
Abstract
Study Design
Retrospective Cohort Study
Objectives
Cervical radiculopathy and peripheral entrapment neuropathies often have overlapping symptoms that are difficult to distinguish on physical examination. Small-scale studies have attempted to report the incidence of this phenomenon, often called double crush syndrome (DCS), with varying results. The present study aims to determine the incidence of concomitant cervical radiculopathy and peripheral nerve compression and to determine if the DCS hypothesis, which states that compression of a nerve at one site leaves it more susceptible to compression at another, is valid.
Methods
The PearlDiver database was queried from 2010 to 2020. The incidence of peripheral neuropathy in cervical radiculopathy was assessed. Propensity score matching was used to determine if patients with cervical radiculopathy were more likely to have peripheral nerve compression compared to controls, and vice versa, to test the DCS hypothesis.
Results
The database contains records of 90,772 632 patients. The incidence of carpal tunnel syndrome (CTS) or peripheral ulnar nerve compression (PUnC) in cervical radiculopathy was 9.98% and 3.15%, respectively. The incidence of both carpal tunnel syndrome and PUnC in cervical radiculopathy was 1.84%. Patients with cervical radiculopathy were more likely than matched controls to have both CTS (P < .001) and PUnC (P < .001). Patients with CTS (P < .001) and with PUnC (P < .001) were more likely to have cervical radiculopathy than the control cohort.
Conclusions
The incidence of DCS is reported. Patients with cervical radiculopathy are more likely than matched controls to have peripheral nerve compression, and vice versa, in support of the DCS hypothesis.
Keywords
Introduction
The term double crush syndrome (DCS) was originally coined in 1973 by Upton and McComas to describe patients with concomitant cervical radiculopathy and peripheral ulnar or median entrapment neuropathies. 1 They reported on a series of complex patients who presented with signs and symptoms of both cervical radiculopathy and peripheral entrapment neuropathies and found that 70% of their 115 patients with peripheral median or ulnar nerve entrapment had signs or symptoms of cervical radiculopathy. Their conclusion cautioned that physicians should be aware of the possibility that these two pathologies may coexist in the same patient.
Studies have attempted to describe the etiology of DCS, with a popular theory being that compression of a nerve at one site leaves it more susceptible to compression at another. Two animal studies found that a double lesion leads to worse function than if each site were compressed independently.2,3 However, the clinical relevance of this conclusion has been drawn into question, with studies finding no increased risk of carpal tunnel syndrome (CTS) in patients with C6-C8 radiculopathy.4–6
While there is no consensus on whether compression at one site leads to an increased risk for compression at another, it is agreed upon that concomitant cervical radiculopathy and peripheral entrapment neuropathies can coexist in the same patient. Therefore, it is critical to know the incidence of DCS to ensure proper treatment of pathology. To date, this has been difficult to distinguish. Upton and McComas found an incidence of 70% in their patient population. Since then, various studies have assessed the incidence of DCS, with estimates ranging from 10.3% to 70%.1,6–9 In addition, there is no clear evidence to support that either gender or comorbidities place patients at higher risk for DCS.7,10–12 Thus, the purpose of this study was to determine the incidence of concomitant cervical radiculopathy and peripheral nerve compression and to determine if the DCS hypothesis, which states that compression of a nerve at one site leaves it more susceptible to compression at another, is valid. Additionally, we aimed to assess demographic factors associated with the diagnosis.
Methods
Patients in this study were identified through the PearlDiver Mariner Database (Pearl Diver Technologies, Fort Wayne, IN) which includes data from over 90 million patients from 2010 to 2020. The database contains inpatient and outpatient records of procedures, diagnoses, and demographic data and includes both public and private insurance. The database is de-identified and does not require institutional review board (IRB) approval.
Patients were identified with International Classification of Disease, 9th and 10th Edition (ICD) and Current Procedural Terminology (CPT) codes (Supplemental Table 1). Patients were separated into initial cohorts based on diagnostic ICD codes: (1) cervical radiculopathy, (2) CTS, (3) ulnar nerve compression, including both cubital tunnel and Guyon’s canal syndrome. To ensure that the patients had severe enough disease to require treatment, patients were only included if they had a corresponding surgical operation based on CPT code: (1) anterior decompression and fusion procedure or cervical disc replacement, (2) carpal tunnel release, and (3) cubital tunnel release or Guyon’s canal release. Patients with a diagnosis of cervical radiculopathy who underwent a cervical procedure were included in the cervical radiculopathy cohort, patients with a diagnosis of CTS who underwent carpal tunnel release were included in the CTS cohort, and patients with a diagnosis of ulnar nerve compression who underwent release were included in the peripheral ulnar nerve compression (PUnC) cohort.
There were two primary outcomes in this study. The first was the incidence of cervical radiculopathy and concomitant peripheral neuropathy, and vice versa, over the 10-year study period. Specifically, we assessed (1) the incidence of CTS in cervical radiculopathy, (2) the incidence of ulnar nerve compression in cervical radiculopathy, (3) the incidence of both CTS and PUnC in cervical radiculopathy, (4) the incidence of cervical radiculopathy in CTS, and (5) the incidence of cervical radiculopathy in PUnC. The second primary outcome was whether patients with a diagnosis of cervical radiculopathy were more likely to have peripheral compression neuropathies, and vice versa, than the general population, to test the DCS hypothesis. Secondary outcomes included patient age, sex, and comorbidity status for each cohort. Comorbidities studied included respiratory disease, cardiovascular disease, hyperlipidemia, osteoporosis, diabetes, and chronic kidney disease.
Chi square tests were used to compare cohorts based on the proportions of patients with individual comorbidities, age greater than 65, and female sex. The following comparisons were made: (1) CTS vs. cervical radiculopathy; (2) PUnC vs. cervical radiculopathy; (3) CTS vs. PUnC; (4) CTS OR PUnC vs. cervical radiculopathy with one peripheral nerve entrapment; (5) cervical radiculopathy alone vs. cervical radiculopathy with a peripheral nerve entrapment; (6) cervical radiculopathy alone vs. cervical radiculopathy with two peripheral nerve entrapments. A Bonferroni correction was used to account for multiple comparisons and significance was set at a P-value of less than .0167. Odds ratios with 95% confidence intervals were calculated for each comparison.
Additionally, propensity score matching was performed to test the DCS hypothesis. Patients were matched based on age, gender, and Elixhauser comorbidity index (ECI). 13 to assess (1) if patients with cervical radiculopathy were more likely to have a diagnosis of carpal tunnel syndrome than the general population, (2) if patients with CTS were more likely to have cervical radiculopathy than the general population, (3) if patients with cervical radiculopathy were more likely to have PUnC than the general population, and (4) if patients with PUnC were more likely to have a diagnosis of cervical radiculopathy (Supplemental Table 2). Odds ratios are reported with 95% confidence intervals. A Bonferroni correction was again used to account for multiple comparisons and a P-value of less than .0167 was considered significant.
Source of Funding
No funding was received to complete this study.
Results
Patient demographics. All 3 = All three diagnoses, including cervical radiculopathy, carpal tunnel syndrome (CTS), and peripheral ulnar nerve compression (PUnC).
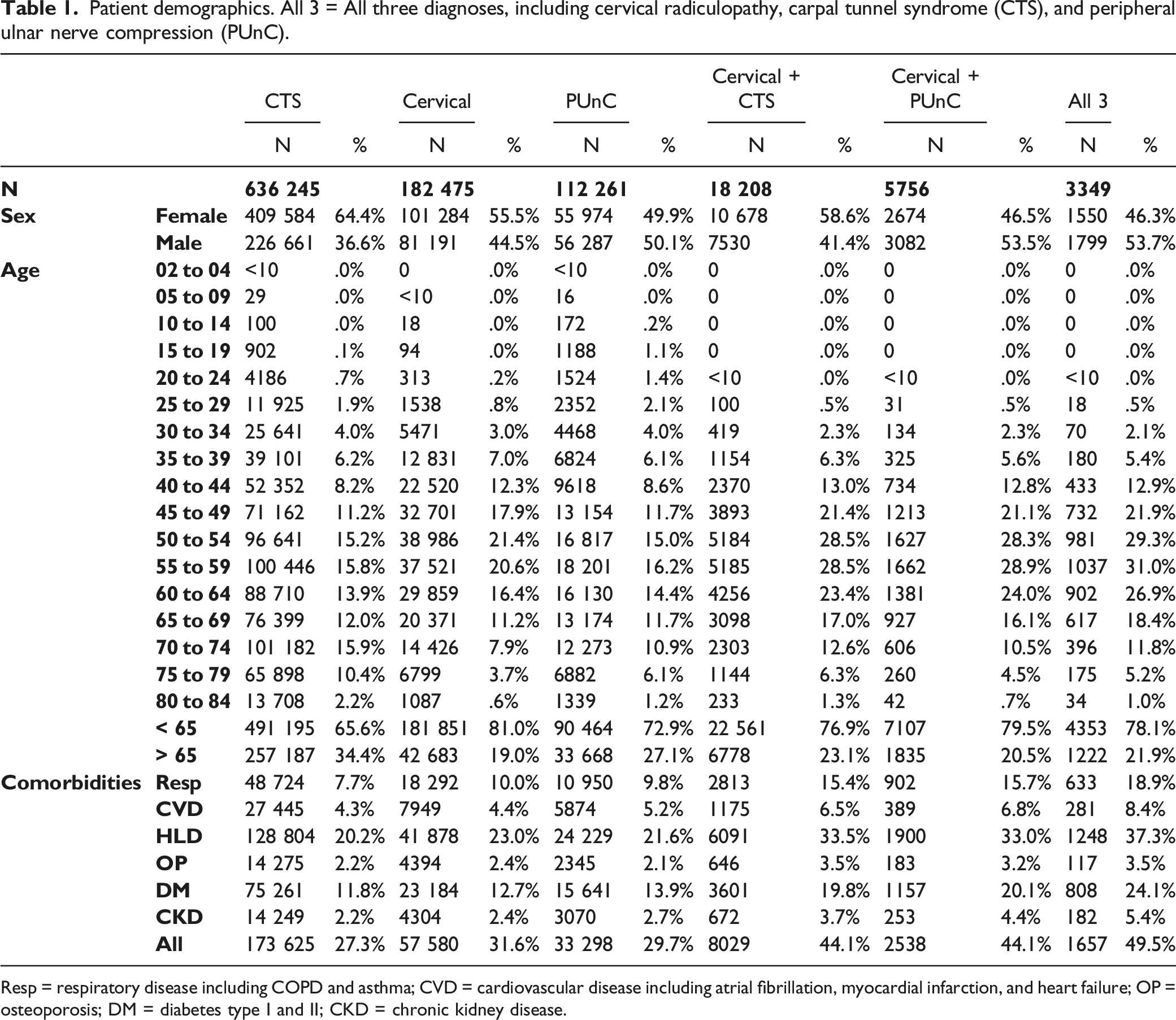
Resp = respiratory disease including COPD and asthma; CVD = cardiovascular disease including atrial fibrillation, myocardial infarction, and heart failure; OP = osteoporosis; DM = diabetes type I and II; CKD = chronic kidney disease.
Cervical Radiculopathy
The cervical radiculopathy cohort included 182 475 patients. Patients were most likely to be aged 50 to 54, 19.01% were over the age of 65, 55.51% were female, the most common comorbidity was hyperlipidemia, and 31.56% of patients had at least one comorbidity (Table 1).
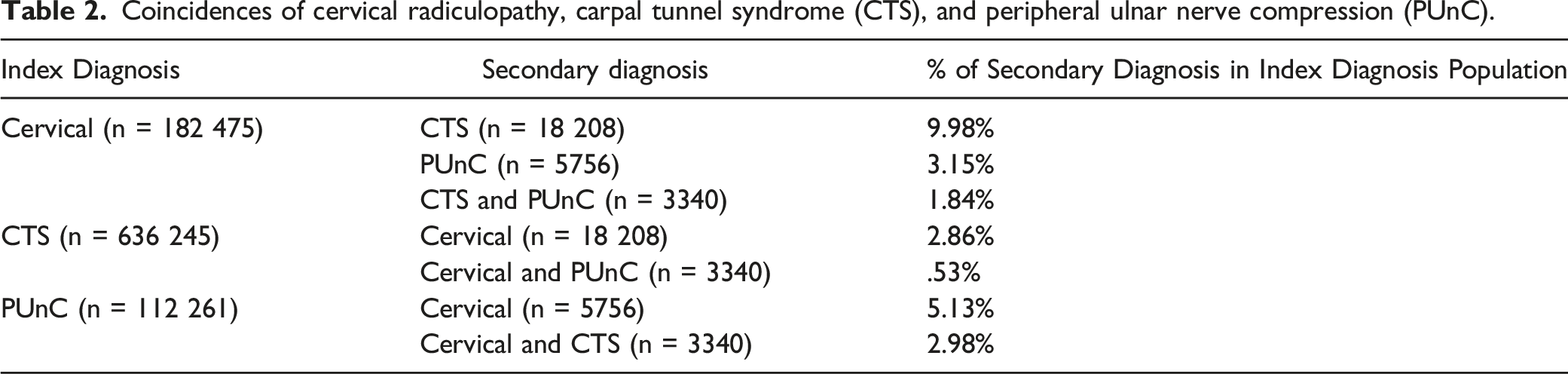
Coincidences of cervical radiculopathy, carpal tunnel syndrome (CTS), and peripheral ulnar nerve compression (PUnC).
Results of the propensity score matched analyses.
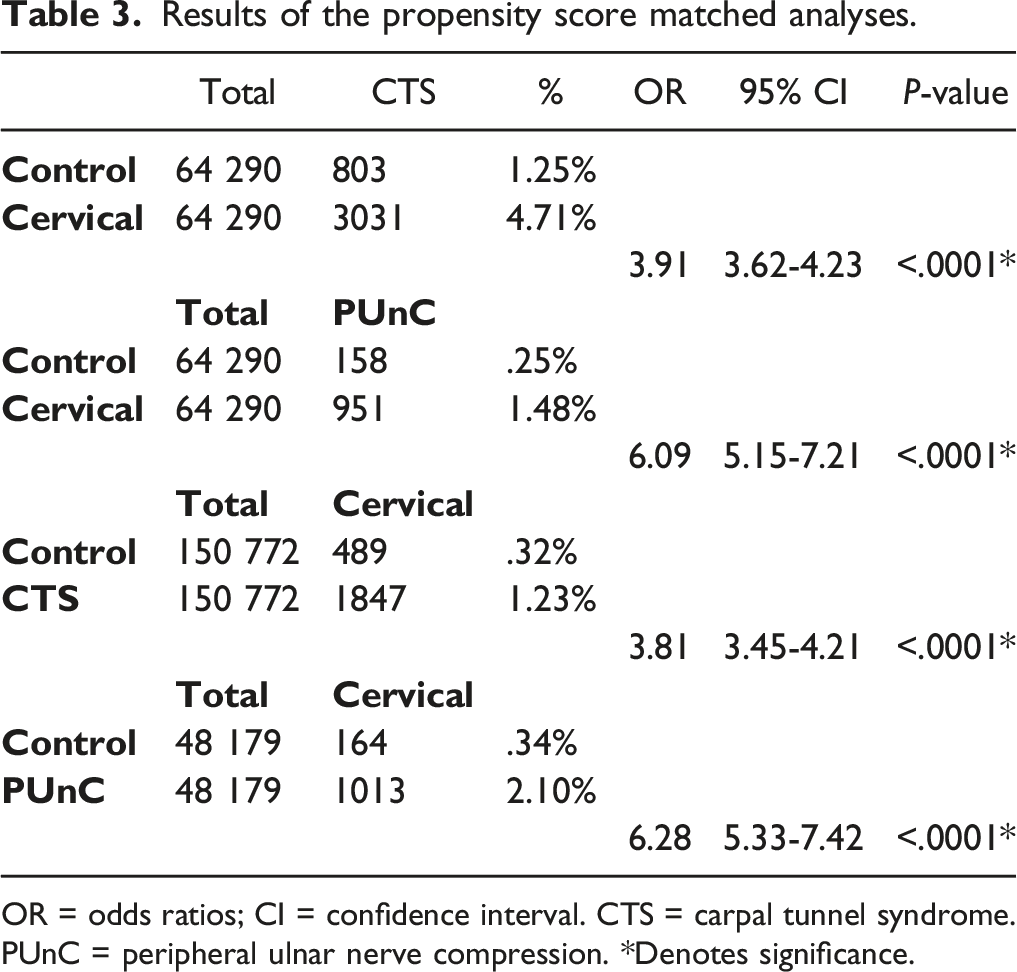
OR = odds ratios; CI = confidence interval. CTS = carpal tunnel syndrome. PUnC = peripheral ulnar nerve compression. *Denotes significance.
Results of intragroup comparisons.
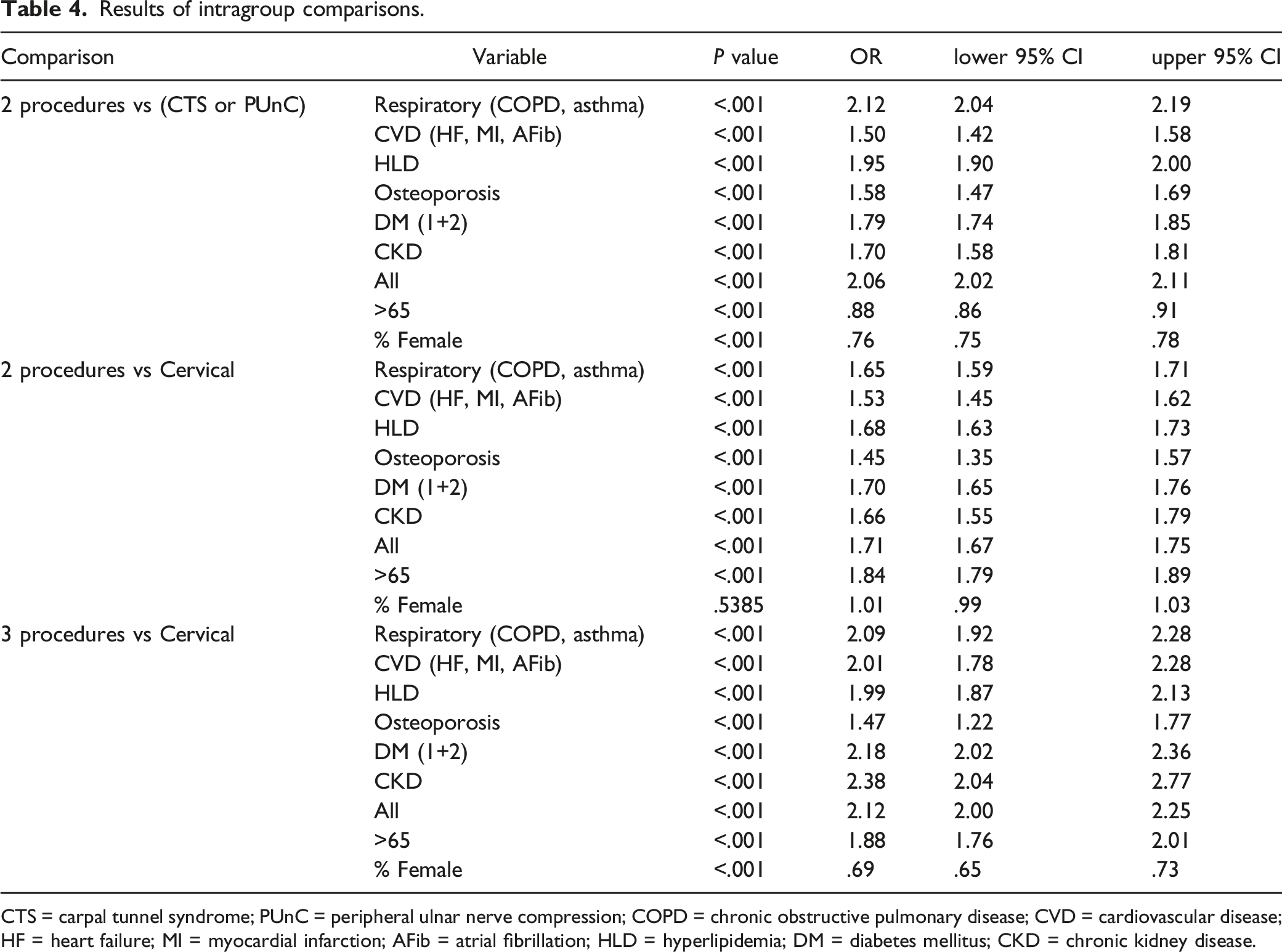
CTS = carpal tunnel syndrome; PUnC = peripheral ulnar nerve compression; COPD = chronic obstructive pulmonary disease; CVD = cardiovascular disease; HF = heart failure; MI = myocardial infarction; AFib = atrial fibrillation; HLD = hyperlipidemia; DM = diabetes mellitus; CKD = chronic kidney disease.
Compared to those with isolated cervical radiculopathy, those with all three diagnoses were more likely to be over the age of 65 (OR 1.88, P < .001, 95% CI 1.76-2.01), have diabetes mellitus (OR 2.18, P < .001, 95% CI 2.02-2.36), respiratory disease (OR 2.09, P < .001, 95% CI 1.92-2.28), cardiovascular disease (OR 2.38, P < .001, 95% CI 2.04-2.77), hyperlipidemia (OR 1.99, P < .001, 95% CI 1.87-2.13), osteoporosis (OR 1.47, P < .001, 95% CI 1.22-1.77), chronic kidney disease (OR 2.38, P < .001, 95% CI 2.04-2.77), and to be male (OR 1.45, P < .001, 95% CI 1.36-1.54) (Table 4).
Carpal Tunnel Syndrome
The CTS cohort consisted of 636 245 patients. The most common age was 70-74 years, 34.37% of patients were over the age of 65 years, 64.38% were female, the most common comorbidity was hyperlipidemia, and 27.29% of patients had at least one comorbidity (Table 1).
The incidence of cervical radiculopathy in the CTS cohort was 2.86% (Table 3). Propensity score matching yielded 150 772 patients per group in both the CTS cohort and the control cohort. Patients in the CTS cohort were more likely to have cervical radiculopathy and undergo a cervical procedure than the control cohort (1.23% vs .32%; OR 3.81, 95%CI 3.45-4.21, P<.0001).
Ulnar Nerve Compression
The PUnC cohort consisted of 112 262 patients. The most common age was 55-59, 27.12% of patients were over the age of 65, 49.86% were female, the most common comorbidity was hyperlipidemia, and 29.66% of patients had at least one comorbidity (Table 1).
The incidence of cervical radiculopathy in the PUnC cohort was 5.13% (Table 3). Propensity score matching resulted in 48 179 patients per group in both the ulnar nerve compression cohort and the control cohort. One thousand and thirteen (2.10%) patients in the PUnC compression cohort had a diagnosis of cervical radiculopathy and underwent cervical surgery compared to 164 (.34%) in the control cohort (OR 6.28, 95%CI 5.33-7.42, P < .0001).
Compared to those who had isolated CTS or ulnar nerve compression, those with two diagnoses were more likely to have diabetes mellitus (OR 1.79, P < .001, 95% CI 1.74-1.85), respiratory disease (OR 2.12, P < .001, 95% CI 2.04-2.19), cardiovascular disease (OR 1.50, P < .001, 95% CI 1.42-1.58), hyperlipidemia (OR 1.95, P < .001, 95% CI 1.90-2.00), osteoporosis (OR 1.58, P < .001, 95% CI 1.47-1.69), chronic kidney disease (OR 1.70, P < .001, 95% CI 1.58-1.81), and to be male (OR 1.31, P < .001, 95% CI 1.28-1.34) Patients with 2 diagnoses were less likely to be over the age of 65 (OR .88 , P < .001, 95% CI .86-.91) (Table 4).
Discussion
Over the 10-year study period, the total incidence of cervical radiculopathy was .40%, the total incidence of CTS was 1.40%, and the total incidence of PUnC was .25%. The incidence of CTS or PUnC in cervical radiculopathy is 9.98% and 3.15%, respectively. The incidence of both CTS and PUnC in cervical radiculopathy is 1.84%. The incidence of cervical radiculopathy in CTS is 2.86%, and the incidence of cervical radiculopathy in PUnC is 5.13%.
The current literature ranges widely when discussing the incidence of peripheral nerve compression in cervical radiculopathy. Upton and McCormic found the incidence of peripheral nerve compression in cervical radiculopathy to be 70%. 1 Several studies have attempted to answer this question since that time. In specific regards to the incidence of CTS in cervical radiculopathy, the current literature ranges in incidence estimates from 10.29%-33%. A retrospective study by Kwon et al of 277 patients with cervical radiculopathy found the incidence of CTS to be 14.1% when reviewing electrodiagnostic studies. 6 A larger scale study of by Lo et al of 765 patients with a similar design found the incidence of concomitant cervical radiculopathy and CTS to be 26%. 8 Ochoa-Cacique assessed patients undergoing carpal tunnel release and cervical surgery for radiculopathy and found the prevalence to be 10.29% in their population. 7 We found the incidence of CTS in cervical radiculopathy to be 9.98% when including all patients who underwent operative treatment, which is below estimates using electromyography and in line with estimates using surgical treatment as an endpoint.
The incidence of ulnar nerve compression in cervical radiculopathy has not been as well reported. One small scale study has been published and found the incidence on electromyography to be 6.5% in their cohort of 80 patients. 14 A small series discussed outcomes of patients with the dual diagnosis who underwent operative treatment at their institution, but did not specify an incidence in their population. 15 The present study found the incidence of ulnar nerve compression in patients with cervical radiculopathy to be 3.15%. In addition, the incidence of both CTS and ulnar nerve compression in cervical radiculopathy was found to be 1.84%.
Few studies have reported on the incidence of cervical radiculopathy in peripheral nerve compression. The largest of these is a retrospective review by Morgan et al of 12 736 limbs who underwent electromyography and found the incidence of cervical radiculopathy in patients presenting with either CTS or peripheral ulnar nerve compression to be 3.4%. 16 This is in line with the current findings, where in the incidence of cervical radiculopathy in carpal tunnel syndrome was found to be 2.86%, and the incidence of cervical radiculopathy in ulnar nerve compression was found to be 5.13%.
The present study also evaluated the DCS hypothesis. The DCS hypothesis states that compression at one site along a nerve leaves it more susceptible to compression at another site. 17 When matching patients based on age, gender, and ECI, patients with cervical radiculopathy were more likely to have CTS or PUnC than controls without cervical radiculopathy. Additionally, patients with either CTS or PUnC were more likely to have cervical radiculopathy than controls without peripheral compression neuropathies. Dellon and Mackinnon tested this hypothesis in 30 rats. 2 The sciatic nerves were compressed proximally or distally, and then five months later a second site of compression was applied, resulting in a significant deterioration in nerve function. They concluded that two sites of compression lead to worse function than a single site and that their findings supported the DCS hypothesis. Nemoto et al performed a two-part study of the DCS hypothesis in sciatic nerves of 50 dogs. 3 In part one, single lesions along the nerves were compared to double lesions, which were found to decrease conduction more than the sum of individual single lesions. In part two, DCS was induced by placing two clamps along the sciatic nerve. Conduction increased to a greater extent when both clamps were released, as opposed to releasing either the proximal or distal clamp. Nemoto et al concluded that a nerve compressed at one site is more susceptible to compression at another, in support of the DCS hypothesis, and recommended that both sites of compression be released to achieve the best result in patients with DCS.
While animal studies have supported the DCS hypothesis, it has been difficult to prove in clinical studies. Bednarik et al matched 60 myelopathic patients to 100 control subjects. 9 The incidence of CTS in the myelopathic cohort was 33%, compared to an incidence of 11% in the control cohort, which was significant. However, no anatomic (ie C8-T1) or laterality association was found in those who had CTS, leading to the conclusion that, while CTS is more common in myelopathic patients than in controls, the findings did not support the DCS hypothesis. Morgan et al came to a similar conclusion in their study of 12 736 limbs. 16 Only .8% of patients were found to meet anatomic requirements of DCS, causing them to conclude that cervical root compression likely does not act as the proximal lesion if DCS does exist. In the present study, we found that patients with cervical radiculopathy were more likely to have a diagnosis of peripheral nerve compression than matched controls without cervical radiculopathy, and vice versa. These findings support the possibility of DCS; however, because EMG and laterality data is not available in the PearlDiver database, our conclusions are limited.
Risk factors for DCS have not been well elucidated. One study identified female gender as a risk factor for DCS, while another reported higher rates in males.8,10 Diabetes was named as a risk factor for DCS, but this has not been confirmed with further investigation. 12 In the present study, patients with isolated cervical radiculopathy were younger than those with isolated peripheral nerve compression. Those with two diagnoses were older than those with isolated cervical radiculopathy but younger than those with isolated peripheral nerve compression. Patients with two or three diagnoses were more likely to have comorbidities, including diabetes. Male gender increased the risk of having two diagnoses compared to isolated peripheral nerve compression and increased the risk of having all three diagnoses.
There are several limitations to our study. First, this is a database study and is reliant on accurate medical coding. Second, we were unable to report patient reported outcomes due to the constraints of using a national database. Third, although the propensity score matching controlled for age, gender, and ECI to test the DCS hypothesis, it is possible that we did not control for all confounding variables in this analysis. Fourth, we were unable to ascertain if patients with a dual diagnosis had the diagnosis on ipsilateral or contralateral sides due to coding limitations, limiting our ability to comment on the DCS hypothesis. Lastly, selection bias was present in this study as patients were included only if they underwent operative treatment for their pathology. Although our results may have been skewed with respect to the true incidence of DCS, this patient selection criteria was used to ensure patients had clinically relevant disease as severity is otherwise unable to be assessed using the PearlDiver database. Additionally, given disease burden inherently differs across patients who either fail or have resolution with conservative management, this limitation is important to highlight as most patients with cervical radiculopathy are adequately treated through conservative therapies. Findings in this study should therefore be limited to populations with cervical radiculopathy and/or peripheral entrapment neuropathies requiring surgical intervention.
Despite these limitations, this is the largest study on patients with concomitant cervical radiculopathy and peripheral neuropathy and the first to report on the concomitant incidences of these three diagnoses in the same population. Furthermore, this is the largest and most comprehensive study to determine demographic risk factors for DCS. Additionally, this subject is applicable to a large proportion of orthopaedic surgeons, including general orthopaedic surgeons, hand surgeons, sports surgeons, and spine surgeons.
In conclusion, the incidence of carpal tunnel syndrome or ulnar nerve compression in cervical radiculopathy is 9.98% and 3.15%, respectively. The incidence of both carpal tunnel syndrome and ulnar nerve compression in cervical radiculopathy is 1.84%. The incidence of cervical radiculopathy in carpal tunnel syndrome is 2.86%, and the incidence of cervical radiculopathy in peripheral ulnar nerve compression is 5.13%. Patients who are male and have more comorbidities are more likely to have more than one diagnosis. Additionally, patients with cervical radiculopathy are more likely than the general population to have peripheral nerve compression, and patients with peripheral nerve compression are more likely than the general population to have cervical radiculopathy. While this supports the DCS hypothesis, our conclusions on this are limited due to lack of anatomic specification in the database used. This may guide physicians when assessing patients to determine the likelihood of concomitant cervical radiculopathy and peripheral entrapment neuropathies.
Supplemental Material
Supplemental Material - The Incidence of Double Crush Syndrome in Surgically Treated Patients
Supplemental Material for The Incidence of Double Crush Syndrome in Surgically Treated Patients by Emily S. Mills, MD, Kevin Mertz, BS, Zoe Fresquez, BS, Andy Ton, BS, Zorica Buser, PhD, MBA, Ram K. Alluri, MD, and Raymond J. Hah, MD in Global Spine Journal.
ORCID iDs
Emily S. Mills, MD https://orcid.org/0000-0002-1777-2969
Kevin Mertz, BS https://orcid.org/0000-0002-9400-2247
Andy Ton, BS https://orcid.org/0000-0002-8891-0353
Zorica Buser, PhD, MBA https://orcid.org/0000-0002-5680-0643
Ram K. Alluri, MD https://orcid.org/0000-0001-5919-707X
Raymond J. Hah, MD https://orcid.org/0000-0001-7513-3519
Footnotes
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.