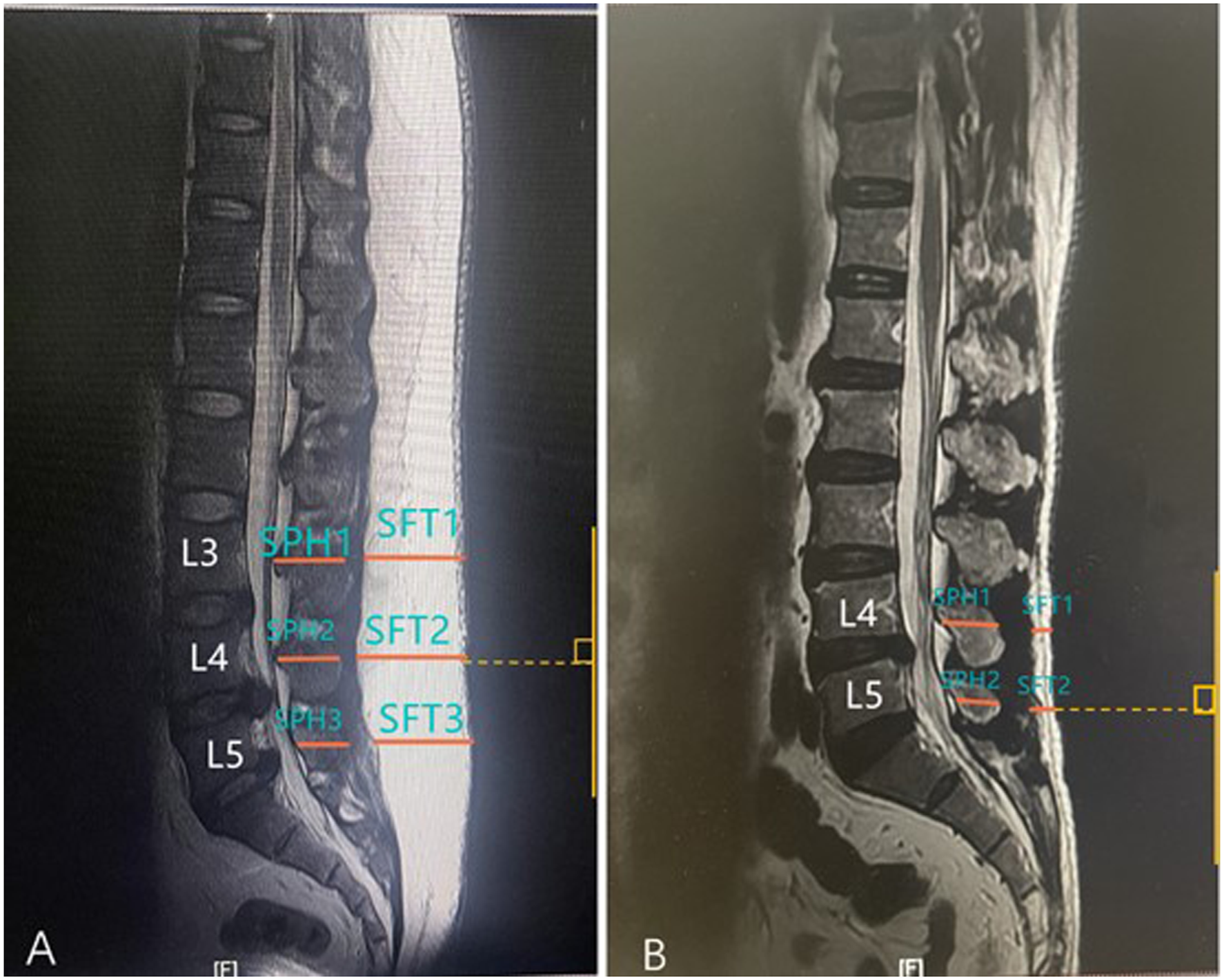
Surgical Method
All surgeries were performed by the same surgical team with an experience of more than 500 TLIF procedures. All patients were under general anesthesia and in a prone position. The skin entry point was located posterior median line. All surgical procedures contained pedicle screw implantation, decompression, lumbar discectomy, and cage filled with bone for interbody fusion. Antibiotics (cefazolin or clindamycin) were given half an hour before surgery and repeated twice 24 hours after surgery.
Statistical Analysis
Data were analyzed using SPSS Statistics 20 (IBM Corporation, Armonk, NY, USA). Univariate analysis was performed using Student’s t test and Chi-squared test. Multivariate logistic regression analysis was performed to conform the independent risk factors for early SSI. Pearson’s correlation analysis was used to assess the correlation between BMI and SLSI. Receiver operating characteristic (ROC) curve analysis was performed to predict the sensitivity of early SSI between SFT and SLSI. AP value <.05 was considered as statistically significant.
Results
General Demographic Data
A total of 3615 patients who underwent TLIF were enrolled in this study, and 42 patients were identified early SSI, 9 cases were excluded due to no preoperative MRI or general demographic data. Therefore, 33 early SSI cases (14 superficial infection, 19 deep infection) were included in analysis. The incidence of early SSI was 1.2% (42/3615). As matched controls, 66 patients were selected from the rest of 3573 non-SIS patients according to the matched criteria. Among 33 cases of early SSI, 5 cases were positive for Staphylococcus aureus, 3 caused by Escherichia coli, 3 caused by Staphylococcus epidermidis, 1 Acinetobacter baumannii and 1 Klebsiella pneumoniae.
General Demographic Between Cases and Matched Controls.
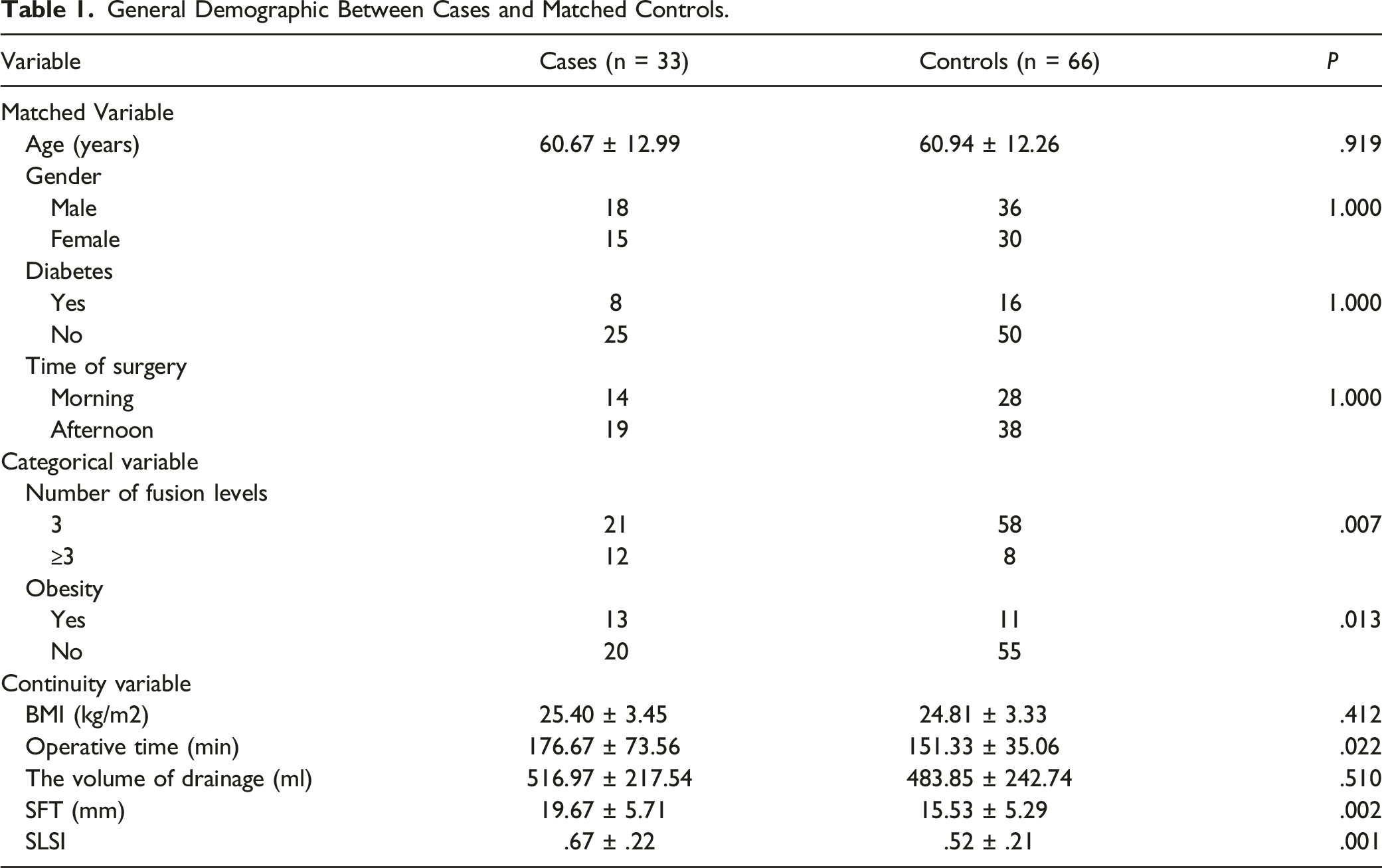
There were no significant differences in age (P = .919), gender (P = 1.000), diabetes (P = 1.000), time of surgery (P = 1.000), BMI (P = .412) and volume of drainage (P = .510) between two groups. number of fusion levels (P = .007), obesity (P = .013), operative time (P = .022), SFT (P = .002) and SLSI (P = .001) were significantly related to early SSI. Figure 2 showed the range of SLSI for cases and controls (the outliers had no influence on the results) Figure 3. The range of SLSI demonstrated for cases and controls. Five outliers had no influence on the results. ROC curve of lumbar SFT and SLSI to Predict SSI after lumbar fusion surgery.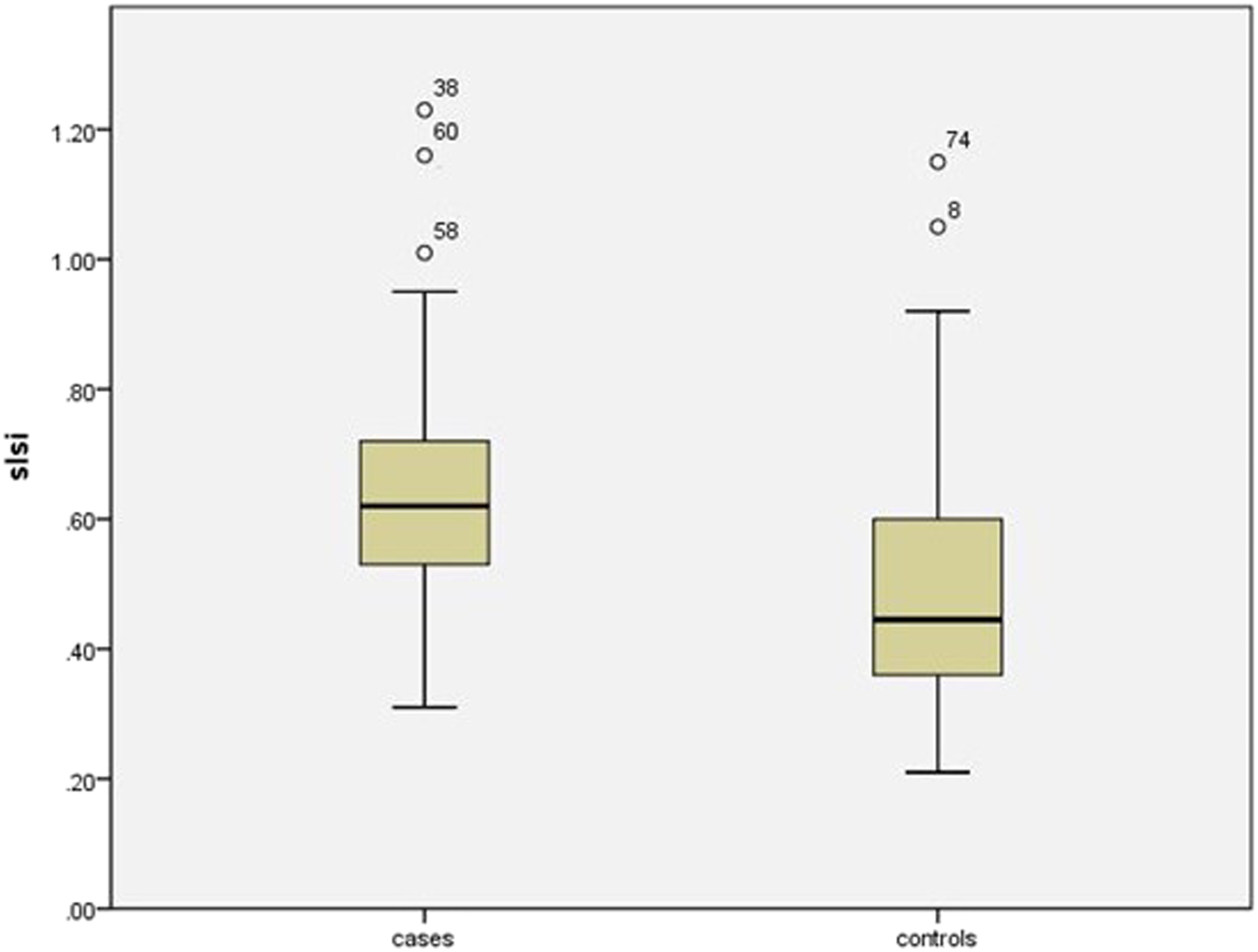
Multivariate Logistic Regression Analysis of Risk Factors for SSI
Independent Risk Factors for SSI using Multivariate Analysis.
Pearson’s Regression Analysis of the Association of SLSI With BMI
Pearson’s correlation analysis revealed that SLSI was moderately correlated with BMI (r2 = .55, P < .001).
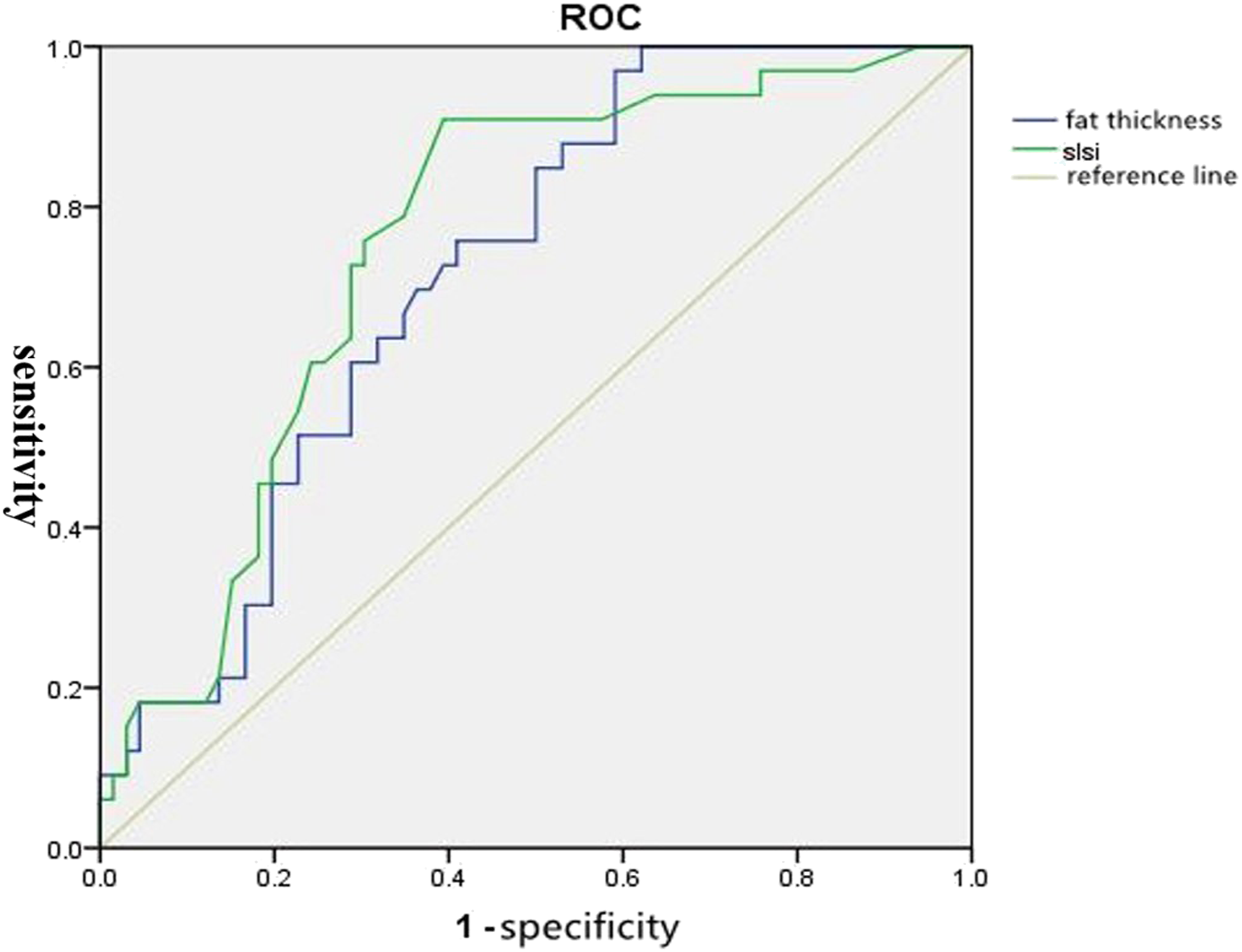
ROC Curve of Lumbar SFT and SLSI to Predict SSI After Lumbar Fusion Surgery
Pearson’s Correlation Analysis of SLSI with BMI.
Discussion
SSI is one of the most frequent complications following lumbar fusion surgery which can prolong the hospitalization days and increase financial burden, even physician-patient disputes.4,16,17 The SSI rate of Lumbar spine surgery has been reported at 1-12%.18-20 In this study, the incidence of early SSI was 1.2%. This is a lower infection rate because we adopted effective perioperative management, such as controlled blood sugar level, appropriate drainage and removal particularly, when drainage volume became less than 50 ml 21 Among early SSI group, bacterial culture of the aspirate was positive in 13 (39%). Previous literature reported culture results was not a prerequisite for early SSI. 22
However, BMI may not accurately represent body weight distribution, because muscle mass can increase weight and result in a higher BMI. A few studies proposed SFT as an evaluation criterion for lumbar fat mass and was a better indicator than BMI.11,12,23 Whereas few studies reported the effects of spinous process height during lumbar spinal surgery. As a result, we performed a retrospective, matched case-control study to explore the correlation between SLSI and early SSI.
In this study, we demonstrated that the ratio of subcutaneous fat thickness in relation to spinous process height was a significant risk factor for early SSI. The linear regression of the data showed BMI may be related to its moderate correlation with SLSI in the surgical site (r2 = .55). This indicated patients had a higher BMI but did not imply high SLSI.
During lumbar fusion surgery, a higher SLSI portended a thicker subcutaneous fat or a shorter spinous process which resulted in exposing difficultly, decreasing blood flow and increasing tissue necrosis.24,25 Operative time and lumbar paravertebral muscle tension are also extended in these patients because of deeper dissection. In addition, the thick subcutaneous fat and short spinous process increased the difficulty of surgery and needed more tissue exposure using electrotome which may lead to fat necrosis. 26 At last, patients with a higher SLSI had a deeper incision which increased the risk of development of a large dead space formation after wound closure. 14
This study invested that the thickness of subcutaneous fat and SLSI were the risk factors for incision infection after lumbar fusion surgery. ROC curve analysis revealed that a higher SLSI in the surgical site was more accurate indicator than SFT for early SSI. In addition, multilevel fusion levels (≥3) and obesity were risk factors for incision infection after lumbar spine surgery, which is comparable with previous researches.7,27,28 The more surgical segments needed the longer exposure time of tissue, and thus the exposure of the surgical incision to the air, which increased the possibility of tissue ischemic necrosis and mechanical damage and increased risk of early SSI. 28
There are several limitations in this study. First, the SSI group had a relatively small sample size. In addition, not all known risk factors for early SSI were included in the present analysis. Furthermore, there are 5 outliers in our study, which had no influence on the results and were included in statistical analysis. Therefore, a prospective study with larger number of SSI cases is necessary to validate this result of SSI after lumbar fusion surgery in the future.
Conclusion
BMI is related to its moderate correlation with SLSI in the surgical site, SLSI is a novel radiographic risk factor for early SSI after lumbar fusion surgery and provides a more precise assessment of the risk of early SSI than lumbar SFT. This index can be used to predict patients of their risk of early SSI and to formulate strategies to minimize this risk.
Footnotes
Author Contribution
Conception and design: Zengxin Gao.
Acquisition of data: Xu Shen, Yu-lei Qian, Yucheng Gao, Pei Zhang
Analysis and interpretation of data: Xu Shen, Yulei Qian, Yucheng Gao, Wenbin Xuan, Lei Zhu.
Drafting the article: Xu Shen, Hang Shi
Critically revising the article: Pei Zhang, Zengxin Gao, Zanli Jiang.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical Approval
All patients in this study obtained informed consent before surgical procedures. The study was performed in compliance with ethical standards and was approved by the institutional review board. The IRB approval number (2021ZDYLL051-P01)