
Abstract
Study Design
Retrospective cohort study
Objective
The aim of this study was to determine the incidence of and risk factors for persistent opioid use after elective cervical and lumbar spine procedures and to quantify postoperative healthcare utilization in this patient population.
Methods
Patients were retrospectively identified who underwent elective spine surgery for either cervical or lumbar degenerative pathology between November 1, 2013, and September 30, 2018, at a single academic center. Patients were split into 2 cohorts, including patients with and without opioid use at 180-days postoperatively. Baseline patient demographics, underlying comorbidities, surgical variables, and preoperative/postoperative opioid use were assessed. Health resource utilization metrics within 1 year postoperatively (ie, imaging studies, emergency and urgent care visits, hospital readmissions, opioid prescriptions, etc.) were compared between these 2 groups.
Results
583 patients met inclusion criteria, of which 16.6% had opioid persistence after surgery. Opioid persistence was associated with ASA score ≥3 (P = .004), diabetes (P = .019), class I obesity (P = .012), and an opioid prescription in the 60 days prior to surgery (P = .006). Independent risk factors for opioid persistence assessed via multivariate regression included multi-level lumbar fusion (RR = 2.957), cervical central stenosis (RR = 2.761), and pre-operative opioid use (RR = 2.668). Opioid persistence was associated with higher rates of health care utilization, including more radiographs (P < .001), computed tomography (CT) scans (.007), magnetic resonance imaging (MRI) studies (P = .014), emergency department (ED) visits (.009), pain medicine referrals (P < .001), and spinal injections (P = .003).
Conclusions
Opioid persistence is associated with higher rates of health care utilization within 1 year after elective spine surgery.
Introduction
As of 2017, the cost of opioid use disorder and fatal opioid overdose was estimated to exceed $1.02 trillion, with the primary economic burden stemming from reduced quality of life and value of life lost due to overdose and death. 1 A multitude of factors have contributed to the current crisis, including opioid misuse, opioid abuse, inappropriate prescribing patterns, and a lack of understanding of adverse effects associated with long-term opioid use. 2 Surgical patients are uniquely enveloped in the opioid crisis, as surgeons and health care providers routinely prescribe opioids for management of acute postoperative pain in both opioid-naïve patients and those with prior opioid use. For both groups of patients, surgery represents a critical exposure event that increases the risk of developing opioid persistence or dependence.3,4 Risk factors in surgical patients younger age, smoking, chronic pulmonary disease, fibromyalgia, psychiatric or medical co-morbidities, prior benzodiazepine use, prior opioid use, and extent of operation.4-9
Patients undergoing spine surgery are at particularly increased risk of developing post-surgical opioid dependence, with 6% to 18% of opioid-naïve patients3,10 and of 52% to 64% of patients with prior opioid-use 11 developing opioid persistence. These worryingly high percentages of persistent opioid use may partially be explained by persistent pain after surgery. However, some studies suggest that patients may also be taking opioid medications for reasons other than pain control, such as difficulty sleeping, and may continue taking opioids to avoid experiencing withdrawal symptoms 12-14 Despite our understanding that patient undergoing spine surgery are generally at increased risk of developing persistent opioid use after their operation, the downstream impact of various opioid use patterns on health care utilization after spine surgery has not been well-established. For example, our review of the literature returned only 2 studies that established a relationship between opioid dependence and increased health care utilization up to 15 months after surgery for adult degenerative scoliosis 15 and degenerative lumbar spondylolisthesis. 16 To our knowledge, no study has comprehensively investigated the relationship between opioid persistence in cervical and lumbar spine surgery patients and postoperative health care resource utilization.
The primary purpose this study was to determine the impact of opioid persistence, as defined as at least 1 new opioid prescription after 180 days postoperatively, on post-operative health care utilization in patients undergoing cervical and lumbar spine surgery. Secondary objectives included quantifying the incidence of opioid persistence in patients undergoing cervical and lumbar spine surgery and identifying key predictive and protective factors associated with opioid persistence. We hypothesized that cervical and lumbar patients with opioid persistence would use more health care resources compared to their counterparts who successfully weaned off any postoperative opioid medications.
Methods
Study Population
This study was approved by the Institutional Review Board (IRB) and a waiver of informed consent was granted. A sample of 583 patients who underwent elective spine surgery between November 1, 2013, and September 30, 2018, were retrospectively identified. All patients underwent surgery by 1 of 3 fellowship-trained orthopaedic spine surgeons at our institution.
Inclusion/Exclusion Criteria
Patients were eligible if they were at least 18 years of age and underwent decompression or decompression and fusion for degenerative cervical or lumbar spine disorders with a minimum follow-up of at least 1 year postoperatively. Patients were excluded if they had a non-degenerative diagnosis or underwent emergent surgery. We chose to focus on the degenerative spine population because these patients, in addition to being most prevalent, most commonly received non-operative care prior to surgery. Therefore, we had an opportunity to track opioid use prior to surgery. Tracking opioid use for patients prior to emergency surgery was more variable; therefore, this patient population was excluded. Additionally, patients were excluded if they underwent a fusion of more than 6 levels, as the extent of surgery would make comparison to other degenerative spine patients more challenging.
Predictor Variables
Charlson Comorbidity Index (modified)
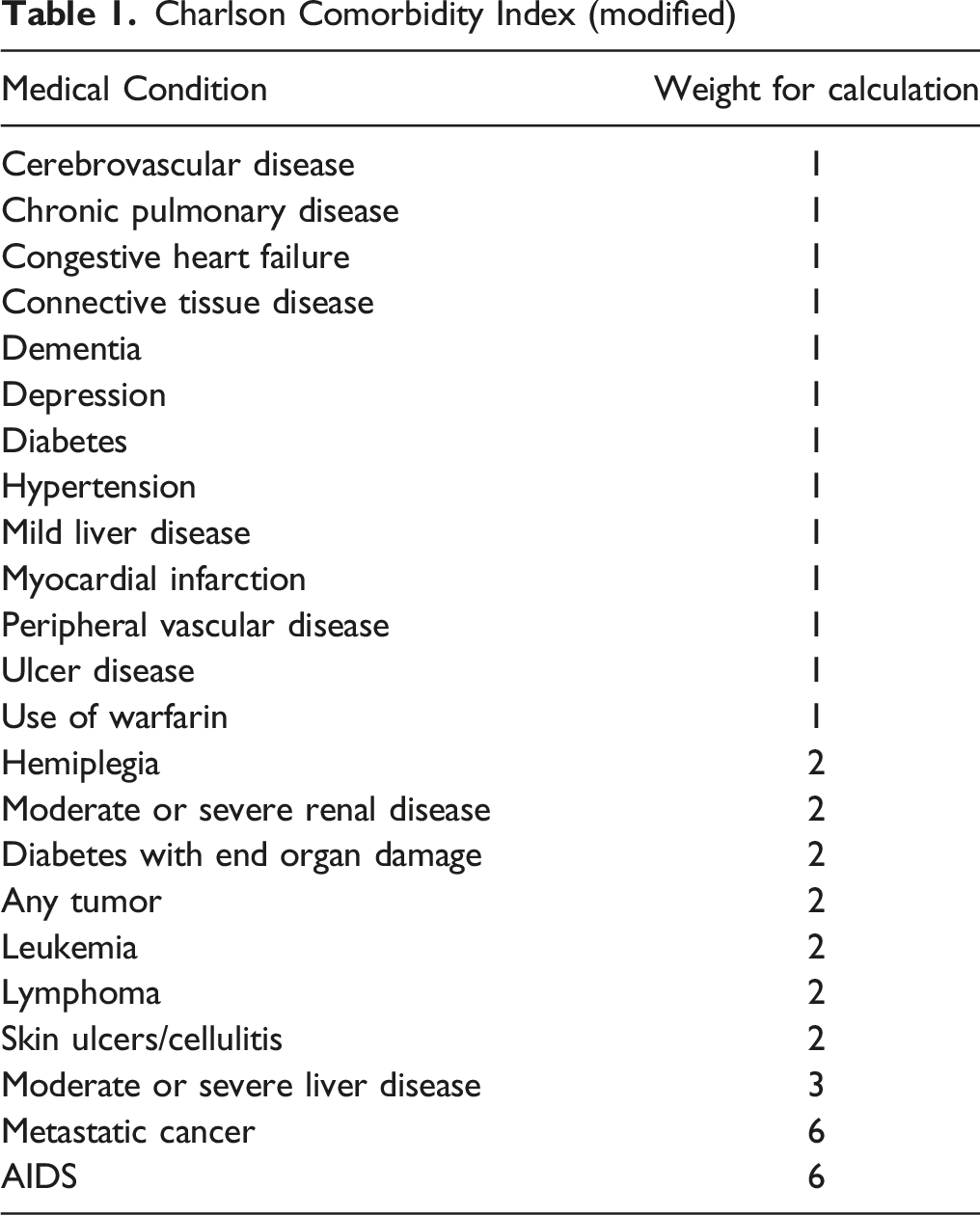
The ASA classification is a tool used to describe and categorize a patient’s physiological status 13 . It has also been shown to be useful in predicting operative risk19,20. ASA scores range from I to VI, in order of worsening health. The CCI is a scoring system that was initially proposed to predict a patient’s mortality within 1 year of hospitalization. 21 The CCI scoring system estimates the degree of a patient’s comorbidity burden; it has been used extensively as a predictor of poor outcomes following a variety of orthopaedic procedures.22-24
Outcome Variables
The number of postoperative opioid prescriptions were totaled at 3 time points: 1) within 90 days, 2) between 90-180 days, and 3) between 180-365 days postoperatively. The electronic medical record (EMR) pertaining to the institution, surrounding academic and private hospital systems participating in the health information exchange platform were reviewed for all opioid prescriptions and healthcare resources utilized. 25 New opioid prescriptions were recorded if the indication was related to postoperative pain. Healthcare resources were recorded if the indication was for routine follow-up or diagnostic workup. Refill orders were reported as a separate prescription. The dose and type of opioid prescribed was not reported. Rather, the total number of opioid prescriptions was used as a proxy for the overall opioid burden for each patient. The main measure of persistent opioid use after surgery was defined as at least 1 new opioid prescription after 180 days postoperatively.
Healthcare Utilization Metrics
Various metrics of healthcare utilization in the first year after index surgery were reported for each patient in the cohort. These included the number of imaging studies – including radiographs (XR), computed tomography (CT) scans, and magnetic resonance imaging (MRI) studies) – emergency department visits, urgent care visits, pain management referrals, and epidural or other spinal injections.
Statistical Analysis
All data was analyzed using the IBM SPSS Version 24 software package (IBM Corporation, Armonk, NY). Chi-squared and Fisher’s exact test, where appropriate, were used to compare categorical predictor variables between patients with and without opioid persistence at 6 months postoperatively. For univariate analysis, sequential binary logistic regression was used to calculate risk ratios (RR) for opioid persistence at 6 months for each individual predictor variable. Variables that were found to be significant in the univariate analysis were included in a multivariate binary logistic regression. Statistical significance was defined as P < .05 for all tests.
Results
Patient Demographics, Comorbidities, and Pre-operative Opioid Use
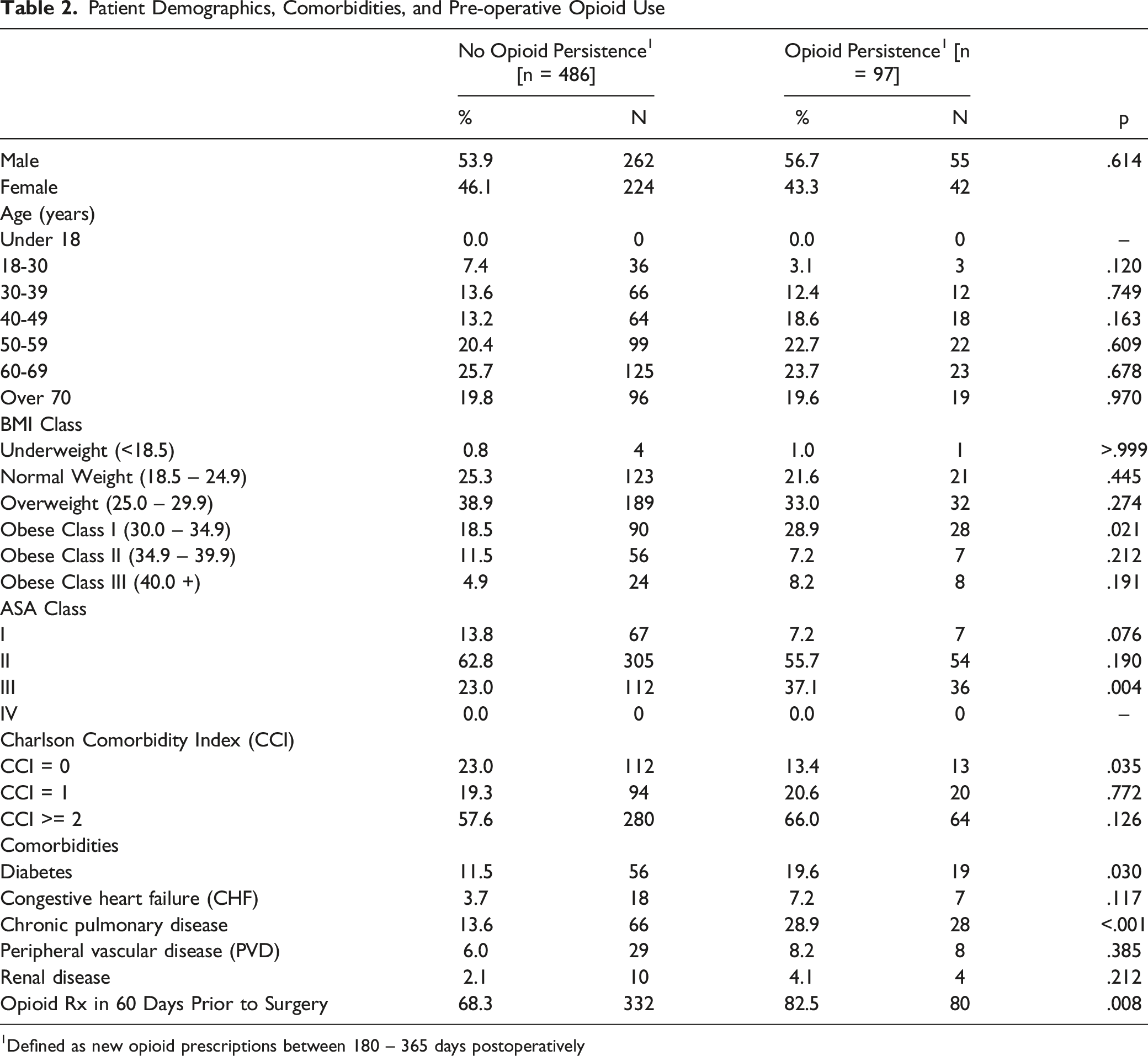
1Defined as new opioid prescriptions between 180 – 365 days postoperatively
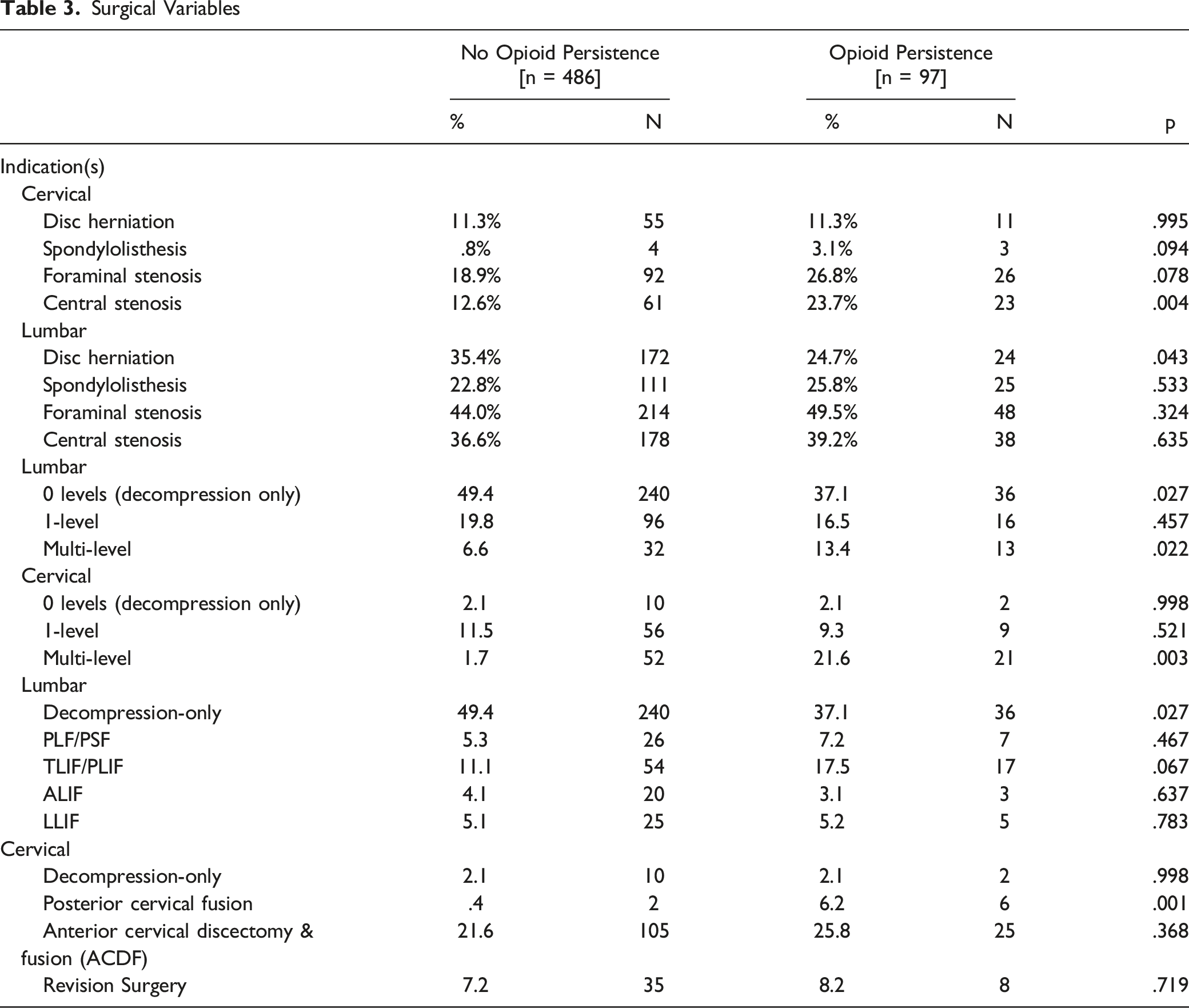
Surgical Variables
Univariate Analysis of Risk Factors for Opioid Persistence
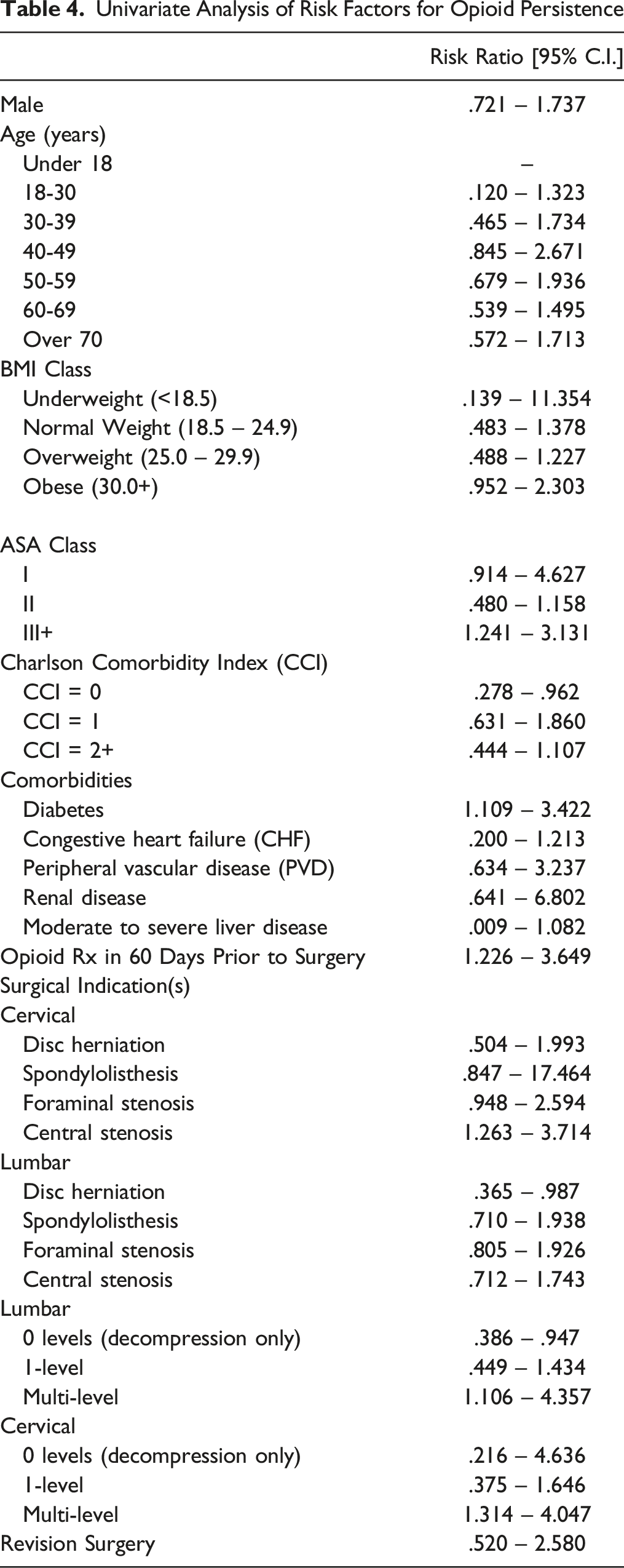
Multivariate logistic regression demonstrated that multi-level lumbar fusion (RR = 2.957, 95% CI: 1.126 – 4.788), cervical central stenosis (RR = 2.761, 95% CI: 1.343 – 4.179), and pre-operative opioid use (RR = 2.668, 95% CI: 1.283 – 4.052) were independent risk factors for opioid persistence following surgery.
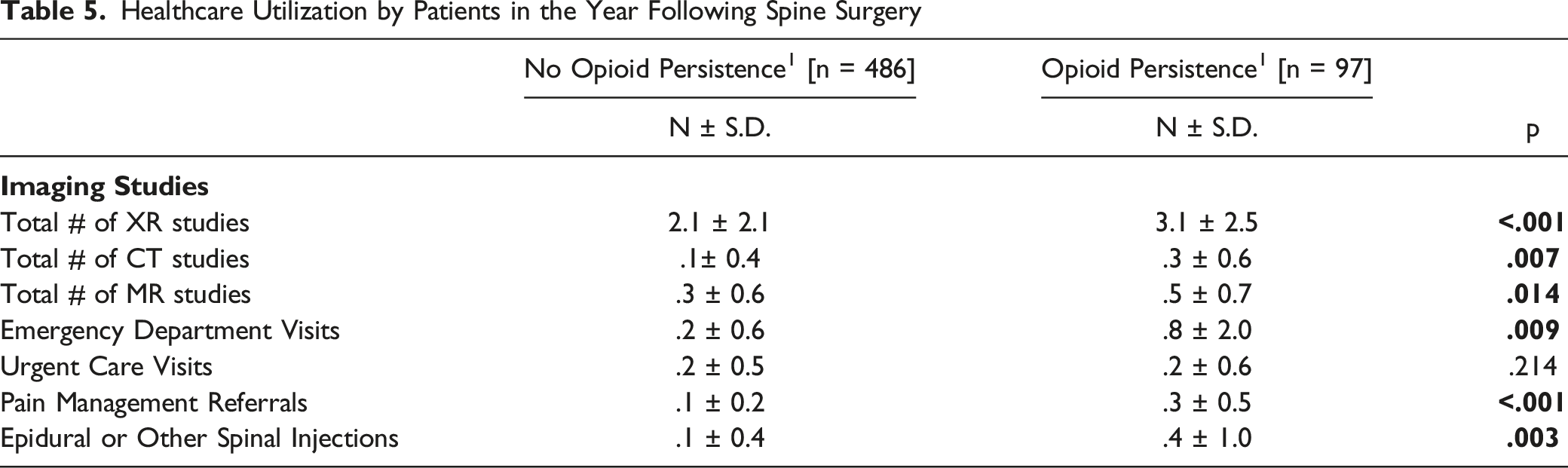
Patients with persistent opioid use were more likely to have higher rates of healthcare utilization in the first year following surgery (Figure 1, Table 5). Specifically, these patients underwent a higher number of imaging studies – radiographs (P < .001), computed tomography (CT) (P = .007), and magnetic resonance imaging (MRI) (P = .014) studies. They also had more visits to the emergency department (P = .009), more pain management referrals (P < .001), and more epidural or other spinal injections (P = .003). Differences in healthcare utilization between patients with and without opioid persistence after surgery. Differences in the mean number of (a) ED and urgent care visits, (b) imaging studies, and (c) opioid prescriptions within 1 year postoperatively. Note: * indicates statistical significance (P < .05); ns = not significant. Healthcare Utilization by Patients in the Year Following Spine Surgery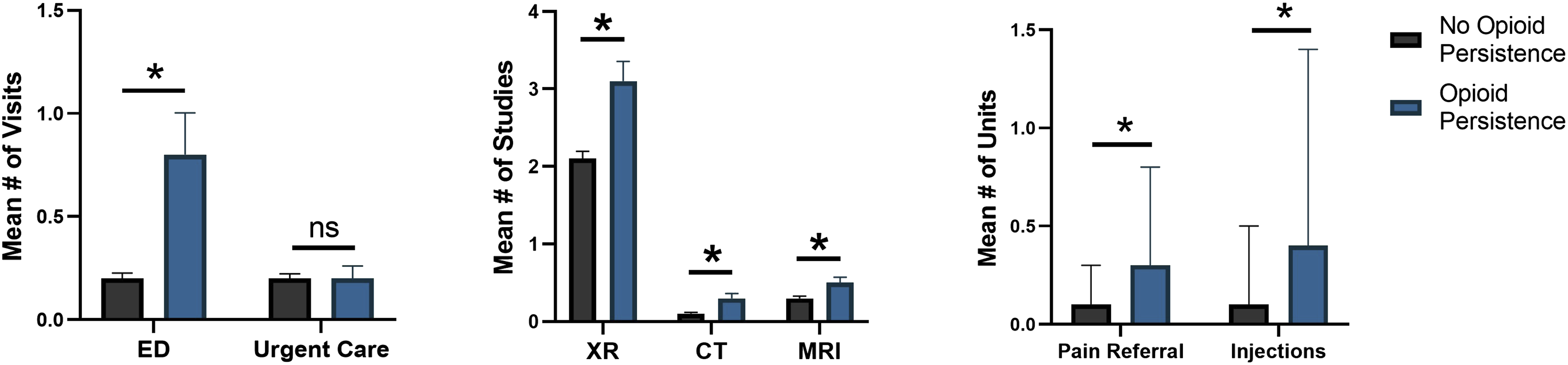
Discussion
Through our single-institution cohort of 583 patients undergoing cervical or lumbar spine surgery, we found that patients with opioid persistence after surgery used more health care resources compared to their counterparts who weaned off all opioid medications by 6 months postoperatively. Persistent opioid users underwent more radiographs, CT scans, MRIs, and incurred more emergency department visits. Moreover, this group experienced more pain management referrals and received more epidural and spinal injections, contributing to an overall greater health care burden.
Our results showed an overall incidence of opioid persistence of 16.6% in patients undergoing spine surgery, with 5.5% in patients who underwent cervical spine surgery and 11.1% in patients who underwent lumbar spine surgery. Rates of opioid persistence for opioid-naïve patients vs prior opioid use patients were 17.5% and 82.4%, respectively. These findings reflect rates of opioid persistence reflected on other studies.8,26-29 Regarding lumbar spine surgery, Goyal et al found that 30% of patients undergoing posterior lumbar fusion and 19% of patients undergoing lumbar decompression experienced opioid persistence 6 month post-operatively. 28 Notably, however, these authors found opioid persistence rates for opioid-naïve patients to be relatively lower, at 5.6% and 2.0% for opioid naïve patients undergoing lumbar fusion and decompression, respectively. 28 Similarly, Connolly III et al reviewed 8377 patients who underwent lumbar fusion surgery and found that 29.9% experienced opioid persistence after surgery, with patients undergoing 360-degree fusion to be most likely to experience long-term opioid use. 27 Uhrbrand et al conducted a prospective, single-center study of 300 patients and found that 7% of opioid-naïve and 51.5% of prior opioid use patients experience opioid persistence. 8 Lastly, in their retrospective review of 5413 patients undergoing surgery for lumbar disc herniation, Karhade et al showed an overall opioid refill rate of 7.7% for all-comers between 90 and 180 days post-operatively. 26
Regarding persistent opioid use after the cervical spine surgery, the literature suggests somewhat higher rates of opioid persistence. Pugely et al reviewed 17 391 patients undergoing anterior cervical discectomy and fusion (ACDF) and posterior cervical fusion (PCF) and found 45.3% of prior opioid users and 6.3% of opioid-naïve patients experienced persistent opioid use at 1 year postoperatively. 10 Similar rates of opioid persistence were reported by Wang et al, who found that 50.7% of prior opioid users and 17.5% of opioid-naïve patients reported ongoing opioid use after surgery for degenerative cervical conditions. 30
Differences in opioid persistence rates between our study and previous studies may partially be explained by (1) differences in the definition of “opioid persistence”, (2) differences in methodology use to capture prescription data, and (3) state-by-state differences in drug monitoring program requirements during the study period during which opioid use data was captured. Regarding definitions of opioid persistence, most studies focused on 1 of 3 categories: patient-reported opioid use, number of prescription refills, or milliequivalent opioid refills after surgery. Within these categories, persistent opioid use can be further stratified. Per Goyal et al, 28 common definitions include “additional use” or more than 1 opioid refill 90 to 180 days after surgery; 4,31,32 “persistent use” or any span of opioid use starting 180 days after surgery and lasting more than 90 days;33,34 or the Consortium to Study Opioid Risks and Trends (CONSORT) definition – which is persistent opioid use that includes either more than 10 opioid refills or more than 120-day supply of opioids.35,36
We chose to follow patient filling prescriptions filled 180 days post-operatively but did not follow account for additional refills or doses due to limitations in our dataset. Additionally, strategies for capturing opioid use after surgery varies by research group, such as chart review vs pharmacy claims data. We constructed our data set primarily through algorithmic chart review and limited the definition of opioid medication to select medications. A more extensive definition of opioid medications and more robust capture through pharmacy claims data could affect findings for opioid use and opioid persistence after surgery. Lastly changes in state regulations for opioid monitoring programs and institutional level changes to opioid reduction initiatives may influence rates of opioid persistence. For example, a large insurance database study of more than 6 million patients prescribed opioids between 2011 and 2015 showed that comprehensive use of mandates to participate in drug monitoring programs reduced additional opioid prescriptions by 6 to 9%. 37 With respect to surgery, a large cross-sectional study of more than 93 000 patients undergoing general surgery, obstetric/gynecologic surgery, or orthopaedic surgery demonstrated initiation of a statewide drug monitor program was associated with an immediate decrease in opioid prescribed prescriptions across all 3 subspecialties. 38
With respect to risk factors for persistent opioid use, we found risk to be multifactorial. Comparing the opioid-naïve vs opioid persistence groups, we found risk factors to include the following: obesity, ASA ≥3, diabetes, opioid prescription within 60 days preoperatively, patients with cervical stenosis, patients undergoing multi-level lumbar posterior spinal fusion, and patients undergoing multi-level cervical fusion. Additionally, our multivariate regression demonstrated that patients at increased risk of persistent opioid use are those with preoperative opioid use (RR = 2.7), with central cervical stenosis (RR = 2.8), or undergoing multilevel lumbar fusion (RR = 3.0).
Multiple studies have investigated risk factors for persistent opioid use after spine surgery. Patient-specific risk factors include younger age,28,39 pre-operative opioid use,40,41 mental health diagnoses,28,40,42-44 smoking, 42 chronic pain syndromes, 42 socioecnomic status, 43 and use of non-narcotic neuro-modulatory medications.42,44 Surgery-specific risk factors are primarily related to include extent of surgery,28,39,40 such as multi-level fusion, discharge opioid greater than 500 morphine milliequivalents (MME), 28 and prescription of long-acting opioids on discharge. 28 Our findings support earlier studies, which demonstrated an association between preoperative opioid use or multi-level lumbar fusion and risk of postoperative opioid persistence. Our result showing an increased risk of opioid persistence in patients undergoing surgery for central cervical stenosis has not been previously reported in the literature. Approach for cervical decompression and fusion (ie, anterior vs posterior) may partially explain these results, as posterior-based procedures are typically associated with more significant neck pain compared to anterior-based procedures. 45
We showed that these at-risk patients with persistent opioid use after cervical and lumbar spine surgery utilized significantly more health care resources compared to their counterparts who were either never prescribed opioids or successfully weaned off opioids by 6 months. Specifically, we found that this patient population makes more emergency department visits, undergoes more diagnostic imaging (ie, radiographs, CTs, and MRIs), receives more pain medicine referrals, and undergoes more spinal injections. To our knowledge, only 2 studies have specifically linked persistent opioid use with increased health care utilization after elective spine surgery. For example, a study of more than 10 000 patients undergoing surgery for degenerative spondylolisthesis showed that patients with persistent opioid use were likely to incur about 2.8 times the overall costs of a patient who was never opioid dependent before or after surgery. 16 The authors calculated this additional in cost to be between $11,660 and $12,039 per patient. A similar study of patients undergoing surgery for adult degenerative scoliosis demonstrated that patients with persistent opioid use incurred up to 3.03 times the costs of patients without prior opioid dependence of post-operative opioid persistence. 15 They estimated the additional cost to be between $8077 and $27,404 per patient.
Our study adds to the limited body of literature regarding the relationship between persistent opioid use and postoperative health care utilization in 2 specific ways. First, prior studies focused on 1 specific type of spinal pathology, such as lumbar degenerative spondylolisthesis or scoliosis. Our study was the first, to our knowledge, to associate persistent opioid use after cervical spine surgery with increased health care utilization. Second, prior studies used overall cost as the primary outcome representative of health care utilization but did not stratify these costs by services provided. Our study breaks down health care utilization into key, billable points of contact with patients (ie, imaging studies, ED visits, etc.). These results can guide payers, providers, and policymakers in understanding where – in the chain of care delivery – persistent opioid use increases health care utilizations.
Efforts to minimize postoperative opioid use are underway at many institutions. For example, some hospitals are developing programs for enhanced recovery after surgery (ERAS), which aim to decrease overall complications and readmissions and ultimately improve recovery. This comprehensive approach to the preoperative, perioperative, and postoperative care has been shown to secondarily reduce opioid use after elective spine surgery. 46 At Northwestern Memorial Hospital, the orthopaedic surgery department has leveraged the electronic medical record to provide recommended dose number and dosage amount for patients being discharged from the hospital. Residents, surgeons, and other health care practitioners are alerted of best practice opioid prescribed patterns for the relevant CPT codes upon patient admission or discharge. Lastly, surgeons in some Scandinavian countries are trialing postoperative, customized opioid tapering programs combined with telephone counseling to help mitigate issues of persistent opioid use after spine surgery.8,14,47
This study is not without limitations. First, this is a retrospective study of prospectively recorded data. Although we believe that our dataset captures more granular data compared to many large national registries and claims-based data sources, we are still limited by the scope of data recorded by our single institution. Second, we only captured diagnostics tests and medical / surgical services conducted at our institution and outside institutions that participate our collaborative health information exchange record system. Although the majority of hospital systems surrounding our institution participate in this information exchange platform, tests and services rendered outside of the systems may not be recorded. Furthermore, our analysis did not account for certain variables that would strengthen the generalizability of the study, such as insurance status, socioeconomic status, and patient-reported outcomes. Next, our study did not focus on the different classes or types of narcotic pain medication. We did not account for different doses or number of pills prescribed. Instead, we used the numbers of prescriptions written as proxy for these variables. Tracking MMEs vs prescription refills may be a more accurate means method for tracking opioid dependence and persistence post-operatively. Our available dataset limited our ability to use MMEs. We anticipate that future research efforts will track opioid persistence with MMEs and associate MMEs with health care utilization. The goal of these effort would be to find an inflection point at which a certain amount of MME preoperatively, perioperatively, or postoperatively predicts opioid persistence and impact health care utilization.
Conclusion
One-in-six patients undergoing elective spine surgery of the cervical or lumbar spine experience persistent opioid use at 6 months postoperatively. Patients with preoperative opioid use, those undergoing surgery for cervical stenosis, and those undergoing multi-level fusion were at highest risk for persistent opioid use. Moreover, those with persistent opioid use utilized more health care resources and services within 1 year postoperatively. Efforts to curb the rising costs of health care must include interventions that target inappropriate opioid use before and after elective spine surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.