
Abstract
Study Design
Retrospective.
Objectives
To report and compare the application of robotic-assisted navigation with an O-arm or three-dimensional (3D) C-arm-assisted pedicle screw insertion in scoliosis surgery, and compare with free-hand technique.
Methods
One hundred and forty-four scoliosis patients were included in this study. Ninety-two patients underwent robotic-assisted pedicle screw insertion (Group A), and 52 patients underwent freehand fluoroscopy-guided pedicle screw insertion (Group B). Group A was further divided into Subgroup AI (n = 48; robotic-assisted navigation with an O-arm) and Subgroup AII (n = 44; robotic-assisted navigation with a 3D C-arm). The evaluated clinical outcomes were operation time, blood loss, radiation exposure, postoperative hospital stay, and postoperative complications. The clinical outcomes, coronal and sagittal scoliosis parameters and the accuracy of the pedicle screw placement were assessed.
Results
There were no significant differences in blood loss and postoperative hospital stay between Groups A and B (P = .406, P = .138, respectively). Radiation exposure for patients in Group A (Subgroups AI or AII) was higher than that in Group B (P < .005), and Subgroup AI had higher patient radiation exposure compared with Subgroup AII (P < .005). The operation time in Subgroup AII was significantly longer than that in Subgroup AI and Group B (P = .016, P = .032, respectively). The proportion of clinically acceptable screws was higher in Group A (Subgroups AI or AII) compared with Group B (P < .005).
Conclusions
Robotic-assisted navigation with an O-arm or 3D C-arm effectively increased the accuracy and safety in scoliosis surgery. Compared with robotic-assisted navigation with a 3D C-arm, robotic-assisted navigation with an O-arm was more efficient intraoperatively.
Introduction
Scoliosis is a common three-dimensional (3D) deformity of the spine, defined as a lateral curvature of the spine in the coronal plane, with a curve of ≥ 10° (Cobb angle measurement), often accompanied by varying degrees of spinal rotation. 1 Posterior scoliosis correction with pedicle screws has become the standard treatment for patients with severe spinal curvature, rapid progression of disease in adolescence, and neurologic symptoms. 2 However, screw placement in scoliosis surgery is challenging owing to vertebral rotation and smaller pedicle size (especially at the concave side) and a more complex 3D structure than normal. These issues increase the potential risk of screw misplacement and cause complications, such as vascular, nerve, and pleural injury.3,4 Currently, the fluoroscopy-assisted free-hand technique is the principal method for pedicle screw implantation. 5 Previous studies reported that the rate of screw malpositioning caused by free-hand pedicle screw insertion during scoliosis correction range from 1.5% to 43%.6-9 In scoliosis cases, even when the pedicles’ trajectories are predetermined and tapped correctly, screws may be inserted into the pedicles incorrectly owing to axial rotation, especially at the apical levels.
To improve pedicle screw positioning, several techniques have been developed, including navigation technologies, such as computed tomography (CT)-guided or robot-assisted technologies. Nolte et al 10 first described computer-assisted image guidance systems in 1995 as a CT-based navigation system. Subsequently, intraoperative CT, such as O-arm and 3D C-arms, were also used in spine surgery for navigation assistance. 11 O-arm navigation provides intraoperative 3D fluoroscopic imaging with an image quality similar to that of CT, and reduces the time needed for computer-assisted surgery. 12 Wolf et al 13 first reported a robotic guidance system used in spinal surgery in 2004, and robot technology has developed rapidly in recent years, which could decrease the risk of misplaced screws and the associated complications.14-16 However, limited studies have reported the application of robotic-assisted navigation using O-arm or 3D C-arm navigation in scoliosis surgery. In 2019, Gonzalez et al 17 first reported an initial intraoperative experience with robotic-assisted pedicle screw placement with Stealth navigation (Medtronic Navigation, Louisville, CO, USA) in pediatric spine deformity. They reported that the accuracy rate of the 314 screws placed in the study was 98.7%, and there were no clinically relevant screw-related complications.
In this series, we are the first study to report and compare the clinical use of robotic-assisted navigation with O-arm- or 3D C-arm-assisted pedicle screw insertion for scoliosis surgery, and compare the associated clinical outcomes, and the accuracy and safety of pedicle screw placement with robotic navigation vs a fluoroscopy-assisted free-hand technique.
Methods
Inclusion and Exclusion Criteria
This study was approved by the ethics committee of Qilu Hospital of Shandong University (KYLL-202208-036), and the study was performed in accordance with the Helsinki Declaration. The inclusion criteria were: (1) patients diagnosed with scoliosis requiring surgical correction; (2) Cobb angle of the main curve < 90°; (3) flexibility indices > 30%; and (4) patients not requiring three-column osteotomy. The exclusion criteria were patients with pulmonary dysfunction, congenital heart diseases, and pulmonary hypertension, or other conditions preventing the patient from tolerating correction surgery.
Patients’ Characteristics
One hundred and forty-four scoliosis patients were included in this study and were divided into 2 groups. Ninety-two patients with an average age of 32.2 years (range 9-66 years) underwent robot-assisted pedicle screw insertion (Group A), namely 18 cases of congenital scoliosis, 8 cases of neuromuscular scoliosis, 30 cases of idiopathic scoliosis, and 36 cases of degenerative scoliosis. Fifty-two patients with an average age of 29.1 years (range 8-69 years) were treated with a fluoroscopy-assisted free-hand technique (Group B), namely 12 cases of congenital scoliosis, 5 cases of neuromuscular scoliosis, 19 cases of idiopathic scoliosis, and 16 cases of degenerative scoliosis. Group A was further divided into Subgroup AI (48 patients who underwent robotic-assisted navigation using an O-arm) and Subgroup AII (44 patients who underwent robotic-assisted navigation using a 3D C-arm).
Surgical Procedures
After general anesthesia, all patients were positioned prone with neurophysiological monitoring (motor- and sensory evoked potentials) to reduce the risk of spinal cord injury during deformity correction. A standard posterior midline incision was used to expose all predetermined levels. In group B, the pedicle screws were implanted with a fluoroscopy-assisted free-hand technique. During the intraoperative fluoroscopy, the surgeons were protected behind a mobile X-ray barrier located 5 m from the patients.
The workflow of the robotic-assisted navigation using an O-arm or 3D C-arm in group A was as follows: First, we connected the TianJi Robot system (TiRobot; TINAVI Medical Technologies Co., Ltd., Beijing, China) and installed the registration and placed it in the operation area so that the registration was within the fluoroscopic field. An intraoperative O-arm (Medtronic, Memphis, TN, USA) or 3D C-arm (Siemens, Erlangen, Germany) was used to perform a CT scan. During the intraoperative scan, the surgeons were out of operation room to avoid radiation exposure. Then, the 3D fluoroscopic images were imported into the TianJi Robot system. The pedicle screw diameter, length, and trajectory were planned in the robotic workstation. The patient tracker was anchored to the spinous process using a clamp. Once registration was confirmed, the screw guider was installed and sent to the surgical field by the robotic arm. The sleeve was placed into the screw guider and brought to the cortical bone surface. A K-wire was drilled into the vertebrae through the sleeve, and the optimal position was confirmed by fluoroscopy. Finally, the cannulated pedicle screws were inserted. After the instrumentation was completed, we verified the screw position using fluoroscopy. If the position was satisfactory according to the O-arm or fluoroscopy, the robotic system was withdrawn. Schwab grade 1 or 2 osteotomy or transforaminal interbody fusion was selected for deformity correction according to the degree of deformity, then vertebral body derotation, distraction at the concave side, and compression at the convex side were performed for better coronal correction, if necessary. Finally, the rods were fully tightened. A custom-made orthosis was used in all patients after surgery for 1-3 months.
Assessment of the Clinical Outcomes
Operation time, radiation exposure, blood loss, postoperative hospital stay, and postoperative complications related to the surgeries were investigated and compared between the groups. The radiation exposure was measured using digital dosimeters.
Radiographic Assessment
Coronal and sagittal assessment of scoliosis
Full-length radiographs, including coronal and lateral views, and right and left supine side-bending views were obtained using a standard protocol. For full-length radiographs, patients were instructed to adopt a comfortable standing posture with their arms positioned with approximately 45° of forward shoulder flexion and to place their fingertips on their mid-clavicular region, bilaterally. The radiological parameters were the primary curve Cobb angle, sagittal vertical axis (SVA), thoracic kyphosis (T4-12), lumbar lordosis, and pelvic incidence. The average value was obtained from the measurements of 2 independent observers.
Apical vertebral rotation assessment
The apical vertebral rotation (AVR) in Groups A and B was measured on CT images pre- and postoperatively. The measurement method is shown in Figure 1.
18
At the same time, the derotation rate was calculated as follows: (preoperative AVR – postoperative AVR) preoperative AVR × 100%. Computed tomography (CT) measurement of apical vertebral rotation. In the axial image, the angle between the axis of the vertebral body and the vertical line is shown. AVR, apical vertebral rotation.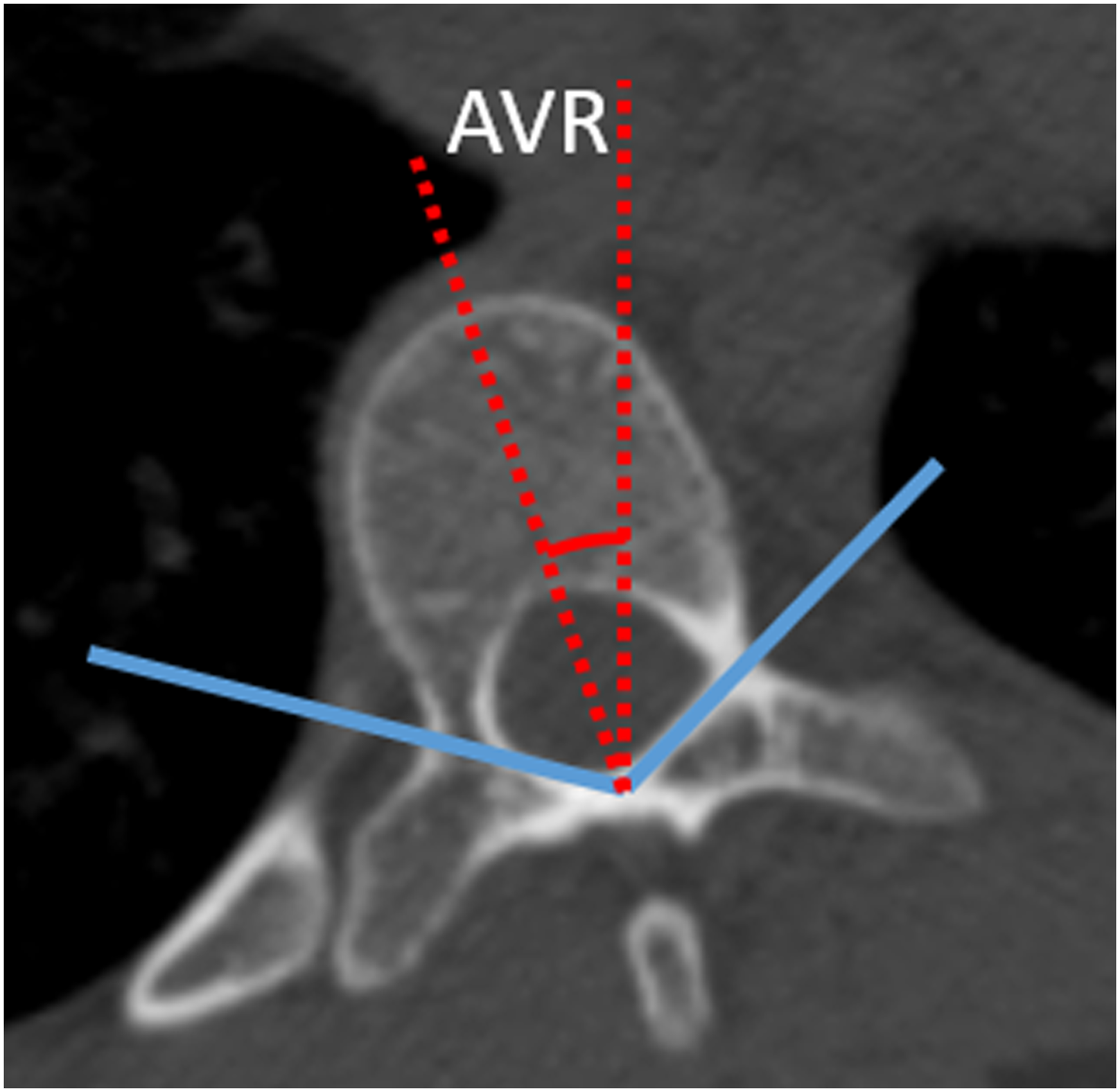
The AVR grade was measured on a standard posteroanterior radiograph postoperatively. 19 When both pedicle screw tips were visible central to the 2 rods (classified as Grade 0 vertebrae), CT measurements of vertebral rotation were between 0° and 8°. In Grade 1 vertebrae, 1 pedicle screw tip was hidden behind the ipsilateral rod, and CT measurements of vertebral rotation were between 9° and 12°. In Grade 2 vertebrae, 1 pedicle screw tip was lateral to its ipsilateral rod, and CT measurements of vertebral rotation were greater than 13°. This grading system could be used to quickly assess postoperative residual AVR and possibly to evaluate for the development of crankshaft over time.
Assessment of the pedicle screws
In the present study, the accuracy of placement of all pedicle screws was evaluated using reconstructed CT image data to improve accuracy. Perforation was assessed using the following screw misplacement grading systems (Figure 2).20,21 Each screw position was classified as grade 0 (no perforation, with the screw completely within the pedicle), grade 1 (perforation < 2 mm), grade 2 (perforation ≥ 2 to < 4 mm), or grade 3 (perforation ≥ 4 mm). Grade 0 and 1 screw positions were considered clinically acceptable, while grades 2 and 3 indicated perforation. In accordance with this grading system, the screw misplacement rates were determined. Pedicle screw misplacement grading.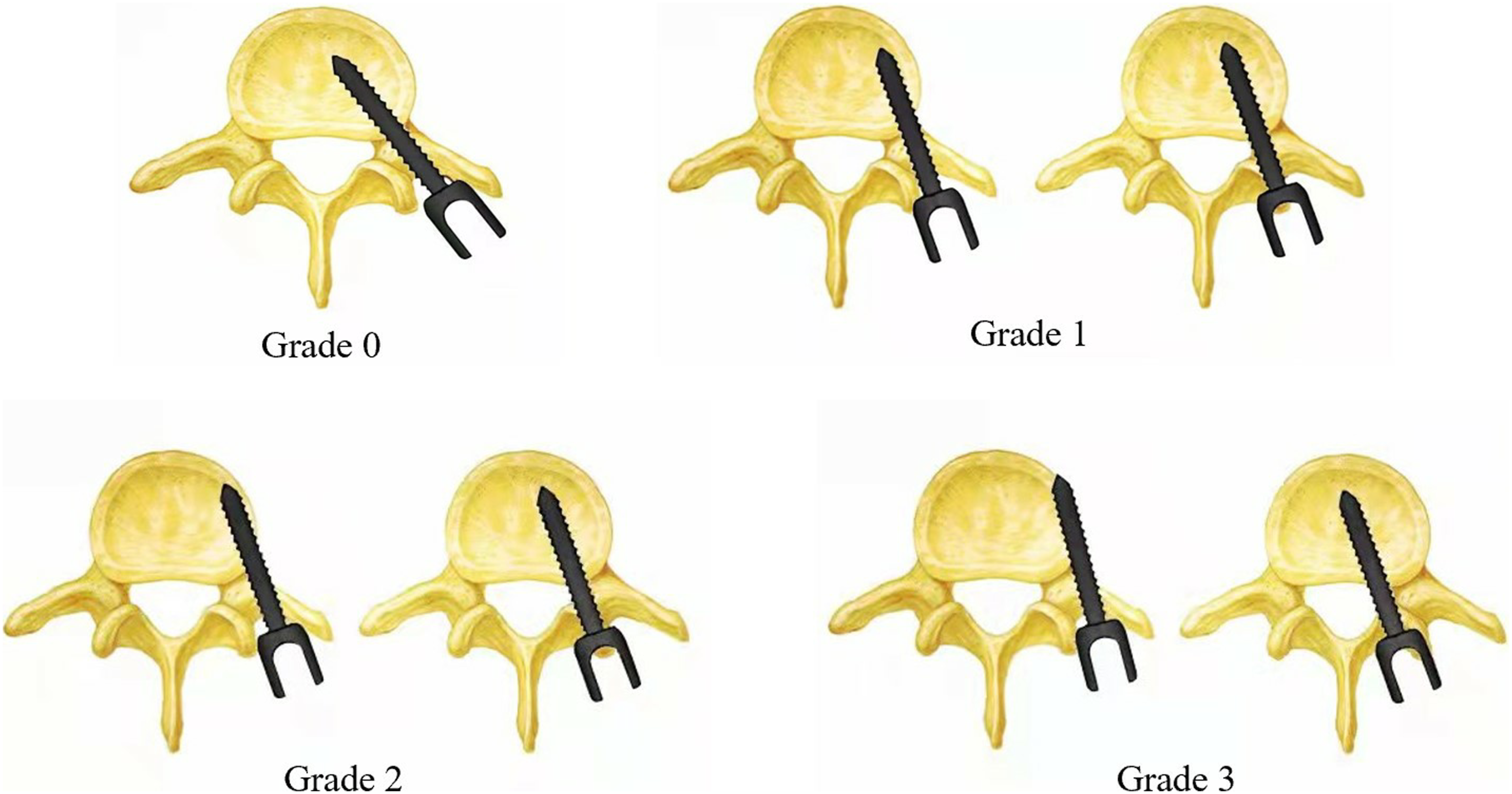
Statistical Analysis
Statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). All continuous data are expressed as mean ± standard deviation. Differences between 2 groups were determined by the independent-samples T test. The chi-square test was used to analyze categorical variables, and the significance level was set at .05.
Results
The Demographic of the Patients.
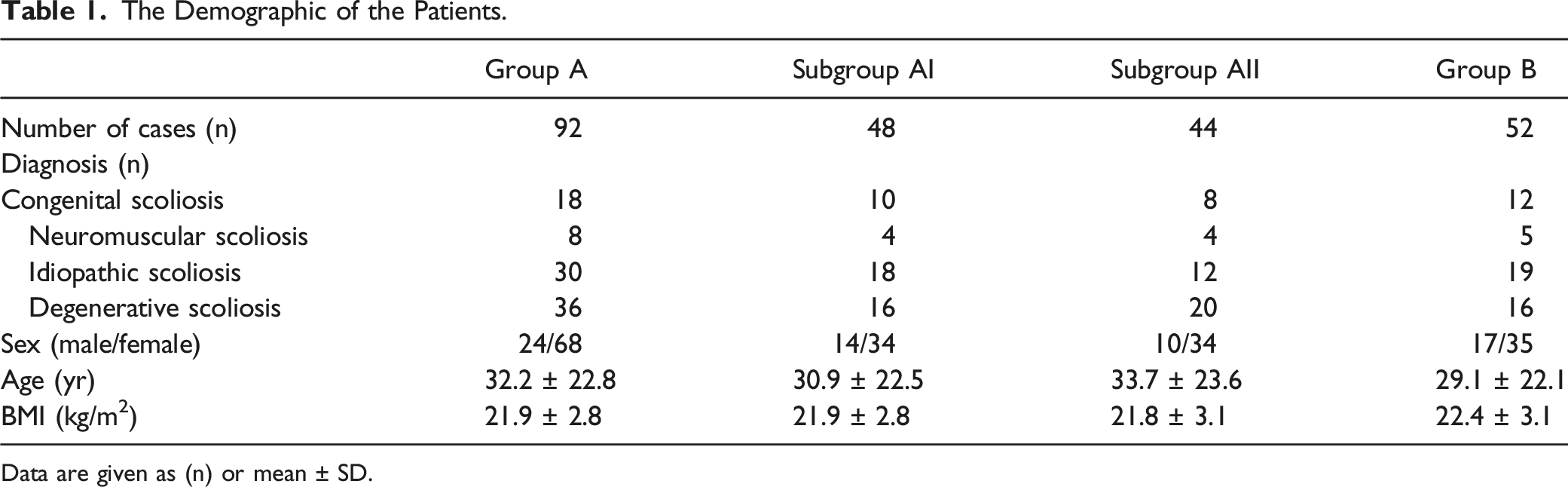
Data are given as (n) or mean ± SD.
The Clinical Outcomes of Patients.
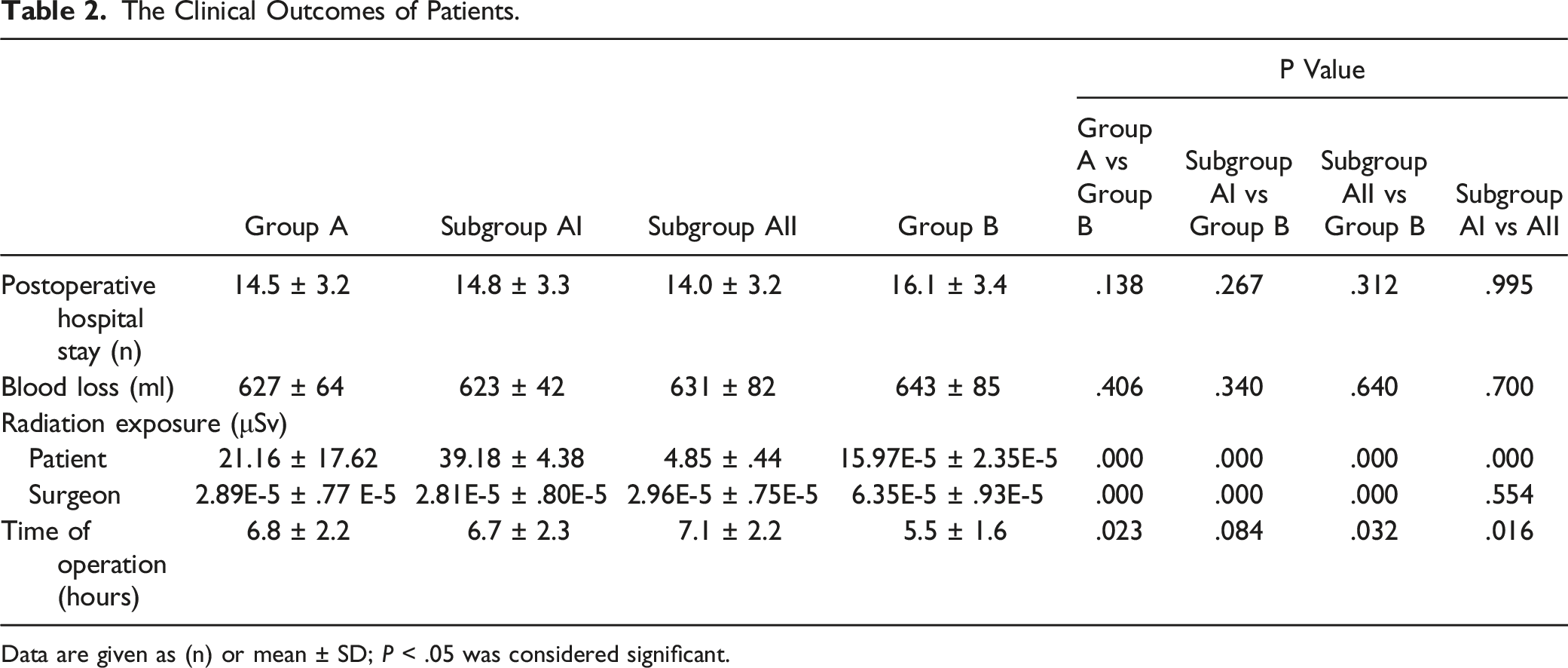
Data are given as (n) or mean ± SD; P < .05 was considered significant.
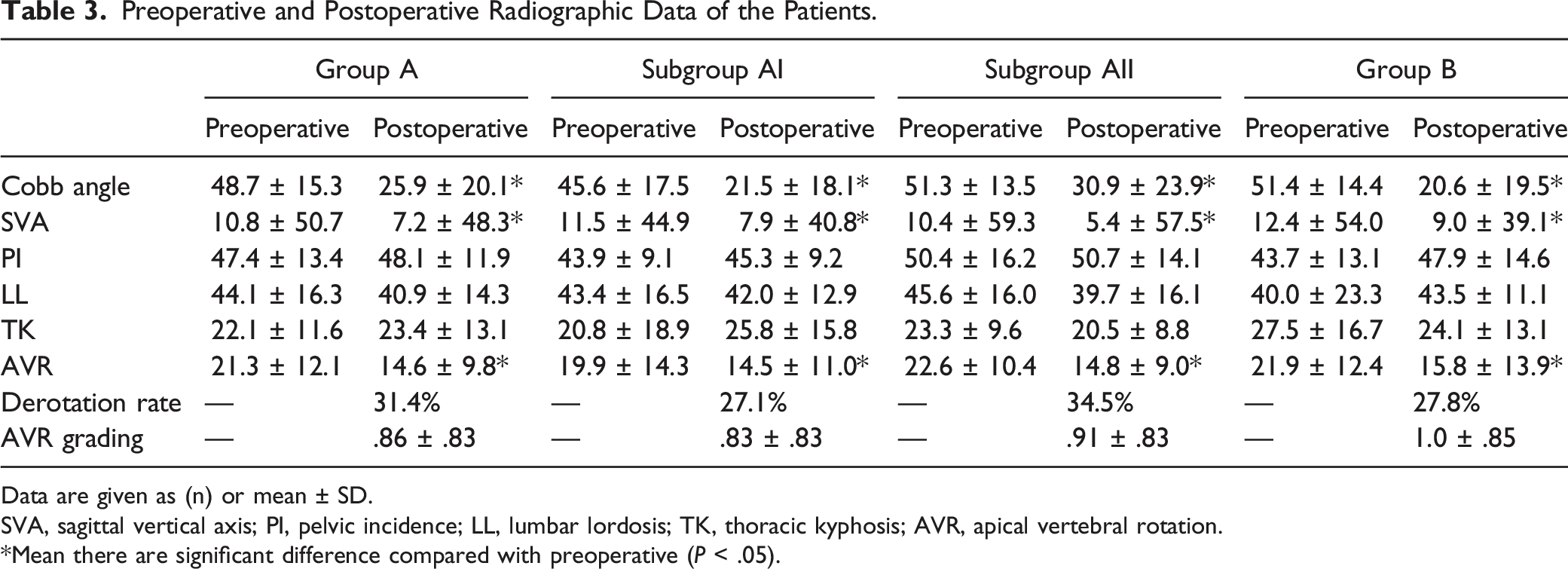
The Cobb angles of the main curve, SVA, and AVR in Group A (Subgroups AI or AII) and Group B improved significantly postoperatively (Figure 3). There were no significant differences in the derotation rate and the AVR grade postoperatively between Groups A and B (P > .05), and similarly, no significant difference between Subgroups AI and AII (P > .05) (Table 3). A 15-years-old female patient was diagnosed with adolescent idiopathic scoliosis (Lenke type 1), and scoliosis surgery using robotic-assisted navigation with an O-arm was performed. Preoperative anteroposterior and lateral plain radiographs of the entire spine (A, B). Anteroposterior and lateral plain radiographs of the entire spine immediately postoperation (C, D). Preoperative and Postoperative Radiographic Data of the Patients. Data are given as (n) or mean ± SD. SVA, sagittal vertical axis; PI, pelvic incidence; LL, lumbar lordosis; TK, thoracic kyphosis; AVR, apical vertebral rotation. *Mean there are significant difference compared with preoperative (P < .05).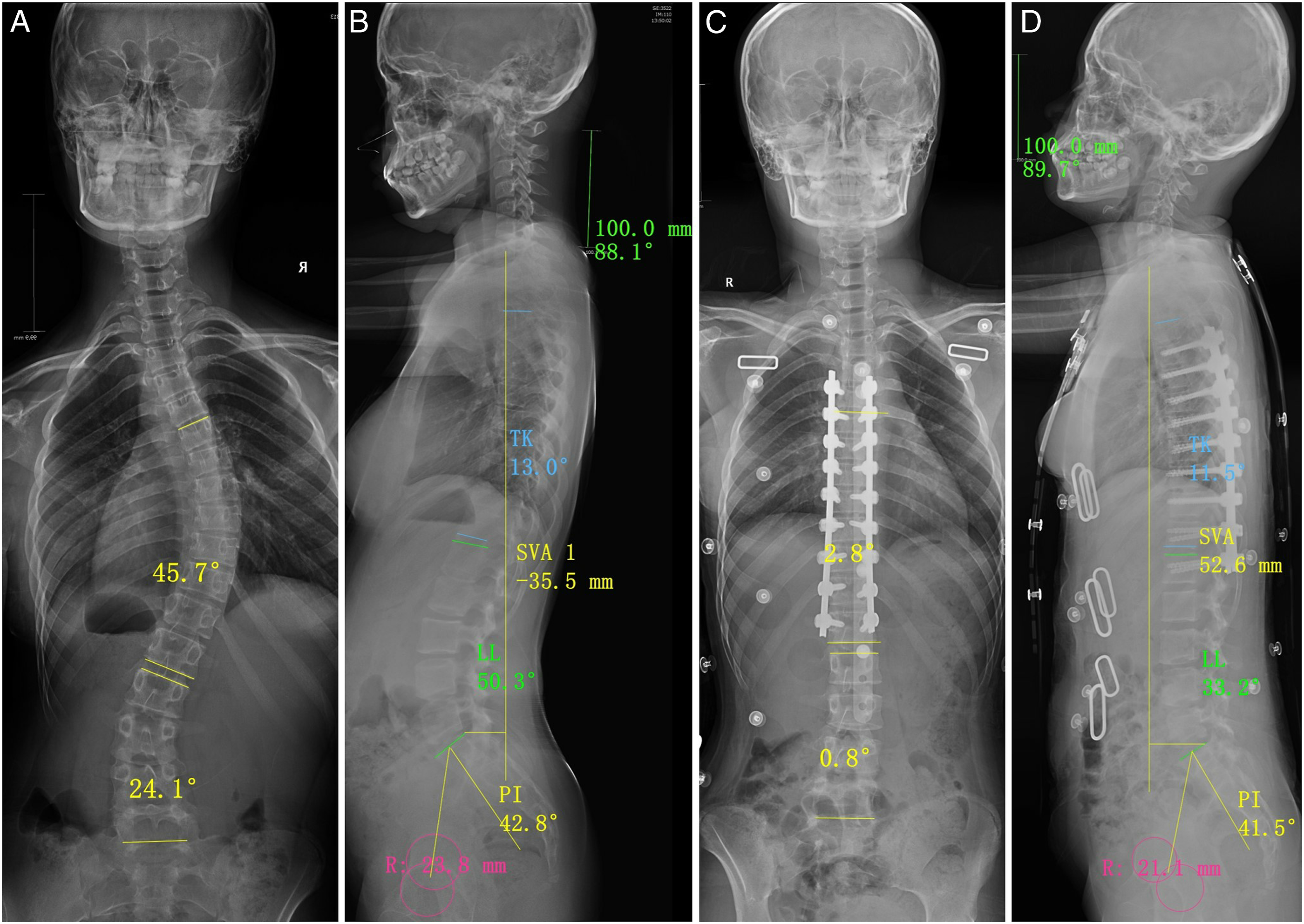
Accuracy of Pedicle Screw Placement.
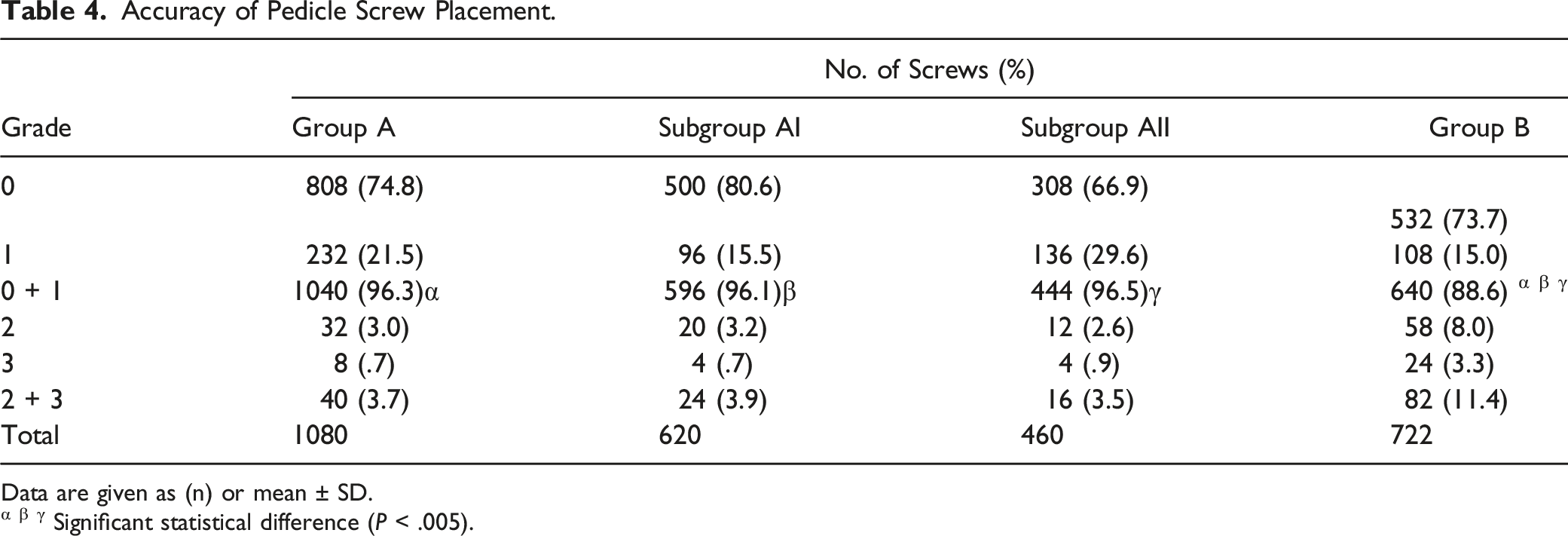
Data are given as (n) or mean ± SD.
α β γ Significant statistical difference (P < .005).
Misplacement of the Pedicle Screws on the Concavity and Convexity in Groups A and B.
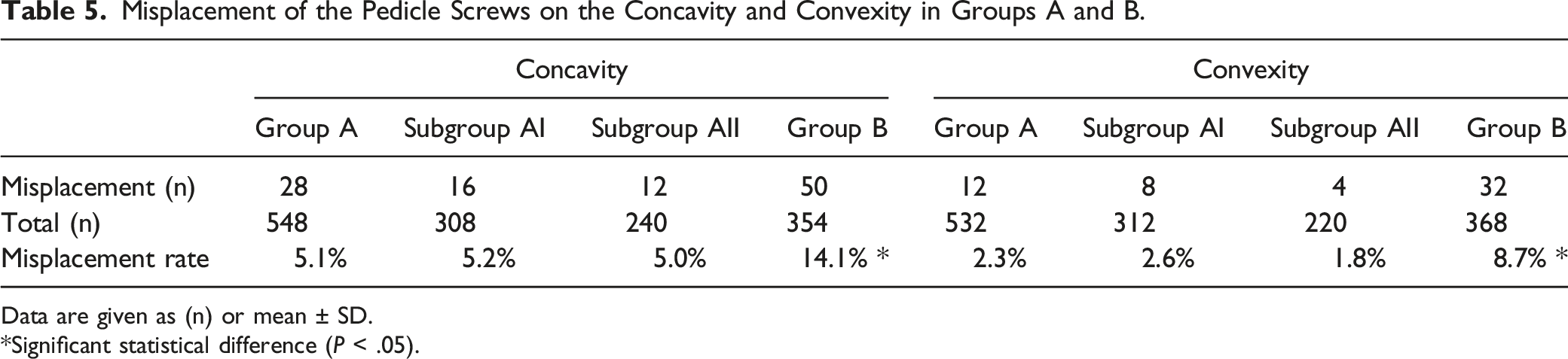
Data are given as (n) or mean ± SD.
*Significant statistical difference (P < .05).
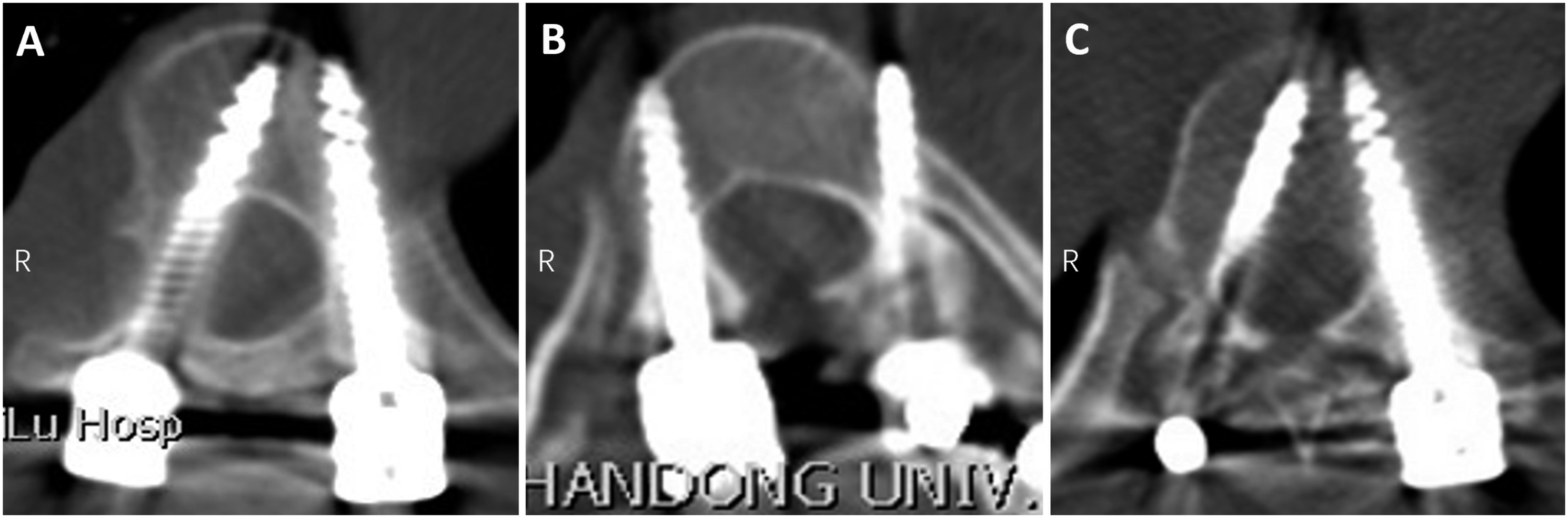
Pedicle screw misplacement. Grade 2 (Right) and grade 1 (Left) misplacement using robotic-assisted navigation with an O-arm (A). Grade 2 (Left) misplacement using robotic-assisted navigation with a three-dimensional (3D) C-arm (B). Grade 2 (Right) and grade 3 (Left) misplacement using a fluoroscopy-assisted free-hand technique (C).
Discussion
Previous studies have shown excellent clinical effects of robot-assisted pedicle screw insertion in spinal surgery.16,22,23 In the present series, radiological parameters, such as Cobb angle and SVA, in Group A (Subgroups AI or AII) and Group B improved postoperatively. In addition, there were no significant differences in the derotation rate, postoperative AVR grade, blood loss, and postoperative hospital stay between Groups A and B. Both the robotic navigation group (robotic-assisted navigation with an O-arm or 3D C-arm) and the freehand group achieved satisfactory clinical outcomes in scoliosis surgery.
One of the concerns regarding robotics is the use of intraoperative 3D imaging, which may expose the patient to significant radiation. Related studies reported that the use of navigation increases radiation exposure to the patient while decreasing radiation exposure to the surgeon and operative team.24,25 Urbanski et al 26 also demonstrated that radiation exposure increased with navigation vs with a freehand technique in scoliosis surgery. In this study, we found that the radiation exposure for patients was higher in Group A (21.16 ± 17.62 μSv) than that in Group B (15.97E-5 ± 2.35E-5 μSv). In addition, compared with robotic-assisted navigation using a 3D C-arm (4.85 ± .44 μSv), robotic-assisted navigation using an O-arm (39.18 ± 4.38 μSv) increased patient radiation exposure. However, the average American civilian is exposed to 3.1 mSv of background radiation per year, and the International Commission on Radiological Protection recommended occupational radiation exposure limit is 20 mSv per year. 24 Therefore, the intraoperative radiation exposure of robotic-assisted navigation in this study is safe and acceptable. The radiation exposure for the surgeon was significantly lower in Group A (Subgroups AI or AII) than that in Group B. We concluded that the medical staff left the room during the robotic scanning and imaging, effectively reducing their radiation exposure.
Operation time is also a concern in robotic surgery. Yu et al 27 reported that robotic navigation was associated with longer operation time vs traditional techniques. In contrast, Kotani et al 12 reported that O-arm navigation decreased the time required to insert pedicle screws without compromising the accuracy of pedicle screw placement in scoliotic patients. In the present study, the operation time in Subgroup AII was significantly longer than that in Subgroup AI and Group B; however, there was no significant difference between Subgroup AI and Group B. Robotic-assisted navigation with an O-arm can register 6-7 spinal levels (for the insertion of 12-14 pedicle screws), while robotic-assisted navigation using a 3D C-arm can register only 3-4 spinal levels (for the insertion of 6-8 pedicle screws) for 1 360° scan. Additionally, compared with robotic-assisted navigation using an O-arm, robotic-assisted navigation using a 3D C-arm requires longer scanning time. Thus, robotic-assisted navigation using an O-arm is more efficient in scoliosis correction surgeries.
Successful and safe insertion of pedicle screws in scoliosis correction surgery are the key points in successful scoliosis correction. Free-hand pedicle screw insertion in scoliotic patients is difficult because of dysplastic pedicles, vertebral rotation, and spinal cord deviation.9,28,29 There is wide variation in reported freehand pedicle screw accuracy, from 1.5% to 43%,6-9 which is likely explained by variation in surgeon training, experience, and case complexity. A thorough understanding and appreciation of the patient’s spine in complex deformity cases is essential for the spine surgeon; however, the 3D nature of the deformed spine is often difficult to visualize even for the most experienced surgeons.
With the development of digital technology, robot-guided surgical and navigation systems are being used more often to facilitate efficient and accurate placement of pedicle screws during spinal surgeries. 30 Previous studies demonstrated lower pedicle screw malposition rates in 3D fluoroscopic navigation systems compared with the traditional freehand technique.31-33 Related studied demonstrated that robot-assisted pedicle screw placement was associated with fewer cortical breaches and screw placement deviations compared with freehand screw placement.16,17,34,35 However, it should be noted that these studies reviewed all cases of robotic instrumentation and did not delineate between degenerative and deformity procedures. Additionally, studies of robotic-assisted navigation using O-arm- or 3D C-arm-assisted pedicle screw insertion in scoliosis surgery are limited. In this study, we found that the accuracy of robotic-assisted navigation with O-arm or 3D C-arm-assisted pedicle screw insertion in scoliosis surgery was significantly higher than that of freehand fluoroscopy-assisted pedicle screw insertion, which was consistent with previous studies to some extent.
We also found no statistical difference in the accuracy of pedicle screw insertion between robotic-assisted navigation using an O-arm or a 3D C-arm. Robotic-assisted navigation using a 3D C-arm can generate cross-sectional, sagittal, coronal, and rotatable stereoscopic images during the operation, provide the operator with a 360° observation angle, and accurately judge the condition of bone and implants in all directions. In contrast, robotic-assisted navigation using an O-arm can quickly provide 3D CT images with patients in the operative position, and updated data can be obtained as needed. The image quality of the O-arm system is almost comparable to that provided by recent multidetector helical CT units. Therefore, both robotic-assisted navigation using an O-arm and a 3D C-arm can achieve similar accuracy of pedicle screw insertion.
Robotic-assisted navigation using an O-arm or 3D C-arm does not ensure 100% accuracy and safety. The present study showed that the pedicle screw misplacement rate was 3.7% in Group A, and 3.9% in Subgroup AI and 3.5% in Subgroup AII. In addition, the misplacement rate in Group A on the concavity was 5.1% (5.2% in Subgroup AI and 5.0% in Subgroup AII) and 2.3% on the convexity (2.6% in Subgroup AI and 1.8% in Subgroup AII). A related study found that in 247 pedicles, on the concave side, 104 (42%) pedicles were hypoplastic (ie, transverse pedicle width < 4 mm). Of the 249 convex pedicles measured, 74 (30%) were hypoplastic (P < .005). 36 Pedicles on the concave side in scoliosis patients tend to be thinner, dysplastic, and more sclerotic, and the spinal cord is in direct contact with the medial wall of the pedicles, compared with non-scoliotic patients, making pedicle screw insertion challenging.9,37 Therefore, we can cautiously conclude that 1 of the main reasons for screw misplacement under robotic-assisted navigation using an O-arm or 3D C-arm is hypoplastic pedicles in patients with scoliosis, especially on the concave side. However, most misplaced pedicle screws were clinically acceptable, in this study. Additionally, it is also critical to improve the accuracy of pedicle screw placement by controlling the patient’s tidal volume and reducing intraoperative lumbar and back movement during robotic navigation. Overall, robotic-assisted navigation using O-arm- or 3D C-arm-assisted pedicle screw insertion can improve the accuracy and safety of screw insertion.
Limitations
This study has some limitations. First, this study was conducted at a single center and included a relatively small number of patients. A large series is needed for accurate assessment of the robotic-assisted technique using an O-arm or 3D C-arm. Second, in our clinical practice, we found that severe rotation of the apical vertebrae, limited rotation range of the robotic arm, and muscle-related obstacles may cause image drift and affect the accuracy of pedicle screw placement. Thus, the Cobb angle of the patients included in this study was less than 90° to avoid image drift during pedicle screw placement and avoid related neurovascular complications.
Conclusion
Robotic-assisted navigation using an O-arm or 3D C-arm can effectively increase the accuracy and safety of pedicle screw placement in scoliosis surgery. Compared with robotic-assisted navigation using a 3D C-arm, robotic-assisted navigation using an O-arm involved higher patient radiation exposure; however, O-arm navigation was more efficient intraoperatively.
Footnotes
Acknowledgments
Authors’ Contributions
Chao Li, Hao Li, and Junxiao Su carried out the entire procedure including the study design, data extraction, statistical analysis, manuscript writing and editing. Xinyu Liu and Lianlei Wang conceived of the study, coordinated and participated in the entire process of drafting and editing the manuscript. Junxiao Su, Zheng Wang, and Donglai Li contributed to the data extraction, literature reviewing and statistical analysis. Suomao Yuan and Yonghao Tian contributed to the study design and data analysis. All authors have contributed significantly. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Nature Science Foundation (81874022 and 82172483 to Xinyu Liu; 82102522 to Lianlei Wang), Shandong Natural Science Foundation (ZR202102210113 to Lianlei Wang) and Shandong Province Taishan Scholar Project to Lianlei Wang.
Ethics Approval
This study was approved by the ethics committee of Qilu Hospital of Shandong University and performed according to the tenets of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from all enrolled patients.
Consent for Publication
The authors agree to publication. This manuscript has not been published in any journals.