
Abstract
Study Design
Retrospective Radiographic Review.
Objectives
The purpose of this study was to investigate the correlation between the sacral slope (SS) and pedicle morphological parameters of the fourth lumbar vertebra in degenerative lumbar spondylolisthesis (DLS).
Methods
Our study included 134 patients with L4-5 DLS. We used preoperative multi-slice spiral computed tomography to measure a range of pedicle morphological parameters, and the SS and percentage of slip distance (SDP) of the L4 vertebra were measured on preoperative standing neutral lumbar radiography. Patients were divided into three groups based on their degree of SS: the low sacral slope (LSS) group with SS values of <35°, the mean sacral slope (MSS) group with SS of 35°–45°, and the high sacral slope (HSS) group with SS > 45°.
Results
As the SS increased across groups, the pedicles of L4 became longer and thinner and the pedicle camber angle was smaller. The SDP, pedicle length parameters were positively correlated with the SS, while pedicle width, height, and camber angle were negatively correlated with the SS in the three groups.
Conclusions
SS had an impact on the degree of spondylolisthesis and on pedicle morphological parameters in patients with DLS, with greater slope resulting in greater impact. The progression of DLS occurred due to the increasing forward shear force of the vertebra being greater than the reverse resistance. The pedicle at the slip level adaptively remodeled, becoming slenderer and tilting inward due to the long-term traction of the two opposing forces.
Keywords
Introduction
Degenerative Lumbar Spondylolisthesis (DLS) is a degenerative disorder defined by Newman 1 as the slippage of a vertebra relative to the adjacent vertebra below it, without a defect of the pedicle isthmus. DLS generally develops in the L4 and L5 vertebra of people over 50 years old. Although its etiology is still controversial, several factors reportedly may affect the development of DLS, including sagittal pelvic imbalance, orientation of the lumbar facet joints, osteoporosis, obesity, and paravertebral muscle atrophy.2-4
Previous literature has explored the influence of spinopelvic sagittal imbalance on DLS development.2,3 Some studies have also suggested that DLS may affect spinopelvic sagittal alignment.5-7 Recently, Tang et al. 8 found a difference in the pedicle morphological parameters between people with DLS and a control group. They believed that there was an adaptive remodeling in the pedicle due to shear stress at the slip level. However, few studies have been reported regarding the effect of spinopelvic sagittal parameters, especially sacral slope (SS), on the percentage of slip distance (SDP) and on pedicle morphological parameters.
Our study had several objectives: to measure the SS, SDP, and pedicle morphological parameters of L4 vertebra in patients with DLS using X-ray and CT images; to compare differences in SDP and pedicle parameters among three SS groups according to the spinopelvic classification proposed by Roussouly et al. 9 ; to clarify the correlation between the SS and SDP, as well as between the SS and the pedicle parameters of the L4 vertebra; and to analyze the mechanism and explore its clinical significance.
Materials and Methods
The study was approved by the ethics committee of our institution. Since this was a retrospective radiographic study, written informed consent was waived. We systematically reviewed medical records and images of all patients with DLS from August 1, 2018, to September 30, 2021. Additionally, a retrospective cross-sectional study was performed. Using the inclusion and exclusion criteria, we enrolled 134 patients in the study (Figure 1). Flowchart demonstrating the inclusion results of research subjects. LSS, low sacral slope; MSS, mean sacral slope; HSS, high sacral slope; SS, sacral slope.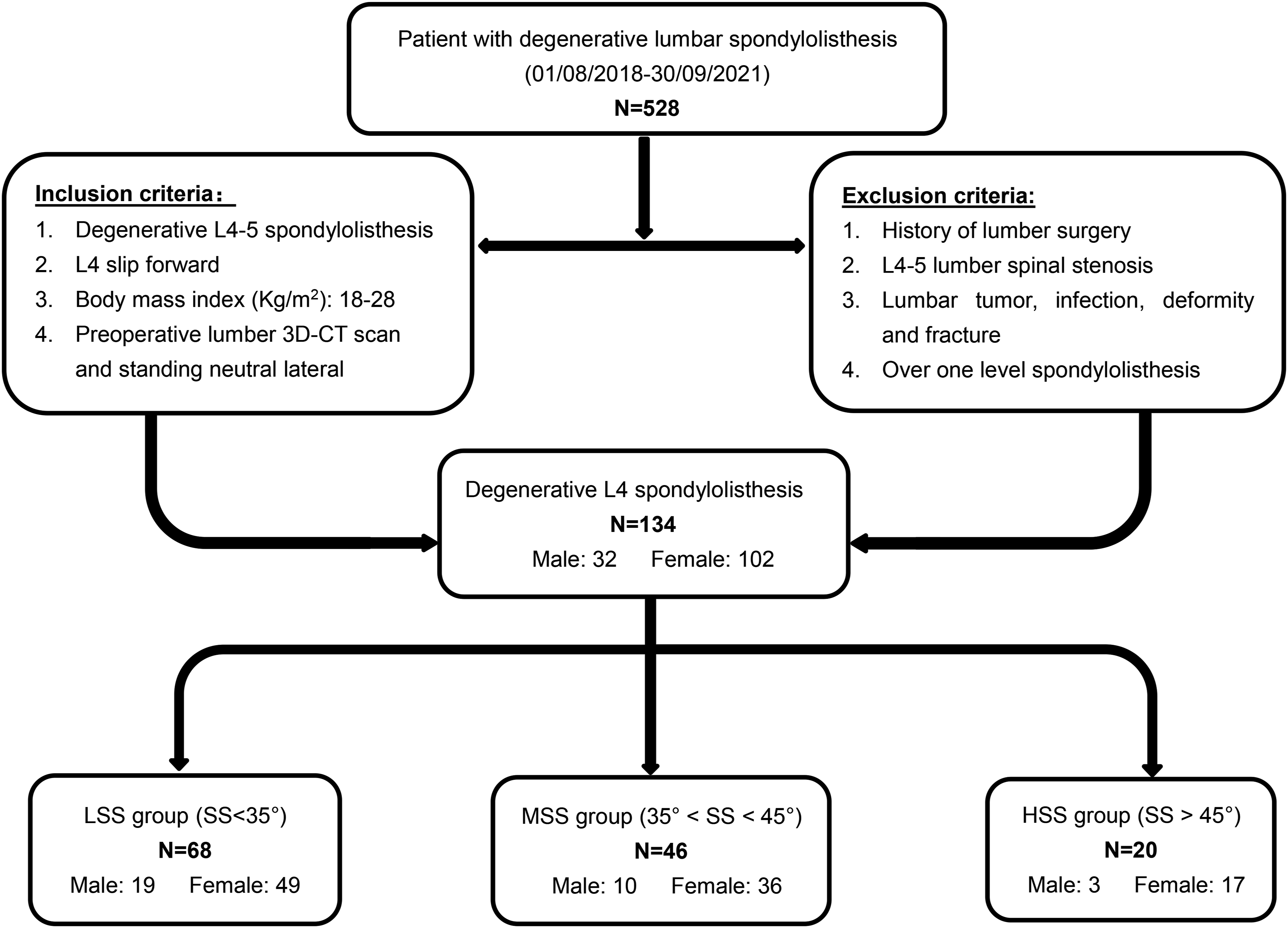
We used the multi-slice spiral computed tomography scanner (United Imaging, China) to scan the patient’s lumbar spine in the supine position before surgery. Both the slice thickness and slice interval were 1 mm. In addition, we used data from a lateral radiograph of the lumbar spine taken in the standing neutral position. Images were reconstructed using a postprocessing workstation. Additionally, we measured all imaging data on a workstation (Syngo, Siemens), which provides an accuracy of 0.1 mm for distance and 0.1° for angle.
Pedicle parameters were measured in accordance with previous method described by Olsewski et al.
10
and Vaccaro et al.11,12 First, we drew the following reference lines on the axial CT images: the first line (A line) was drawn to connect the bilateral transverse processes, the second line (B line) was drawn perpendicular to A line dividing the vertebral body equally on the central axis, the third line (C line) was drawn tangent to the posterior edge of the vertebral body, and the last one (D line) parallel to the pedicle was drawn via the central axis of the pedicle. The parameters of pedicle length, pedicle screw trajectory length, pedicle width, and pedicle camber angle were measured on the mid-pedicle cut image. Pedicle height was measured on the middle sagittal plane of the pedicle using CT images (Figure 2). The SS was the angle between the superior endplate of S1 and the horizontal plane on X-ray images.
13
Additionally, according to the method proposed by Bourassa-Moreau et al,
14
the SDP was calculated as the ratio of the length of the slip distance of the L4 vertebra to the length of L5 endplate on lumbar radiograph. Diagram showing the reference lines and measurement of pedicle parameters. (a) Pedicle length (PL): the distance between A line and C line in the longitudinal pedicle axis line (yellow arrow); pedicle screw trajectory length (PSTL): the distance between A line and the anterior margin of the vertebral body in the central axis of the pedicle (red arrow); pedicle width (PW): the width of the narrowest part perpendicular to D line (blue arrow); pedicle camber angle (PCA): the angle between B line and D line (green arrow). (b) Pedicle height (PH): the shortest distance between the superior and inferior cortices of the pedicle in sagittal CT images (red arrow). Correlation between SS and L4 pedicle parameters in three groups. SS was significantly positively correlated with PL (A), while negatively correlated with PW (B), PH (C), and PCA (D). PL, pedicle length; PW, pedicle width; PH, pedicle height; PCA, pedicle camber angle.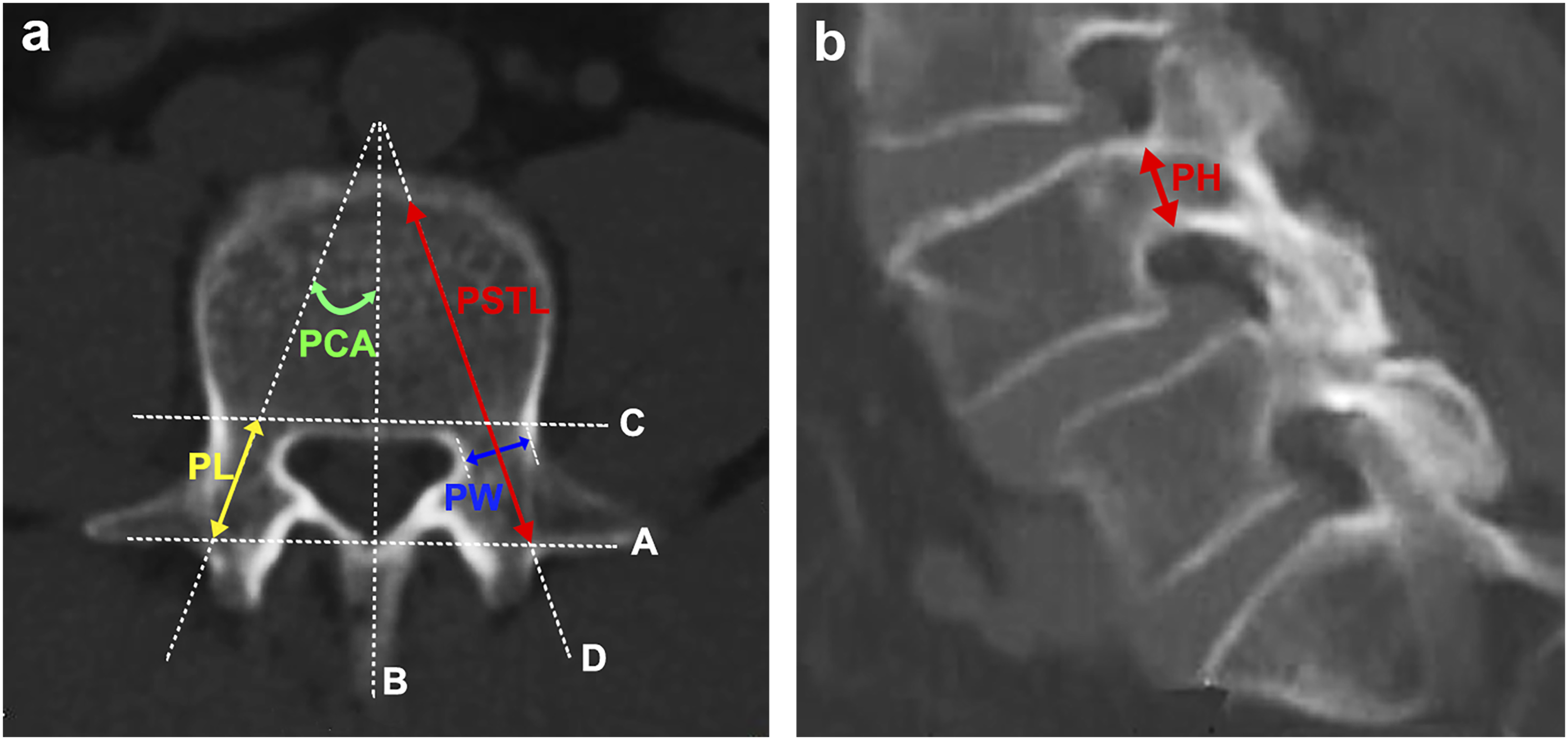
All parameters were measured by two well-trained physicians, and mean values of the right and left sides of L4 pedicle morphological parameters were calculated. The severity of spondylolisthesis was classified as grade I, II, III, or IV according to the Meyerding system of classification. The following general characteristics were recorded: age, sex, height, weight, and body mass index (BMI). Patients were grouped by degree of SS using the system proposed by Roussouly et al. 9 : the low sacral slope (LSS) group had SS values of less than 35°; the mean sacral slope (MSS) group had SS values of 35°–45°, and the high sacral slope (HSS) group had SS values greater than 45°.
Statistical Analysis
We used SPSS 26.0 software (SPSS, Chicago, IBM, USA) to perform statistical analysis. All data were expressed as the mean ± standard deviation. Differences in pedicle parameters based on side (right or left) and sex (male or female) in the three groups were compared using the independent samples t-test. An analysis of variance was performed to compare the value of pedicle parameters and general characteristics (age, height, weight, and body mass index) in different groups. For post-hoc multiple comparisons of all individual group, we used the Least Significant Difference Test. Correlational analyses were performed using the Pearson correlation coefficient. The Chi-square test was used to compare categorical variables. A P-value < 0.05 was considered statistically significant.
Results
Clinical characteristics among the three groups.
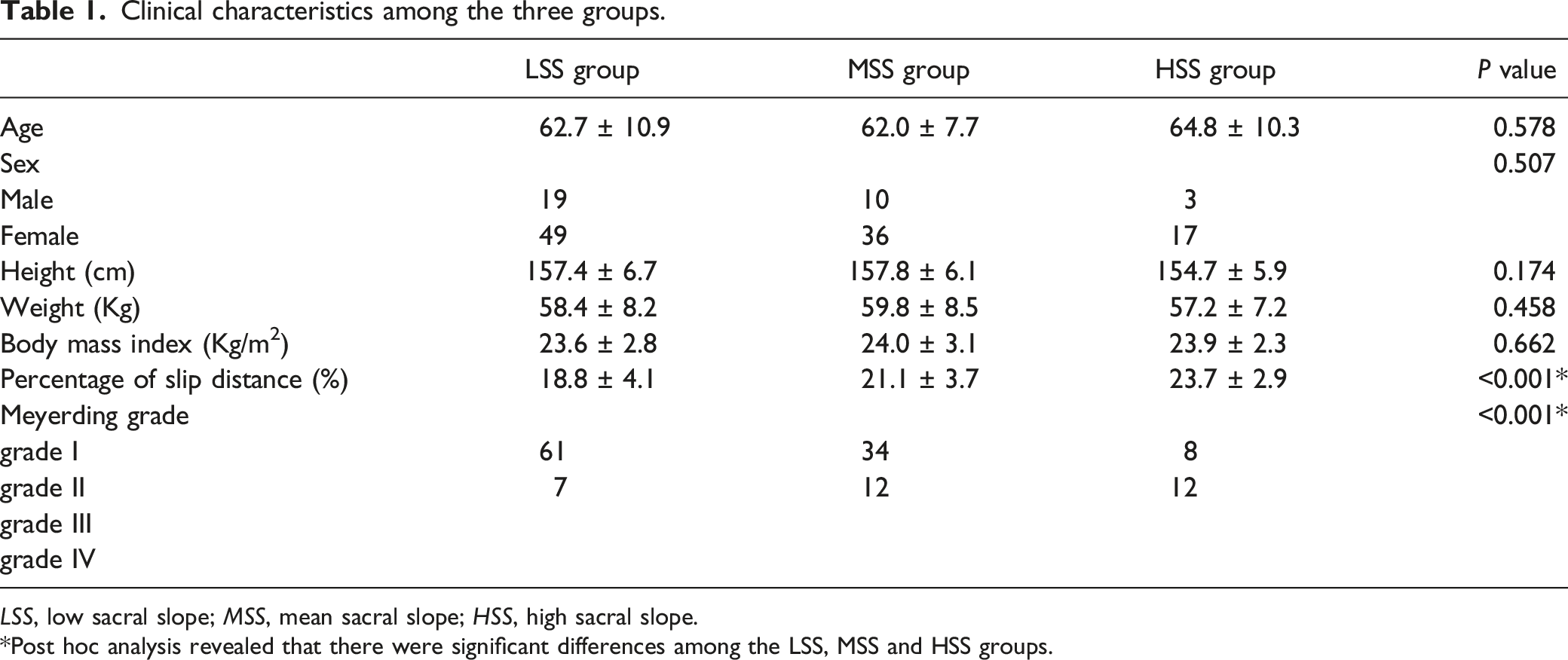
LSS, low sacral slope; MSS, mean sacral slope; HSS, high sacral slope.
Post hoc analysis revealed that there were significant differences among the LSS, MSS and HSS groups.
Difference of L4 pedicle parameters in side and sex.
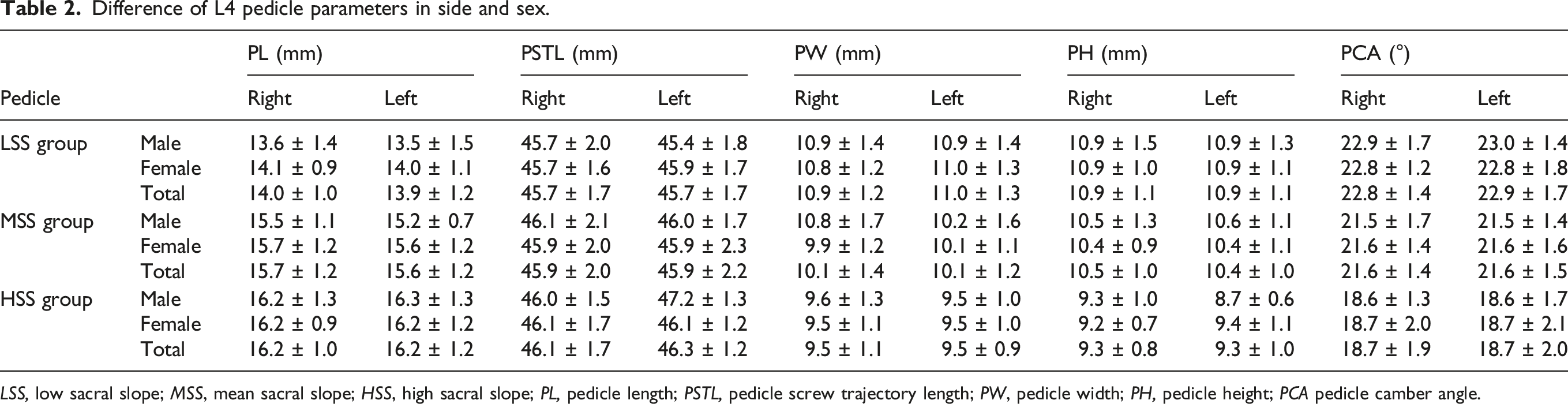
LSS, low sacral slope; MSS, mean sacral slope; HSS, high sacral slope; PL, pedicle length; PSTL, pedicle screw trajectory length; PW, pedicle width; PH, pedicle height; PCA pedicle camber angle.
Comparison of L4 pedicle parameters among the LSS, MSS, and HSS groups
Difference of L4 pedicle parameters among the LSS, MSS, and HSS groups.
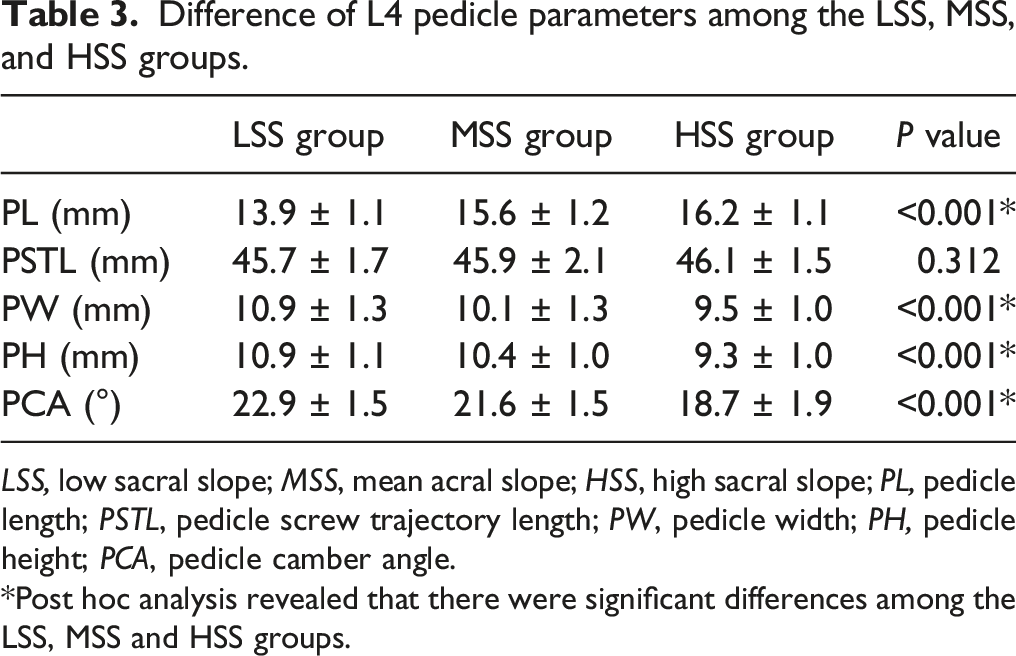
LSS, low sacral slope; MSS, mean acral slope; HSS, high sacral slope; PL, pedicle length; PSTL, pedicle screw trajectory length; PW, pedicle width; PH, pedicle height; PCA, pedicle camber angle.
Post hoc analysis revealed that there were significant differences among the LSS, MSS and HSS groups.
Correlation between SS and the degree of spondylolisthesis, and between SS and pedicle morphological parameters of the L4 vertebra in the three groups
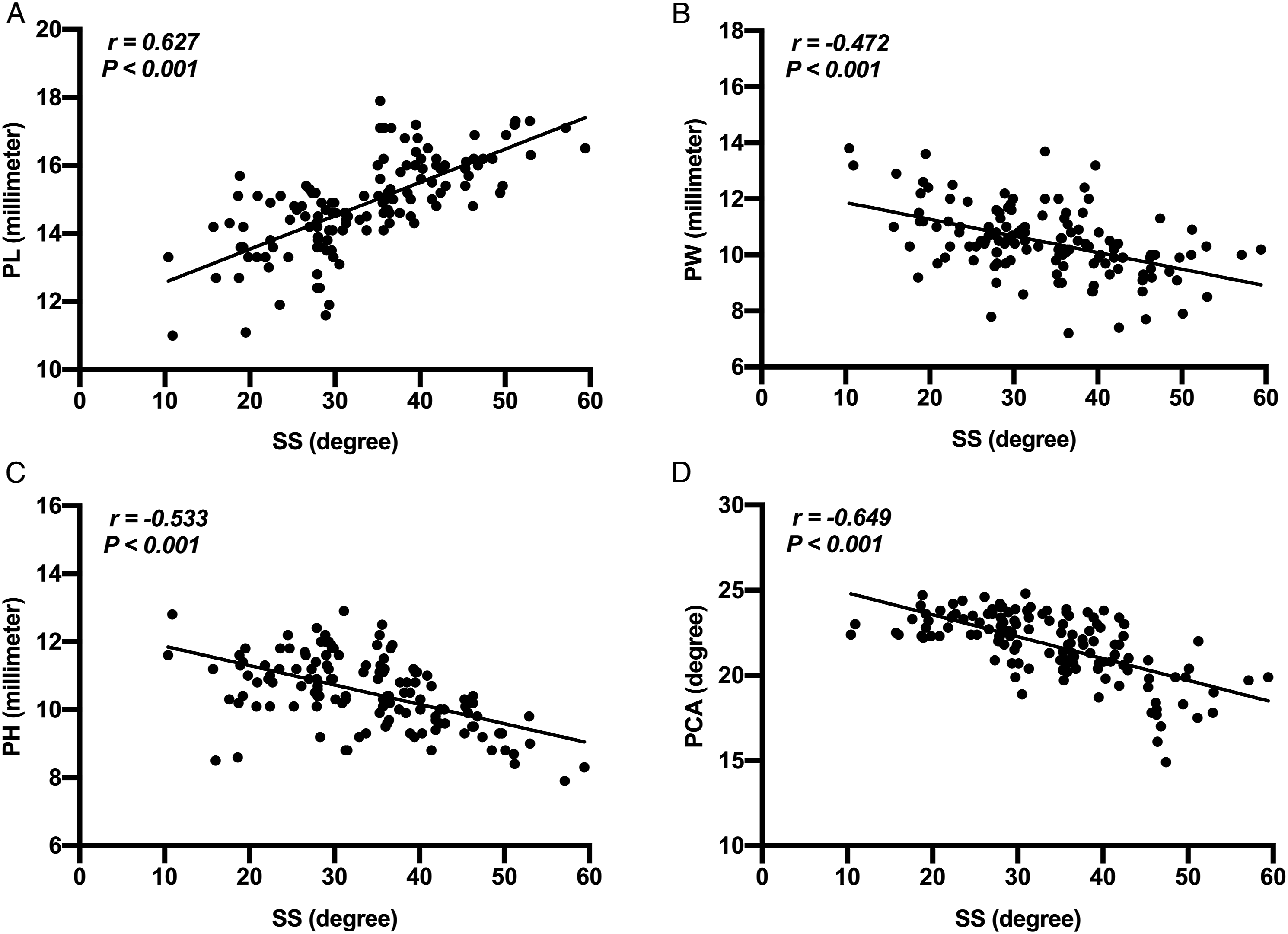
Pearson’s correlation analysis showed that the SS was significantly positively correlated with the SDP of the L4 vertebra (r = 0.540, P < .001).
Furthermore, the SS was significantly positively correlated with pedicle length (r = 0.627, P < .001), and it was negatively correlated with pedicle width (r = −0.472, P < .001), height (r = −0.533, P < .001), and camber angle (r = −0.649, P < .001) (Figure 3).
Discussion
In present study, we found that SS was correlated with the degree of spondylolisthesis as well as with morphological parameters of the pedicle. SS, a sagittal morphologic parameter of the pelvis, has an impact on the balance of the spine and pelvis. Legaye et al. 15 demonstrated that the shape of the pelvis was significantly correlated with SS and pelvic tilt, and SS was also closely related to lumbar lordosis. To further investigate the relationship between lumbar degenerative disease and SS, Roussouly et al.9,16 classified four types of spinopelvic sagittal alignment according to the value of SS and lumbar lordosis curves. Moreover, they identified different degenerative disorders associated with different spinopelvic types.2,9,17,18 Other studies have reported a correlation between degenerative spinal diseases and SS. Lim et al. 19 compared the SS of people with DLS to that of the normal population and found that patients with DLS had a significantly greater SS (33.6° ± 9°) than the normal population (29.6° ± 8°). Funao et al. 20 and Lai et al. 3 also reported similar results in their study and proposed that a greater SS may be a predisposing factor for the development of DLS.
DLS is a common lumbar disease in the elderly, and surgical intervention is necessary for many patients. The pedicle screw is an auxiliary tool essential to establishing spinal stability. Morphological characteristics of the pedicle greatly impact appropriate selection and accurate implantation of the pedicle screw. Recently, Tang et al. 8 found that pedicle morphological parameters in patients with DLS were different from those of a normal population and changed with the degree of slip, thereby affecting implantation of pedicle screws. While previous studies have reported that a greater SS may be a predisposing factor for DLS, our study contributed to the body of knowledge about the impact of SS on both the degree of slip and the pedicle morphological parameters.
Our study featured 134 patients with average values of SS (33.6° ± 9.7°), which was consistent with the previous study results. 19 We found that compared with the HSS group, the SDPs in the LSS group and MSS group were significantly smaller, and a similar difference was found in the LSS group compared to the MSS group. Furthermore, SDP was significantly correlated with SS, indicating that higher SS may be an important factor in DLS development. Finally, by analyzing the differences of morphological parameters of the L4 pedicle among different groups, we found that compared with LSS and MSS groups, the L4 pedicle in the HSS group had a significantly longer pedicle length, smaller pedicle width and camber angle, and lower pedicle height. Moreover, pedicle parameters in the MSS group showed similar changes compared with the LSS group. Notably, no previous studies have reported the pedicle morphological difference in L4 vertebra relative to different values of SS in patients with DLS.
In our study, the average pedicle camber angle in the HSS group (18.7°) was significantly smaller than in the LSS (22.9°) and MSS groups (21.6°). Nojiri et al. 21 used CT images to measure the axial angle of the pedicle in 136 patients with lumbar diseases and found that the angles in the DLS group and lumbar stenosis group were significantly smaller than those in the normal population. Yu et al. 22 used CT images to measure the safe range of pedicle screw placement in 40 adult volunteers. They found that under the Du, Magerl, and Roy-Camille’s measurement techniques, the safe range of the axial angle of L4 pedicle was 12.82° ± 0.92°, 12.49° ± 0.82°, and 7.86° ± 0.95°, respectively. The differences in the axial angle of the pedicles in different degrees of SS should be considered when placing pedicle screws, because the precise orientation of the screw is necessary to avoid misplacement.
Why are there differences in pedicle morphology among LSS, MSS, and HSS groups in DLS? We propose the following answer: First, there is a great difference in the sagittal biomechanical balance of the lumbar spine in different degrees of SS. Roussouly et al.
9
have proposed that the force exerted on the lumbar spine is the sum of vectors of gravity and muscular force (G). The force exerted on each vertebra may be divided into two forces when standing: a forward shear force, parallel to the vertebral endplate (F1), and a compression force perpendicular to the plate (F2). Roussouly et al.
9
and Lai et al.
3
developed a static equation for force on the lumbar spine as
In addition to impacting DLS, SS can significantly determine the degree of lumbar lordosis. Stagnara et al.
23
demonstrated the relationship between SS and lumbar lordosis; the more the sacrum was tilted, the greater the lumbar curvature, while a more horizontal SS resulted in a flatter lumbar curvature. For each lumbar functional unit, stress acts mainly on the disc and vertebrae in low lumbar curvature. An increase in lumbar curvature will cause the lumbar gravity line to move backwards
9
; thus, the more the lumbar spine is curved, the greater the impact of the shear stress exerted on the pedicle (Figure 4). In our study, the apparent changes of the pedicle morphology in the MSS and HSS groups compared with the LSS group support this view. Illustration demonstrating mechanics analysis of the L4 vertebra in different degrees of SS. G, the sum of vectors of gravity and muscular force; F1, a forward shear force parallel to the vertebral endplate; F2, a compression force perpendicular to the plate; α, the angle between F1 and G. Shear force (F1) increases with increasing SS, leading to progression of slip. The more tilted the sacrum, the greater the lumbar curvature, and the stress point is backward and closer to the pedicle.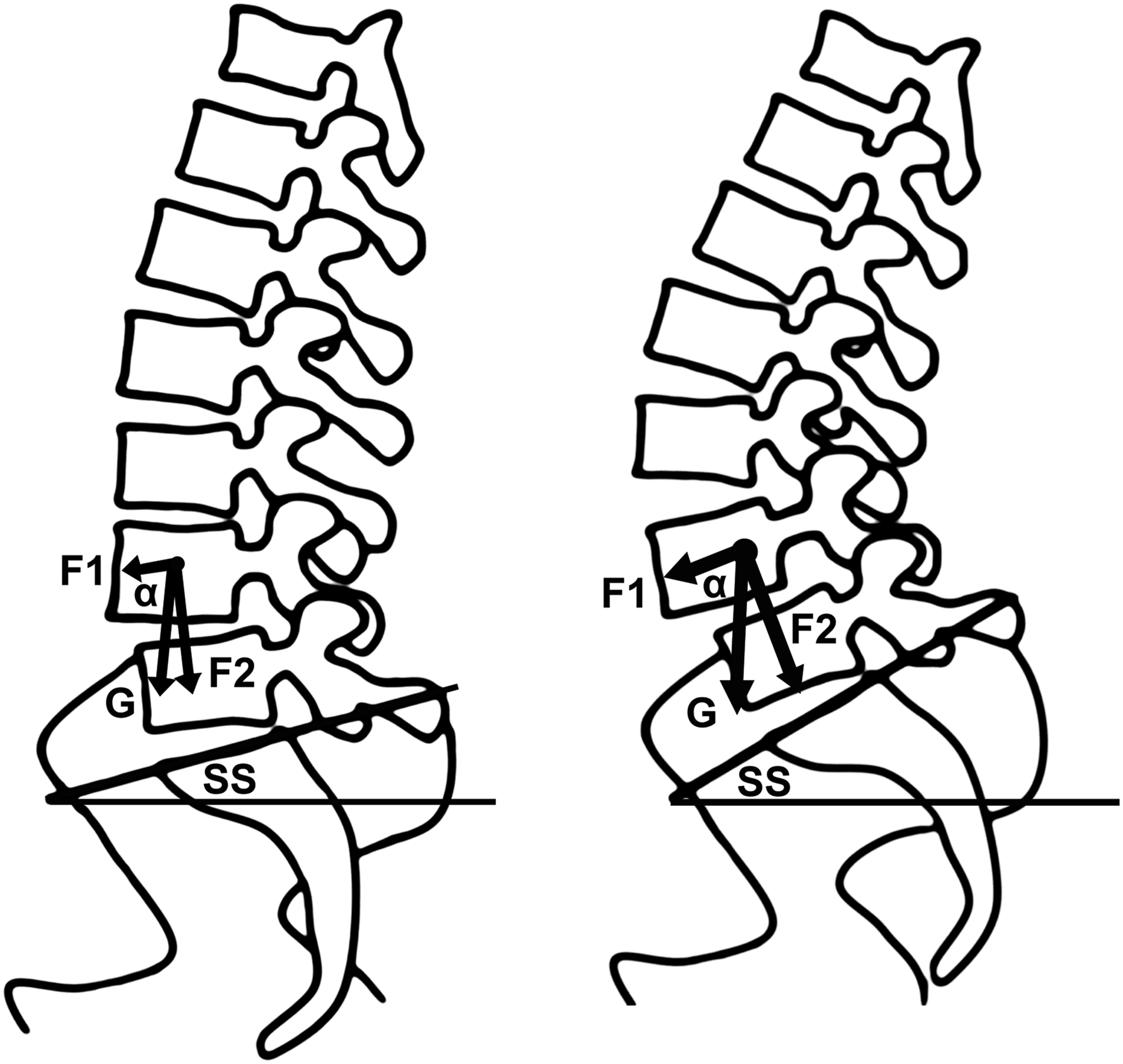
Second, the intervertebral disc is considered indispensable to the maintenance of spinal stability, and abnormal stress on it can result in adaptive remodeling of the vertebral arch. The disc acts as a bridge connecting two adjacent vertebrae, and the semi-liquid composition of the nucleus pulposus distributes the pressure and balances the force on the whole intervertebral disc. Research shows that an intact disc is a restraint force against further slippage and maintains the stable balance of spinal segments.4,24,25 In patients in our study, they were similarly accompanied by the degeneration of the intervertebral disc below the slip vertebra, supporting the theory that disc degeneration is associated with the biomechanical changes in the lumbar and related to the progression of slippage. We propose that the greater the tilt of the sacrum, the greater the anterior shear forces on the lumbar functional units. Meanwhile, backward movement of the stress point causes the intervertebral disc to sustain abnormal compressive forces and shear forces, which accelerates the degeneration of the posterior intervertebral disc below the slip level. With the acceleration of disc degeneration, its capacity to maintain spinal stability is greatly weakened. Therefore, as the spondylolisthesis becomes unstable and progresses, the intact vertebral arch shows an adaptive remodeling due to increasing abnormal stress traction.
Finally, the posterior facet joint and ligaments also play an essential role in resisting the progression of spondylolisthesis.26,27 When the forward shear force of the vertebra increases and causes the progression of slippage, the pedicle serves as the mechanical bridge between the vertebral body and the posterior facet joint, and can resist the forward shear force through the backward resistance of the facet joints and ligaments. Research has shown that the morphology of the facet joints at the slip site in DLS differs from that of normal people, and the change of orientation in the sagittal plane and axial plane is further modified by DLS. Thus, we propose that the pedicle undergoes stress remodeling due to the traction of two long-term opposite forces. The causality between facet joint morphology and DLS is still controversial. However, we noticed degenerative manifestations such as articular surface hyperplasia and sclerosis in the facet joints of our study subjects, supporting the idea that the change is partially a result of stress remodeling (Figure 5). Illustration showing the force and adaptive remodeling of the pedicle in degenerative lumbar spondylolisthesis (DLS). Green arrow indicates the forward shear force of the slipped vertebra; blue arrow, the abnormal compression force, which accelerates the disc degeneration below the slip level and weakens its capacity to maintain stability (yellow arrow); purple arrow, the backward reverse force of the posterior facet joints and ligaments; and red arrow, the adaptive remodeling of the pedicle at the slip level. White circle and white arrow indicate the stress degeneration of facet joints in sliding vertebra with serious hyperplastic and sclerotic in the sagittal plane and axial plane, respectively.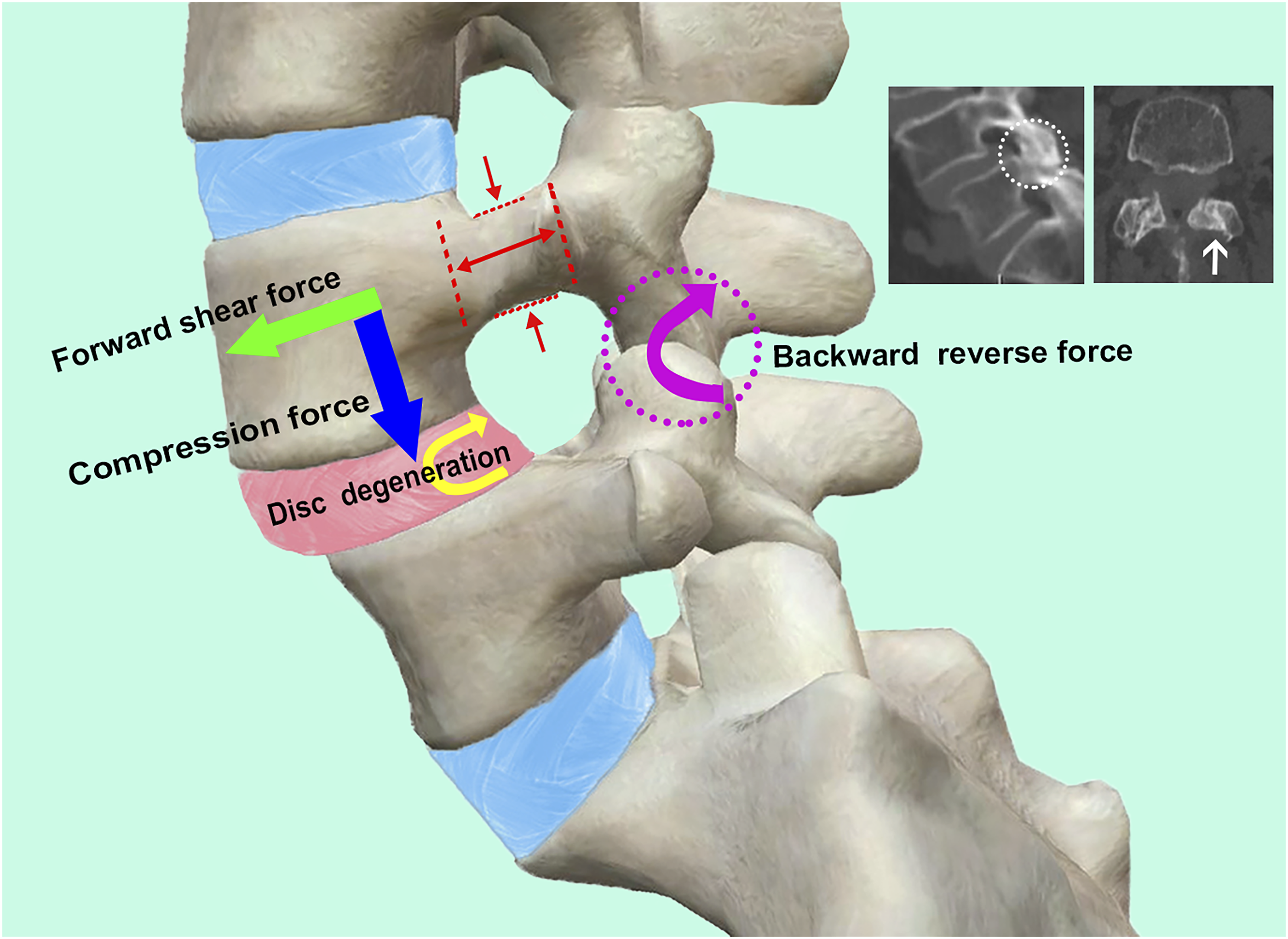
Previous studies at the slip level of DLS have shown that the joint space is significantly narrowed, the facet joint surface is hyperplastic and sclerotic, and the degree of facet osteoarthritis is more severe than normal population.28,29 Tang et al. 8 proposed that the facet degeneration in the slip segment was a self-protection mechanism, when the slippage progresses. In addition, Cho et al. 28 proved that the amount of facet fluid was related to the degree of slip in DLS, and they considered that this facet degeneration was caused by increased facet load. Chuang et al. 7 reported that sagittal lumbosacral imbalance usually results in tension over the facet joints and overuse of muscles, which is related to low back pain. Based on the above evidence, we speculate that people with a more tilted orientation of the sacrum are more likely to have low back pain after lumbar activities compared to people with a lesser degree of SS.
Our study had some limitations. First, a small number of cases, lack of normal population comparison, were included in this single-center, retrospective study. Second, our study did not include people with isthmic spondylolisthesis because we suspected that, due to the early fracture of the isthmus in this type of spondylolisthesis, the influence of mechanical force on the pedicle could be limited. Further research is needed to verify this hypothesis.
Conclusion
In summary, sacral slope has an impact on the degree of L4 vertebrae slippage and pedicle morphological parameters of DLS. In the case of greater sacral tilt, the following progression of sagittal biomechanical changes occurs in the slipped vertebra: 1) the forward shear force of the slipped vertebra increases; 2) the gravity line of the lumbar is backward and closer to the pedicle due to the increase in lumbar curvature; 3) the acceleration of intervertebral disc degeneration weakens its capacity to maintain stability and resist the forward shear force; 4) the posterior facet joints and ligaments exert a reverse force to resist the forward shear force; 5) the progression of spondylolisthesis occurs when the forward shear force of the vertebra is greater than the reverse resistance. The intact pedicle is subject to the forward shear force of the vertebrae and the backward reverse force of the facet joints and ligaments. Under the long-term traction of two opposite forces, the pedicle at the slip level adaptively remodels to become slenderer and more tilted inward. Our study confirmed that the pedicle parameters of pedicle length, width, camber angle, and height were significantly correlated with SS, and the SDP was also significantly correlated with SS. This finding supports our view that the stress change caused by increase in degree of SS is an important reason for the adaptive remodeling of the pedicle during the progression of DLS. To the best of our knowledge, this is the first report to demonstrate the effect of SS on the degree of slip and pedicle morphological parameters in DLS. The information obtained in this study may help clarify the mechanism of the onset and development of DLS, and the measurement of the SS and pedicle morphologic parameters is helpful for the assessment of the sagittal balance of the spinopelvic structure and for guiding accurate pedicle screw placement.
Footnotes
Acknowledgments
The authors would like to thank all the patients of the Affiliated Hospital of Southwest Medical University for allowing to publish the paper and to use their images taken during hospital admission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Approval was obtained from the Institutional Review Board (No. KY2022058).
Informed Consent
Since this was a retrospective radiographic study, written informed consent was waived.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.