
Abstract
Study Design
Prospective observational cohort.
Objectives
To examine the cost-effectiveness of IntraOperative ElectroMyeloGraphy (IO-EMG) by evaluating how often an abnormal IO-EMG signal changed the surgeon’s surgical plan, or replaced a pedicle screw either intra-operatively or as a second unplanned surgery.
Methods
Patients undergoing instrumented posterolateral lumbar fusion were monitored with intraoperative triggered EMG’s. Pedicle screws were placed freehand from L1 to S1 by attending physicians and fellows. Concern for pedicle breach was a screw stimulation<10 mA.
Results
There were 145 cases with a total of 725 pedicle screws placed. Mean age was 57.8 ± 14.2 yrs, OR time was 238 ± 95 minutes, EBL was 426.8 ± 354.3cc. Mean number of surgical levels fused was 2.7 ± 1.1. 686 (95%) screws stimulated at >10 mA and 39 (5%) screws stimulated at <10 mA. All 39 screws were removed and pedicles re-examined. Intraoperative screw repositioning was necessary in 8 of 145 cases (6%). No patient required a return to the OR for screw repositioning. As a worst case cost analysis, assuming the 8 patients requiring intraoperative screw positioning would have returned to the OR at a cost of $11,798 per readmission, the per patient cost is $651 which is less than the ION per patient cost of $750.
Conclusions
Only 1% of the 725 lumbar pedicle screws placed in 8 of 145 cases required repositioning. Due to the infrequency of pedicle wall breaches and the cost of ION, the utility of this modality in straightforward lumbar fusions should be critically evaluated.
Introduction
With the increasing numbers of spine surgery performed in the US in the last few years, 1 the incidence of perioperative neurologic deficits also increased by 54% from .68% in 1999 to 1.05% in 2011. 2 As a result, intraoperative neuromonitoring (IONM) was introduced initially in the 1970s to reduce neurologic deficits. 3 IONM has had significant technologic advancements over the past few decades, which led to its increased utilization.
Combined somatosensory-evoked potentials (SSEPs) and motor-evoked potentials (MEPs) in IONM help prevent irreversible neurologic injury, especially in complicated spinal deformity surgery.4,5 On the other hand, evoked electromyography (EMG) in IONM is commonly used as a means for assessing the accuracy of pedicle screw placement during instrumented spine fusion. 6 Recent studies have questioned the reliability of EMG due to its low specificity (19% to 73%).7,8 EMG also has an inherently low signal-to-noise ratio, making interpretation challenging. 9 Additionally, it relies on the quality and experience of the neuromonitoring technician.
The cost effectiveness of IONM has been debated for decades.10,11 IONM is important in detecting and preventing neurologic deficit following pediatric and adult deformity correction, revision surgeries, and vertebral osteotomies.12,13 However, intraoperative EMG (IO-EMG) in detecting pedicle screw malposition has limited benefit in routine uncomplicated posterolateral spine fusion due to relative infrequency of neurologic complication. 14 The objective of this study is to determine if IO-EMG is to examine the cost-effective of IO-EMG by evaluating how often an abnormal IO-EMG signal changed the surgeon’s surgical plan, or the surgeon replaced a pedicle screw either intra-operatively or as a second unplanned surgery.
Materials and Methods
Study Design and Patients
After receiving Institutional review Board Approval patients undergoing instrumented posterolateral fusion with traditional pedicle screw trajectory for degenerative conditions at a single multi-surgeon spine center between 2017 and 2018 were identified. Patients undergoing non-elective cases, adult or pediatric deformity cases, fusion for tumor, trauma or infection were excluded.
Surgical Technique and Intraoperative Care
Posterior instrumented spinal fusions were performed prone on a Jackson table with the abdomen free. A forced-air warming device was used to maintain normothermia. A standard open midline approach was utilized, intertransverse fusion beds were prepared uniformly, and pedicle screws were inserted in the standard fashion using anatomical landmarks from L1 to S1. Postero-anterior (PA) and cross-table lateral x-rays were taken to check instrumentation positioning. Additionally, each pedicle screw was stimulated with triggered EMG following return of full motor twitches. Concern for pedicle breach was identified with a stimulation value of less than 10 mA. Cases were performed by attending spine surgeons and spine fellows.
Data Collection
Patient demographic and preoperative characteristics were documented. The recorded characteristics included the following: age, sex, diagnosis, height, weight, operative time, estimated blood loss, EMG data, action with EMGs below threshold, use of navigation or fluoroscopy, whether a fellow or attending inserted screws. Cost of the IO-EMG was requested from the Norton Revenue Integrity team. Cost of screw repositioning when required during the same anesthetic or when the patient has to be brought back to surgery to reposition a screw was requested.
Statistical Analysis
The cost-effectiveness of IO-EMG was determined using expected utility value analysis using TreeAgePro by determining the relative rate of identifying a misplaced screw using IO-EMG during the index surgery and the need to take the patient back to surgery to reposition a misplaced screw.
IRB Statement
This study was approved by the University of Louisville Institutional Board under an Expedited Review procedure and granted a waiver of informed consent (HSPPO#16.0145/NHRO#16.N0043).
Results
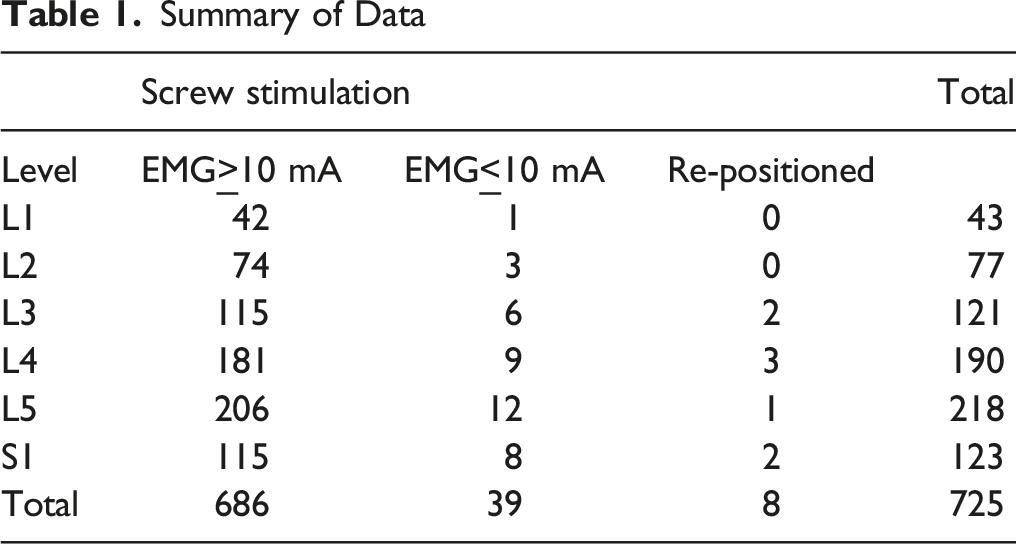
There were 145 cases with a total of 725 pedicle screws placed. Mean age was 57.8 ± 14.2 years, OR time was 238 ± 95 minutes, EBL was 426.8 ± 354.3cc Mean number of surgical levels fused was 2.7 ± 1.1. 686 (95%) screws stimulated at >10 mA and 39 (5%) screws stimulated at <10 mA. All 39 screws were removed and pedicles were re-examined.
Summary of Data
Discussion
IONM has been employed by spine surgeons since the 1970s for both adult and pediatric deformity correction, trauma and tumor resection.15-17 IONM has also been used commonly in elective lumbar fusions. However, in routine lumbar fusion surgeries, controversy exists whether or not IO-EMG can decrease the risk of iatrogenic neurological injury from pedicle screw wall breaches.
While IO-EMG can monitor the integrity of the pedicle wall,18,19 false negative rates can be as high as 3.5%, 20 which render IO-EMG unreliable to surgeons. Similarly, Parker et al looked at 2450 screws, correlated positive IO-EMG readings (<5 mA) with postoperative CT scan, and found a sensitivity of 43.3% of actually having radiographic pedicle wall breaches. 21 Another important factor to consider is that pedicle breaches do not necessarily lead to clinically significant adverse outcomes. Mura et al and Kim et al reported that only .5-2% of patients with malpositioned screws had significant nerve root irritation.22,23
With the advancement of surgical technique and imaging, the rate of neurologic damage is quite low. Our study showed that only 5% of screws had suboptimal (<10 mA) readings. Even after removal and re-examination, 5% of cases required screw repositioning. Similarly, a recent large database study by Ajiboye et al found that the risk of neurologic injury following posterior lumbar fusion was 1.36% with EMG and 1.34% without EMG (24). Furthermore, IO-EMG was unable to decrease incidence of malpositioned percutaneous pedicle screws, while also contributing to increased surgical time. 25 Given IO-EMG’s limited benefit in preventing neurologic complications in routine spine fusions, IONM only adds to cost without significantly improving outcomes. As a worst case cost analysis, assuming that the 8 patients requiring intraoperative screw positioning would have needed a return to the OR instead of having the malpositioned screw repositioned during the index surgery, the cost would be $11,798 per readmission, the per patient cost is $570 which is less than the IONM per patient cost of $750. The recent advent of CT-based navigation and robotic assisted placement of pedicle screws will likely make IO-EMG obsolete.
There are a few limitations of our study. First, cost estimation of IONM is difficult due to the complex involvement of neurophysiology technician and neurophysiologist, actual IONM device, and disposable materials. This could potentially vary widely based on geography. Similarly, hospital readmission and reoperation cost was simplified for cost effectiveness calculation. However, even with the worst-case assumption that all patients with malpositioned instrumentation had revision surgery, IONM failed to show a significant cost benefit. On the other hand, indirect cost from lost wages and the emotional and physical burden of readmission were not included. The economic burden for the hospital and surgeon from potential malpractice litigation could dramatically increase the overall cost. Secondly, the cost-effectiveness calculation may not be generalizable to all practice types as it depends on rate of screw malposition. Tertiary spine centers where CT-based navigation or robots are utilized can have low rate of screw malposition, but community-based spine practices where free-hand instrumentation is predominant can have higher rate of screw malposition, which can find IO-EMG cost effective. Another limitation of this study is the lack long-term patient outcome data on the clinical sequelae of pedicle screw malpositions.
Conclusion
Only 1% of the 725 lumbar pedicle screws placed in 7 of 145 cases required repositioning. Due to the infrequency of pedicle wall breaches and the cost of ION, the utility of this modality in straightforward lumbar fusions should be critically evaluated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
All authors are employees of Norton Healthcare, CY and MB have no relationships to disclose. RKO receives consulting fees from Medtronic and Nuvasive; royalties from Nuvasive, CHC receives consulting fees from Alphatec, DePuy, Medtronic and Nuvasive; royalties from Alphatec and Springer and is a paid speaker for Medtronic and Nuvasive, JLG receives royalties and consulting fees from Acuity and Medtronic; consulting fees from Medtronic, Stryker and Mazor, MD receives consulting fees from Medtronic and Nuvasive, LYC receives consulting fees from the National Spine Health Foundation, All authors’ institution receives grants from OREF, NIH, ISSG, SRS, TSRH, Pfizer, Cerapedics, Medtronic, and Empirical Spine.