
Abstract
Study design
Systematic Review.
Objectives
The aim of this systematic review is to evaluate the efficacy of non-invasive procedures in relieving chronic pain due to Failed Back Surgery Syndrome (FBSS).
Methods
Since patients who suffered from FBBS are often non-responders to analgesics, we compared Visual Analogical Scale for low back and leg pain, Oswestry Disability Index, trial success rate, adverse events and complications between conservative treatment groups and control groups.
Results
The included studies were 15. Spinal Cord Stimulation (SCS) was performed in 11 trials; 4 studies assessed the efficacy of different epidural injections; one study evaluated repetitive Transcranial Magnetic Stimulation. All the studies reported back and leg pain relief after treatment with SCS, with a significant superiority in high frequences (HFS) group, compared to low frequences (LFS) group. Moreover, disability decreased with each non-invasive treatment evaluated. Epidural injections of steroids and hyaluronidase have shown controversial results. Adverse events were described in 7 studies: lead migration, hardware-related events, infection and incisional pain were the most reported. Finally, trial success rate showed better outcomes for HFS.
Conclusions
Our systematic review highlights the efficacy of conservative treatments in FBSS patients, with an improvement in pain scores and a decrease in disability index, especially after SCS with HFS. However, due to the lack of homogeneity among trials and population characteristics, further studies are needed to confirm the effectiveness of non-invasive interventions in patients affected by FBSS.
Keywords
Introduction
Failed Back Surgery Syndrome (FBSS) is defined as a “surgical end-stage after one or several operative interventions on the lumbar neuroaxis, indicated to relieve low back pain (LBP), radicular pain or the combination of both without positive effect. 1 Spine surgery is widely used as a definitive approach to treat chronic low-back pain, especially when conservative treatments fail. 2 However, 10-40% of patients experience recurrent or persistent low‐back pain with or without leg pain after technically successful spinal surgery.3,4Although a clear etiology has not been defined yet, several risk factors have been associated with the development of FBSS including recurrent spine pathology, surgical complications, postoperative inflammation and epidural fibrosis.5,6 The accumulation of inflammatory mediators may alter nerve sensitive function, leading to chronic neuropathic pain. 7 Moreover, the formation of postoperative scar tissue can result in adhesions to the dura mater and damage nerve roots. 8 First-step therapies are physical therapy and pain medication, although FBSS is often non-responding to analgesic drugs. 9 Further treatments may include interventional procedures, ie steroid injections, percutaneous endoscopic adhesiolysis and neurostimulation before considering re-surgery, which has been shown to be effective only in 5-30% of patients. 10 However, although the availability and continuous development of such different options, a clear consensus about the best therapeutic choice is still missing. The aim of this systematic review is to investigate the efficacy of non-invasive procedures in the management of low chronic pain due to failed back surgery syndrome.
Materials and Methods
Inclusion Criteria
All included studies were randomized clinical trials (RCTs) and observational studies (OS) published in English, that investigated the effectiveness of conservative treatments in patients affected by LBP previously treated with surgical treatment. Conservative treatments included epiduroscopy, epidural injection and Spinal Cord Stimulation (SCS), with high and low frequencies of stimulation. Exclusion criteria were the use of pharmacological treatment, secondary surgical treatment, and studies in which patients underwent multiple non-invasive treatments.
Search Methods
We performed a systematic literature search according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines using PubMed–Medline, Scopus, and Google ScholaR.The following search strings were adopted: ((((((((("failed back surgery syndrome"[All Fields]) AND ("treatment"[All Fields])) OR (("failed back surgery syndrome"[All Fields]) AND ("management"[All Fields]))) OR (("failed back surgery syndrome"[All Fields]) AND ("neurolysis"[All Fields]))) OR (("failed back surgery syndrome"[All Fields]) AND ("denervation"[All Fields]))) OR (("failed back surgery syndrome"[All Fields]) AND ("nerve ablation"[All Fields]))) OR (("failed back surgery syndrome"[All Fields]) AND ("radiofrequency"[All Fields]))) OR (("failed back surgery syndrome"[All Fields]) AND ("neuromodulation"[All Fields]))) OR (("failed back surgery syndrome"[All Fields]) AND (spinal cord stimulation))) OR (("failed back surgery syndrome"[All Fields]) AND ("steroid injection"[All Fields])). After removing duplicates, two review authors (G.F.P. and S.D.M.) evaluated the abstracts of eligible studies, and any discrepancy was examined with the third reviewer (F.R.). Finally, two reviewers (G.F.P. and S.D.M.) read the full articles to assess the studies for inclusion in this review.
Data Collection, Analysis, and Outcomes
Two independent reviewers (G.F.P. and S.D.M.) conducted data extraction. The following data were extracted: authors, year of publication, study design, level of evidence (LOE), numbers of participants in study and control groups, age and sex of participants, previous surgery and surgical level, duration of pain, type of treatments, follow-up, and results. Visual Analogical Scale (VAS) for low back pain and leg pain, Numeric Rating Scale (NRS) for low back pain and leg pain and Oswestry Disability Index (ODI) were assessed as outcomes in the included studies. The trial success rate was evaluated as patients with a >50% reduction of VAS for back pain. Finally, adverse events and complications were compared between conservative treatment groups and control groups.
Risk of Bias Assessment
The risk of bias of the included RCTs was performed by two reviewers (G.F.P. and S.D.M.) through the Cochrane risk-of-bias tool. That tool classifies seven items as low, unclear, or high risk of bias. Finally, in case of 6-7 items at low risk of bias, the studies reported low risk of bias; for 4-5 items at low risk of bias, the studies reported unclear risk of bias; for <4 items at low risk of bias, the studies reported high risk of bias.
Results
Results of the Search
The literature search produced 1070 articles. After removal of duplicates, 1009 articles were screened for title and abstract, leading to 40 eligible papers, which were read in full-text. Then, 24 studies were refused for the following motivations: not reporting selected outcomes (n = 10), non-specific design of the study (n = 5), non-conventional conservative treatment used (n = 4), same population with lower follow-up (n = 4), protocols of RCT (n = 2) Finally, 15 studies were included in the systematic review (Figure 1). Preferred reporting items for systematic review and meta-analysis (PRISMA) flow diagram.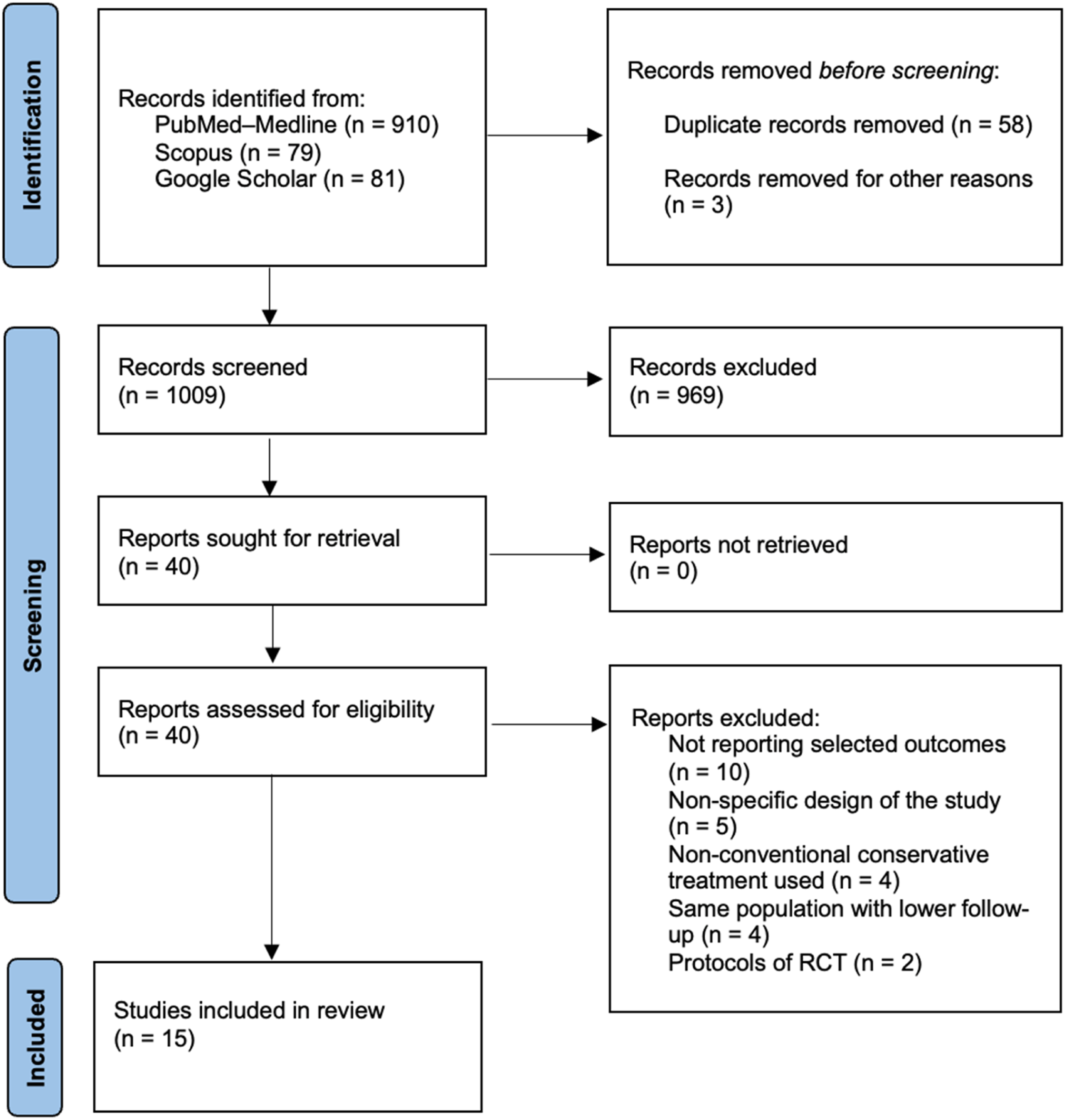
Characteristics of the Included Studies
Main characteristics of the included studies.
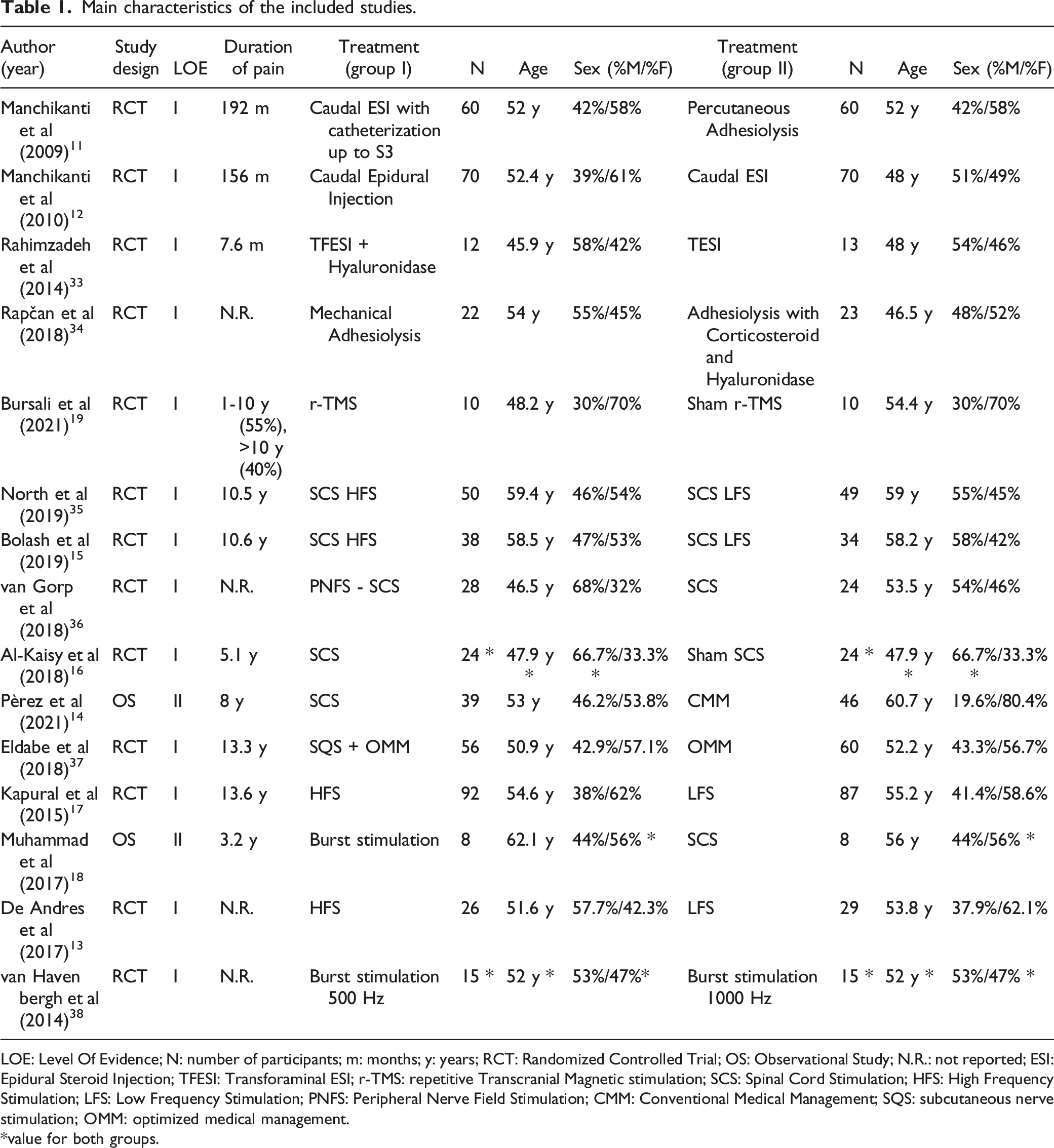
LOE: Level Of Evidence; N: number of participants; m: months; y: years; RCT: Randomized Controlled Trial; OS: Observational Study; N.R.: not reported; ESI: Epidural Steroid Injection; TFESI: Transforaminal ESI; r-TMS: repetitive Transcranial Magnetic stimulation; SCS: Spinal Cord Stimulation; HFS: High Frequency Stimulation; LFS: Low Frequency Stimulation; PNFS: Peripheral Nerve Field Stimulation; CMM: Conventional Medical Management; SQS: subcutaneous nerve stimulation; OMM: optimized medical management.
*value for both groups.
Clinical Results of the Included Studies.
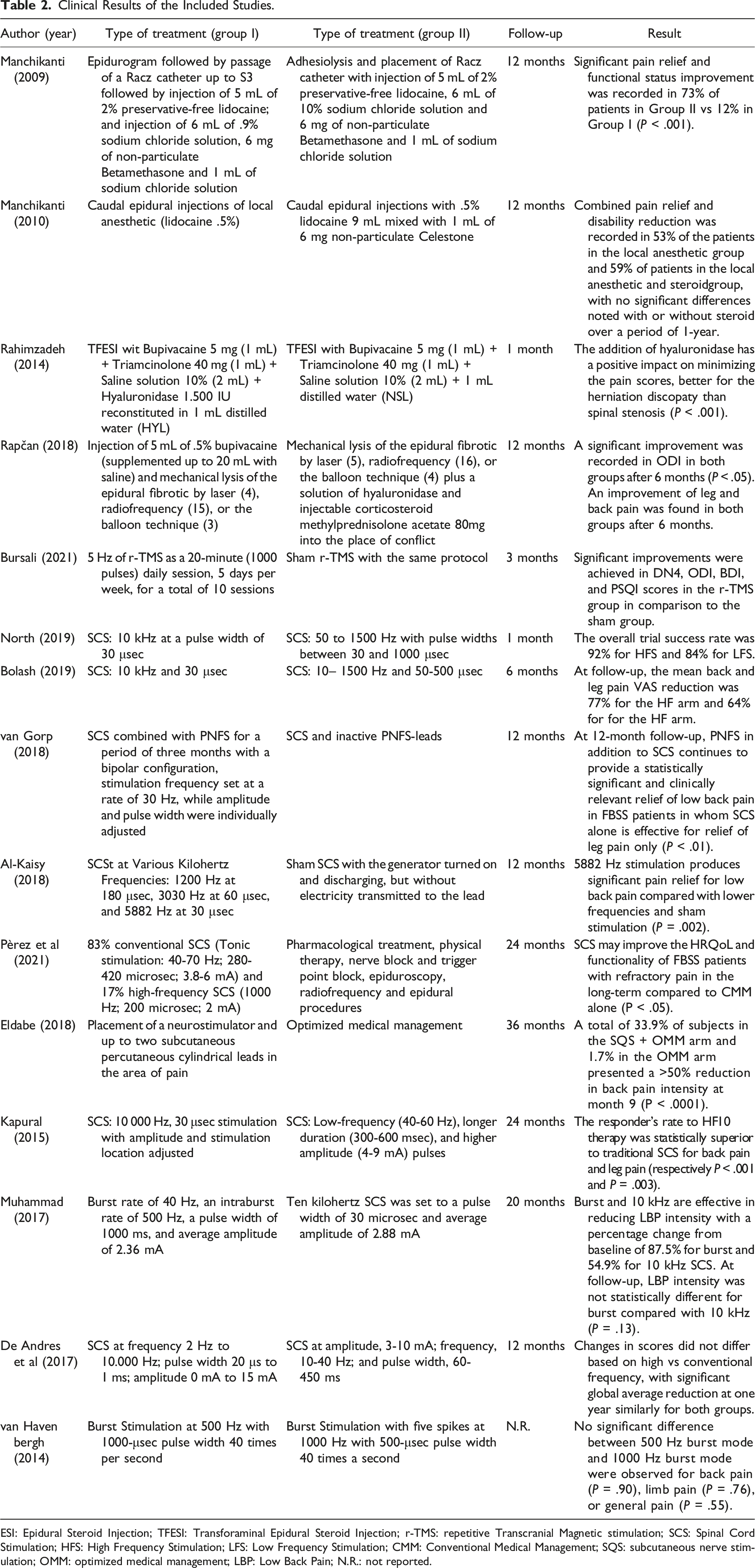
ESI: Epidural Steroid Injection; TFESI: Transforaminal Epidural Steroid Injection; r-TMS: repetitive Transcranial Magnetic stimulation; SCS: Spinal Cord Stimulation; HFS: High Frequency Stimulation; LFS: Low Frequency Stimulation; CMM: Conventional Medical Management; SQS: subcutaneous nerve stimulation; OMM: optimized medical management; LBP: Low Back Pain; N.R.: not reported.
Clinical Outcome Data
Clinical Outcomes.
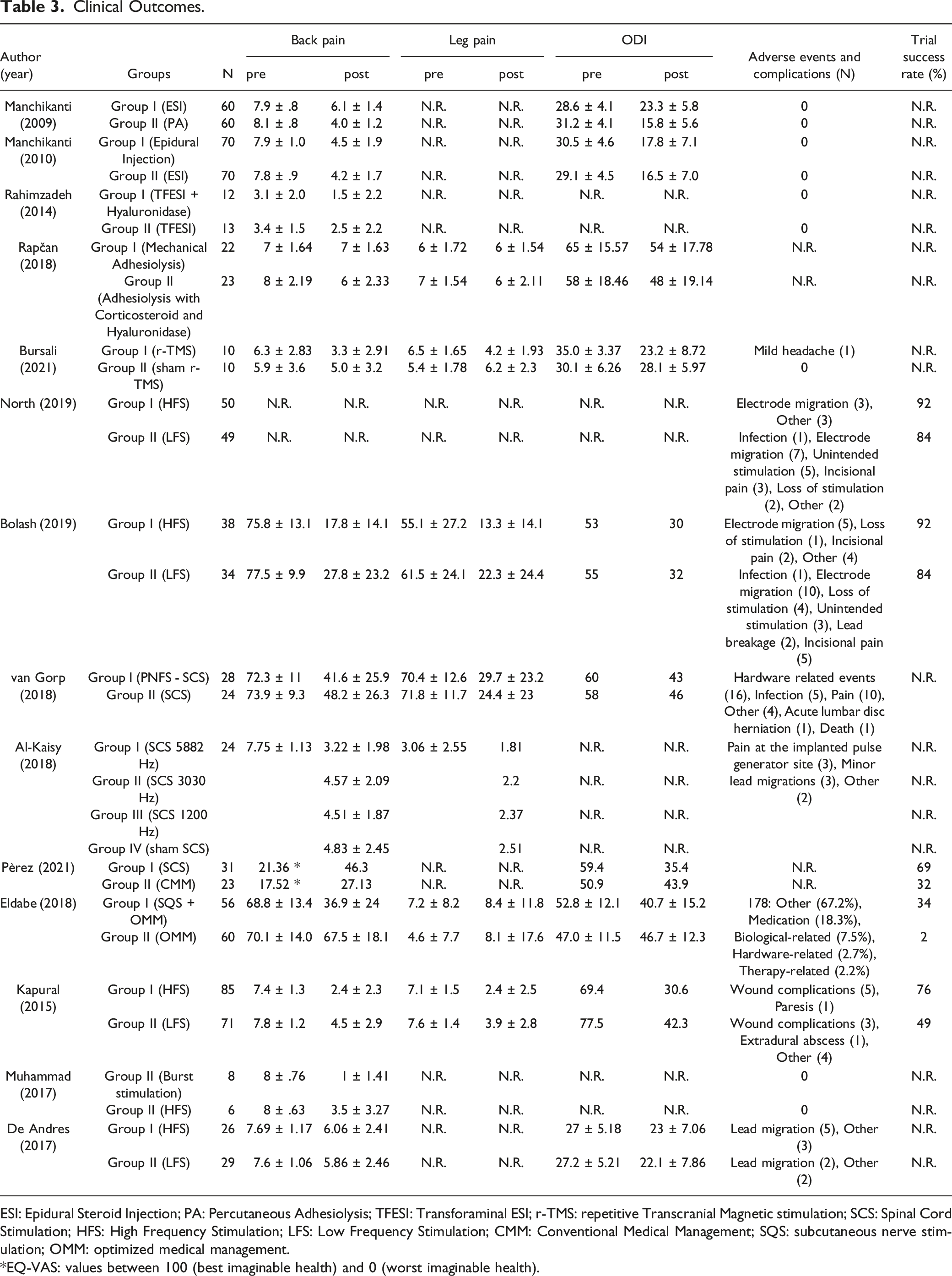
ESI: Epidural Steroid Injection; PA: Percutaneous Adhesiolysis; TFESI: Transforaminal ESI; r-TMS: repetitive Transcranial Magnetic stimulation; SCS: Spinal Cord Stimulation; HFS: High Frequency Stimulation; LFS: Low Frequency Stimulation; CMM: Conventional Medical Management; SQS: subcutaneous nerve stimulation; OMM: optimized medical management.
*EQ-VAS: values between 100 (best imaginable health) and 0 (worst imaginable health).
Methodological Evaluation
Cochrane Risk-of-Bias Tool for Randomized Controlled Trials.
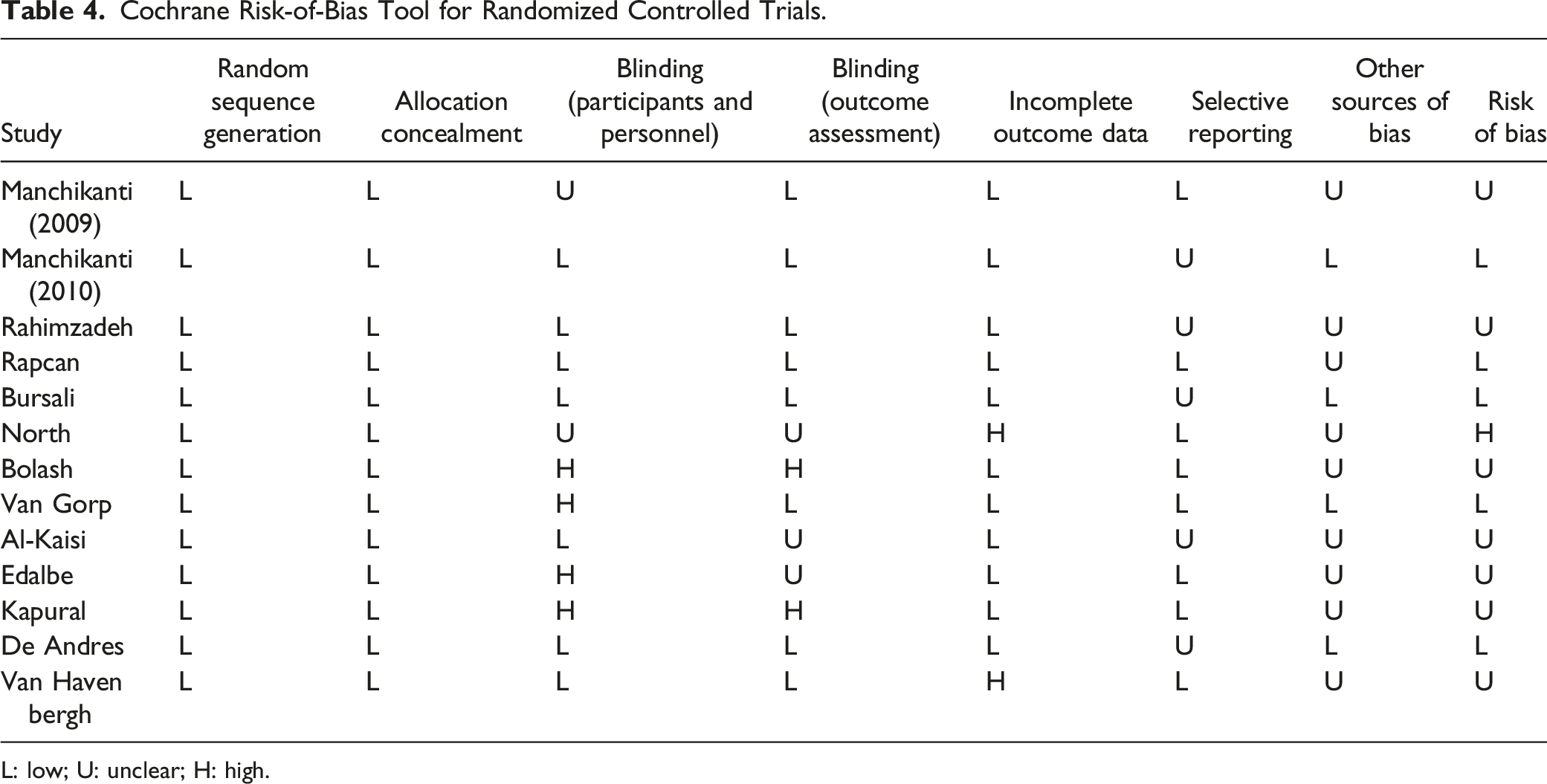
L: low; U: unclear; H: high.
Discussion
Pain management in FBSS remains a challenge and only a few studies have been performed to investigate the efficacy of conservative treatments for chronic low-back pain and leg pain. These patients are often non-responders to analgesics, and non-invasive approaches such as epiduroscopy, epidural injection and Spinal Cord Stimulation may be effective therapeutic choices, as alternatives to spine surgery. The role of epidural injections of steroids and hyaluronidase in FBSS is still controverted, due to a paucity of literature. Injections in the epidural space in back and leg pain have shown controversial results so far.20-23 Moreover, the effectiveness of hyaluronidase in producing pain relief in FBSS and spinal stenosis is largely unknown. Epidural scar tissue could be disrupted by hyaluronidase, a lysing enzyme that is supposed to enlarge the spread of other injected drugs, such as corticosteroids, reducing fibrosis in the epidural space during epiduroscopy. Few trials have studied the effects of injections in epidural space. Devulder et al 24 and Yousef et al 25 demonstrated that hyaluronidase administration improved pain scores. In a study by Schulze et al, 26 corticosteroids and hyaluronidase targeted injection induced a reduction of back pain and inflammation, with a resulting epidural neuroplasty. Heavner et al 27 compared the use of epidural saline plus hyaluronidase to saline alone and they did not show significant differences in clinical outcome. Recent trials have showed that addition of hypertonic saline to the solution in patients with FBSS improves short term pain control,25,28 probably due to its osmotic and anti-edema action nearby nerve roots. Another non-invasive treatment for chronic pain in FBSS patients is Spinal Cord Stimulation. SCS consists of electrical stimulation of the dorsal columns of the spinal cord, using a high frequency of stimulation of 10 kHz (HFS) or a lower frequency of 1500 Hz or less (LFS). Some systematic reviews and meta-analyses concluded that SCS decreases analgesics consumption, reduces pain, and improves quality of life while being also cost-effective.29-31 Compared to the past, SCS systems have been implemented with more options and components, so the debate is now on efficacy, cost-utility, adverse events, and indications. The predominant indication continues to remain stable for neuropathic pain from FBSS. The National Institute for Health and Care Excellence (NICE) in the UK recommends SCS as a treatment for patients suffering from refractory chronic neuropathic pain conditions, including chronic low back pain. In a systematic review and meta-regression analysis, 32 SCS is described as an effective pain-relieving treatment for FBSS in those with predominant leg pain, independently of a prior history of back surgery. However, this study included almost exclusively case series, therefore RCTs are needed to confirm the effectiveness of SCS in the chronic low back pain population with predominant low back pain. The evidence for SCS in the treatment of neuropathic pain is continuing to grow as more prospective and randomized trials are being performed. In all the included studies, the performed procedures have determined clinically relevant pain relief for LBP and leg pain. Moreover, it has been shown a statistically significant decrease in LBP and leg pain in FBSS patients treated with SCS HF, compared with SCS LF or sham stimulation. It has been demonstrated an improvement in ODI in all the treated groups. However, there were no significant differences among the various study groups. Finally, no adverse events or complications occurred in the patients who underwent ESI, while only a low percentage of patients treated with SCS reported complications. Furthermore, among the complications, most were represented by electrode migration or pain. Therefore, it can be stated that these are safe and easily practicable treatments. The most important limitation of this research is determined by the lack of homogeneity among the included studies, which did not allow us to carry out a meta-analysis among the LOE I studies. The literature search produced studies that mainly investigated two procedures (ESI and SCS), but with different comparisons among the groups. In fact, the patients underwent several different interventions in the included trials, with great heterogeneity of type and duration of the treatments. Moreover, population characteristics could not be guaranteed to be the same in all the studies.
Conclusion
Our systematic review highlights the efficacy of conservative treatments in FBSS patients, with an improvement in pain scores and a decrease in disability index, especially after SCS with HFS, while the role of epidural injections of steroids and hyaluronidase is still controversial. Many therapeutic options could be evaluated as possible alternatives to spine surgery, yet the etiology of the syndrome is still not cleaR.There’s an open debate about efficacy, adverse events, indications and cost-effectiveness, therefore further studies may implement our knowledge and demonstrate the superiority of a particular treatment over the others.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.